Emergencies
Επείγοντα
60 images · 2 sub-chapters
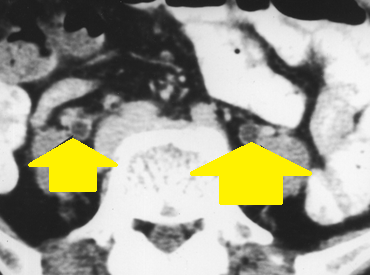
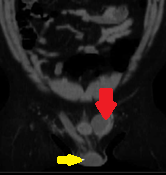
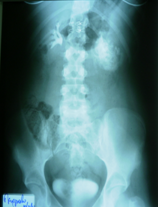
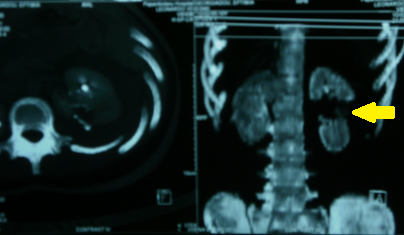
Retroperitoneal CT Scan.Yellow arrows-Bilateral ureteral dilatation.(Courtesy Dr.V.Penopoulos).
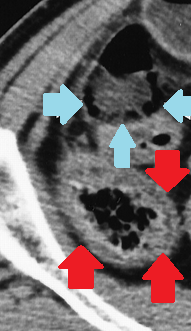
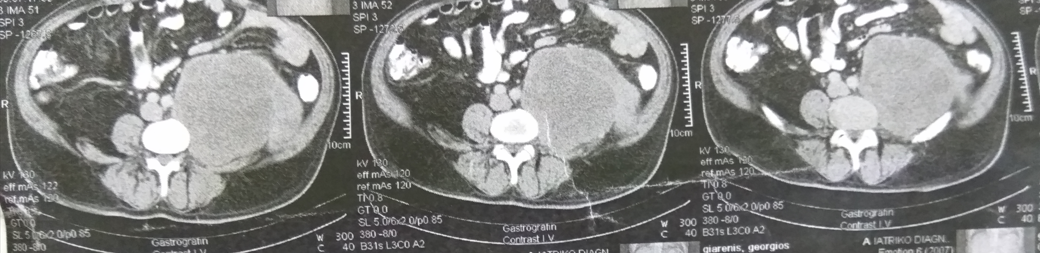
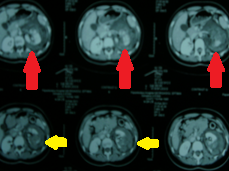
Abdominal CT Scan.Diffuse thickening and edema of the small bowel wall, indicative of mesenteric ischemia. Light blue arrows - Colonic wall thickening indicative of ischemia.(Courtesy Dr.V.Penopoulos).
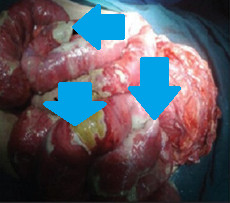
Exploratory laparotomy – Multiple perforations in another patient with polyarteritis nodosa. Courtesy Dr. V. Penopoulos.

Abdominal CT Scan.Diffuse thickening and edema of the small bowel wall.(Courtesy Dr.V.Penopoulos).

Exploratory Laparoscopy.Edematous small bowel loops with focal areas of ischemia.(Courtesy Dr.V.Penopoulos).

