Rare Syndromes & Systemic
Σπάνια Σύνδρομα & Συστηματικά
123 images

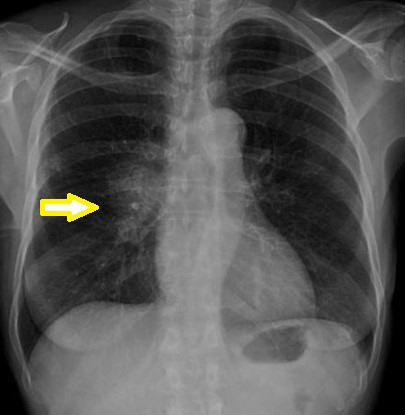




YELLOW NAIL SYNDROME - BILATERAL PLEURAL EFFUSIONS . (Courtesy Dr . V . Penopoulos).
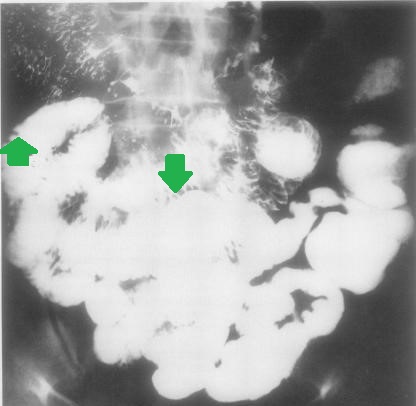
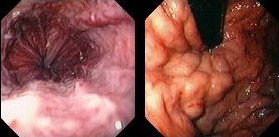
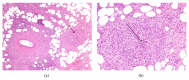
YELLOW NAIL SYNDROME - INTESTINAL LYMPHANGIECTASIA . (Courtesy Dr . V . Penopoulos).




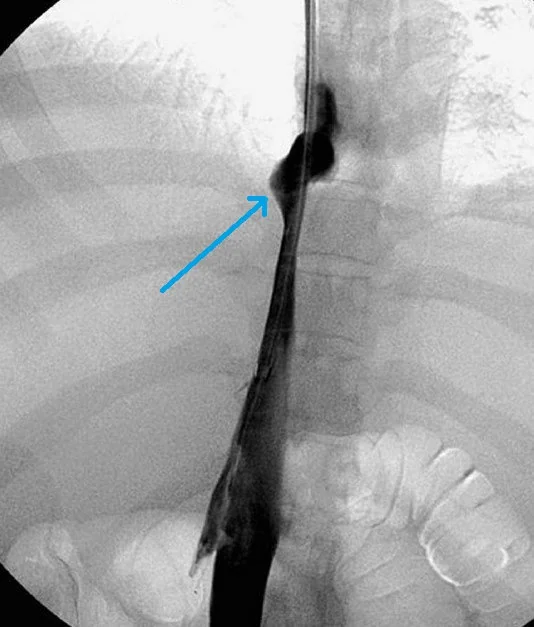
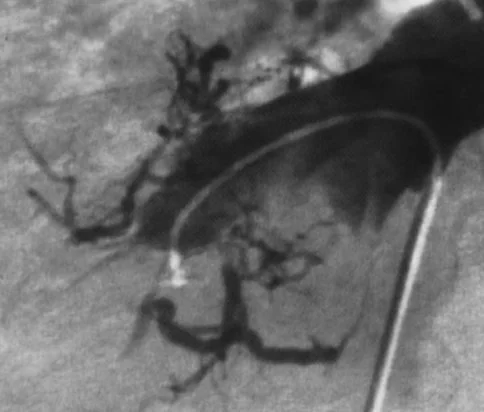
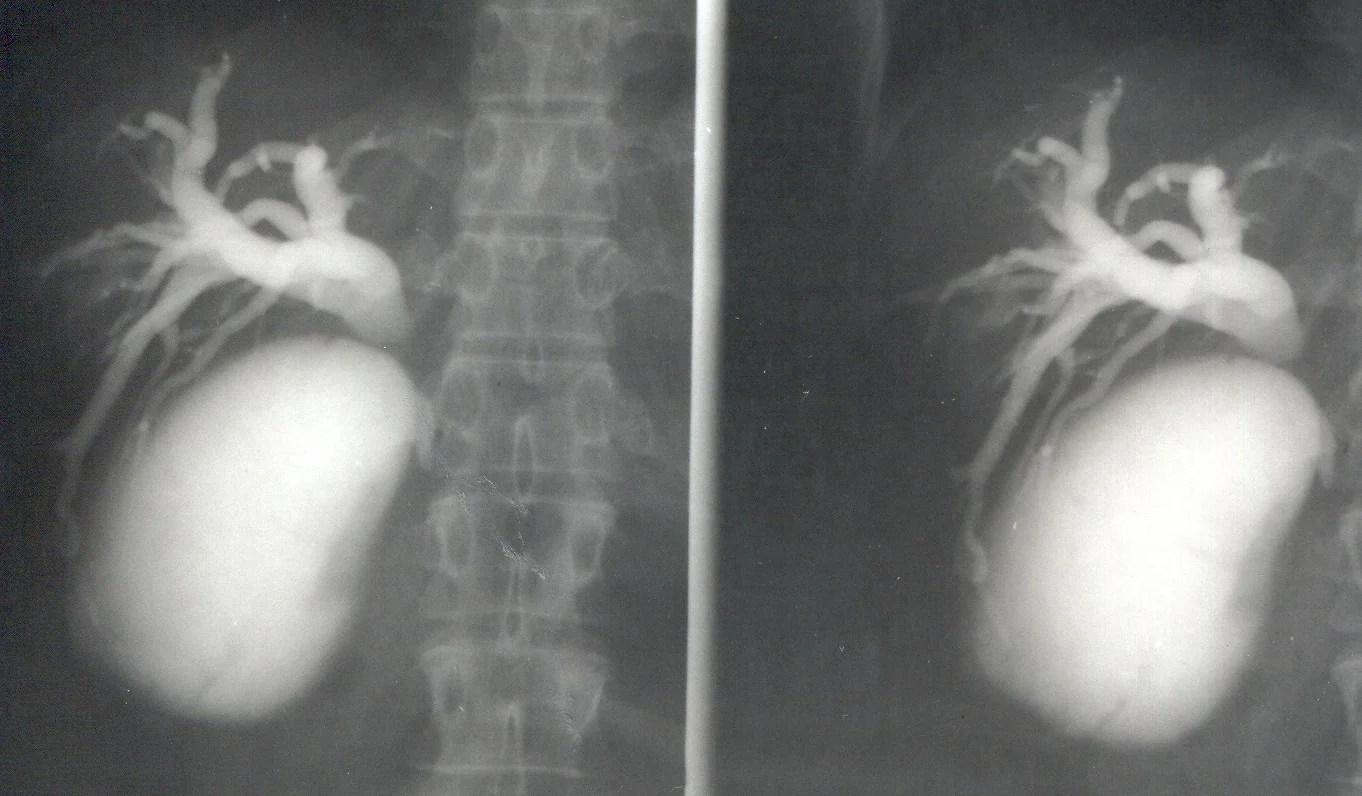
PELVIC CONGESTION SYNDROME - OVARIAN PHLEBOGRAPHY . (Courtesy Dr . V . Penopoulos).

