Surgical Management of Polypoid Lesions of the Gallbladder.
Πολυποειδείς Βλάβες Χοληδόχου Κύστεως .
Introduction
Polypoid lesions of the gallbladder are divided into benign and malignant. Malignant polypoid lesions include gallbladder carcinomas, which constitute the fifth most common malignancy of the gastrointestinal tract and the most common malignancy of the biliary system.
Benign polypoid lesions of the gallbladder are subdivided into true tumors and pseudotumors. Most polypoid lesions of the gallbladder are classified as pseudotumors and include polyps, hyperplasia, and various other lesions.
Adenomas constitute the most commonly encountered benign neoplasms of the gallbladder, while cholesterol polyps represent the most frequent pseudotumors of this organ. Polyps may be single or multiple, and their size is usually less than 10 mm.They do not show a predilection for any particular anatomical location within the gallbladder and are usually attached to its wall by a thin, narrow stalk. No malignant potential has been identified in this type of pseudotumor.
Adenomas are the most common type of benign gallbladder neoplasm.They do not show a predilection for development in any specific location of the gallbladder and may be associated with or coexist with gallstones or cholecystitis. The premalignant nature of adenomas remains controversial.
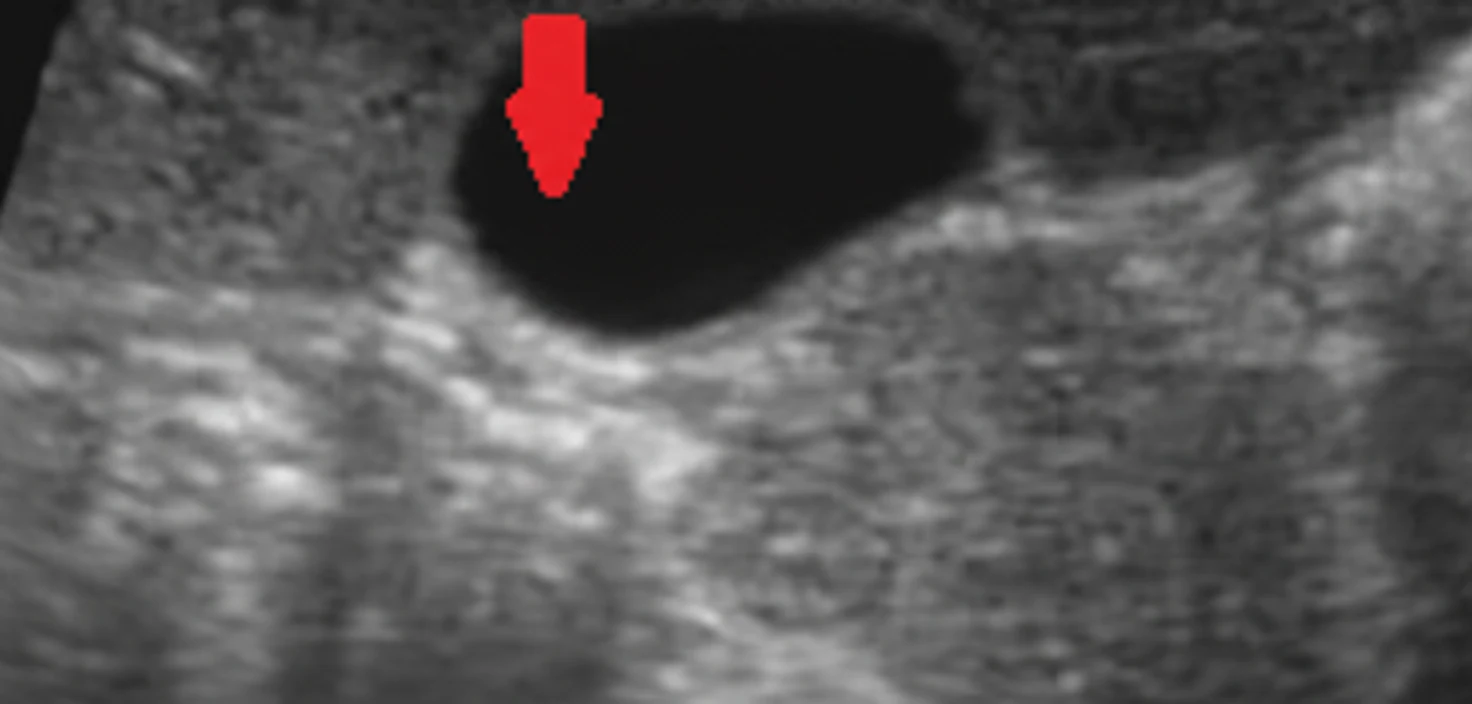
Ultrasonographic examination has proven significantly superior to computed tomography and cholecystography in demonstrating polypoid lesions of the gallbladder.In cases of polyps, a mass fixed to a normal-thickness gallbladder wall is demonstrated, without the presence of acoustic shadowing.
Since gallbladder carcinomas usually present as polypoid lesions, the distinction between benign polypoid lesions and malignancies is extremely difficult, even with the use of high-resolution imaging techniques.
