08
Hernias
Κήλες
132 images · 3 sub-chapters
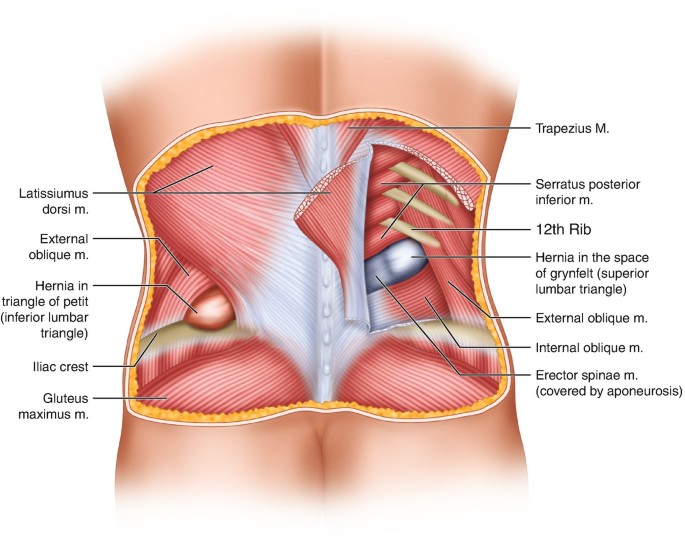
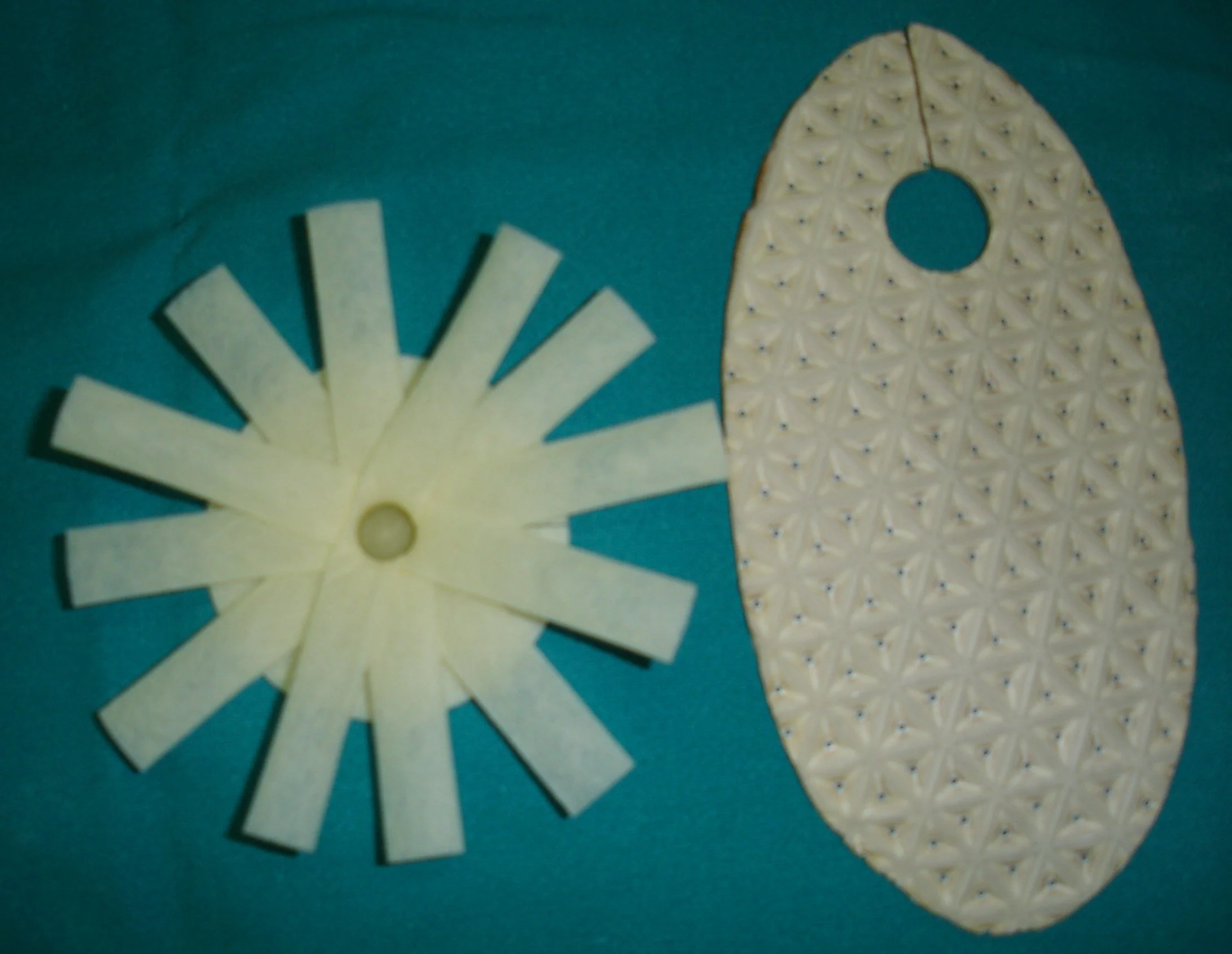
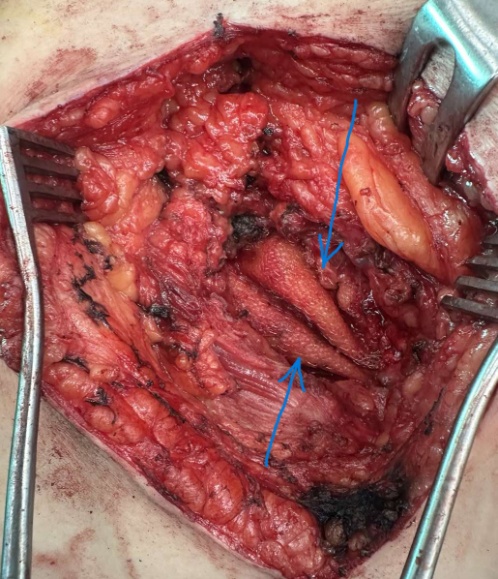