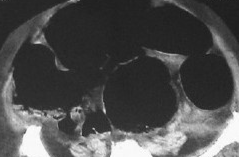






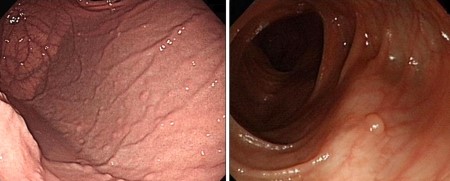



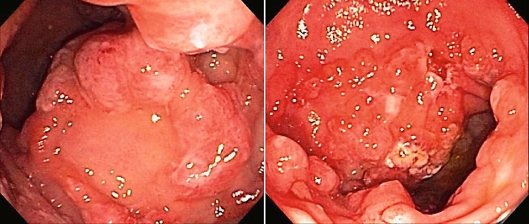
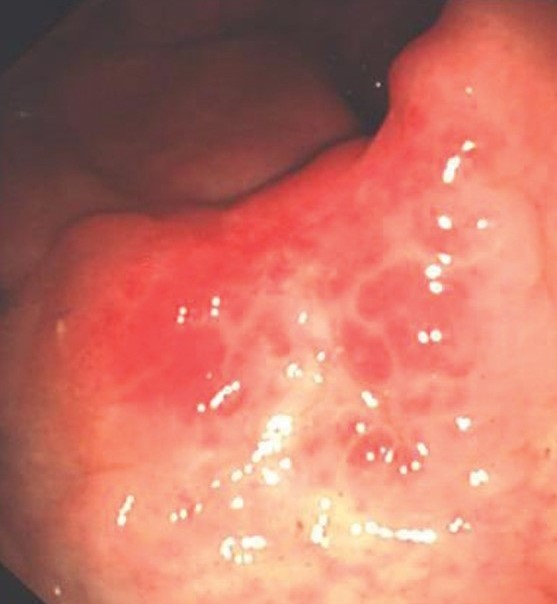
COWDEN SYNDROME - MULTIPLE GASTRIC POLYPOSIS . (Courtesy Dr . V . Penopoulos).
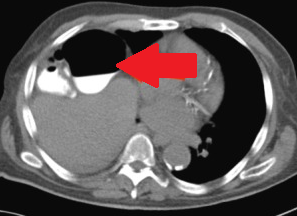






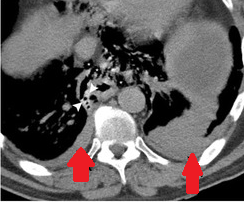
Boerhaave Syndrome . Chest CT scan. Bilateral pleural effusions, more prominent on the left (Courtesy Dr. V. Penopoulos)
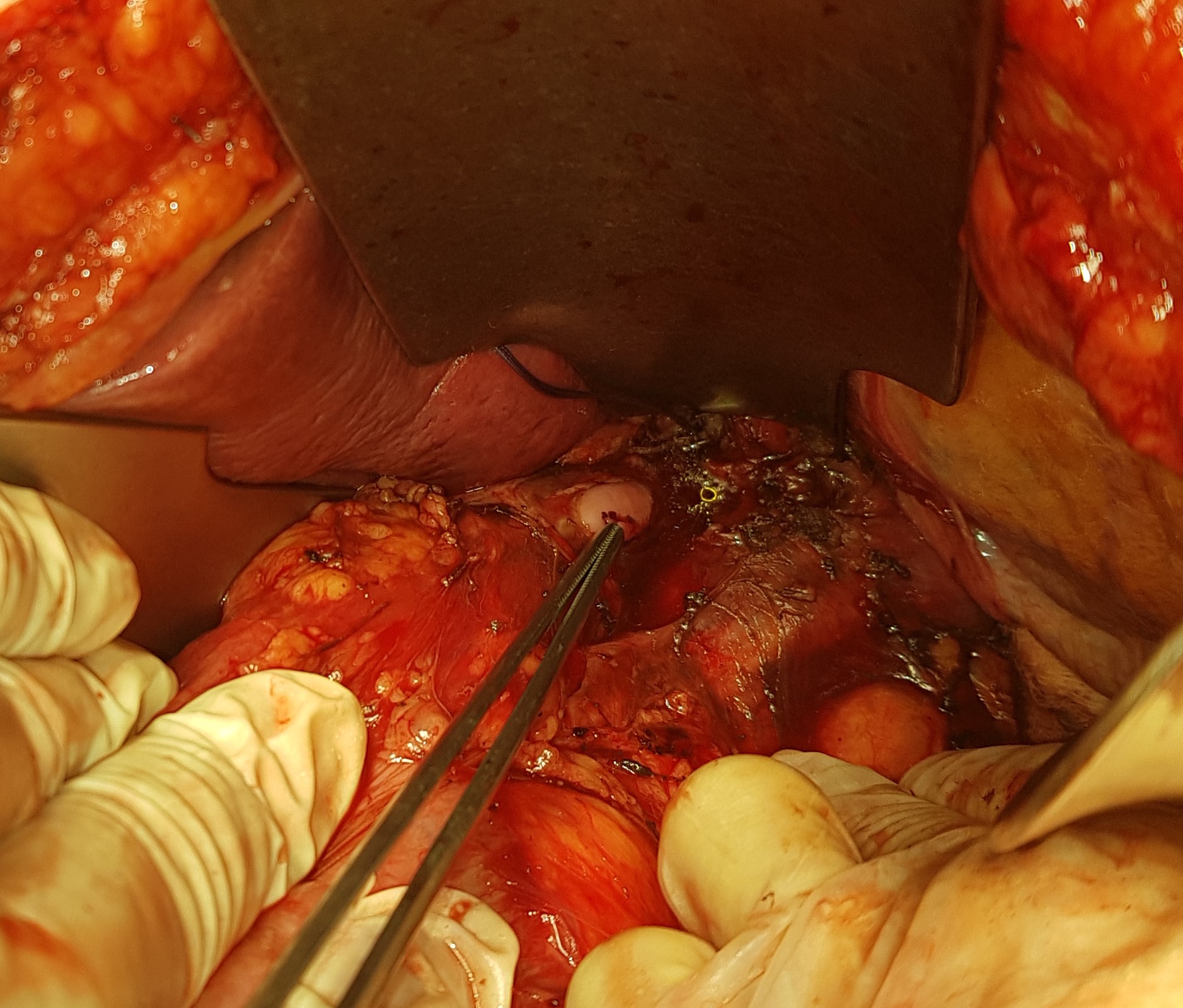
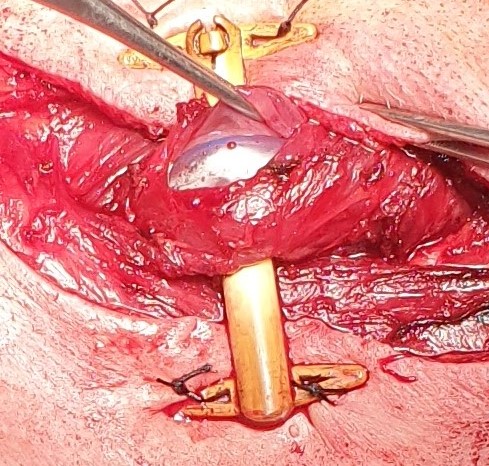
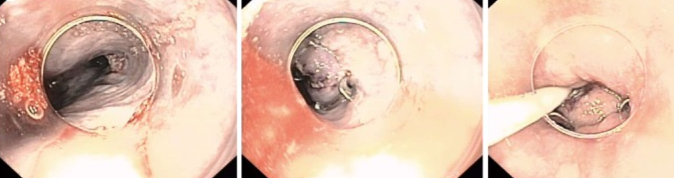
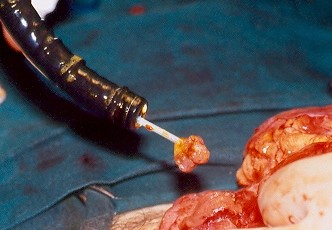
Boerhaave Syndrome . Forceps at the site of lower esophageal perforation (Courtesy Dr. V. Penopoulos)