Material - Methods
We retrospectively reviewed 38 cases of patients who were diagnosed sonographically with gallbladder polyps and were managed in our Department during the period 2015-2019. We analyzed the demographic characteristics of the patients as well as their symptoms and imaging findings.In the cases managed surgically, we additionally assessed the histopathological findings.
Results
The mean age of the patients examined was 53.2 years (range 27-79 years). The male:female ratio was 1:1. Overall, 36/38 patients had symptoms that could be associated with gallbladder disease.
Of these, 32/36 had right upper quadrant pain that could be characterized as biliary colic, and 2/36 had symptomatology of acute cholecystitis. Among the remaining 4 patients, two were evaluated for epigastric pain and one for investigation of high fever, during which the gallbladder polyp was incidentally detected on ultrasonography.Finally, one patient was evaluated for jaundice of unknown etiology, without significant findings in the biliary tree on ultrasonography.
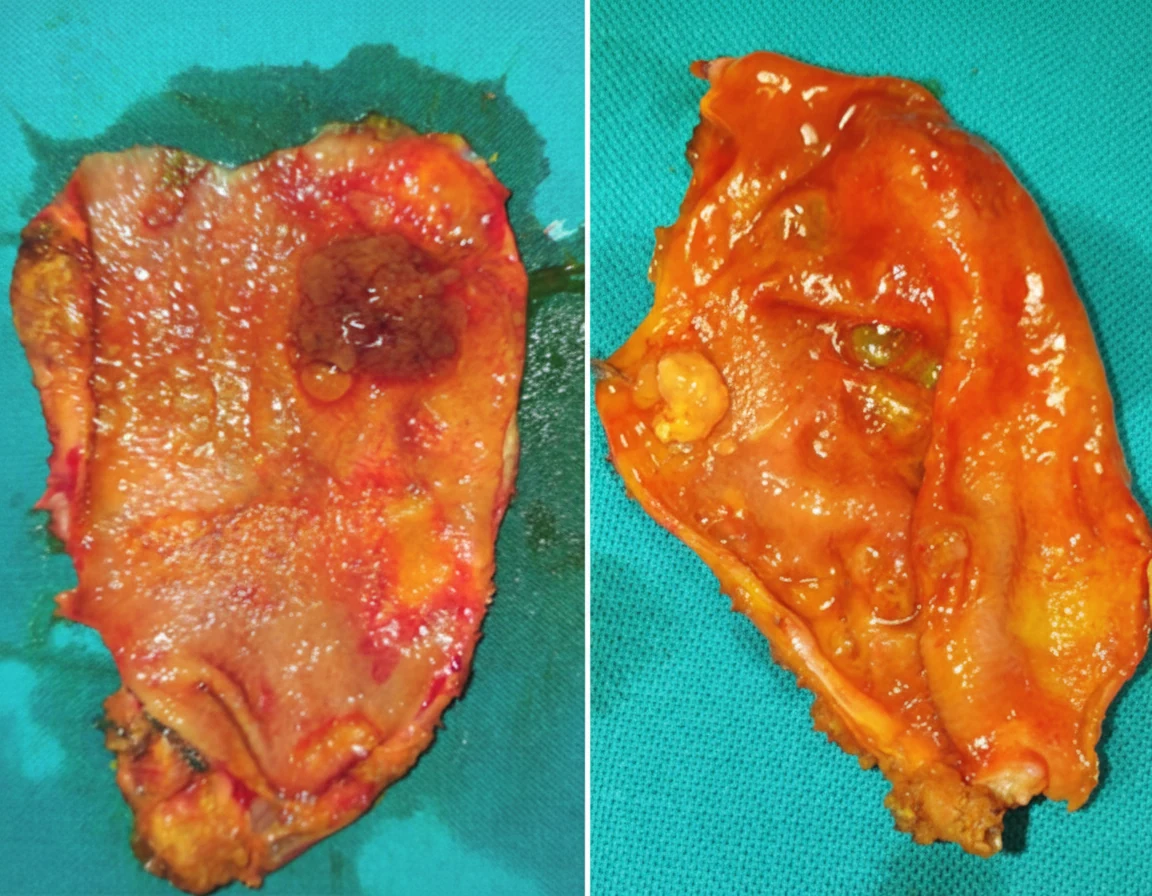
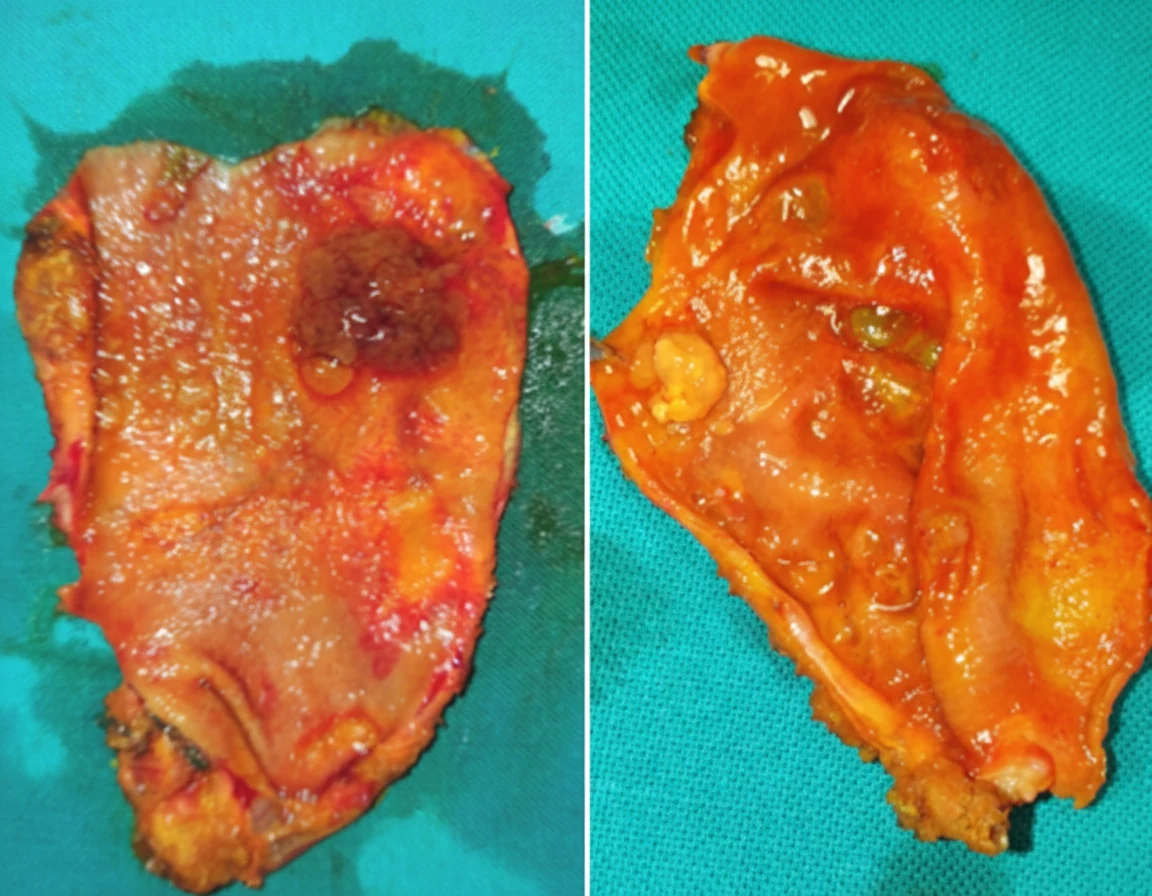
The size of the lesion was noteworthy in only 18 of the 38 patients. Of the 34 patients operated on in total, only 11 were found to have histopathologically confirmed polypoid lesions. On histological examination of the excised gallbladders, one was normal, 7 had cholesterol polyps, one showed polypoid cholecystitis, and two had true gallbladder neoplasms.One patient had a gallbladder adenoma, while the other had adenocarcinoma. The incidence of malignancy was 2.94%, that is, 1/34. All patients with neoplastic polyps had a solitary lesion greater than 1 cm in diameter, while patients with non-neoplastic lesions had multiple lesions smaller than 1 cm in diameter.
In all operated patients except one, pathological gallbladders were found histopathologically. This indicates the presence of chronic cholecystitis, even in the absence of polyps.
Discussion
