Brenner Tumor of the Ovary - An Incidental Finding.
Ωοθηκικός Όγκος του Brenner.
Introduction
Brenner tumor was first described in 1907 by Fritz Brenner, who hypothesized that it originated from the granulosa cells of the ovarian follicles. Histological examination reveals solid or cystic epithelial cell nests resembling urothelium, surrounded by fibrous stroma.Interestingly, these tumors can also develop in extra-ovarian sites and display the same histological picture as those found in the ovaries. Extra-ovarian Brenner tumors are extremely rare and were first reported by Robinson in 1950.To date, 16 cases of extra-ovarian Brenner tumors have been identified, located in the lower abdomen, pelvis, broad ligament, vagina, and testis or peritesticular tissues.
Brenner tumor is a rare ovarian neoplasm belonging to the group of surface epithelial neoplasms of the organ.The mean age of occurrence is 50 years; it accounts for 1.4-2.5% of all ovarian neoplasms and has a predilection for postmenopausal women. These tumors are usually asymptomatic and are most often discovered incidentally during operations for other causes.Most are benign, and only 5% exhibit rapid growth or are of borderline histological malignancy.
We present the case of a female patient with a history of colectomy for colorectal cancer and metachronous recurrence in the left lower abdomen with entrapment of the left ureter, in whom the concurrent presence of a neoplasm in the right ovary was found, which proved to be a benign Brenner tumor.
Case Report
A 52-year-old multiparous woman presented to our Outpatient Clinic complaining of persistent abdominal pain of 10 days' duration. Two years earlier, she had undergone sigmoidectomy for the management of a colorectal adenocarcinoma and had received adjuvant chemotherapy postoperatively.
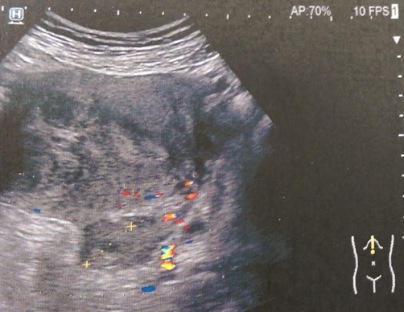
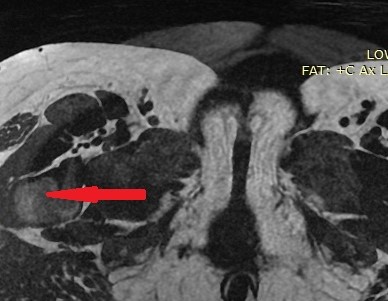
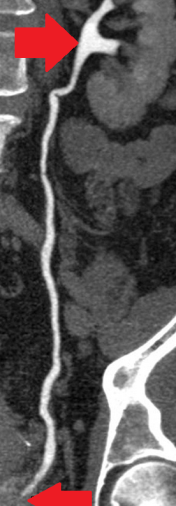
Since then, she had been under close follow-up by her treating oncologist, diligently completing the required clinical and imaging examinations. With the onset of pain in the lower abdomen, she sought immediate medical attention and was investigated with abdominal ultrasound and CT/MRI of the lower abdomen.Both examinations revealed the presence of a neoplasm arising from the right ovary, a simple cyst of the left ovary, and moderate dilation of the left ureter due to external compression at its lower third, most likely due to recurrence of the primary disease and/or the presence of a toumor seeding in the left iliac fossa.