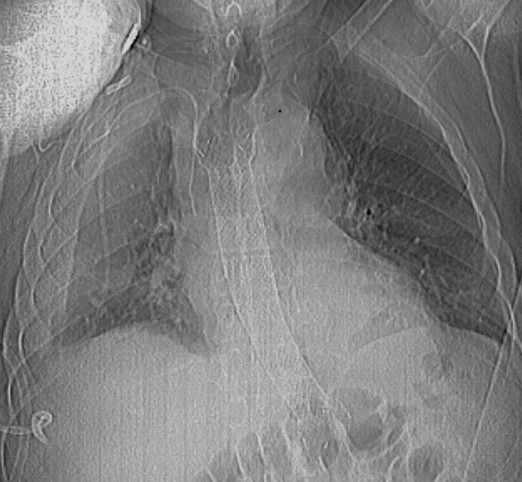

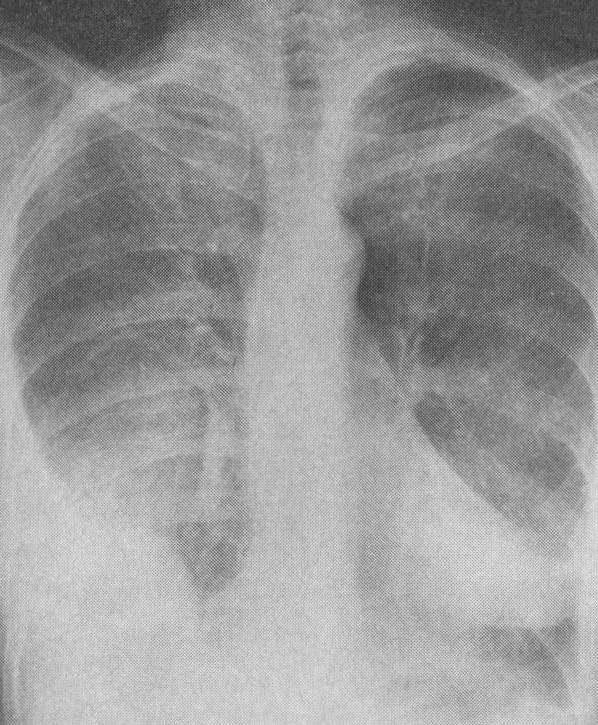
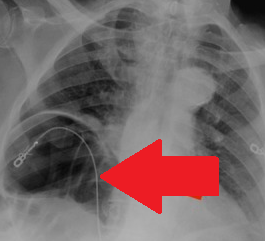
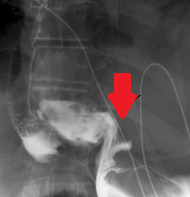
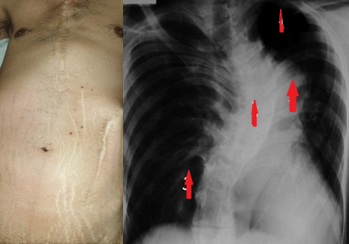
Boerhaave Syndrome. Plain Chest X-Ray.Presence of free air in the mediastinum.(Courtesy Dr.V.Penopoulos).

