Skin & Soft Tissue
Δέρμα & Μαλακά Μόρια
323 images


















































































































































































































































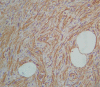
Immunohistochemical staining, strongly positive for vimentin (Courtesy Dr. V. Penopoulos)

Immunohistochemical staining, strongly positive for smooth muscle actin (Courtesy Dr. V. Penopoulos)

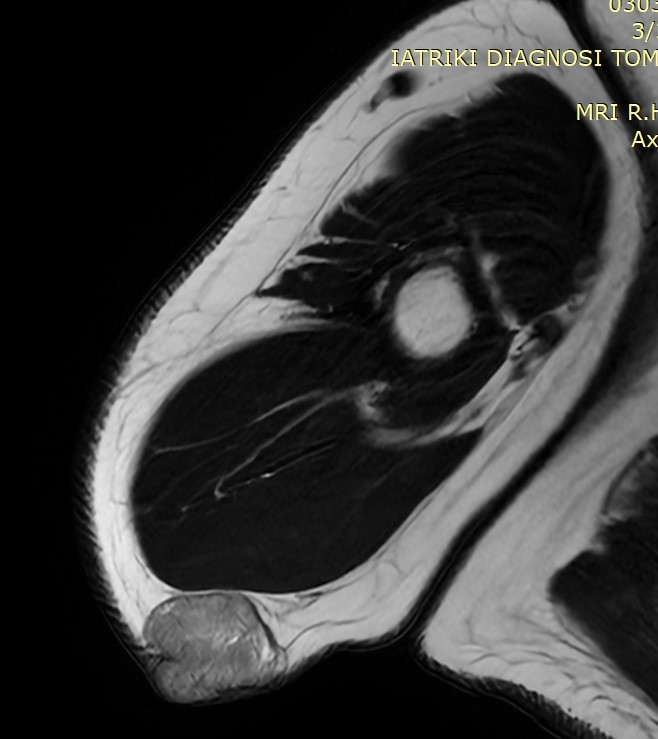
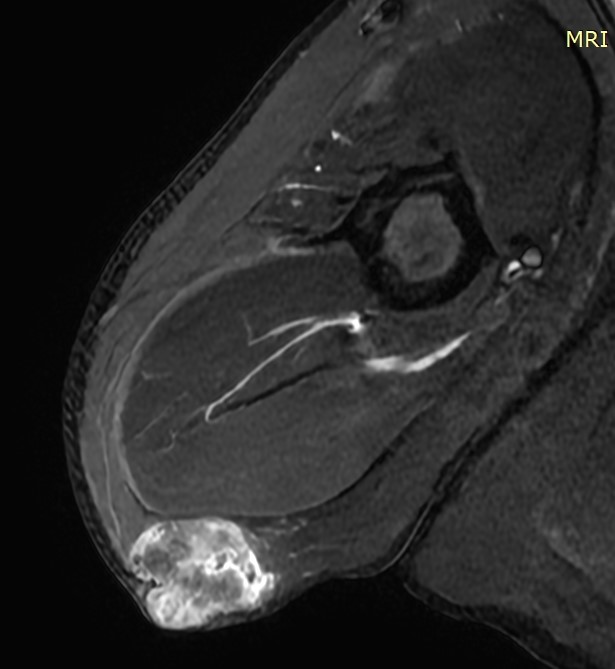
MRI Left shoulder.The subcutaneous "mass" is evident.(Courtesy Dr.V.Penopoulos).


Pyoderma gangrenosum lower limps in ulcerative colitis patients without stomas.(Courtesy Dr.V.Penopoulos).



Pyoderma gangrenosum lower limps in ulcerative colitis patient without stoma.(Courtesy Dr.V.Penopoulos).