Chest CT Angio.Red arrow - Extensive dilatation of the Pulmonary artery.Absence of pulmonary embolism findings.(Courtesy Dr.V.Penopoulos).
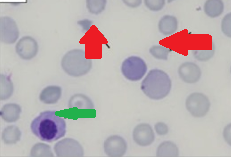
Peripheral blood smear.Red arrows - Schistocytes.Green arrow - Erythroblast.(Courtesy Dr.V.Penopoulos).
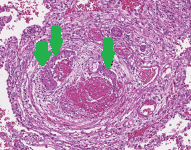
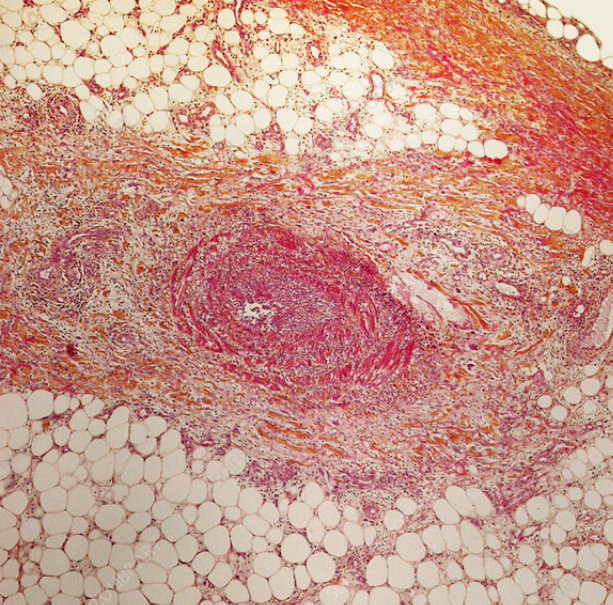
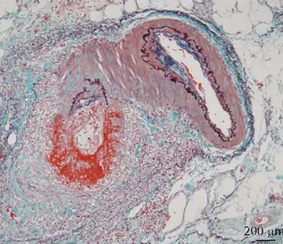
Fibroblast proliferation in the vascular intima, thrombosis, tumor cells embolization.(Courtesy Dr.V.Penopoulos).
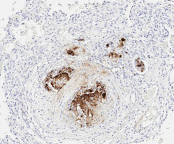
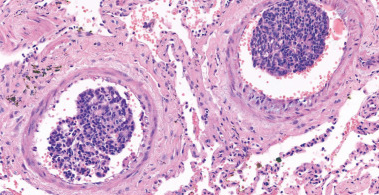
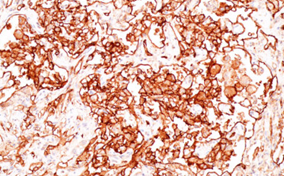
Immunohistochemical examination.Tumor cells embolization.(Courtesy Dr.V.Penopoulos0.
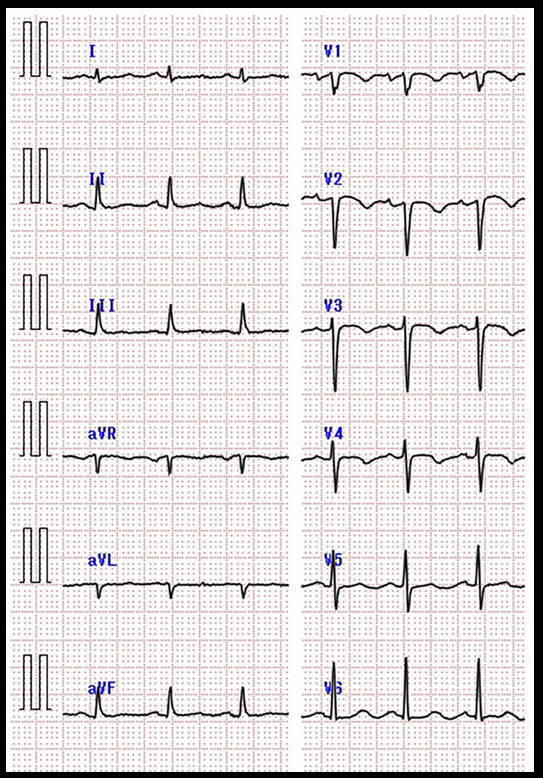
ECG.Inverted T waves in leads V1-V4,indicative of right ventricular strain.(Courtesy Dr. V. Penopoulos).
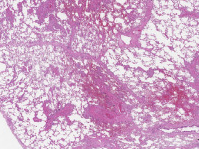
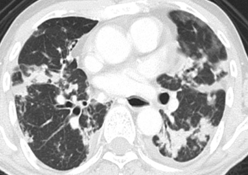
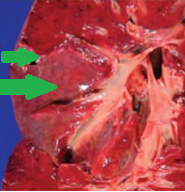
Gastric carcinoma .Pulmonary Tumor Thrombotic Microangiopathy.(Courtesy Dr.V.Penopoulos).