In general, surgical intervention is not required in young patients in whom very small gallbladder polyps are found and who are free of symptoms. All patients presenting with dyspeptic complaints, without painful episodes consistent with biliary colic, should be managed conservatively.
Cholecystectomy is indicated in patients with large gallbladder polyps exceeding 10 mm in size, regardless of symptomatology.
In patients with polypoid lesions of the gallbladder smaller than 10 mm, cholecystectomy is indicated only if risk factors for complications coexist, such as age greater than 50 years and the coexistence of gallstones.
If the gallbladder polyp is smaller than 10 mm and risk factors for complications are absent, we consider a watch-and-wait strategy to be reasonable.
Conclusions
Although gallbladder polyps are rare, they constitute a significant health problem, as they potentially represent a precursor of gallbladder carcinoma.
Based on the available data and the results and experience gained from our study, we propose cholecystectomy in the following situations: 1) presence of symptomatic lesions, regardless of size; 2) presence of polyps larger than 10 mm, as they carry a risk of carcinoma development; 3) when polyps exhibit rapid growth in size.
Polyps smaller than 10 mm discovered incidentally and not removed should be evaluated sonographically every 6 months. This policy is particularly crucial for sessile polyps, in which the likelihood of the presence or development of a small carcinomatous polyp is greater than in pedunculated polyps.
Finally, asymptomatic lesions smaller than 10 mm must be removed if the patients are older than 50 years and coexisting cholelithiasis is present.
- Gallbladder polyps are found in 4-7% of ultrasound examinations
- Size >10 mm is the strongest indicator for cholecystectomy (12% malignancy rate)
- Polyps 6-9 mm require surveillance ultrasound every 6-12 months
- Single sessile polyps and age >50 are additional risk factors
- Frozen section during cholecystectomy guides the need for radical resection
Sign in to join the discussion
Loading...