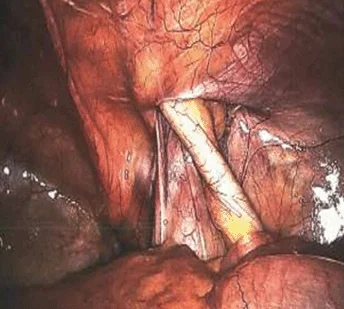
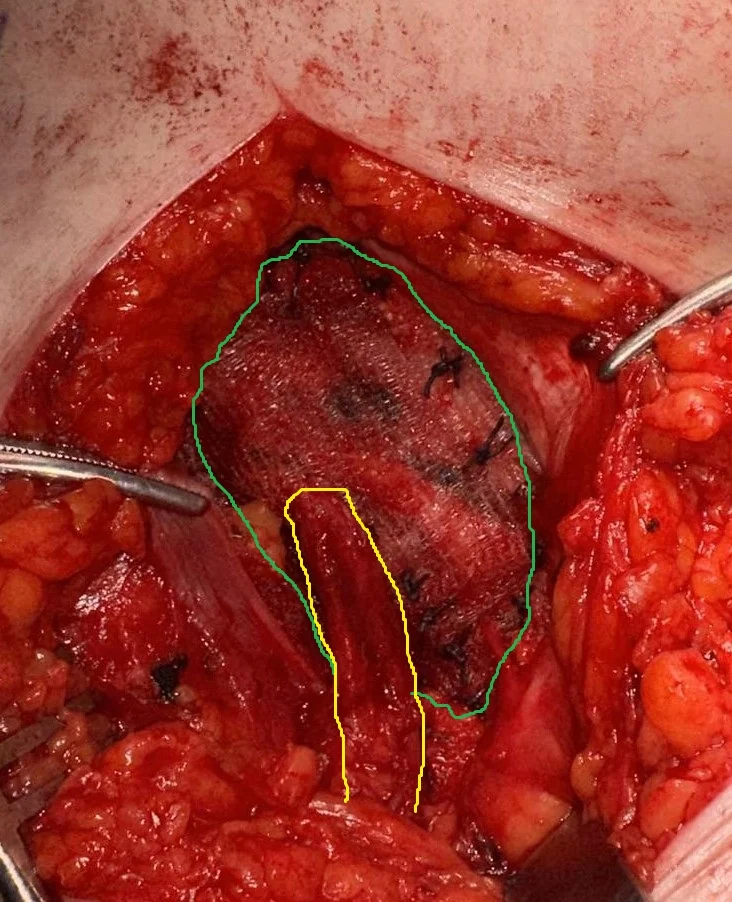
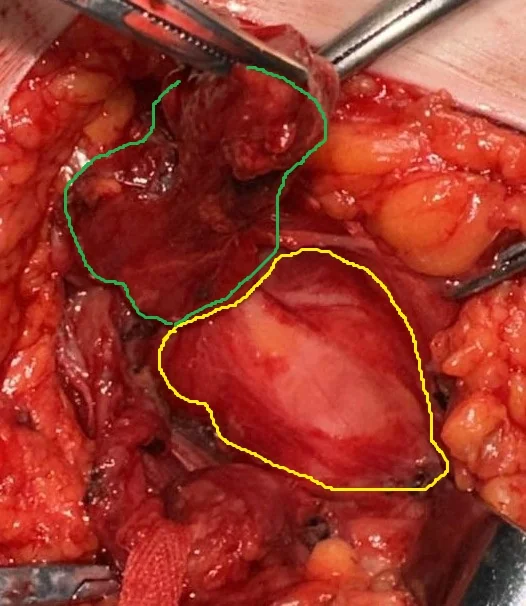
Anatomy of Lumpar Hernias.