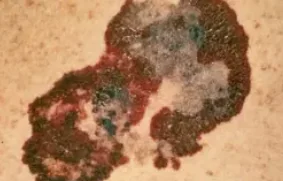
Non ulcerated Kaposi's Sarcoma lesions on the plantar aspect of the right foot (Courtesy Dr. V. Penopoulos)


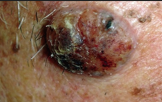
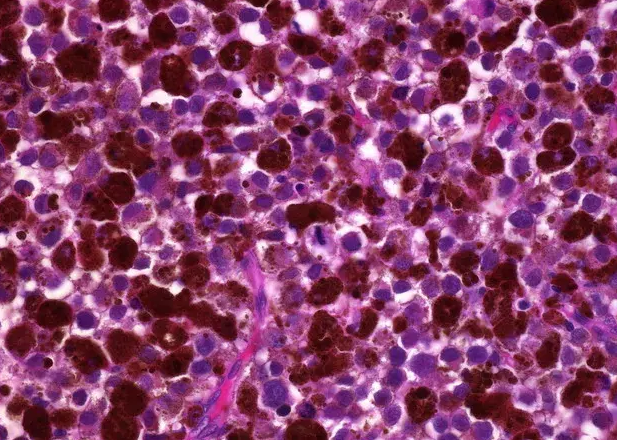
Pathological examination of the skin lesion.Hematoxylin-eosin staining showed nests of monomorphic tumor cells with big, atypia, deep stained nucleus, and active mitotic figures but no obvious melanin . (Courtesy Dr. V. Penopoulos)

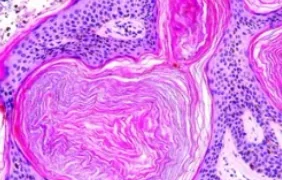
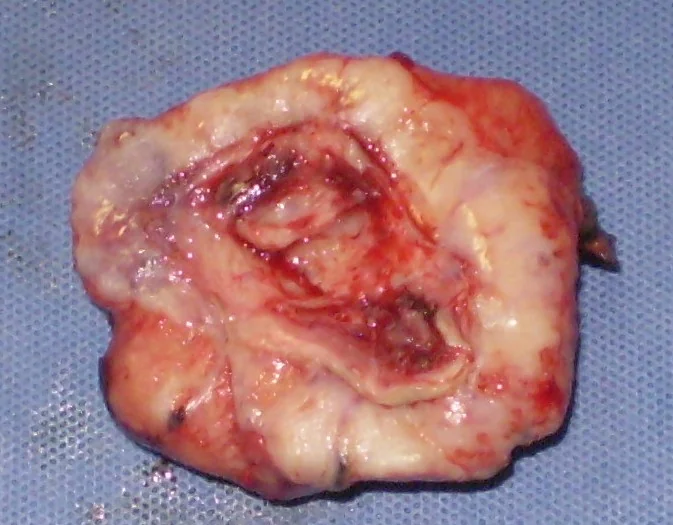
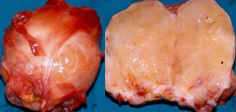
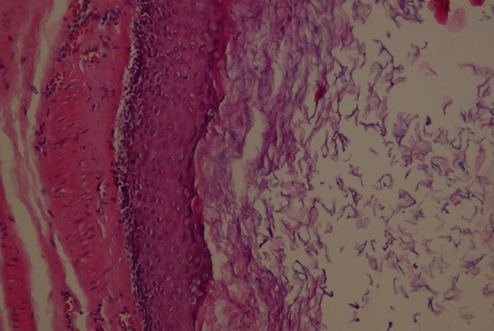
Gross image of excised cystic tumor.Epidermoid cyst. (Courtesy Dr. V. Penopoulos)

