Postoperative Thrombotic Thrombocytopenic Purpura following Restorative Proctocolectomy.
Μετεγχειρητική Θρομβωτική Θρομβοπενική Πορφύρα.
Introduction
Thrombotic thrombocytopenic purpura (TTP) is a rare, life-threatening disease characterized by acute episodes of thrombocytopenia and microangiopathic hemolytic anemia, which occur due to the deposition of platelets and von Willebrand factor polymers, the formation of thrombi in arterioles and capillaries throughout the body, ultimately resulting in organ ischemia.TTP may be idiopathic or secondary. There is a clinical syndrome resembling TTP that appears postoperatively and is termed postoperative TTP.
The acute development of thrombotic thrombocytopenic purpura (TTP) postoperatively constitutes a recently recognized syndrome, which, like classic or idiopathic thrombocytopenic purpura, manifests in various ways, including microangiopathic hemolytic anemia, thrombocytopenia, fever, renal failure, and mental disturbances.
Although most reports of postoperative TTP are associated with cardiovascular surgical procedures, there are very few reports linking it to orthopedic and other surgical interventions.
Case Report
We present the case of a 43-year-old female patient who underwent surgical treatment (total orthoproctocolectomy, creation of a J-shaped ileal pouch, pouch-anal anastomosis, and temporary protective ileostomy) for the management of ulcerative pancolitis refractory to conservative medical therapy.
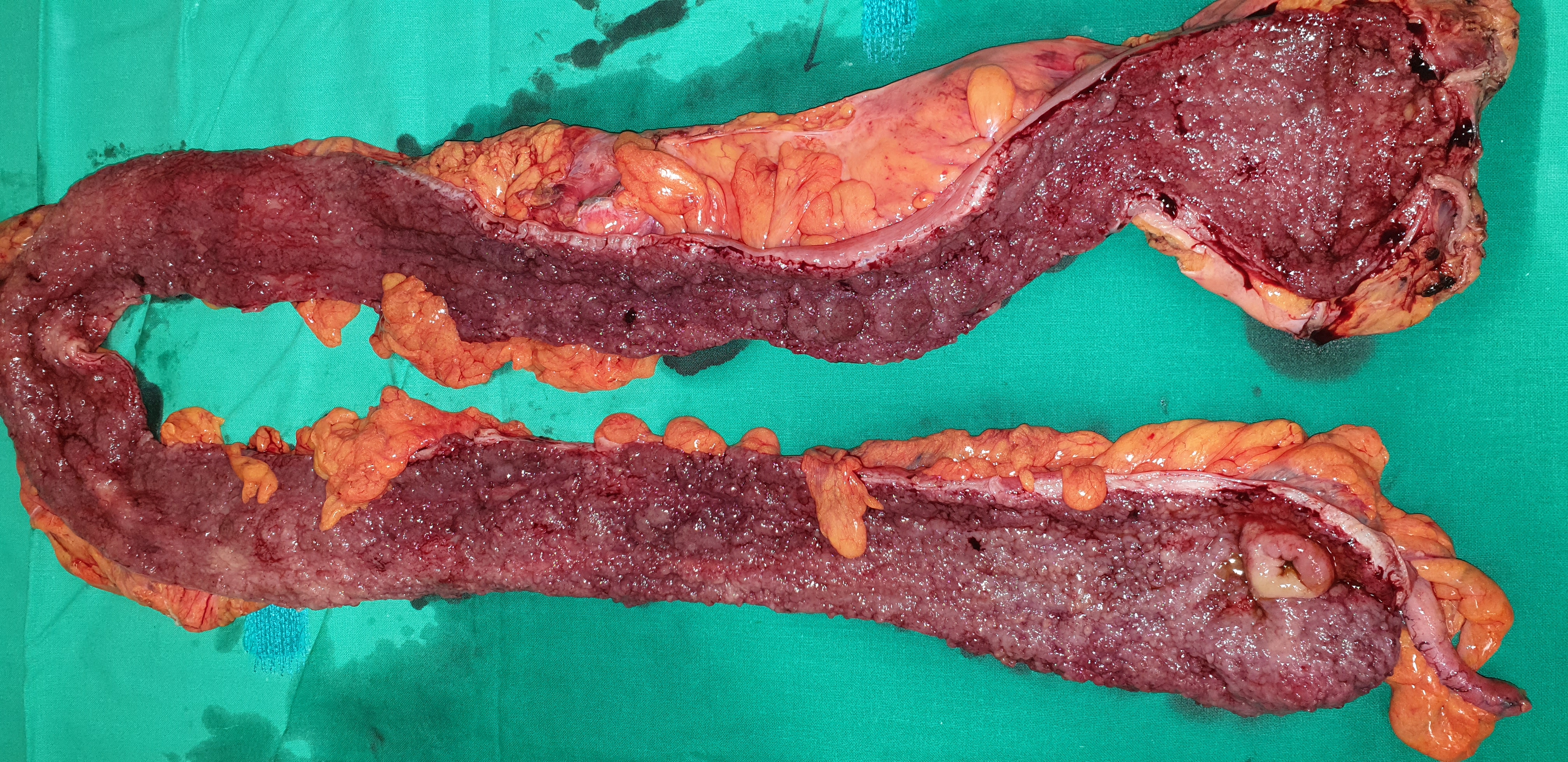
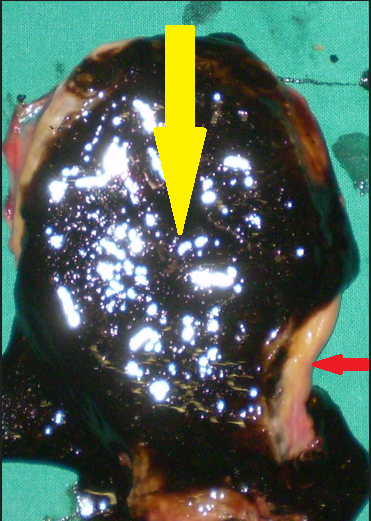
Her postoperative course was uneventful; however, on the 9th postoperative day, she developed septic-type fever and tenderness in the right hypochondrium. Thorough clinical, laboratory, and imaging investigation revealed the presence of acalculous cholecystitis (thickened gallbladder wall and presence of biliary sludge).
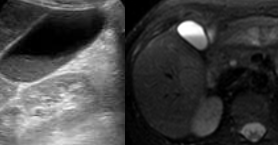
Based on the above findings and the negative remaining laboratory workup, we concluded that the patient's symptoms were attributable to the development of acalculous cholecystitis, and we performed a cholecystectomy for its management.