Boerhaave Syndrome . Upper gastrointestinal endoscopy. Esophageal perforation (Courtesy Dr. V. Penopoulos)
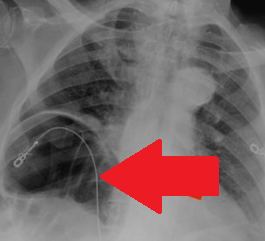
Chilaiditi Syndrome . Chest X-Ray.The interposition of the right hepatic flexure between the liver and the right hemidiaphragm is obvious.(Courtesy Dr.V.Penopoulos).
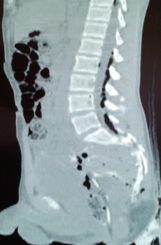
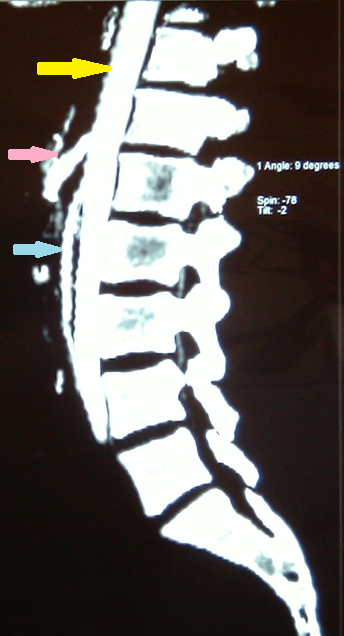
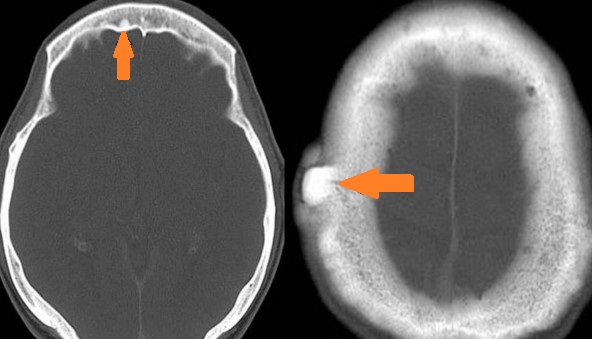
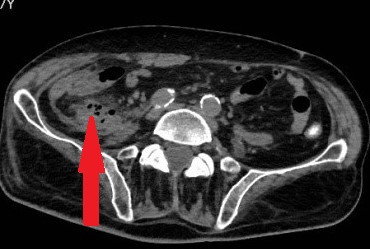
MRI of the lumbosacral spine. Air is clearly visible within the spinal canal (Courtesy Dr. V. Penopoulos)

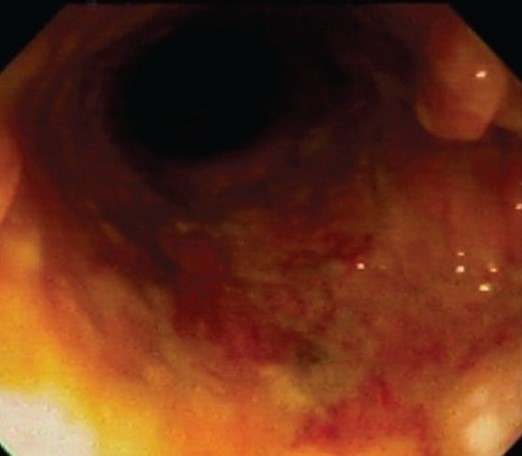
Rectal injury sustained when the patient fell onto a sharp object.(Courtesy Dr. V. Penopoulos).
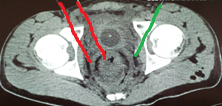
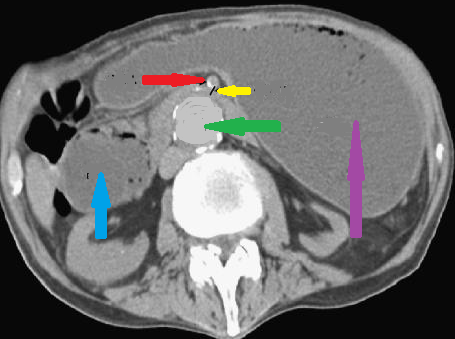
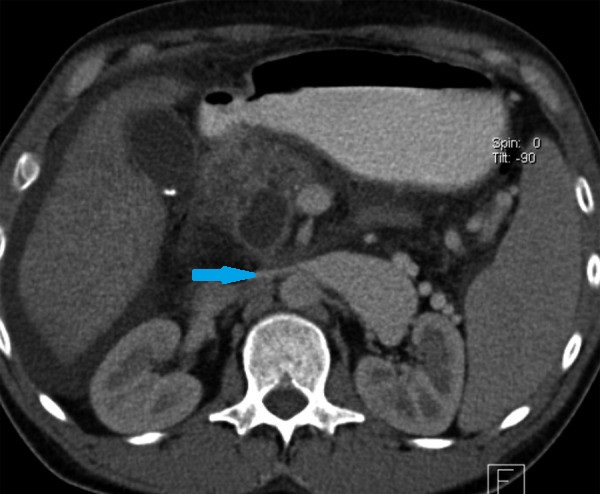
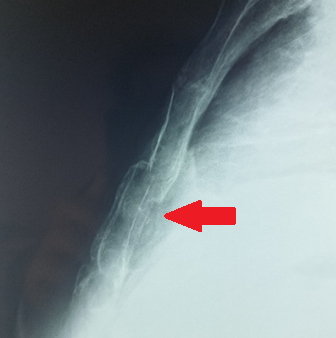
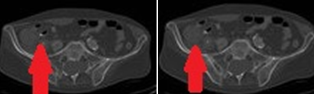
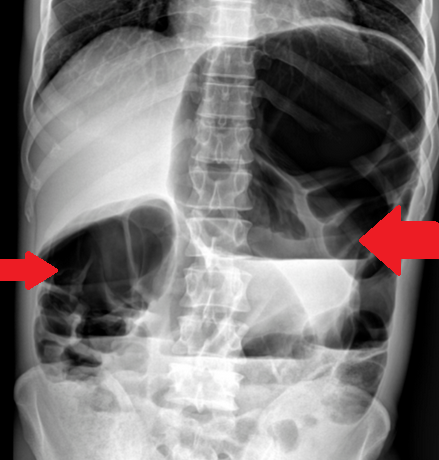
Rectal Injury . Red arrows. Thickened rectal wall. Green arrow. Fascia of the levator ani muscle (Courtesy Dr. V. Penopoulos)


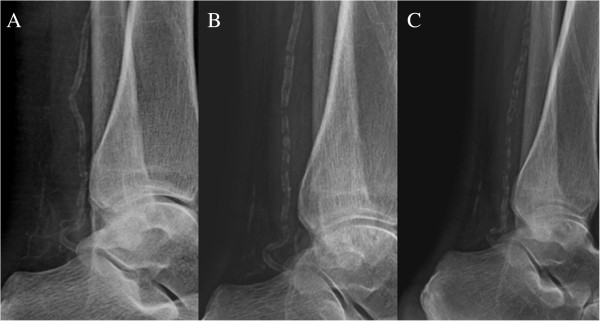
Plain radiographs of lower legs, knees and ankles. Substantial calcifications were visible in the posterior tibial artery and a network of small vessels in the retromalleolar region. In the knees, the joint space exhibited obvious small vessel calcification. (Courtesy Dr. V. Penopoulos).