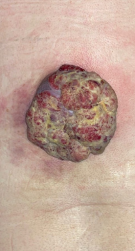
Macroscopic view of the left shoulder.Amelanotic melanoma.( Courtesy Dr . V . Penopoulos ).
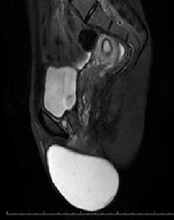
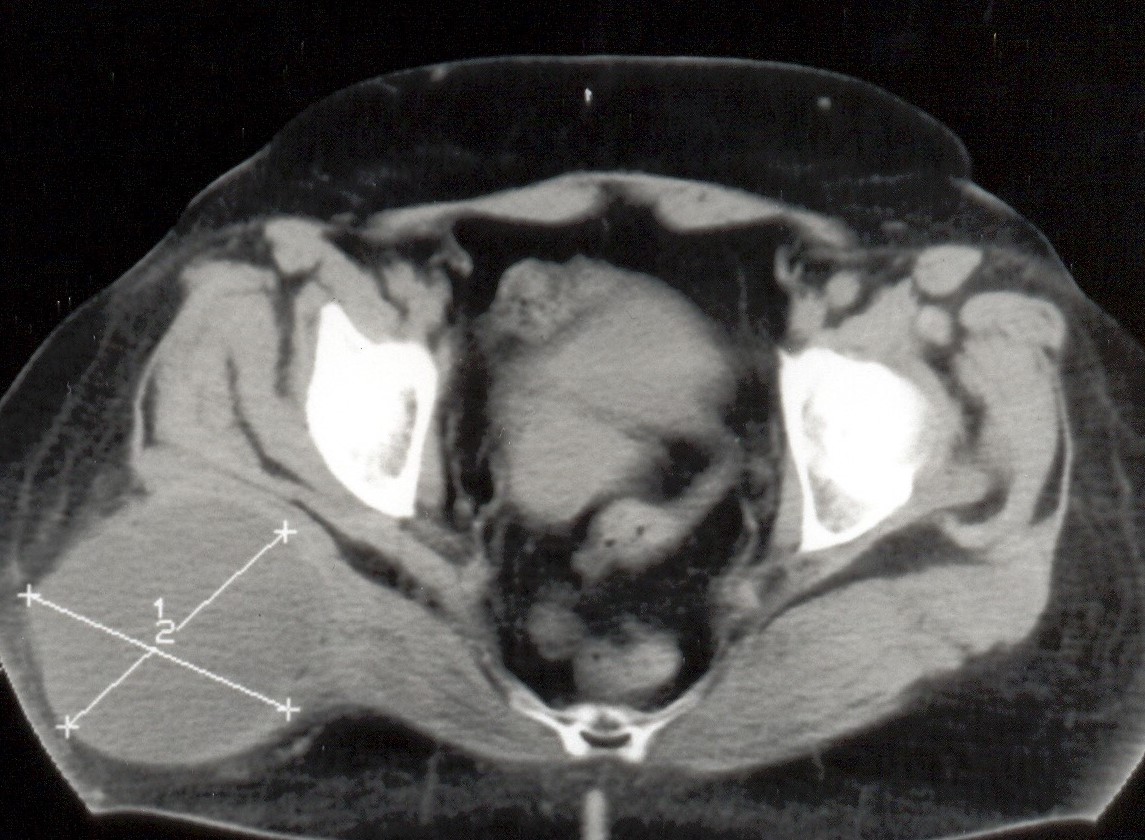
Pelvic MRI - Presence of a cystic mass with well-defined margins, without contrast enhancement after gadolinium administration (Courtesy Dr. V. Penopoulos)


MRI demonstrated a well circumscribed lesion with predominantly fat equivalent signal intensity. Hibernoma .( Courtesy Dr . V . Penopoulos ) .
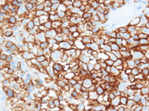
Immunohistochemistry: positivity for CD34 in tumoral cells (Courtesy Dr. V. Penopoulos).

Tumour in the lower paravertebral region, compatible with DFSP.( Courtesy Dr . V . Penopoulos ) .
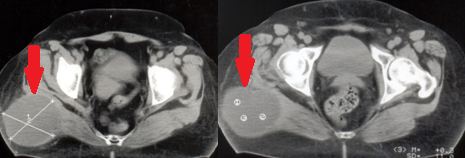
Figure 1 . CT Scan . Sizable tumour in the right buttock . Intramuscular Myxoma .( Courtesy Dr . V . Penopoulos ) .