Immediately postoperatively, the patient's symptoms subsided; however, 5 days later, she presented with a clinical picture of postoperative TTP.We reached this diagnosis after detailed hematological investigations and after excluding the presence of disseminated intravascular coagulation syndrome, anticoagulant-associated thrombocytopenia, and potential toxic effects of pharmacotherapy.
The patient was transferred to the ICU, where she was immediately treated with plasmapheresis, as would be the case for classic TTP, along with supportive therapy. The patient was discharged from the hospital after two months without experiencing a relapse of her condition.

Discussion
Postoperative thrombotic thrombocytopenic purpura (postoperative TTP) constitutes a recently recognized, life-threatening clinical syndrome, with significant similarities to classic TTP (thrombotic thrombocytopenic purpura) regarding its presentation and response to early treatment with plasmapheresis.
To date, 29 cases of postoperative TTP have been reported. The majority of cases occur as a complication of cardiothoracic and vascular surgical procedures, while very few cases are associated with orthopedic operations and gastrointestinal tract surgery.
Characteristically, patients develop microangiopathic hemolytic anemia and consumptive thrombocytopenia 5 to 9 days after the surgical procedure, with variable presence of fever, renal function impairment, and altered level of consciousness.
The pathogenesis of postoperative TTP is hypothetical, but most likely involves the release of large quantities of high molecular weight von Willebrand factor (vWF) polymers, as a result of endothelial damage occurring during surgical procedures, in an environment of borderline levels of vWF-cleaving enzymes.The large number of postoperative complications that may mimic clinical manifestations similar to TTP results in confusion, ultimately leading to delayed initiation of life-saving plasmapheresis therapy.
