Premature Metastasis of Renal Cell Carcinoma.
Πρόχρονη Μετάσταση Καρκίνου Νεφρού.
Introduction
Clear cell renal cell carcinoma is the most common type of renal malignancy and is encountered in 80-90% of all cases of malignant tumors of this organ. It mainly affects African American men between the 6th and 8th decade of life.Smokers who smoke at least 20 cigarettes daily are also at increased risk of developing this malignancy. This cancer is usually asymptomatic, but there are also cases of patients who present with hematuria, abdominal pain, and a palpable mass in the lumbar region.This malignancy is also diagnosed through the manifestation of metastases in distant sites, such as the lungs, liver, lymph nodes, and adrenal glands. A more rare site of metastatic presentation is the skin, which accounts for approximately 1-3.3% of cases, constituting a late manifestation of the disease.
Although the presentation of a metastatic carcinoma from an unknown primary malignant tumor site constitutes a clearly recognized entity, the underlying causes of the failure of manifestation/presentation of the primary disease remain largely unclear/unknown.
The explanation for this phenomenon ranges from spontaneous regression of the primary tumor to early manifestation of metastasis, prior to the appearance of a less aggressive primary tumor.
We report the case of a premature metastasis in a 66-year-old patient, who presented without the presence of a primary tumor/malignancy in the kidneys, and the subsequent aggressive development/manifestation of a primary cancer of the right kidney 5 months later.
Case Report
A 66-year-old female patient, with an unremarkable personal medical history, presented at the outpatient clinic of our department, complaining of the presence of a slowly growing swelling in the anterior chest wall. The patient declared herself a smoker, but denied taking any medications or consuming alcohol.Her family history was unremarkable, and the swelling under examination had been present for at least 4 months. On clinical examination, we palpated a subcutaneous swelling measuring 1.6 x 2.5 cm in the anterior chest wall. It was mobile, painless, of soft/elastic consistency, and non-pulsatile.We observed no other skin lesions or swellings on the rest of her body.

Laboratory workup of the patient was normal and, under the clinical impression that this was a lipoma, we performed ultrasound examination, which revealed the presence of an ovoid, solid, and well-defined swelling in the subcutaneous space.

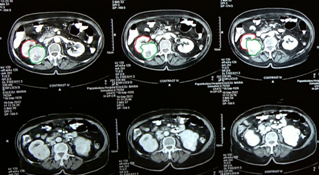
Despite a negative clinical examination, we performed CT of the abdomen and thorax before proceeding with excision of the swelling.

Under local anesthesia, we proceeded with excision of the swelling and were met with an unpleasant surprise when we were informed that histopathological and immunohistochemical examination revealed the presence of a metastatic clear cell renal cell carcinoma.
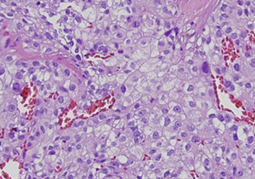
Histopathological examination: Solid sheets of cells, with clear to vacuolated cytoplasm and the presence of macronuclei. The delicate microvasculature is characteristic/typical of clear cell renal cell carcinoma. The neoplastic cells were positive for Ca IX, CD10, and RCC, while they were negative for Sox10 (melanoma), PLAP (germ cell tumors), GCDFP-15, CK7 (breast tumors), and CD31 (vascular tumors).
Due to the imaging inability to identify the primary focus, the patient was placed under close follow-up (clinical and imaging). Five (5) months later, we identified the presence of a large tumor in the right kidney.