Cardiac ECHO . Dilated right ventricle suggestive of pulmonary hypertension.(Courtesy Dr.V.Penopoulos).
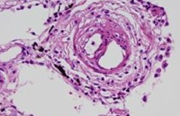
Fibroblast proliferation in the vascular intima, thrombosis, tumor cells embolization.(Courtesy Dr.V.Penopoulos).
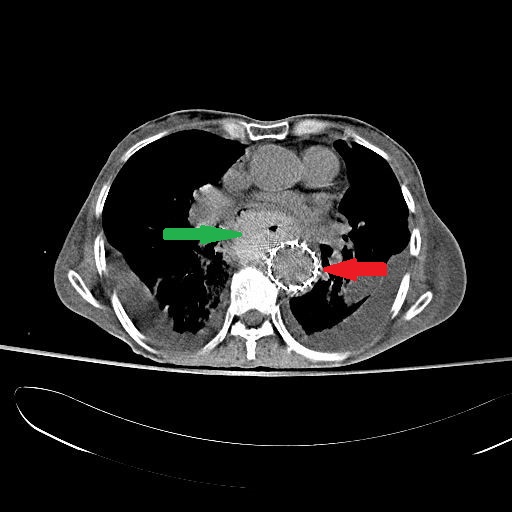
Chest CT Scan. 3rd post-op day : Aortic stent in place ( red arrow ).Minimal air detected in the mediastinal haematoma( green arrow ). (Courtesy Dr . V . Penopoulos) .
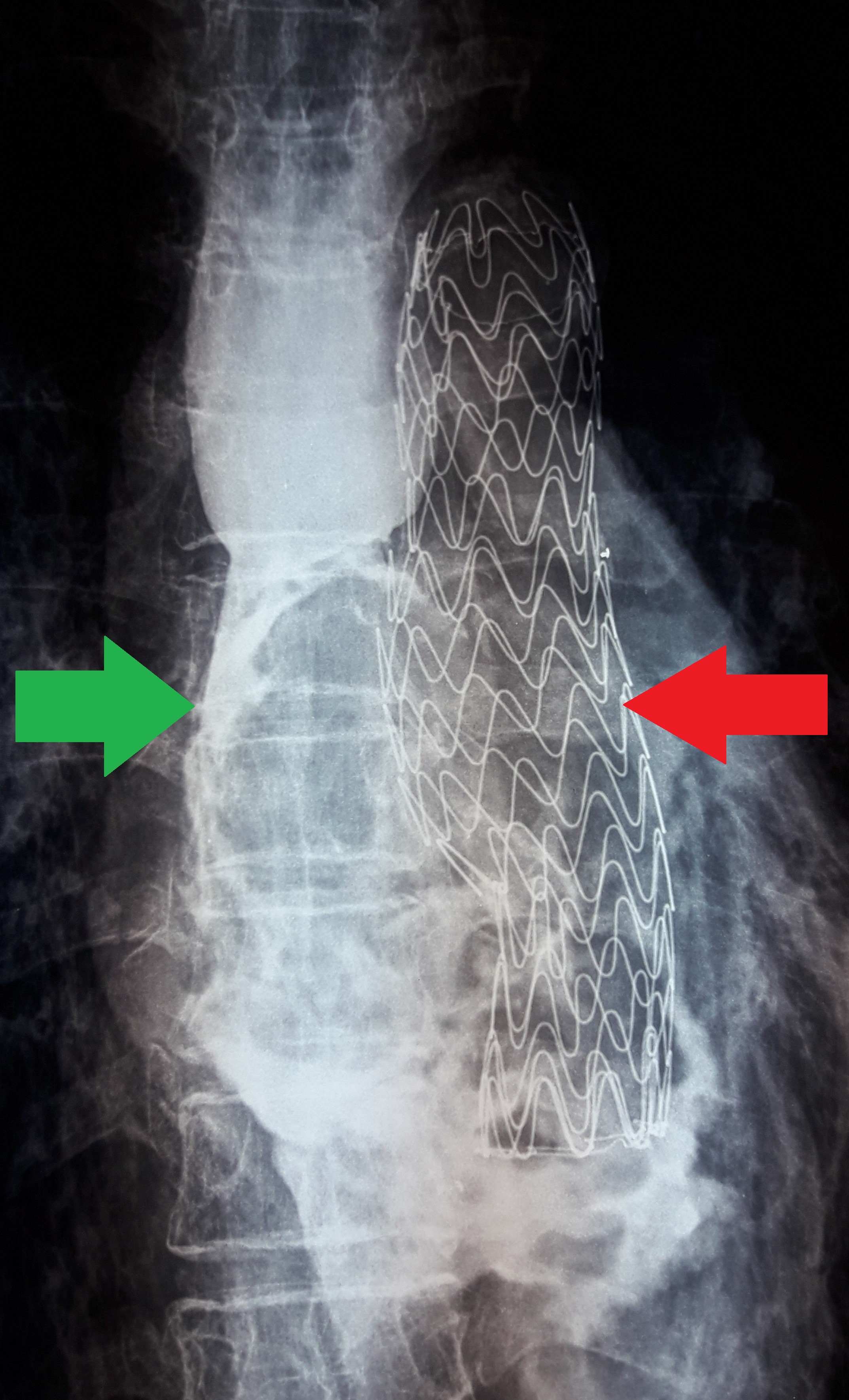