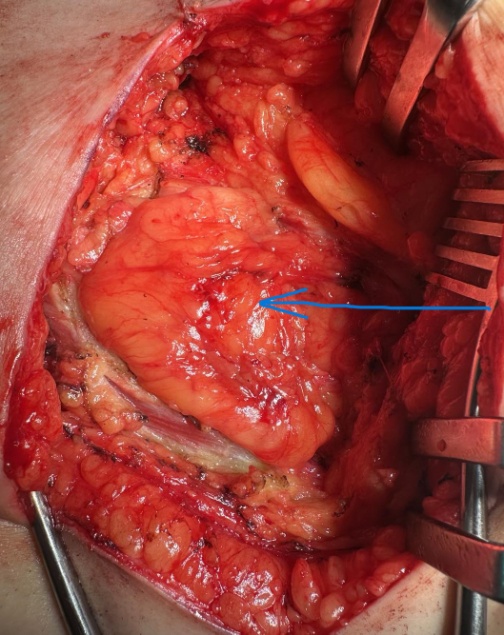
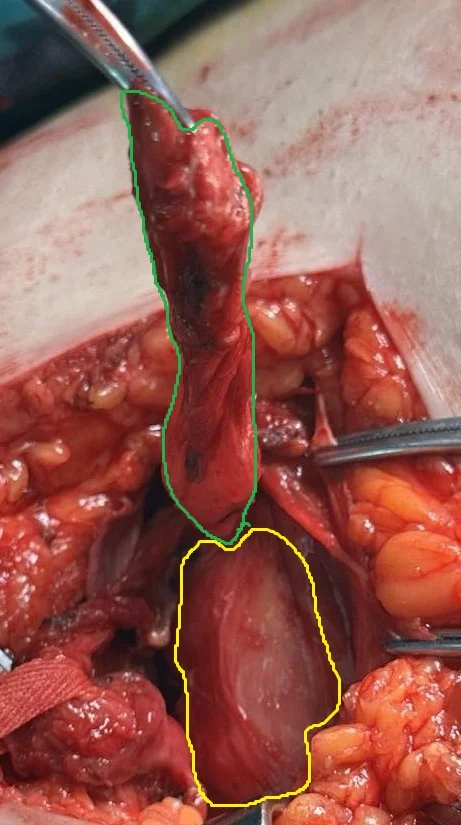
Protruding lumpar hernia through the triangle of Petit.(Courtesy Dr.V.Prnopoulos).