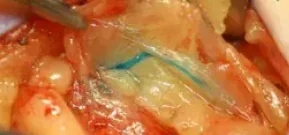
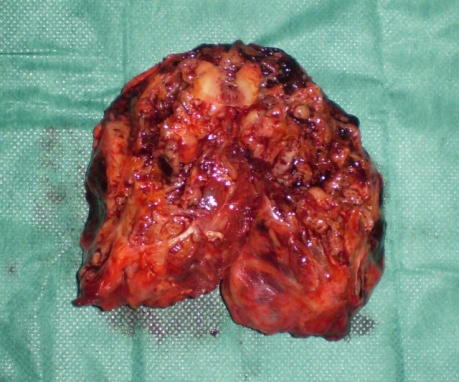
Complete excision of the Hibernoma is evident . ( Courtesy Dr . V . Penopoulos ) .
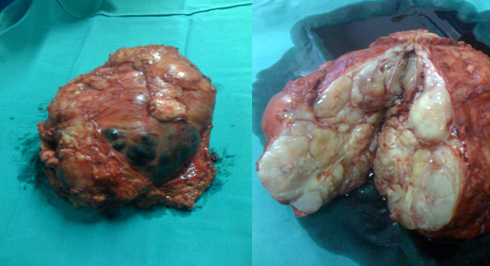
Cut surface of the excised tumor. Hibernoma . (Courtesy Dr . V . Penopoulos) .

Immunohistochemistry positivity for CD99 in tumoral cells (Courtesy Dr. V. Penopoulos).
CT Scan . Sizeable tumour in the right buttock . Intramuscular Myxoma . ( Courtesy Dr . V . Penopoulos ) .
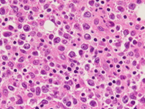
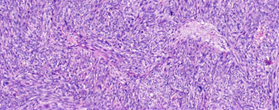
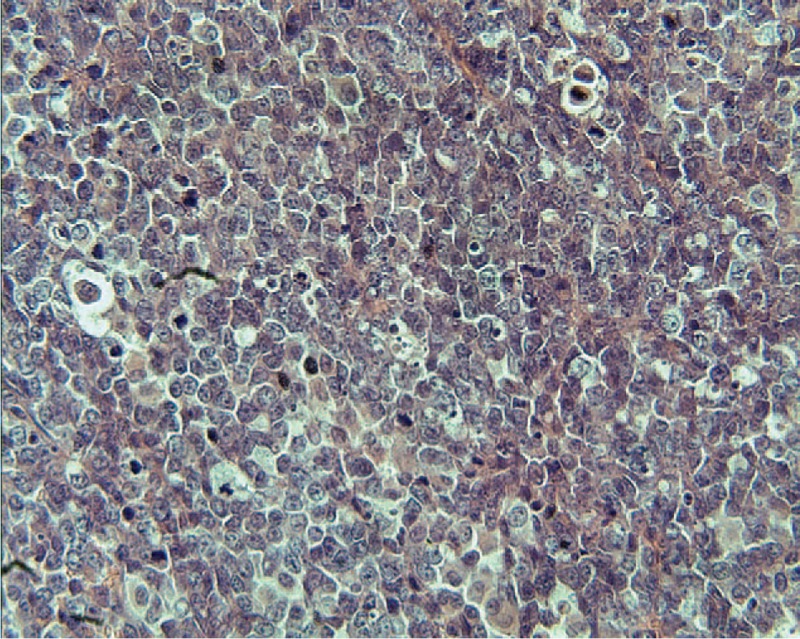
Histopatology . Proliferation of large, atypical lymphoid cells accompanied by small lymphocytes - Lymphoma .(Courtesy Dr. V. Penopoulos).
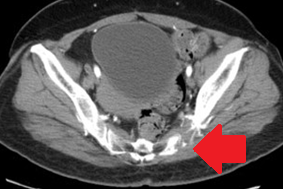
Pelvic CT Scan. Evident involvement/destruction of the sacroiliac joint. (Courtesy Dr. V. Penopoulos)
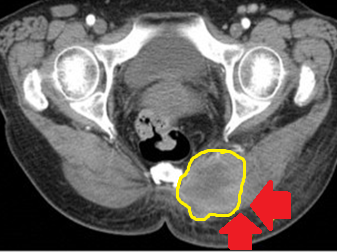
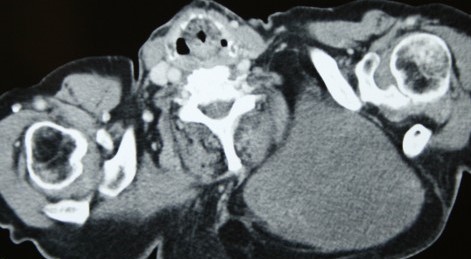
Pelvic CT scan.Yellow outline - Left gluteal mass with evident central necrosis. Lymphoma .(Courtesy Dr. V. Penopoulos)
Immunohistochemical study for CD20, reveals the presence of large atypical lymphoid cells. (Courtesy Dr. V. Penopoulos).

