Primary Gastrointestinal Stromal Tumor (GIST) of the Liver.
Πρωτοπαθές GIST Ήπατος.
Introduction
Gastrointestinal stromal tumor is the most common type of mesenchymal tumor, predominantly encountered in the gastrointestinal tract. The tumor arises from the cells of Cajal, which are responsible for the motility of the gastrointestinal tract.
Stromal tumors of the liver are rare, and only a few cases have been reported in the literature (23 cases between 2003 and 2019). The primary stromal tumor of the liver is usually found as a cystic tumor, which is identified histopathologically and immunohistochemically by testing for CD117, DOG-1, and S100.
The treatment of choice for most stromal tumors, or stromal tumors outside the gastrointestinal tract, is surgical excision, as most of them are localized.
Case Report
A 56-year-old patient presented at the outpatient clinic of our department, complaining of epigastric pain, loss of appetite, and malaise. He had initially been investigated at a regional hospital with a CT scan, the report of which was confusing, as it described the presence of a tumor infiltrating the stomach and the left lobe of the liver.
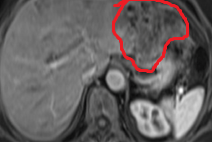
On clinical examination, a palpable mass was noted in the epigastrium. Tumor markers (alpha-fetoprotein, CEA, and CA 19-9) were normal, so we decided to further investigate the patient with MRI, the images of which revealed the presence of a well-defined mass measuring 13.1 x 19 cm, with a multilobulated contour, low signal intensity on T1-weighted images and high signal intensity on T2-weighted images, compressing the stomach.Gastroscopy and colonoscopy were negative for pathological findings.
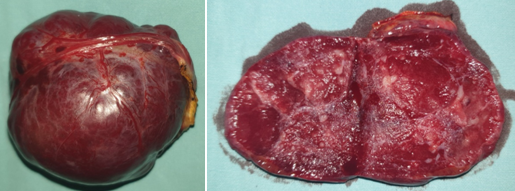
We decided to proceed with excision of the tumor, which exhibited hemorrhagic components and calcifications.
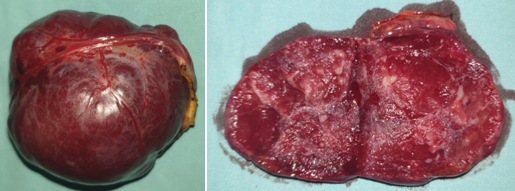
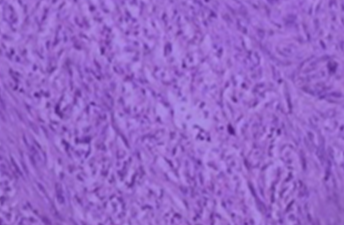
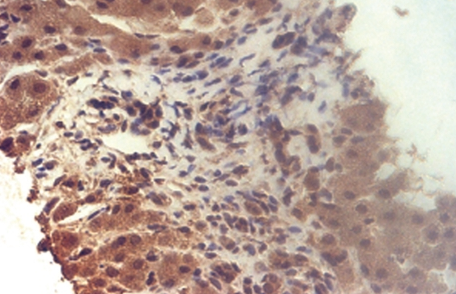
The patient had an uneventful postoperative course. Histopathological and immunohistochemical studies revealed the presence of a primary stromal tumor of the liver, with positive expression for CD117 (++), DOG-1 (++), S100, and Ki-67 (+1%).
The patient was discharged from the hospital 6 days later and, on the oncologist's recommendation, received 3 cycles of adjuvant chemotherapy. Six years later, he remains in excellent general condition, without recurrence or other hepatic foci.
Discussion
Stromal tumor is the most common tumor arising from mesenchymal tissue in the gastrointestinal tract. The lesion arises from the interstitial cells of Cajal. These cells are responsible for activating the motility of the gastrointestinal tract.These tumors are usually located at sites of the gastrointestinal tract, such as the stomach, small intestine, large intestine, and esophagus. Stromal tumors are solid lesions, sometimes with cystic components and calcifications, but rarely with cystic morphology.When these lesions hemorrhage internally or develop necrosis, they may contribute to the formation of large cystic masses. This appearance is more frequently encountered in patients receiving tyrosine kinase inhibitors. However, the exact cause of the development of cystic stromal tumors remains unclear.
The development of primary stromal tumors outside the gastrointestinal tract, and particularly in the liver, is extremely rare, and is reported only in a few cases.
In previous studies, cells resembling the interstitial cells of Cajal have been identified in the portal vein of humans and animals using immunohistochemical stains, which have similar functions and structures to true interstitial cells of Cajal.Further research has shown that these cells are present in the human embryonic liver as precursor or progenitor cells, meaning that they have the capacity to differentiate into other cell types. From the above, it can be concluded that the rare stromal tumors of the liver can develop from these undifferentiated cells.
MRI imaging of these tumors often demonstrates large, well-defined masses, exerting pressure on adjacent organs and anatomical structures. In our case, the patient had a large lesion in the left lobe of the liver, well-defined, measuring 13.1 x 19 x 8.6 cm, compressing the stomach and exhibiting imaging characteristics of low signal intensity on T1-weighted images and high signal intensity on T2-weighted images.The solid components and wall of the lesion showed enhancement during the arterial, venous, and delayed phases.
The differential diagnosis includes: 1) liver abscess, with presence of necrosis and internal hemorrhage; 2) hemorrhagic infected hepatic cyst; 3) hemorrhagic cyst of the pancreatic tail; 4) hemorrhagic tumor of the stomach; and 5) pancreatic pseudocyst.
Regarding tumor marker levels, such as alpha-fetoprotein, CA 19-9, and CA 125, they may show slight deviations from normal values and raise suspicion of malignancy; however, it must be categorically emphasized that there are no specific markers that define the presence of these particular neoplasms.
The therapeutic management of these tumors is surgical excision, as in most cases the lesion is localized. An alternative option is the use of radiofrequency or microwave ablation, with encouraging initial results.
Conclusions
Primary stromal tumor of the liver is a rare and difficult-to-diagnose tumor, due to atypical clinical and imaging findings. Therefore, when a large, cystic or non-cystic lesion is detected in the liver, the possibility of this neoplasm should be considered.
- Primary hepatic GIST is extraordinarily rare (<20 reported cases)
- Diagnosis requires exclusion of primary GI source through endoscopy
- IHC: CD117+ and DOG1+ confirms GIST; molecular analysis identifies KIT mutations
- Hepatic resection with clear margins is the surgical treatment
- Adjuvant imatinib is recommended for intermediate and high-risk tumors
Sign in to join the discussion
Loading...