Esophagography revealed contrast medium leakage from the mid-esophagus to the mediastinum ( green arrow ) . Aortic stent in place ( red arrow ) . ( Courtesy Dr . V . Penopoulos ) .
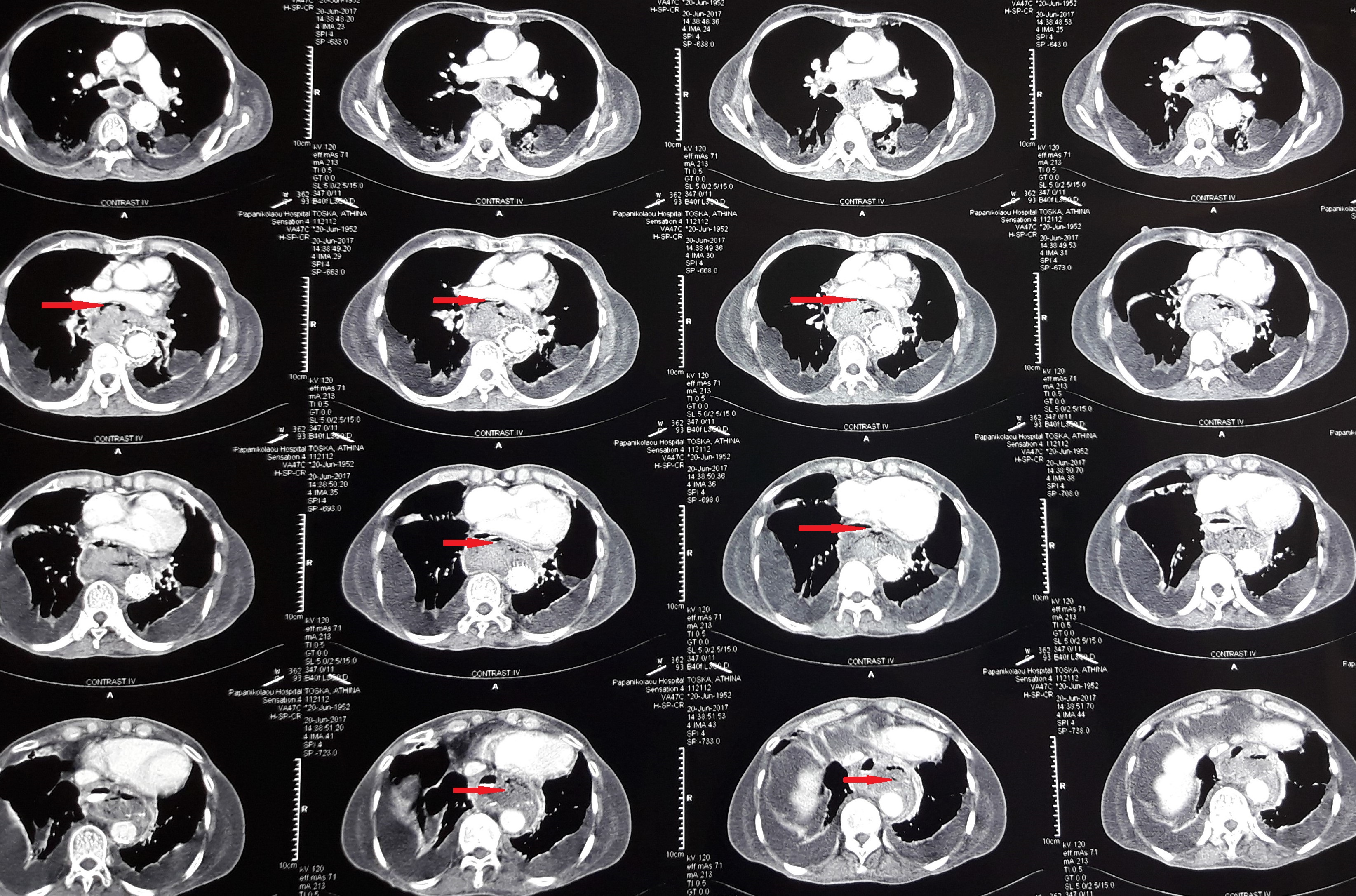
Chest CT Scan 6th post-op day : increased accumulation of air is detected in the mediastinal haematoma ( red arrows ). ( Courtesy Dr . V . Penopoulos ) .
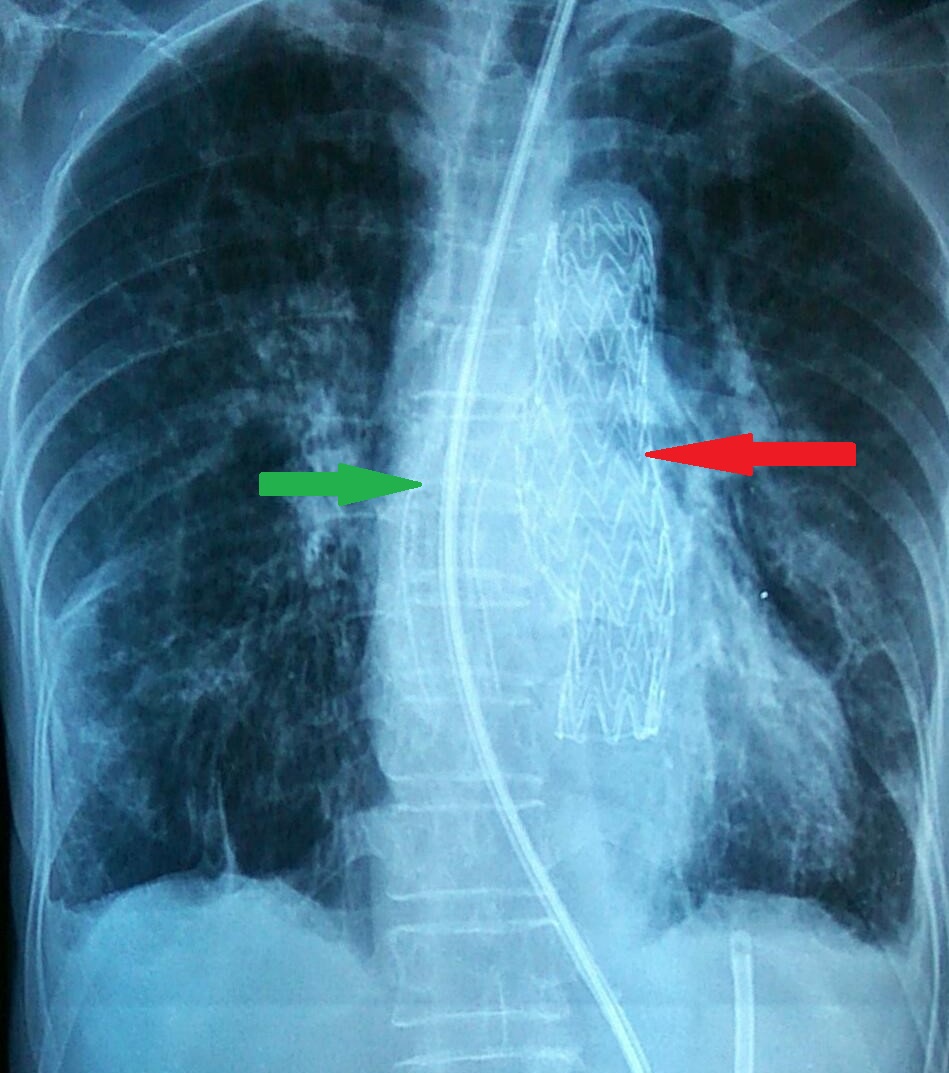
Oesophageal ( green arrow ) and Thoracic Aorta ( red arrow ) stents in place (Courtesy Dr. V. Penopoulos)