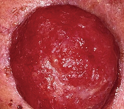
Solitary, ulcerated, and bleeding papilloma of the lumbar region.(Courtesy Dr.V.Penopoulos).

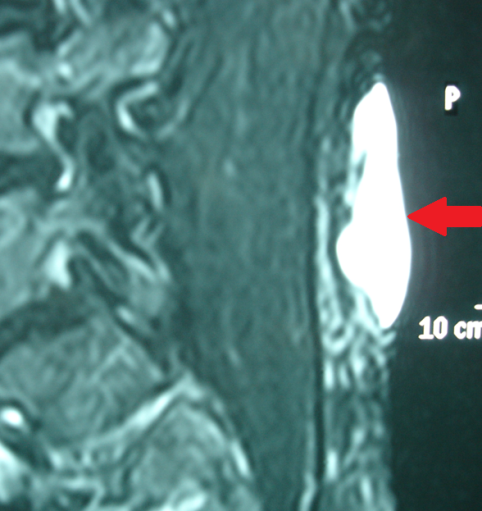
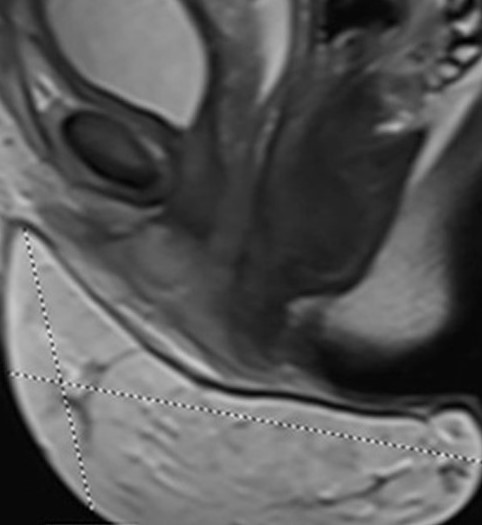
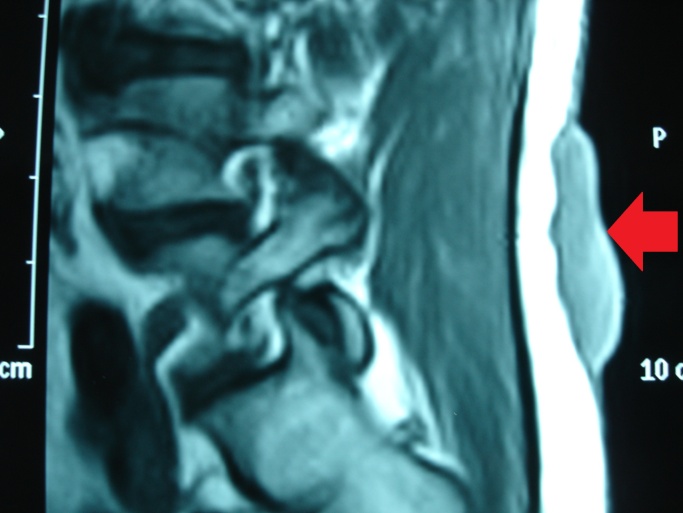
Lumbar MRI — The lesion is clearly confined to the skin and subcutaneous tissue (Courtesy Dr. V. Penopoulos)
Lumbar MRI — The lesion is clearly confined to the skin and subcutaneous tissue (Courtesy Dr. V. Penopoulos)
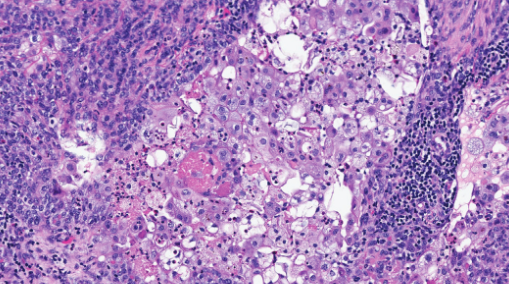
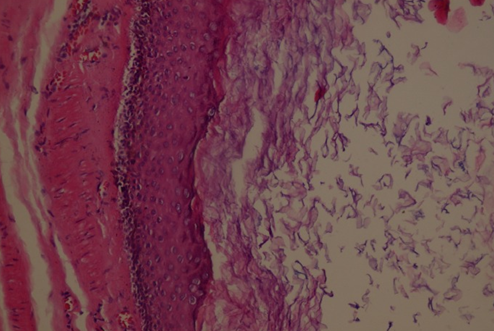
Hematoxylin–eosin staining. Extensive sebaceous differentiation of the neoplastic cells throughout the entire extent of the “lesion,” with distinct sebaceous nodules and foci of apoptosis and necrosis within the carcinomatous islands. The neoplastic cells exhibit marked mitotic activity.
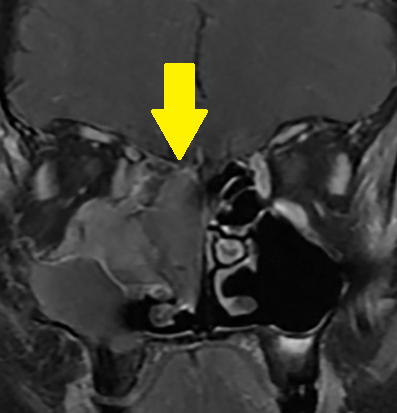
Presence of a solid mass occupying the right nasal cavity and extending into the right maxillary sinus.(Courtesy Dr.V.Penopoulos).