Plain radiographs of lower legs, knees and ankles. Substantial calcifications were visible in the posterior tibial artery and a network of small vessels in the retromalleolar region. In the knees, the joint space exhibited obvious small vessel calcification. (Courtesy Dr. V. Penopoulos).
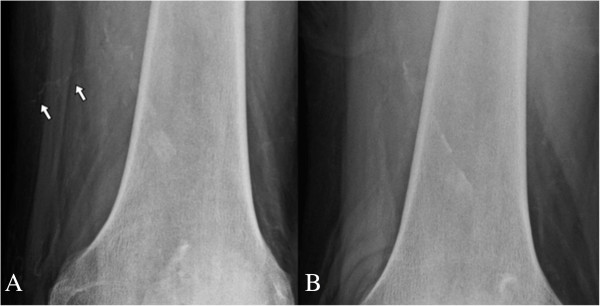
Plain radiographs of lower legs, knees and ankles. Substantial calcifications were visible in the posterior tibial artery and a network of small vessels in the retromalleolar region. In the knees, the joint space exhibited obvious small vessel calcification. (Courtesy Dr. V. Penopoulos).




Multiple Myeloma . Bone scintigraphy – Presence of multiple osteolytic foci (Courtesy Dr. V. Penopoulos)


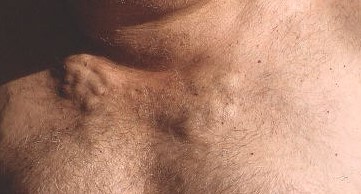
Typical Holt Oram syndrome’s hands malformations . ( Courtesy Dr . V . Penopoulos ) .
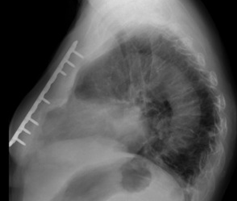

Figure 1 . Typical Holt Oram syndrome’s hands malformations . ( Courtesy Dr . V . Penopoulos ) .
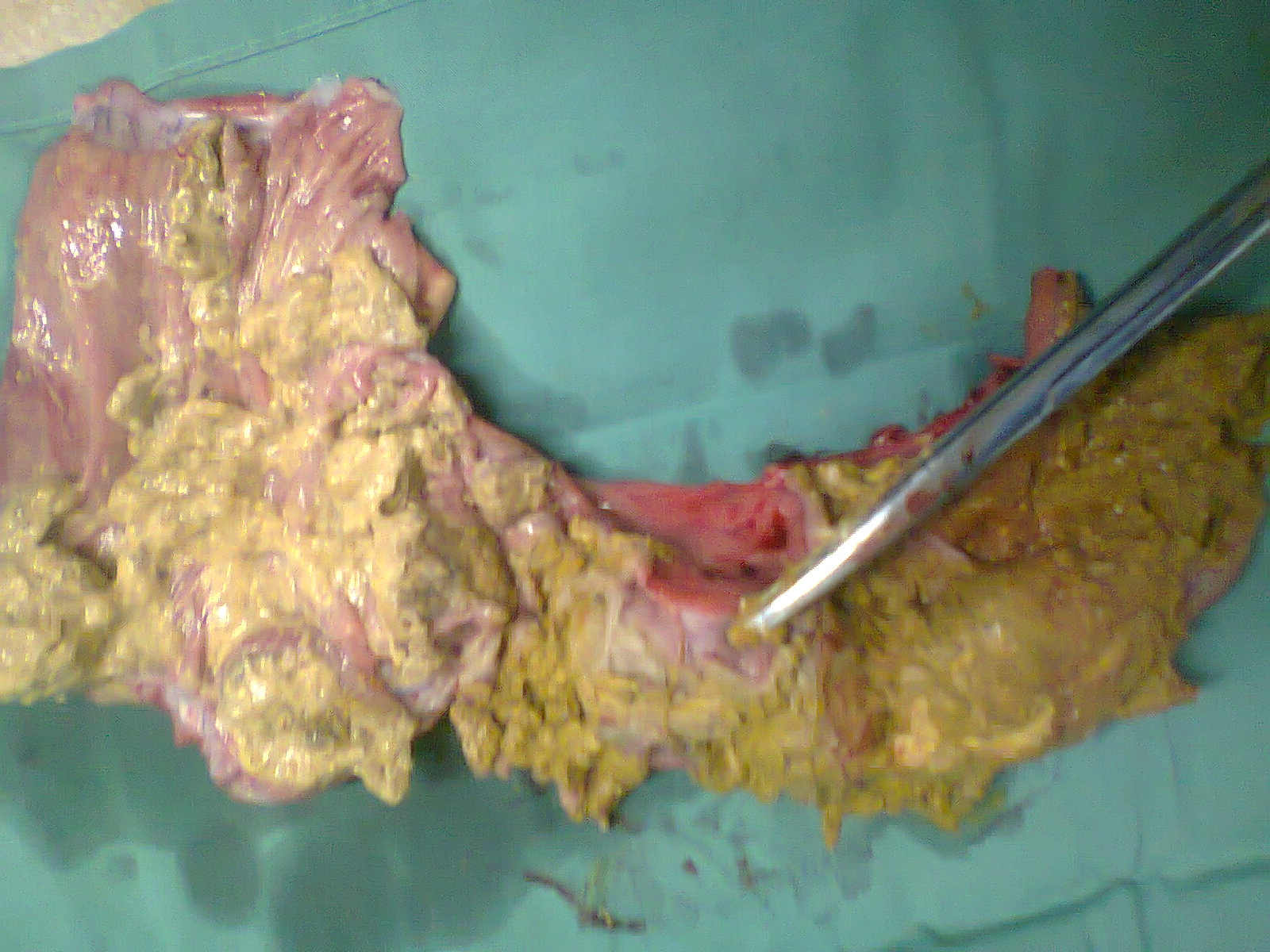
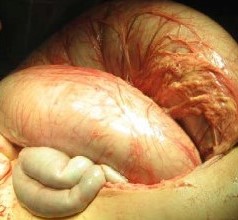
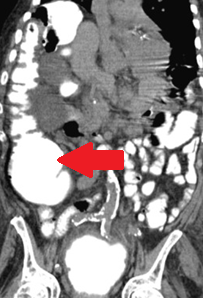
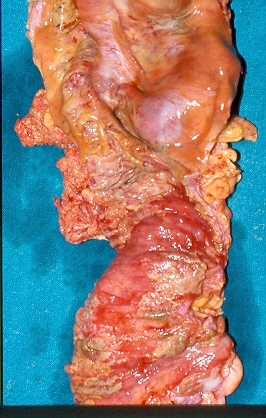
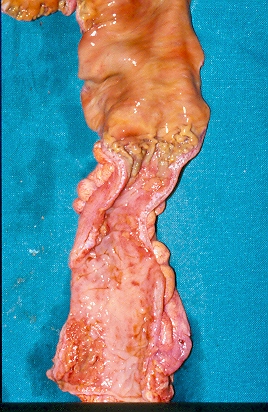
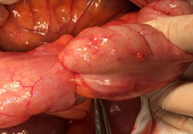
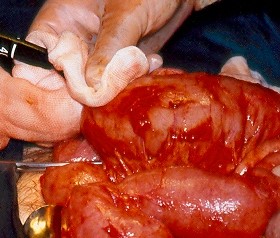
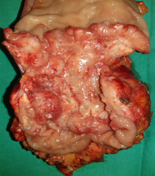
DIOS .Right Hemicolectomy specimen . The impacted mucofeculent material in the terminal ileum is clearly seen (Courtesy Dr. V. Penopoulos)