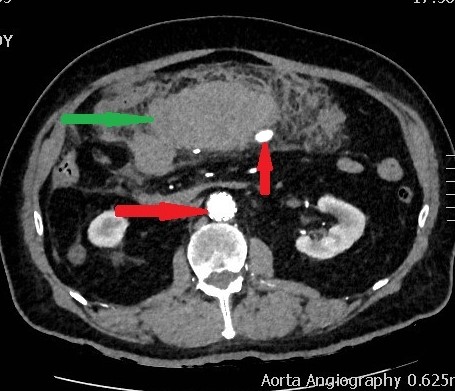
CT Angiography. Green arrow - Sizeable hematoma.Vertical red arrow - Pseudoaneurysm. Horizontal red arrow - Aorta.(Courtesy Dr.V.Penopoulos).
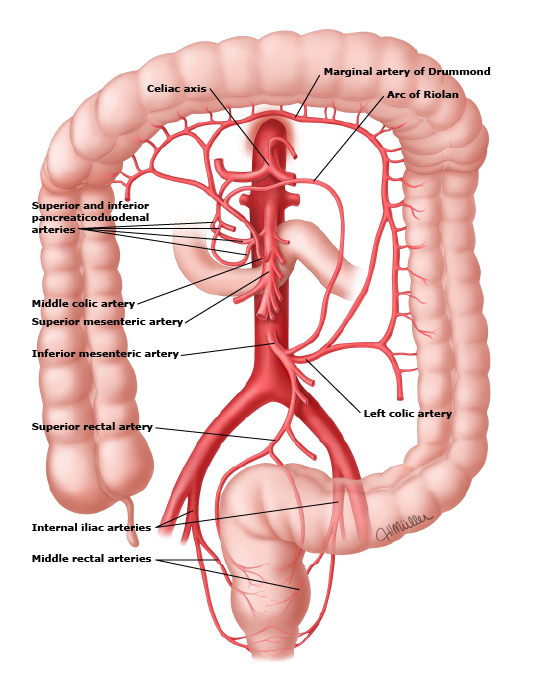
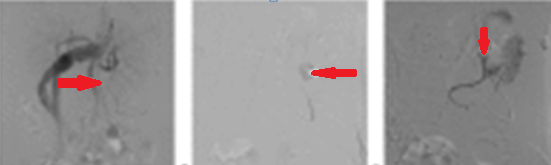
Angiography after embolization of the artery near the distal end of the pseudoaneurysm in the arterial arc of Riolan, demonstrating the coils in correct position. The sigmoid and superior rectal arteries were visualized while the pseudoaneurysm was not (Courtesy Dr. V. Penopoulos)