Presence of a solid mass occupying the right nasal cavity and extending into the right maxillary sinus.(Courtesy Dr.V.Penopoulos).

Extra-ocular sebacous glands adenocarcinomas. (Courtesy Dr . V . Penopoulos).
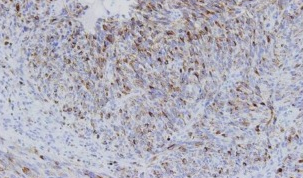
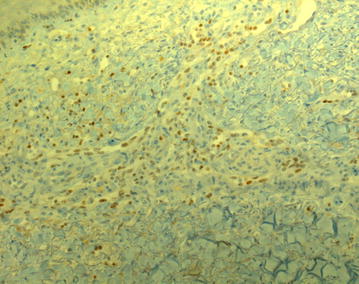
Immunohistochemical examination – Positivity for HMB45 marker (Courtesy Dr. V. Penopoulos)
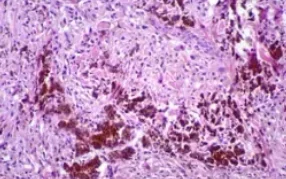
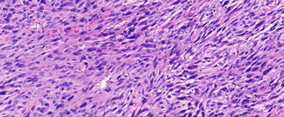
Histopathological examination revealing the presence of plump,spindle-shaped cells with prominent nuclei and melanin pigment.(Courtesy Dr.V.Penopoulos).