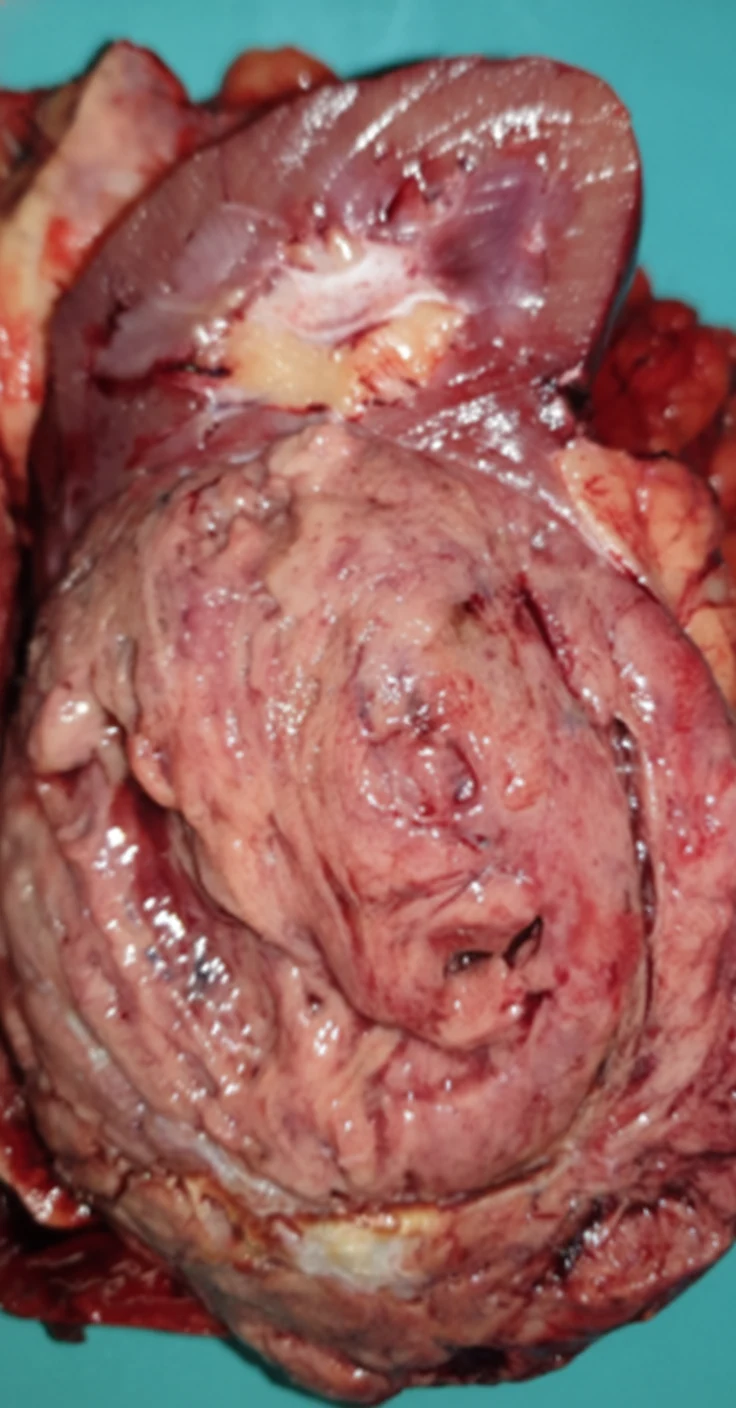
Subsequently, we performed staging of the disease, which did not reveal the presence of other secondary localizations, and so we proceeded with right nephrectomy.
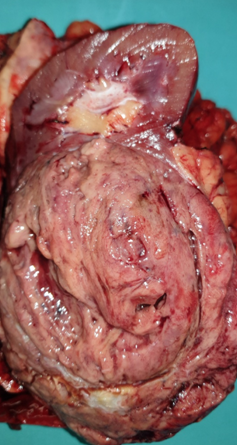
The patient had an uneventful postoperative course and was discharged from the hospital 5 days later. Histopathological examination was absolutely identical to the excised metastatic focus of the chest wall.
She was referred and received adjuvant chemotherapy from the oncologist, to whom her follow-up was subsequently assigned.
As far as we know, the patient was alive 3 years later, without local recurrence or the appearance of distant metastases.