Post operative abdominal CT Scan . Regression of hematoma . No signs of bowel obstruction or ischemia (Courtesy Dr. V. Penopoulos)
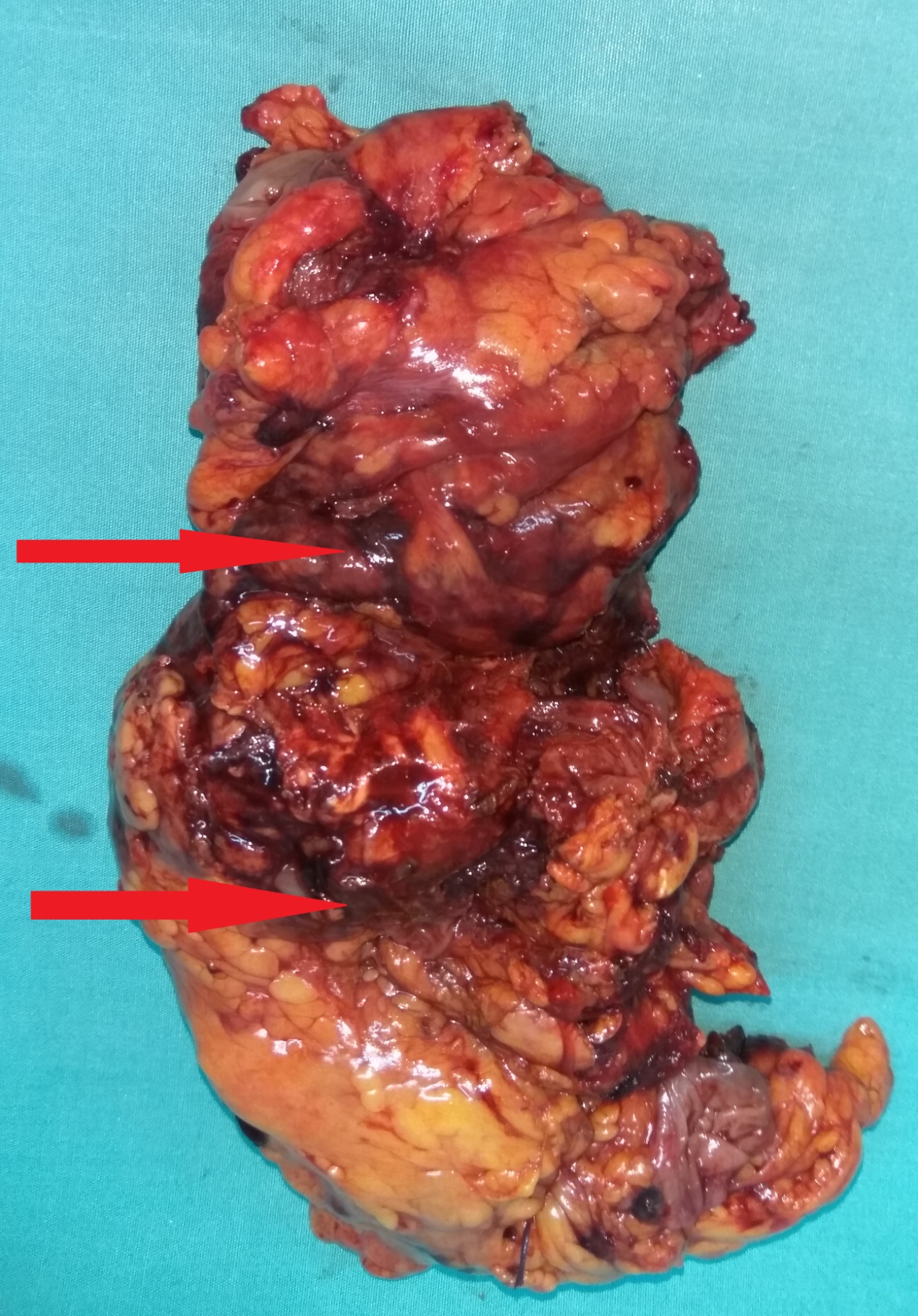
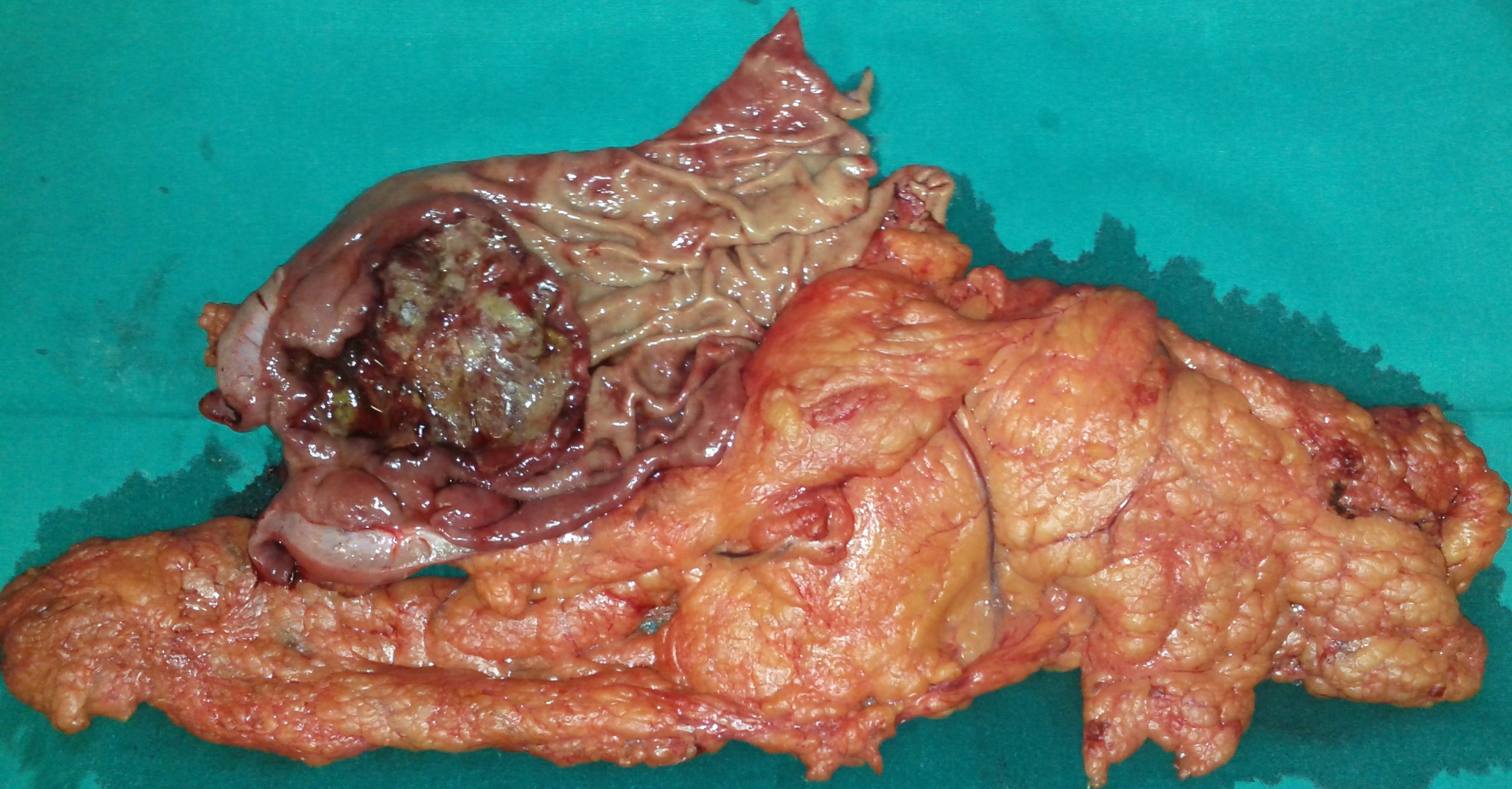
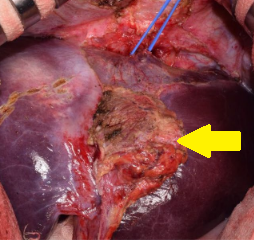