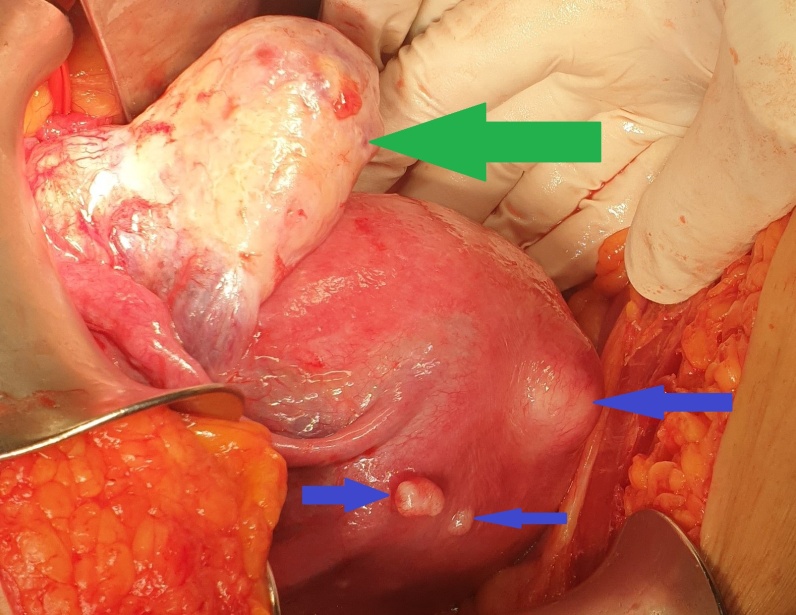
On clinical examination, the patient had stable vital signs, mild tenderness in the lower abdomen, particularly on the right, where there was a palpable, mobile mass measuring approximately 16 × 8.5 cm. Staging of the primary disease was negative for the presence of distant metastases.Based on the above findings, we proceeded with an exploratory laparotomy. Upon entering the abdomen, we identified the presence of a multilobulated solid tumor in the right ovary and a simple cyst in the left ovary. Additionally, we found significant dilation of the left ureter as a consequence of external pressure from a seed at the level of the bifurcation of the left common iliac artery.Finally, we confirmed the presence of multiple uterine fibroids, while both fallopian tubes were normal.
We initially performed peritoneal lavage and sent the material for cytological examination. In a preoperative discussion with the patient, she expressed a negative attitude toward the idea of performing a total hysterectomy with bilateral salpingo-oophorectomy, so we proceeded with a right salpingo-oophorectomy and sent the specimen for frozen section biopsy, which revealed the presence of a benign Brenner neoplasm.
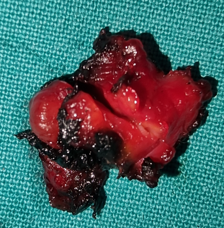
Subsequently, we removed the implant adjacent to the left ureter, resulting in its complete liberation.
Despite thorough examination, we found no other focus of disease in the peritoneal cavity, so we removed the simple cyst of the left ovary and enucleated two subserosal uterine fibroids.
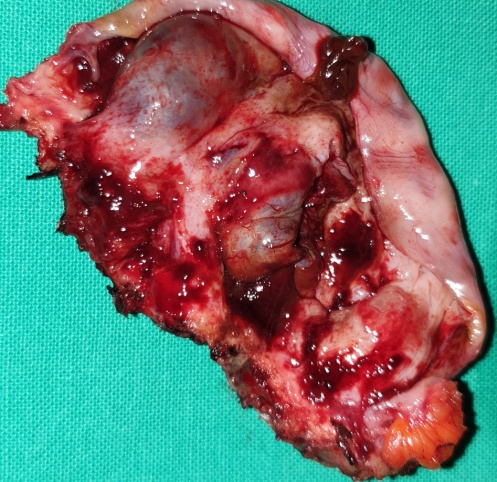

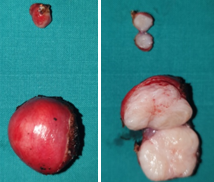

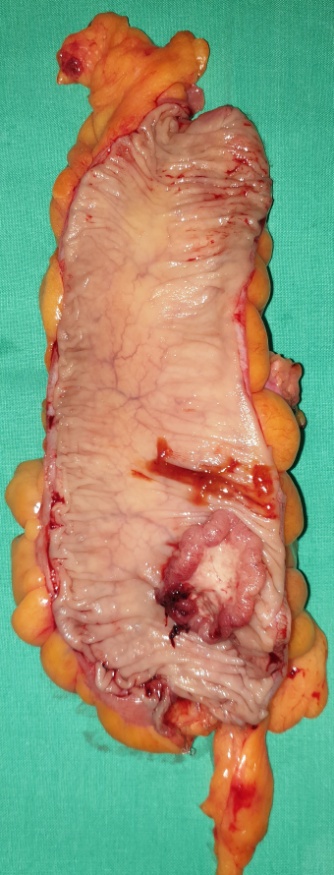
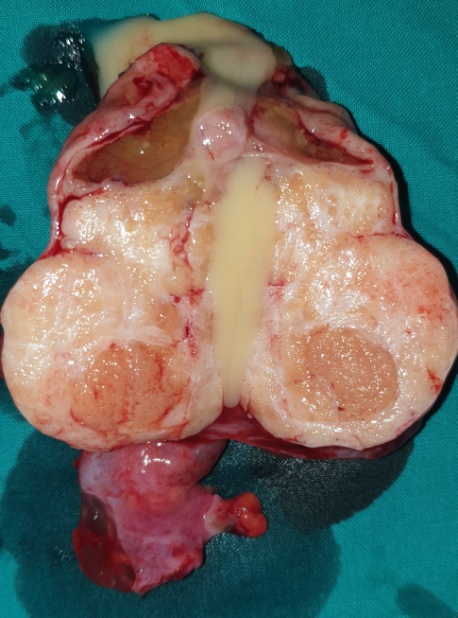
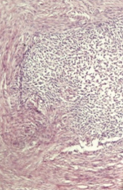
Macroscopically, the neoplasm was multilobulated, with white, shiny, nodular surfaces. On cross-section, well-circumscribed whitish nodules were revealed, surrounded by fibromatous tissue. Histopathological examination revealed the presence of well-circumscribed epithelial cell nests with clearly defined borders, surrounded by abundant fibromatous stroma. The epithelial cells were ovoid or polygonal, with pale cytoplasm and ovoid nuclei.All the above findings were indicative of a benign Brenner neoplasm in the right ovary. The removed seed revealed the presence of an adenocarcinoma of the same histological appearance as the primary sigmoid neoplasm. Finally, the removed left ovarian cyst and uterine fibroids were consistent with a benign simple cyst and benign fibroids, respectively.Cytological examination was negative.