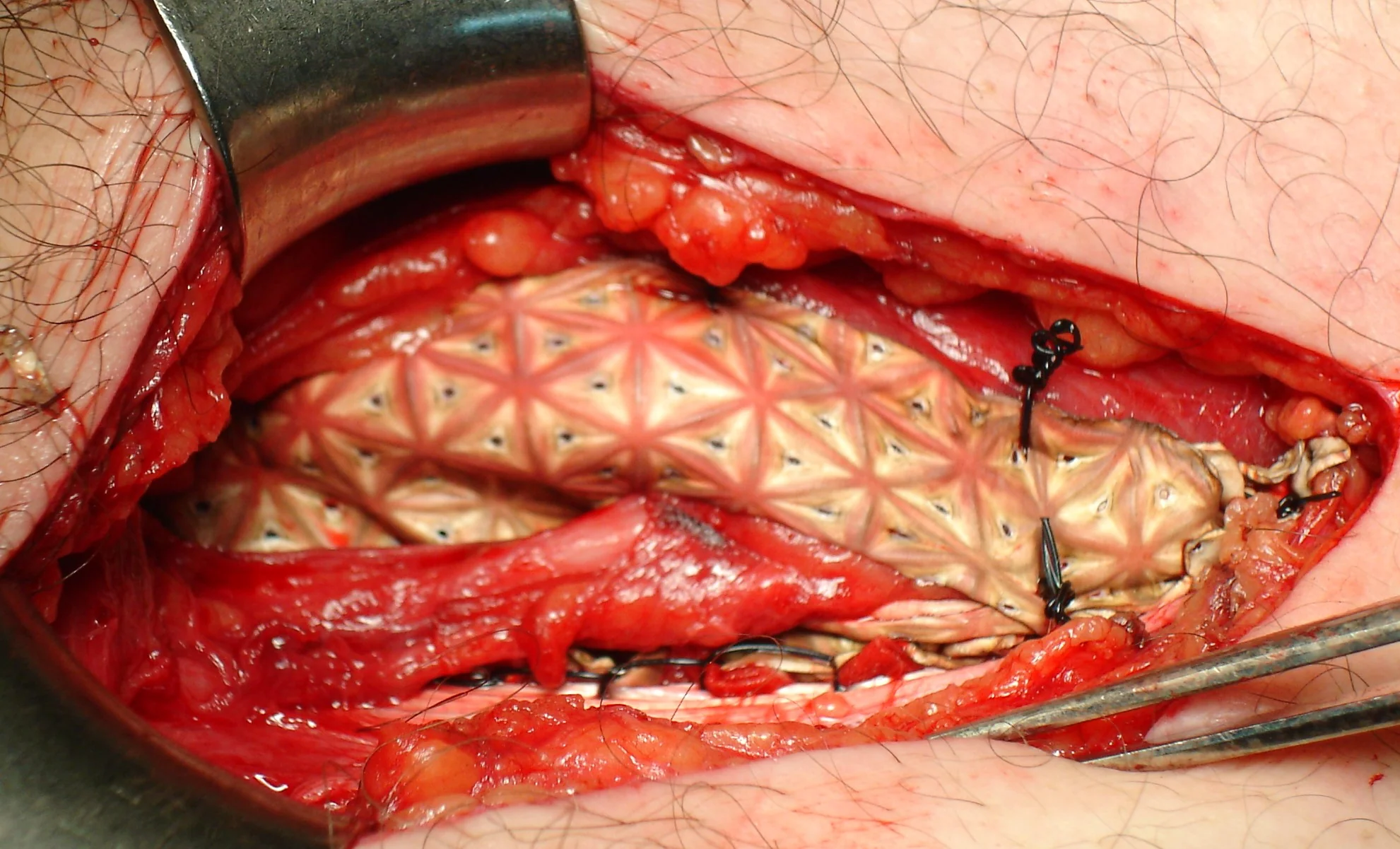
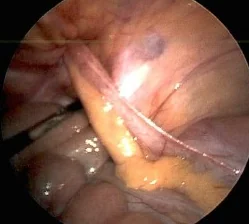