The occurrence of TTP represents one of the most difficult diagnoses for the clinician after cardiothoracic or other surgical procedures, due to the rarity of the disease and the limited specificity of clinical and laboratory signs and symptoms.The classic pentad (thrombocytopenia, anemia, fever, neurological and renal disturbances) is present in its entirety in only a very small number of patients. Consumptive thrombocytopenia and microangiopathic hemolytic anemia (MAHA), as demonstrated by fragmented red blood cells on blood smears and elevated LDH levels, constitute extremely useful laboratory findings for the clinician.However, these abnormalities may also be found in a variety of other conditions characterized by diffuse microcirculatory thrombosis (thrombotic microangiopathies), such as classic hemolytic uremic syndrome (HUS), atypical aHUS, disseminated intravascular coagulation (DIC) syndrome, or septic states.
Postoperative development of TTP is frequently attributed to the acquired development of ADAMTS13 autoantibodies, resulting in severe ADAMTS13 deficiency. This condition is often associated with cardiothoracic or vascular surgical procedures and is believed to be caused by endothelial damage.The above may occur following the release of large quantities of vWF under conditions of low levels of the vWF-cleaving protease, ADAMTS13. This protease regulates the size of vWF polymers and constitutes an important mediator for platelet adhesion.ADAMTS13 regulates the size of vWF by cleaving a peptide bond in the A2 domain. Without this regulation, the accumulation of ultra-large vWF polymers leads to microvascular platelet thrombi, destruction of red blood cells and platelets, resulting in compromised blood flow to vital organs such as the brain and kidneys.
The laboratory tests used for the diagnosis of postoperative TTP include detection of vWF antigens and polymer patterns, as well as the activity and presence of ADAMTS13 protease autoantibodies. Identification of the responsible antibodies may help establish the diagnosis of TTP and provide prognostic information regarding response to plasmapheresis therapy and the risk of relapse.Studies have demonstrated that cases of severe protease deficiency show good response to plasmapheresis, at rates approaching 80-90%, but simultaneously carry significant risks of disease relapse in at least one-third of cases.
Clinical prediction rules, utilizing available laboratory information (creatinine, platelet count, d-dimer levels, reticulocyte count, indirect bilirubin, etc.) have proven useful for decision-making in the acute phase.The initial therapeutic approach for acquired postoperative TTP includes immunosuppression and plasmapheresis, in order to suppress antibody production, reduce antibody titers, and provide supplemental ADAMTS13 protease. Although the finding of reduced ADAMTS13 activity aids in the diagnosis of TTP, treatment must be initiated before laboratory results become available.Indeed, clinicians determine the duration of plasmapheresis based on platelet count recovery and resolution of hemolysis and neurological symptoms, rather than on restoration of ADAMTS13 protease activity.
Reviewing the English-language literature, we identified very few reports of postoperative TTP development following cardiothoracic procedures (mitral and aortic valve replacement), vascular procedures (aortic aneurysm), after childbirth, after orthopedic procedures, after urological procedures (transurethral prostatectomy), after bone marrow transplantation, after plastic surgery procedures, after esophagectomy for cancer, after liver transplantation, but no reports following colectomies and specifically total orthoproctocolectomy for medically uncontrolled ulcerative colitis.
Therefore, it is very important for clinicians and IBD surgeons to remain vigilant regarding the possibility of postoperative TTP occurrence, in order to promptly recognize the phenomenon and treat it at an early stage, thereby preventing as much as possible both morbidity and mortality
Conclusions
To the best of our knowledge, the case we described represents the first report of postoperative TTP occurrence following total colectomy for ulcerative colitis. Because the mode of presentation can be confused with other early postoperative complications, solid knowledge of the syndrome is essential.The diagnosis of postoperative TTP is made by exclusion, as with classic TTP, and patient management must be immediate in order to reduce morbidity and mortality. Although it is encountered rarely, surgeons and clinicians of all specialties must remain on alert in order to diagnose as quickly as possible this life-threatening condition and treat it immediately with plasmapheresis in a controlled environment.
- Postoperative TTP is a recently recognized life-threatening syndrome resembling classic TTP, developing 5-9 days after surgery with microangiopathic hemolytic anemia and consumptive thrombocytopenia
- Diagnosis requires exclusion of DIC, heparin-induced thrombocytopenia, and drug toxicity; ADAMTS13 activity and vWF multimer analysis are key investigations
- Plasmapheresis achieves 80-90% response rates but carries approximately 33% recurrence risk
- This is the first reported case of PTTP following total orthoproctocolectomy for ulcerative colitis
- Early recognition and immediate plasmapheresis in an ICU setting are critical for reducing morbidity and mortality
Sign in to join the discussion
Loading...