The patient's postoperative course was uneventful, and she was discharged from the hospital 6 days later.15 days later, we performed an intravenous pyelography, which demonstrated complete liberation of the left ureter, and therefore we referred the patient for oncological evaluation and treatment.
Discussion
Brenner tumor of the ovary constitutes a solid ovarian tumor that is usually asymptomatic. Although predominantly solid on imaging and pathological examination, their association with serous and mucinous cystadenomas reaches 30%.They are usually an incidental finding. Among symptomatic patients, the most common symptoms are vaginal bleeding, palpation of a pelvic mass, and pelvic pain. In most cases, they are unilateral, with only 5-7% of cases showing bilateral development.It is generally accepted that Brenner neoplasms originate from the surface epithelium of the ovaries or from the pelvic mesothelium, following metaplasia into transitional cells, resulting in the creation of typical urothelium-like structural elements.The histological patterns encountered in Brenner tumors are benign, with very few reports of borderline or malignant cases.
Unfortunately, diagnosis is difficult with imaging studies (ultrasound, CT, or MRI), as they lack specificity due to the non-specific characteristics of the neoplasm, with images resembling those of fibromas, fibrothecomas, and pedunculated leiomyomas.
Grossly, benign Brenner tumors are well-circumscribed with a hard or fibromatous, gray-white or slightly yellow cut surface. Occasionally, they acquire a rough consistency due to calcium deposition. Borderline Brenner tumors are characteristically cystic and unilocular or multilocular, with papillary cauliflower-like masses projecting into one or more lobes.Malignant Brenner tumors are solid or cystic, with mural nodules, without distinctive features.
Microscopically, Brenner tumors consist of abundant dense fibrous stroma with epithelial nests of transitional cells resembling cells lining the urinary bladder.The fibrous elements are less prominent in borderline or malignant Brenner tumors.
Most Brenner tumors are candidates for surgical excision. Due to their markedly circumscribed nature, they are easily identified and do not invade adjacent tissues.Surgical excision offers cure and eliminates any existing symptoms. Malignant Brenner tumors invade adjacent tissues and metastasize to other anatomical structures, but they are so rare that no management guidelines have been formulated.Even these, however, if detected early, are primarily managed with surgical excision.