Right Hemicolectomy specimen . The impacted mucofeculent material in the terminal ileum is clearly seen (Courtesy Dr. V. Penopoulos)
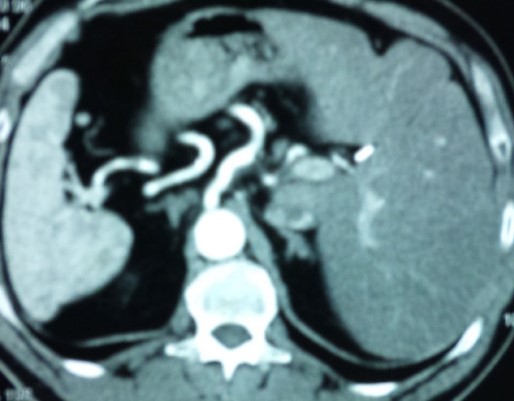
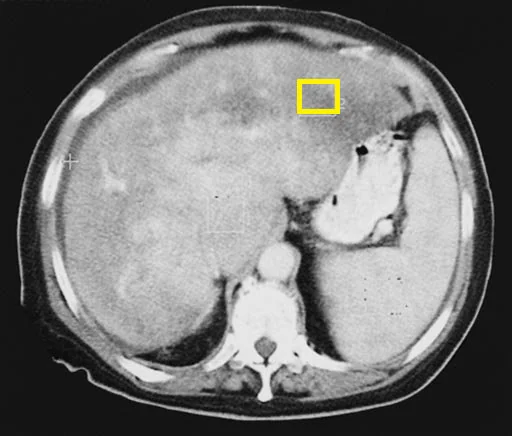
Marfan's Syndrome . Abdominal CT Scan . Abscess formation . ( Courtesy Dr . V . Penopoulos ) .

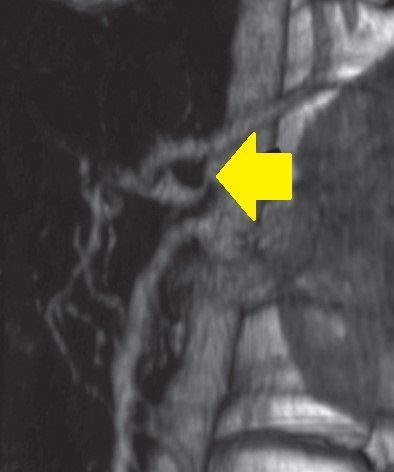
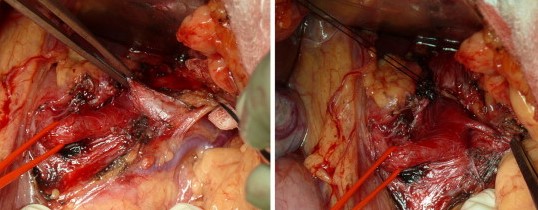
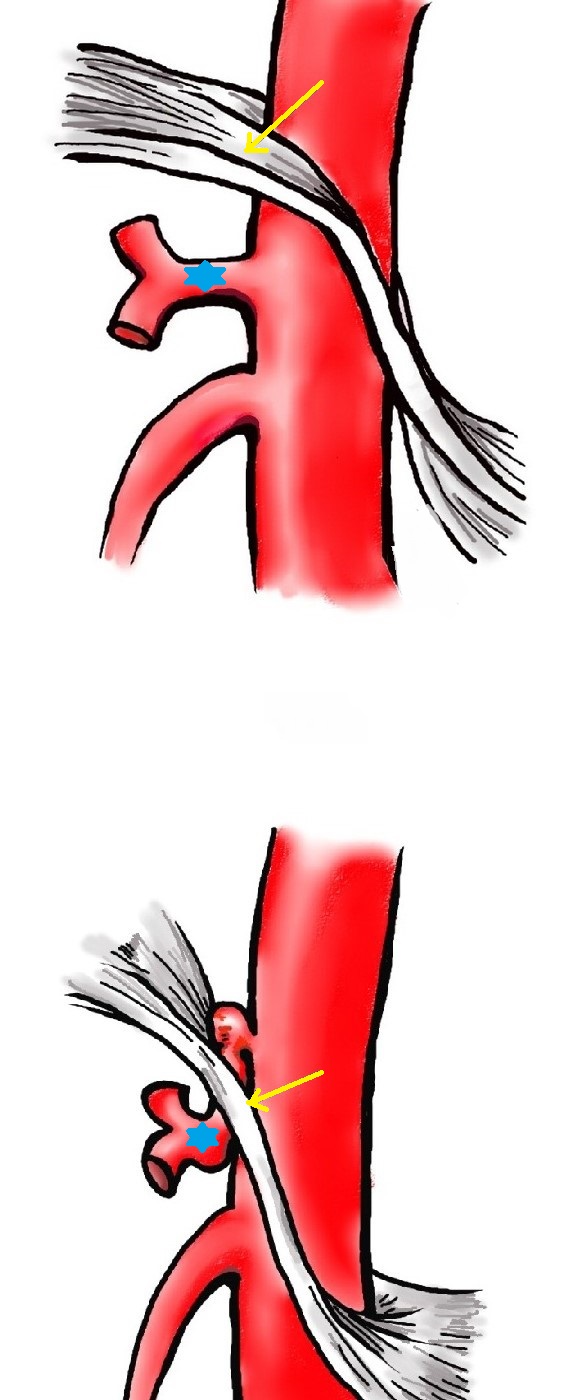
Marfan's Syndrome . Intercostal artery reconstruction protecting the spinal cord in patients undergoing extensive thoracoabdominal aortic aneurysm repair or aortic dissection . ( thoraco-abdominal incision ) .( Courtesy Dr . V . Penopoulos ) .
Marfan's syndrome . Pectus excavatum , striae atrophicae and prominent scoliosis . (Courtesy Dr . V . Penopoulos) .