Rectosigmoid specimen.Red arrows - Direct infiltration of sigmoid colon.(Courtesy Dr.V.Penopoulos).
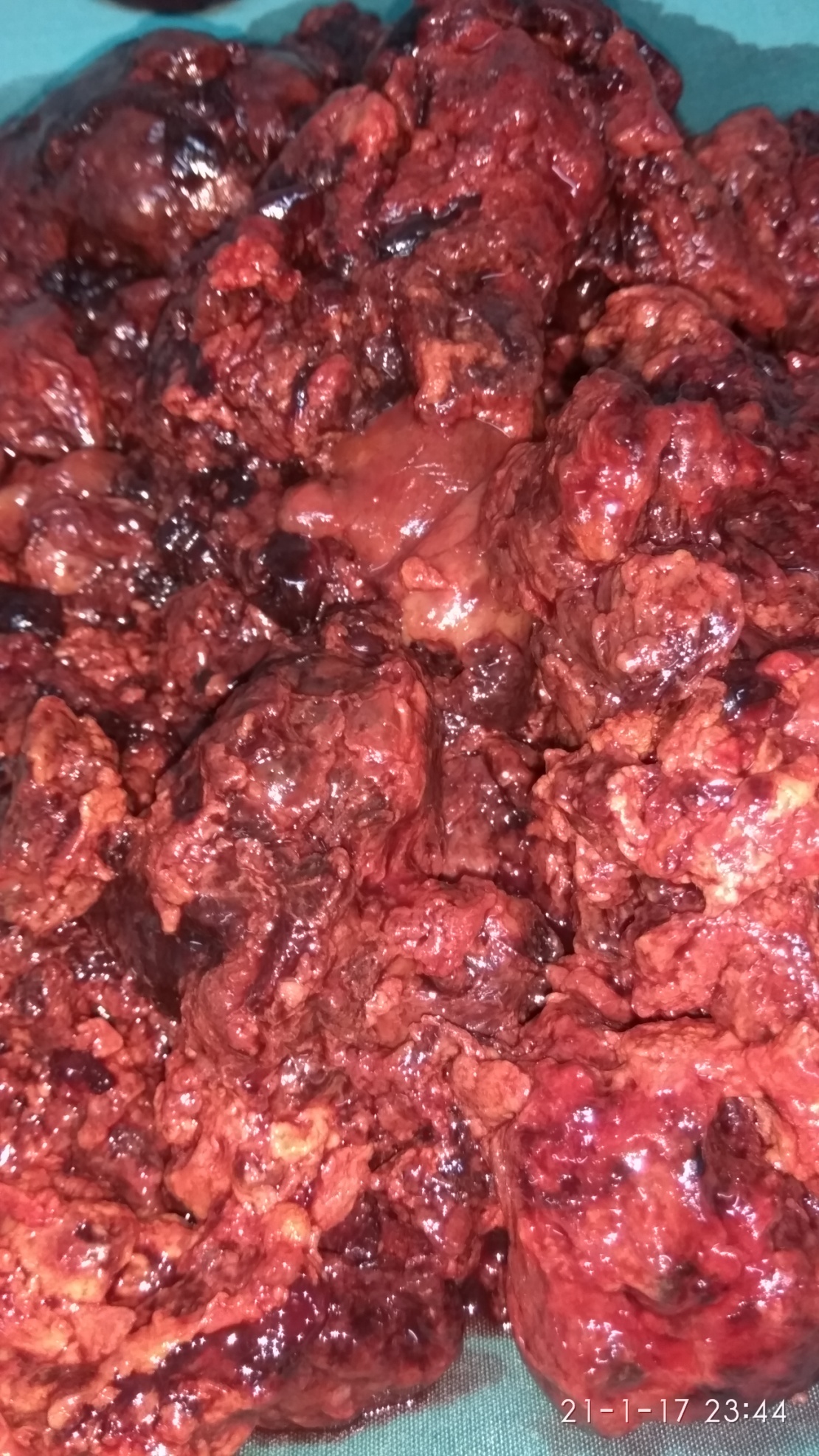
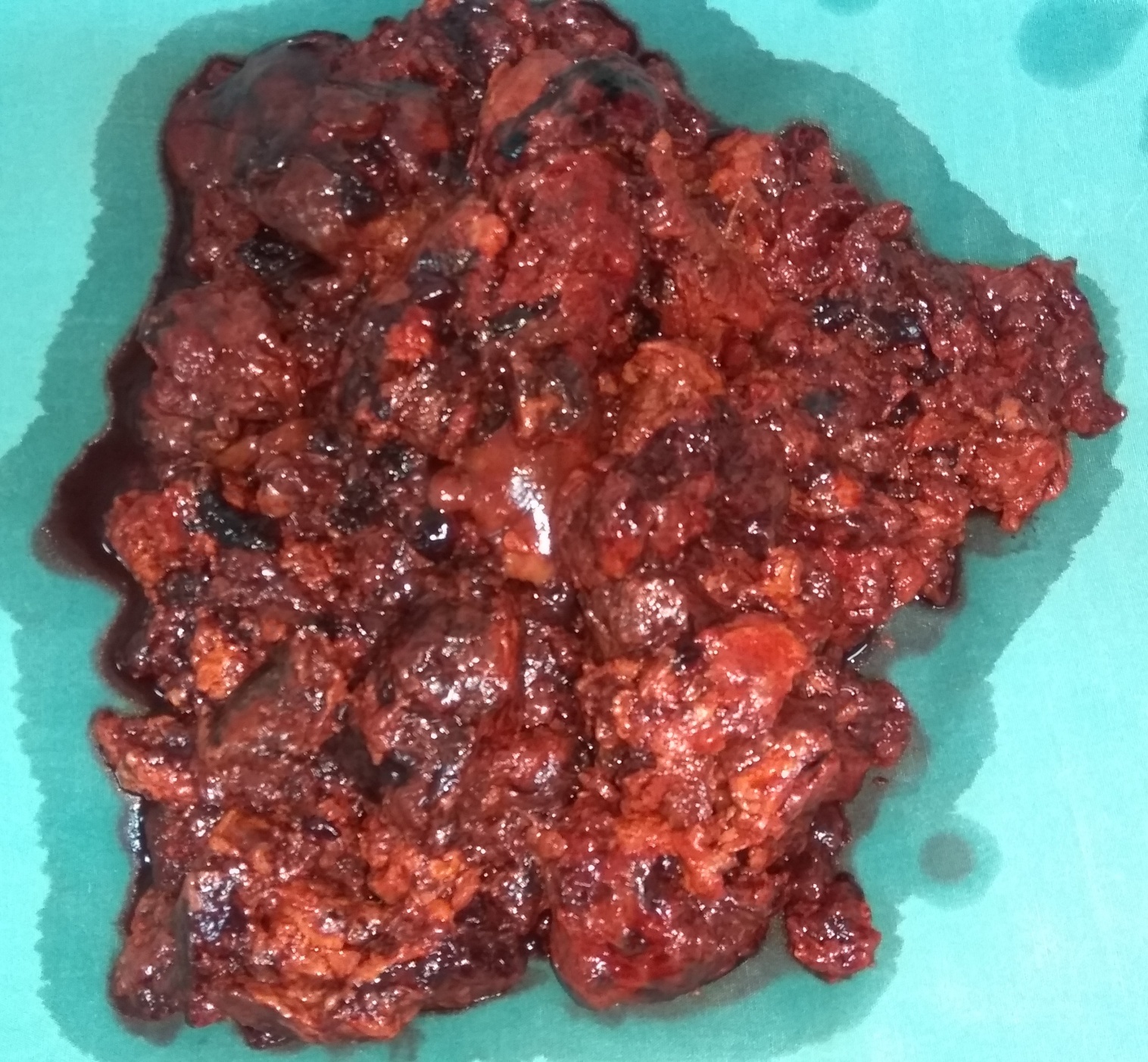
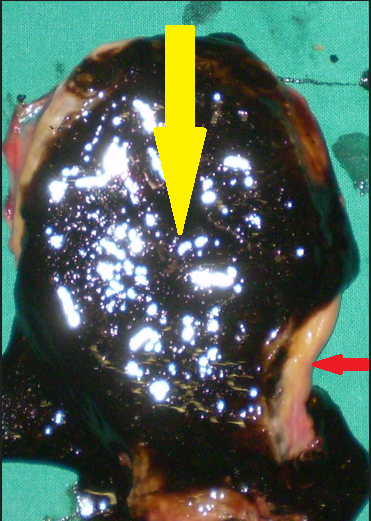
Detailed macroscopic view of retroperitoneal angiosarcoma.(Courtesy Dr.V.Penopoulos).