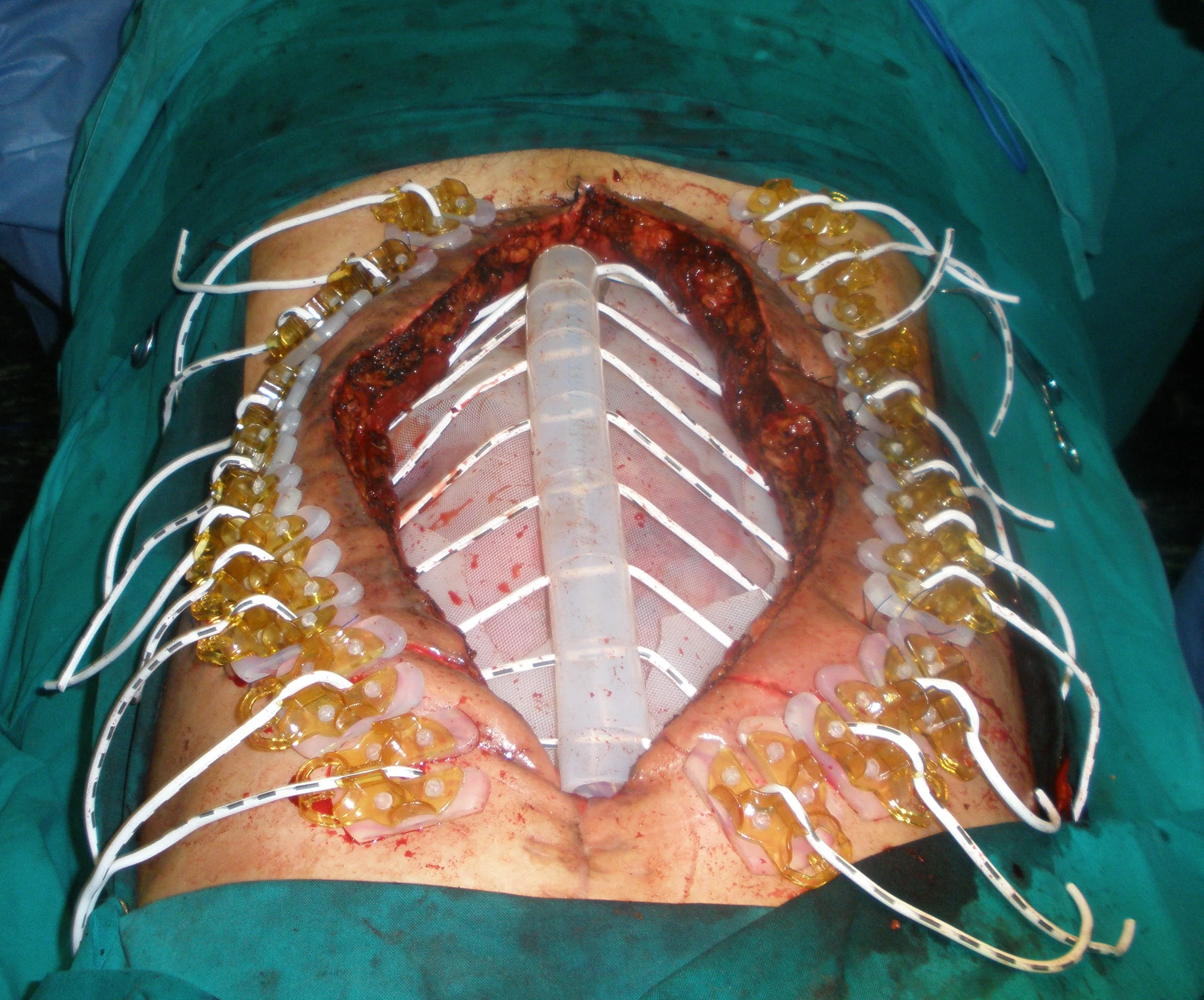
Inlay hernia mesh repair.(Courtesy Dr.V.Penopoulos).

