Novel Management of Chylous Ascites following Laparoscopic Nissen Fundoplication.
Χυλώδης Ασκίτης.
Abstract
The development of chylous ascites is a rare complication following laparoscopic Nissen fundoplication. This case highlights the importance of strict adherence to the surgical principles required during this particular operation, in order to minimize the likelihood of iatrogenic injuries that may lead to significant morbidity. Nevertheless, should this particular complication arise, transabdominal glue embolization constitutes a safe and effective method for the management of thoracic duct injury, when conservative efforts have failed.
Introduction
Chylous ascites is a rare and challenging complication that may be caused by abdominal injuries, neoplasms, inflammatory conditions, and as a consequence of various surgical procedures. Iatrogenic injury usually occurs when dissection is performed near the base of the mesentery, in the retroperitoneum, or at the cisterna chyli of Pecquet, resulting in injury/damage to the abdominal lymphatic vessels.
Performing a laparoscopic Nissen fundoplication may cause lymphatic vessel injury, although very few cases have been reported in the international literature. All cases were managed with conventional conservative methods, namely cessation of oral feeding, administration of enteral or total parenteral nutrition, and upon failure, transabdominal surgical ligation of the injured lymphatic vessel.
The use of glue embolization of the injured lymphatic vessel for the management of chylothorax is increasingly reported in the international literature. Although located at a different anatomical site, chylous ascites can be managed in the same manner, by transabdominal embolization of the injured lymphatic vessel proximal to the site of leakage.
We describe the case of a patient who underwent laparoscopic Nissen fundoplication at another hospital for the management of gastroesophageal reflux disease and was transferred postoperatively to our Department for the management of persistent chylous ascites that did not respond to conservative therapy.
To the best of our knowledge, this particular technique has very rarely been used for the management of lymphatic vessel injuries.
Case Report
A 46-year-old male patient with a longstanding problem of gastroesophageal reflux disease refractory to conservative therapy underwent laparoscopic Nissen fundoplication at another hospital in our city. According to his account, the entire procedure progressed uneventfully, and he was discharged 2 days later.
After 20 days, the patient presented to the Emergency Department of our Hospital, severely dehydrated, with clinical and laboratory findings of prerenal renal failure. From the history, it emerged that he had been persistently coughing and experiencing difficulty breathing for the past 4 days.
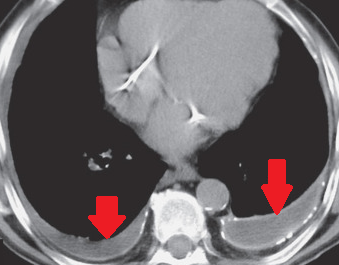
Clinical examination revealed significant abdominal distension accompanied by diffuse tenderness, while chest and abdominal CT scans revealed the presence of bilateral pleural effusions and ascitic fluid in the peritoneal cavity. We aspirated both the pleural effusions and the ascites and requested biochemical analysis, which revealed high levels of albumin and triglycerides in all samples (154 mg/dL).
With this finding, we established the diagnosis of bilateral chylothorax and chylous ascites. Subsequently, the patient was transferred to the Thoracic Surgery Department, where bilateral chest tubes were placed and 1.2 liters of chylous content was drained from both thoracic cavities.
Oral feeding was discontinued, and the patient received total parenteral nutrition and somatostatin intravenously. Despite conservative management, the chyle leak continued, so due to the inability to locate the site of injury, ligation of the thoracic duct was performed between the aorta and the azygos vein at the level between the 8th and 9th ribs on the right.
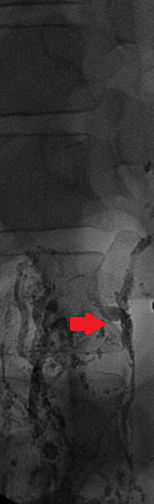
Unfortunately, despite the successful procedure, the leakage continued, and our assistance was again sought to resolve the problem. After transfer to our department, we decided to perform bipedal lymphangiography, which revealed extensive leakage from the thoracic duct at the level of T9 and accumulation in the left hypochondrium.
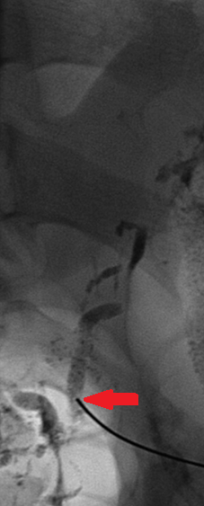
With the assistance of the interventional radiologist, catheterization of the thoracic duct was achieved below the site of leakage, and embolization was performed with N-butyl cyanoacrylate glue. The intervention was entirely successful and resulted in the gradual reduction of output from the thoracic drains as well as the abdominal circumference.
After complete drainage, the chest tubes were removed, and the patient, free of symptoms, resumed oral feeding. He was discharged from the hospital a few days later, and after 6 months, he was symptom-free, eating freely by mouth, had achieved significant weight loss, his abdominal circumference had returned to normal levels, and there were no findings suggestive of chylous ascites recurrence.

Discussion
Performing laparoscopic Nissen fundoplication is now the method of choice for the management of gastroesophageal reflux disease. The most common complications of the method are pneumothorax, pneumomediastinum, esophageal perforation, gastric perforation, hemorrhage, and mesenteric vein thrombosis.