Discussion
Approximately 25-30% of patients with clear cell renal cell carcinoma present with metastases at the time of diagnosis, but fewer than 5% of them have a solitary metastasis. Neoplasms with sarcomatoid features have the worst prognosis.
Our patient presented initially with a symptomatic metastatic focus/metastasis, while the primary cancer was evidently absent.The primary malignancy appeared 5 months after excision of the solitary metastasis.
This phenomenon was first reported in the case of a 51-year-old patient who presented with a symptomatic brain metastasis, while the primary lung cancer was eventually identified 5 years after excision of the solitary metastasis.
We tried to find the most suitable term to describe this situation. The terms "synchronous metastasis" and "metachronous metastasis" are fully understandable, referring to the time of appearance of metastasis in relation to the appearance/development of the primary neoplasm.Synchronous metastasis means simultaneous manifestation/revelation of the metastasis and the primary tumor, while metachronous means subsequent development/appearance of the metastatic focus after the primary tumor. The term "premature" clearly describes the phenomenon we report in our communication, i.e., the appearance of the metastatic focus before the revelation of the primary malignancy.
POSSIBLE HYPOTHESES EXPLAINING THE PHENOMENON.
In the case of the classical model of delayed metastatic dissemination, the metastatic sequence of events constitutes a sequential, multi-step process, during which cancer cells depart from the primary cancer and enter the lymphatics, blood vessels, and body cavities, where they are deposited in nearby or distant sites, before proliferating/developing and colonizing ectopic tissues.It is known that metastases display a preference for specific sites and require/need these key sites in order to thrive/develop.
Recently, there is evidence supporting the model of early dissemination, namely the fact that metastasis occurs early in the life cycle of carcinogenesis.
Kaplan et al., experimenting with mice, demonstrated that cancer cells transmit signals involving VEGFR1 (vascular endothelial growth factor receptor 1) and fibronectin to bone marrow cells, in order for them to migrate to distant organs and establish an environment willing/prepared to host metastases.This phenomenon precedes the formation of micrometastatic colonies in these organs by 4 to 6 days. The case of our report, although undocumented, could be explained on the basis of the theory of the early dissemination model.
There are some clinical similarities between our case and the phenomenon of burnout of cancers, which is more frequently encountered in germ cell malignancies.In patients with the above burnt-out cancers, the metastatic foci are identified first, in the presence of the regressed tumors/cancers, with the latter being diagnosed due to the appearance of distinct histopathological features.
However, we must admit that our case differs, as the primary tumor exhibits a clearly aggressive clinical behavior after excision of the metastatic focus, with transition of the radiological image from invisible to a 14 cm lesion over a period of 5 months, something that does not correspond with regression of the primary cancer.
Conclusions
Premature metastasis of Renal Cell Carcinoma represents an uncommon and aggressive clinical presentation that underscores the unpredictable biological behavior of renal malignancies.
Early metastatic spread may occur even in the absence of advanced local disease or typical radiologic findings, creating significant diagnostic and therapeutic challenges.
We present a case of a sarcomatoid clear cell renal cell carcinoma, demonstrating the extremely rare phenomenon of "premature metastasis", directly supporting the model of early metastatic dissemination.
This case highlights the importance of maintaining clinical vigilance and performing thorough systemic evaluation in patients with renal cell carcinoma, particularly when atypical symptoms or rapidly progressive disease are present.
Early recognition of metastatic involvement and timely multidisciplinary management are essential for optimizing treatment strategies and improving patient outcomes.
- Cutaneous metastasis as first presentation of occult RCC is rare but well-documented
- Skin lesions with vascular appearance and clear cell histology should prompt renal imaging
- IHC: PAX-8+, CD10+, RCC antigen+ confirms renal origin
- Radical nephrectomy for the primary plus systemic targeted therapy for metastatic disease
- Early cutaneous metastasis does not preclude long-term survival with combined treatment
Sign in to join the discussion
Loading...