Marfan's syndrome . Patient’s abnormally long and slender fingers (arachnodactyly).(Courtesy Dr.V.Penopoulos).

Marfan's Syndrome . Severe pes planus (talipes calcaneovalgus) .( Courtesy Dr . V . Penopoulos ) .
Marfan's Syndrome . Abdominal CT Scan . Acute Appendicitis .( Courtesy Dr . V . Penopoulos ) .


Compartment Syndrome . Fasciotomy of the left lower extremity (Courtesy Dr. V. Penopoulos)


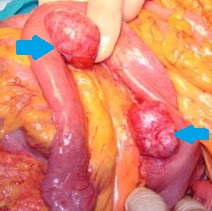
Peutz-Jeghers Syndrome . Removed polyps, endoscopically and surgically (Courtesy Dr. V. Penopoulos)
Peutz-Jeghers Syndrome . Removed polyps, endoscopically and surgically (Courtesy Dr. V. Penopoulos)
Peutz-Jeghers Syndrome . Removed polyps, endoscopically and surgically (Courtesy Dr. V. Penopoulos)
Peutz-Jeghers Syndrome . Removed polyps, endoscopically and surgically (Courtesy Dr. V. Penopoulos)
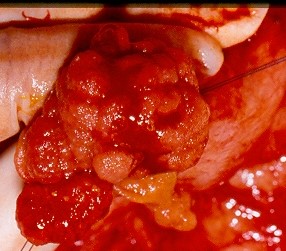
Peutz-Jeghers Syndrome . Malignantly transformed ileal polyp (Courtesy Dr. V. Penopoulos)
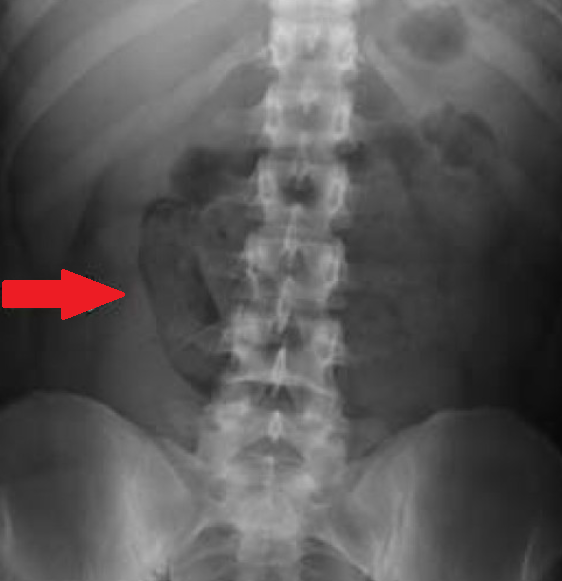
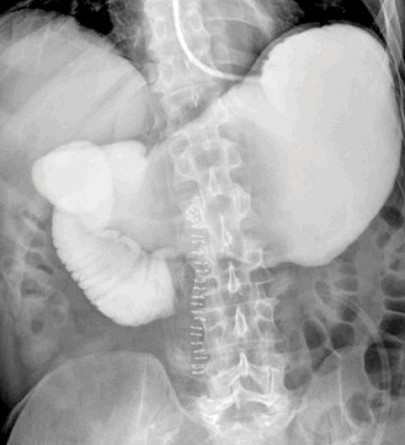
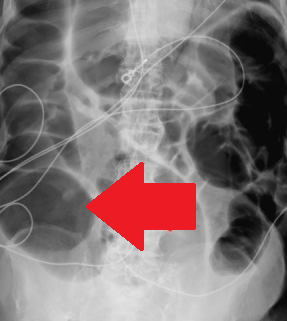
Peutz-Jeghers Syndrome . Plain abdominal X-Rays.Small bowel air-fluid levels.Intussusception.(Courtesy Dr.V.Penopoulos).
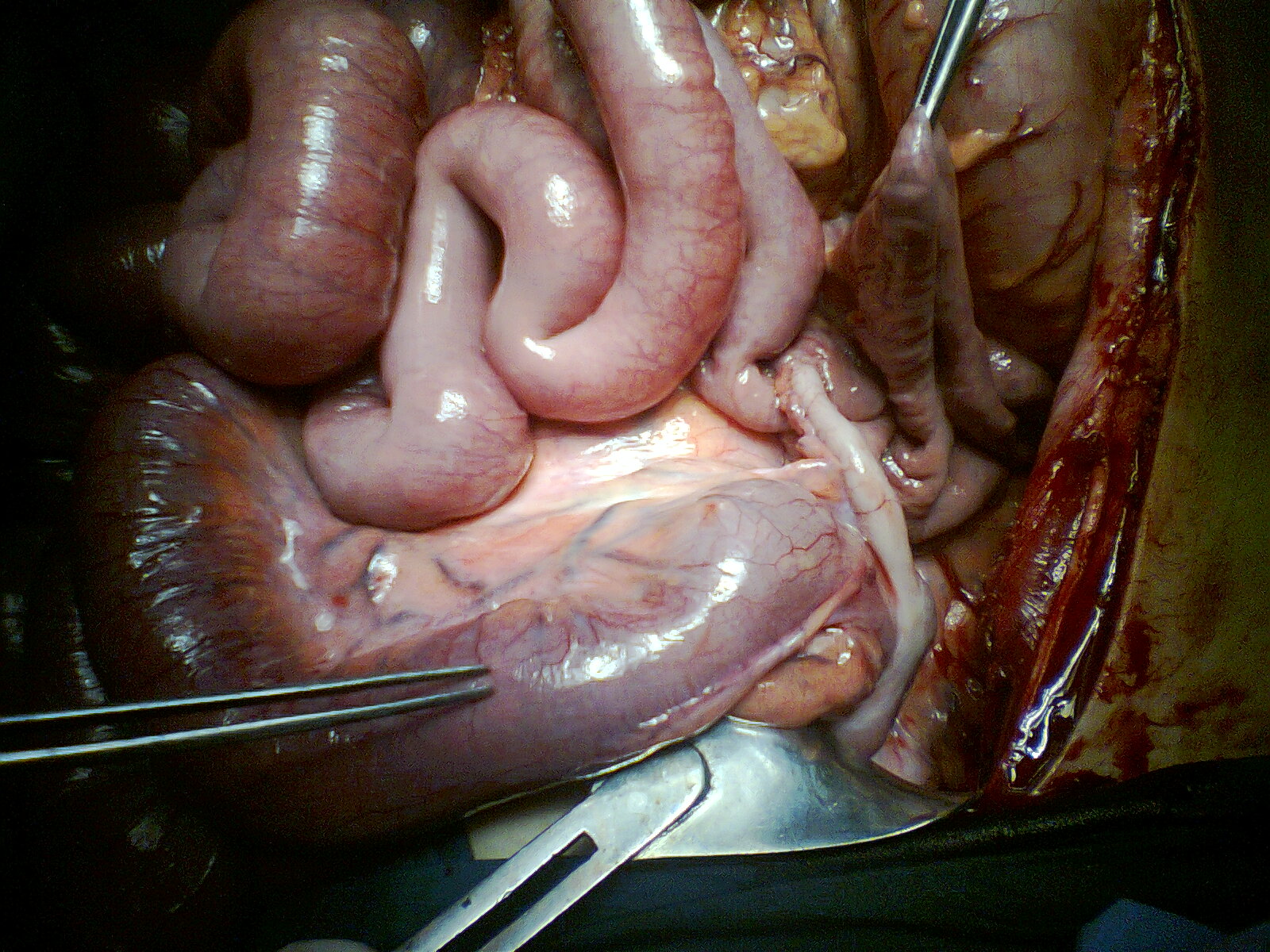
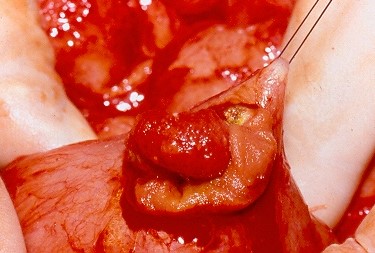
Peutz-Jeghers Syndrome . Benign polyp – lead point of intussusception (Courtesy Dr. V. Penopoulos)
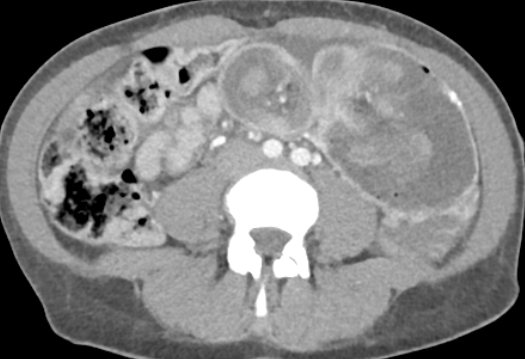
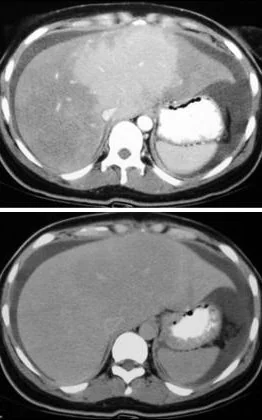
Peutz-Jeghers Syndrome . Abdominal CT Scan.Small bowel intussusception.(Courtesy Dr.V.Penopoulos).
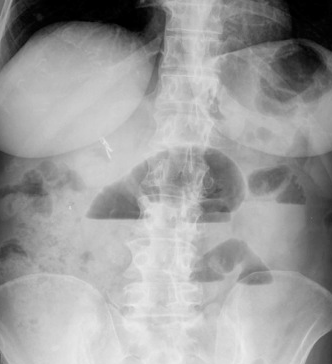
Peutz-Jeghers Syndrome . Plain abdominal X-Rays.Small bowel air-fluid levels.Intussusception.(Courtesy Dr.V.Penopoulos).