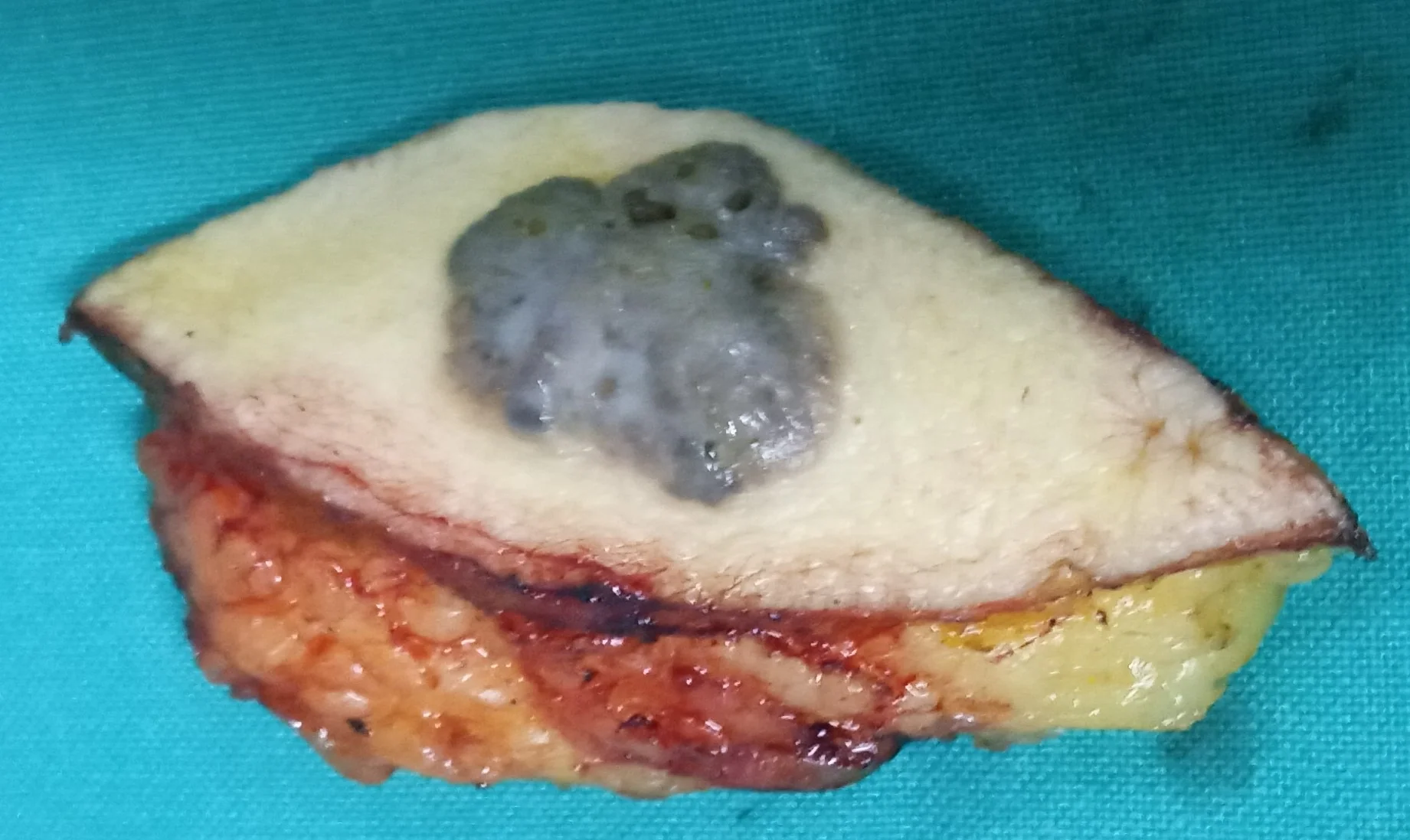
Macroscopic view of right arm cystic lesion.Sebaceous adenocarcinoma .(Courtesy Dr.D.Sgouridi).
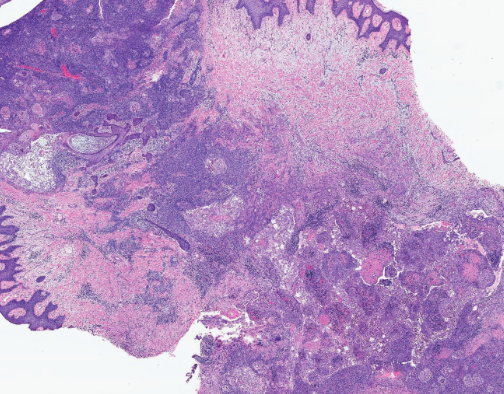
Hematoxylin–eosin staining. Layers/sheets and nodules of infiltrative basaloid blast-like cells, with areas of squamous