The WHO has classified Brenner tumors into three categories: 1) benign, 2) borderline (atypically proliferating), and 3) malignant. Benign tumors are the most common, representing 95% of cases; borderline tumors represent 5%, and malignant tumors less than 1%.They constitute neoplasms originating from the surface epithelium of the ovaries, and their microscopic features resemble those of the extrarenal urinary tract lined by urothelium. Borderline Brenner tumors are epithelial tumors appearing as cellular islands or irregular epithelial masses projecting into cystic areas, differentiated from the dense connective tissue at the periphery.They constitute neoplasms originating from the surface epithelium of the ovaries, and their microscopic features resemble those of the extrarenal urinary tract lined by urothelium. Borderline Brenner tumors are epithelial tumors appearing as cellular islands or irregular epithelial masses projecting into cystic areas, differentiated from the dense connective tissue at the periphery.Finally, malignant Brenner tumors are characterized by cellular atypia and stromal invasion.
Both borderline and malignant Brenner tumors may coexist with benign Brenner tumors, leading many researchers to support the view that both borderline and malignant tumors develop from benign Brenner tumors.
According to some authors, 25-36% of cases coexist with other neoplasms, such as mucinous cystic tumors, serous cystic adenomas, or even cystic dermoid teratomas. The presence of other neoplastic or non-neoplastic lesions in the female genital tract is attributable to the fact that Brenner tumors contain cells with secretory functions that produce estrogens, hormones responsible for the development of various lesions due to endometrial hyperplasia, causing vaginal bleeding or the development of ovarian neoplasms.
Brenner tumors occur both premenopausally and postmenopausally, with a mean age at diagnosis ranging between 46 and 63 years. Specifically, benign tumors develop in women aged 30 to 59 years, while borderline and malignant tumors occur in older women, between 45 and 60 years.Most borderline tumors, if diagnosed early, have a favorable prognosis following surgical excision, with 5-year survival rates of 99% and 10-year survival rates of 97%. Very rarely, cases of disease recurrence have been reported.Even borderline tumors, if left untreated, may cause local complications due to adhesion to adjacent tissues.
Conclusions
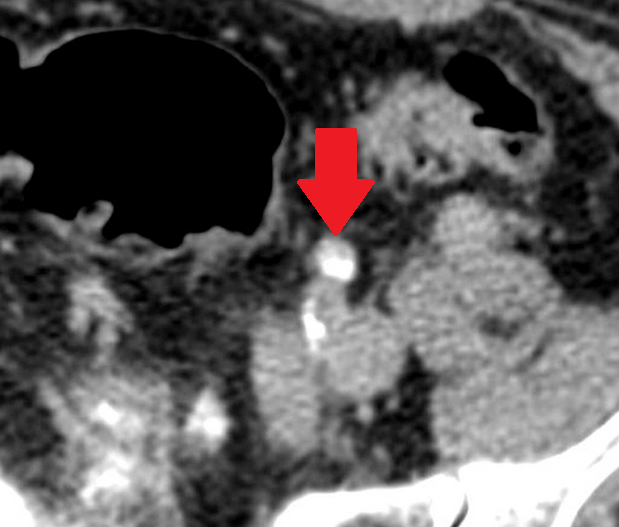
Brenner tumors are rare ovarian surface epithelial neoplasms, accounting for 1.4-2.5% of ovarian tumors, with a predilection for postmenopausal women. Most are asymptomatic and discovered incidentally. The solid nature of the mass with calcifications in a postmenopausal woman raises suspicion for Brenner's tumor, though the definitive diagnosis required histopathological confirmation.
- Brenner tumors constitute 1.5-2.5% of ovarian tumors and are predominantly benign
- They typically present as incidental findings in postmenopausal women with non-specific symptoms
- Imaging characteristically shows a solid mass with calcifications
- Histological hallmark is transitional epithelial nests with coffee-bean nuclear grooves in fibrous stroma
- Surgical excision is curative for benign Brenner tumors; accurate classification is essential to distinguish from malignant variants
Sign in to join the discussion
Loading...