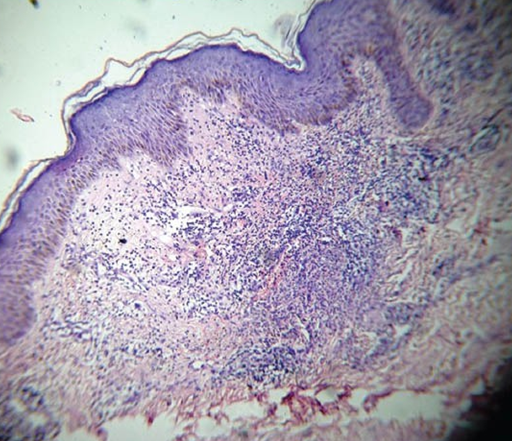
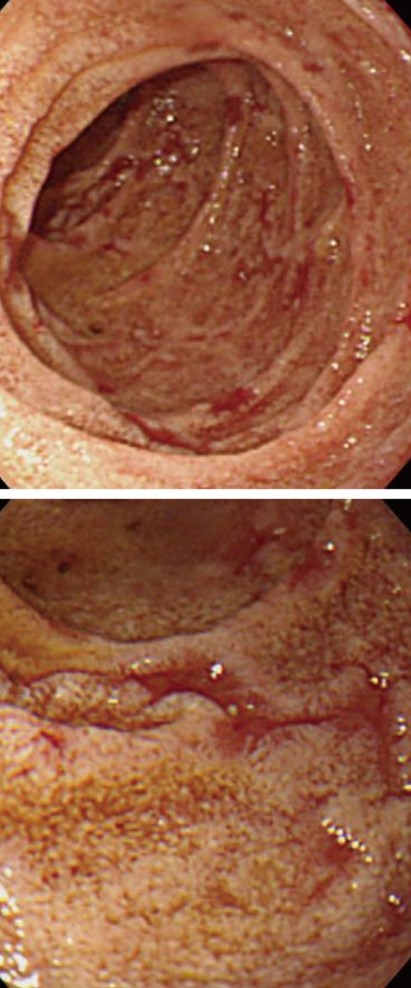
Sweet syndrome . Rectosigmoid adenocarcinoma .Large bowel obstruction . (Courtesy Dr.V.Penopoulos).

Sweet syndrome . Rectosigmoid adenocarcinoma .Large bowel obstruction . (Courtesy Dr.V.Penopoulos).