differentiation, necrosis, and focal neutrophilic microabscesses.
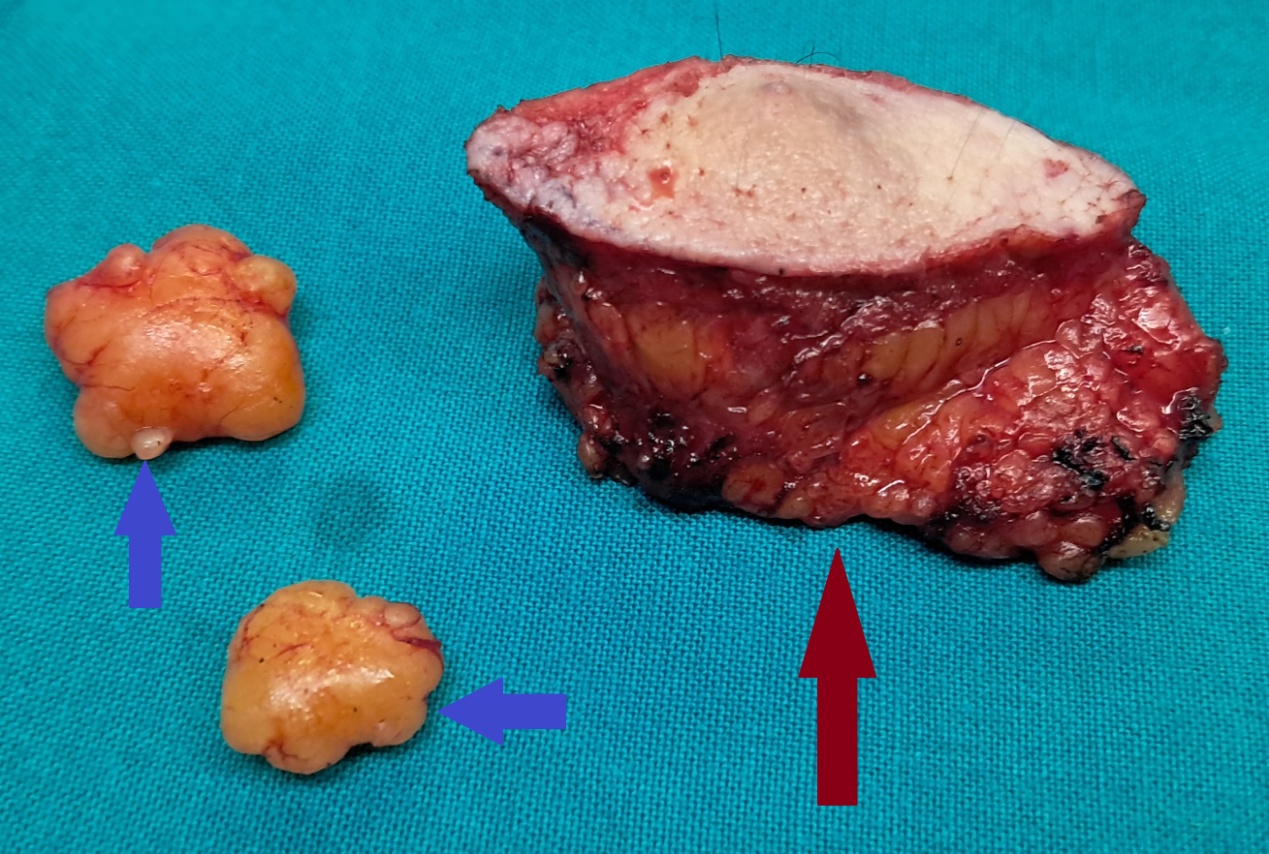
Blue arrows - Lipomas.Brown arrow - Sebaceous gland adenocarcinoma.(Courtesy Dr.D.Sgouridi).


Purulent Hidradenitis. Abscesses , draining sinuses and scarring . (Courtesy Dr . V . Penopoulos ) .