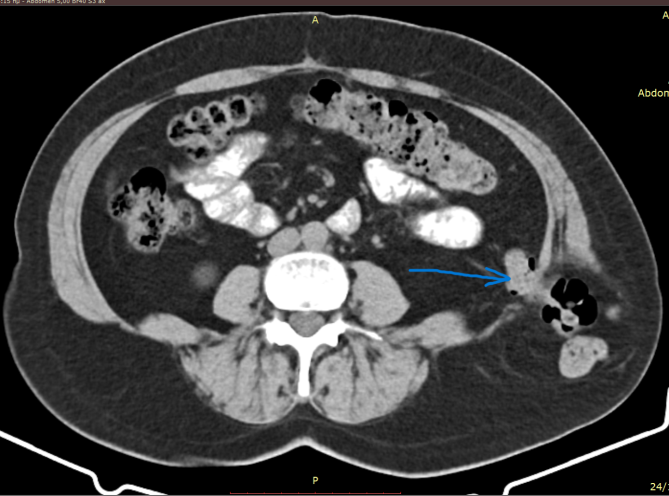
CT of the abdomen 1 (one) year after surgical repair of the lumbar hernia. Complete elimination of the defect (Courtesy Dr. V. Penopoulos)
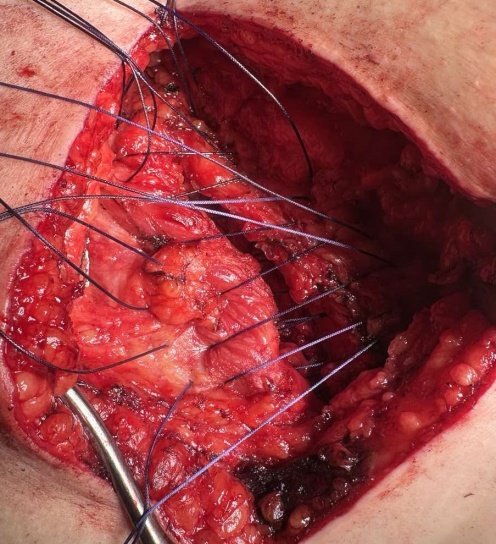
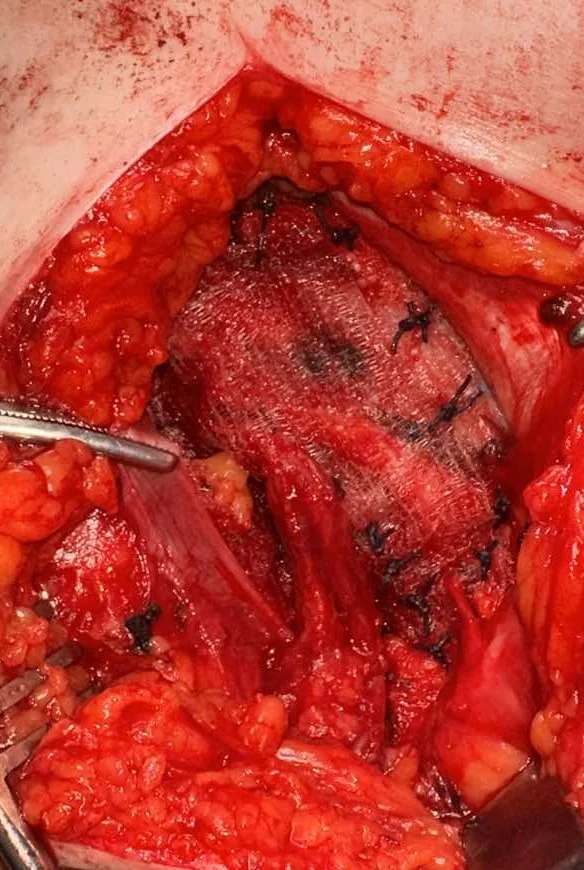
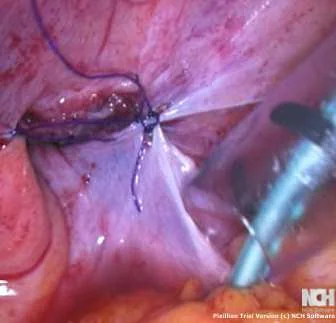
Closure of the defect with interrupted Vicryl No. 2 sutures without tension (Courtesy Dr. V. Penopoulos)

Protruding swelling above the left posterior iliac crest.(Courtesy Dr.V.Penopoulos).