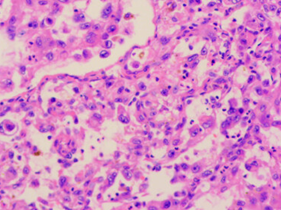
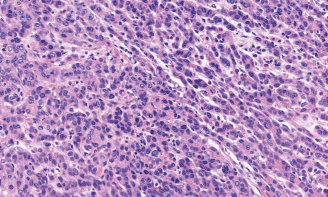
Epithelioid malignant cells, with evident cellular atypia and mitotic figures (Courtesy Dr. V. Penopoulos)

Displaced testicle found just before the external inguinal ring.(Courtesy Dr. V. Penopoulos).

Red arrow — Displaced testis in the left inguinal region. Yellow arrow — Right testis within the scrotum (Courtesy Dr. V. Penopoulos)
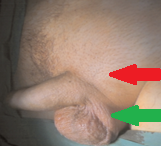
Red arrow - Displaced testicle in the left inguinal region.Green arrow - Empty left hemiscrotum.(Courtesy Dr.V.Penopoulos).
Catheterization of the thoracic duct and glue injection. (Courtesy Dr. V. Penopoulos)

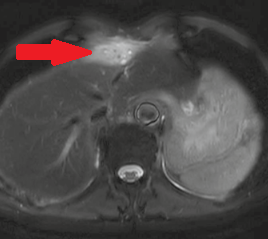
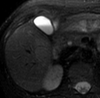
Abdominal CT scan. Red arrow – Ascites. Purple arrow – Spleen. Green arrow – Liver (Courtesy Dr. V. Penopoulos)
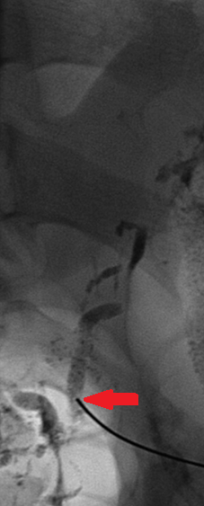

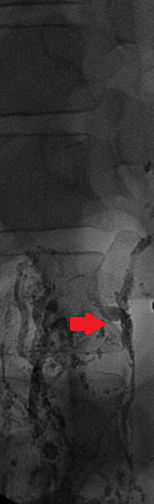
Cystography.Red arrow-Exit of the contrast from the ruptured urinary bladder.(Courtesy Dr. V. Penopoulos)
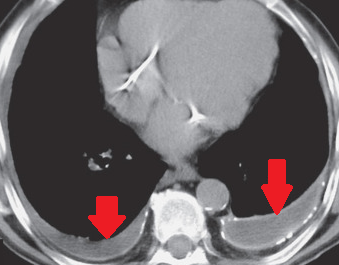
Chest CT scan – Bilateral pleural effusions. Chylous Ascites . (Courtesy Dr. V. Penopoulos)

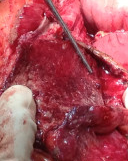
Intraoperative view (after repair of the bladder perforation) (Courtesy Dr. V. Penopoulos)

Postoperative cystography-Negative for leakage.(Courtesy Dr. V. Penopoulos).

Intraoperative view of the posterior wall bladder's rupture.(Courtesy Dr. V. Penopoulos).

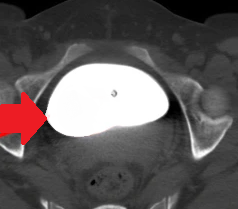
Αbdominal CT Scan . Rupture of urinary bladder.(Courtesy Dr. V. Penopoulos)
Thickened gallbladder wall and presence of biliary sludge.(Courtesy Dr.V.Penopoulos).
Yellow arrow – Biliary sludge. Red arrow – Thickened gallbladder wall (Courtesy Dr. V. Penopoulos)
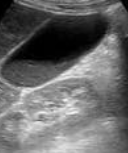
Thickened gallbladder wall and presence of biliary sludge (Courtesy Dr. V. Penopoulos)
Acute Abdomen
(0 images)No images in this chapter yet.
Trauma
(0 images)No images in this chapter yet.