The development of chylous ascites is reported as an extremely rare occurrence, as it is more commonly observed during lymphadenectomies, pancreaticoduodenectomies, peripheral splenorenal shunts, and aortic surgical procedures. The anatomy of the thoracic duct and its relationship to the esophagus and stomach make this complication rare, provided the procedure is performed safely and with the appropriate care.
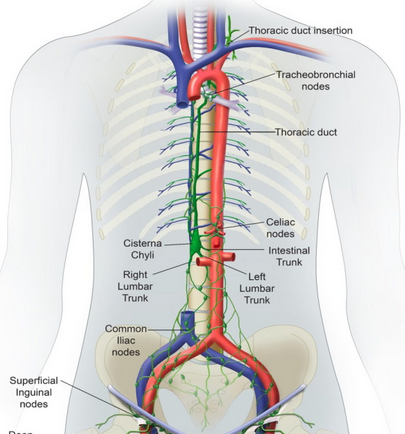
The thoracic duct is the largest lymphatic channel in the body. Apart from the areas of the right head, neck, upper extremities, and thorax, this channel is responsible for draining lymph from the rest of the body.The flow begins at the level of the cisterna chyli within the abdomen, acting as a confluence point for other smaller lymphatic vessels originating from the lumbar region, intestine, liver, and lower intercostal sources, located between the abdominal aorta and the azygos vein.It courses behind the right crus of the diaphragm, along the right posterior mediastinum, with its final destination near the confluence of the left subclavian vein with the left internal jugular vein. The true presence of a cisterna chyli is found in only 50% of individuals, while in the remainder where it is absent, this anatomical confluence is replaced by smaller abdominal and lower extremity lymphatic channels that drain directly into the thoracic duct.
The anatomical course of the thoracic duct in relation to the esophagus demonstrates the rarity with which this injury should occur during laparoscopic Nissen fundoplication, if performed with the requisite care.
However, there are two steps during the operation that deserve particular attention. First, particular care is needed when entering the retroperitoneum medial to the right crus of the diaphragm, when opening the retroesophageal window before the final passage of the gastric fundus. This step is critical, as lymphatic channels are exposed, rendering them susceptible to injury or thermal damage from diathermy use if the retroesophageal dissection extends too far posteriorly.The second step that renders the thoracic duct vulnerable to injury is the moment of re-approximation of the two diaphragmatic crura, as obstruction of the duct may occur during this maneuver. In the case we report, it is rather evident that the injury occurred by the first mechanism, as the lymphangiography revealed lymph leakage from the duct into the peritoneal cavity.
This complication could have been avoided if the dissection on the posterior surface of the esophagus had been performed in the correct plane. The postoperative occurrence of this complication is initially managed conservatively, with surgical intervention reserved for refractory cases.
First-line conservative management includes dietary changes, such as a low-fat diet (long-chain triglycerides) or alternatively complete cessation of oral feeding and administration of intravenous total parenteral nutrition.
Most cases of chylous ascites development after laparoscopic Nissen fundoplication are successfully managed with dietary changes alone. Other cases attributed to other etiologies were managed pharmacologically with the administration of somatostatin and/or octreotide.
Surgical intervention is indicated in persistent cases, with maintenance of symptoms despite dietary restrictions and deterioration of the patients' general condition. In our patient's case, despite the failure of conservative and surgical methods, we ultimately managed the thoracic duct injury problem using the unconventional method of glue embolization.
Lymphangiography constitutes the examination of choice for imaging the lymphatic system. This technique precisely locates the site of injury and allows exclusion of the leak by embolizing the duct with lymphangiographic glue. The substance used has the characteristic of bonding rapidly and effectively, polymerizing upon contact with anionic substances such as plasma, blood cells, endothelium, or normal saline, causing a local inflammatory reaction, ultimately resulting in fibrosis.
This technique was first described by Cope et al in 1998. In a series of 42 patients, the author demonstrated that it is a safe and effective method for definitive or partial resolution of the problem in 74% of patients with refractory chylothoraces.
Although it has been used primarily for the management of chylothoraces, the application of the technique is the same in the case of lymphorrhea into the peritoneal cavity. The thoracic duct is punctured transabdominally at the level of the cisterna chyli under continuous fluoroscopic guidance, and then embolization is performed before the site of injury, in the abdomen or thorax.
Conclusions
The development of chylous ascites constitutes a rare complication following laparoscopic Nissen fundoplication. This case highlights the importance of adherence to the surgical principles required during the performance of this particular procedure, in order to minimize the chances of iatrogenic injuries that may lead to significant morbidity.
Nevertheless, should this specific complication occur, transabdominal glue embolization constitutes a safe and effective method for managing thoracic duct injury if conservative efforts fail.
- Chylous ascites is a rare complication of laparoscopic Nissen fundoplication caused by lymphatic vessel injury during hiatal dissection
- Conservative management (NPO, TPN, octreotide) should be the first-line treatment for postoperative chylous ascites
- Percutaneous transabdominal lymphatic embolization with cyanoacrylate glue is a viable minimally invasive alternative when conservative measures fail
- Lymphoscintigraphy and MR lymphangiography are essential for localizing the site of lymphatic leakage
- This novel approach avoids the morbidity of surgical re-exploration while achieving definitive treatment
Sign in to join the discussion
Loading...