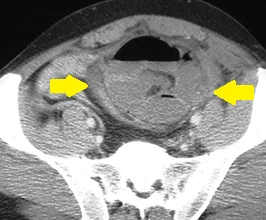
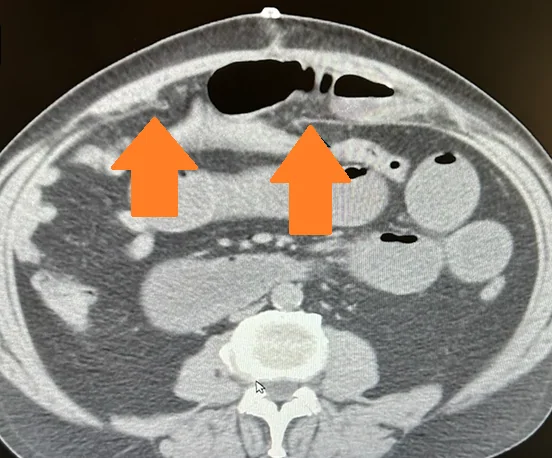
CT Scan.Protrusion of large bowel through the inferior lumpar triangle.(Courtesy Dr.V.Penopoulos).
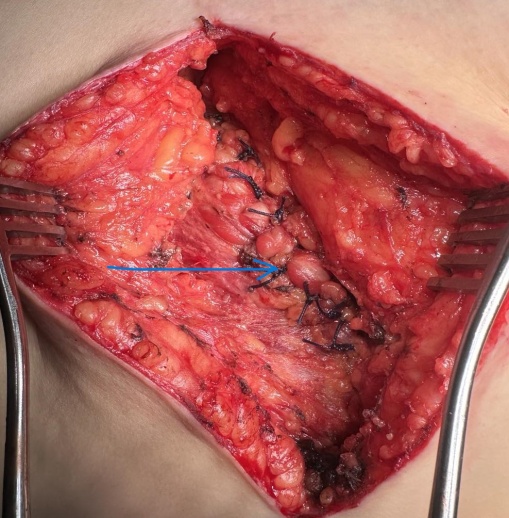
Complete elimination of the defect.(Courtesy Dr.V.Penopoulos).

CT of the abdomen 1 (one) year after surgical repair of the lumbar hernia. Complete elimination of the defect (Courtesy Dr. V. Penopoulos)
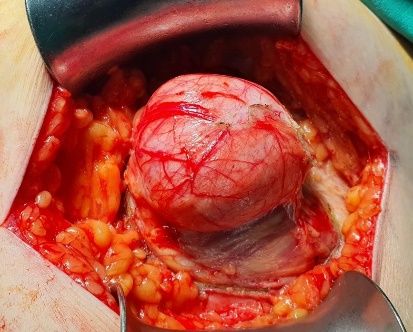
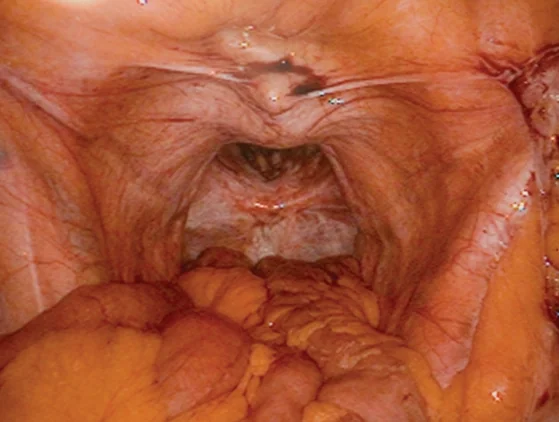
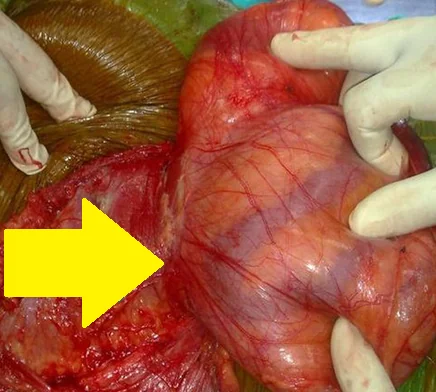
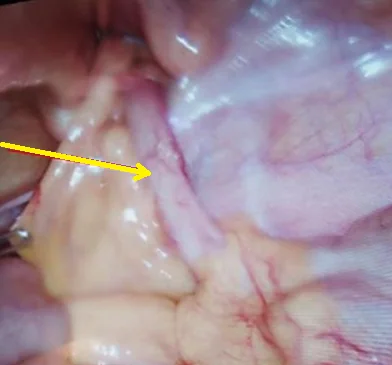
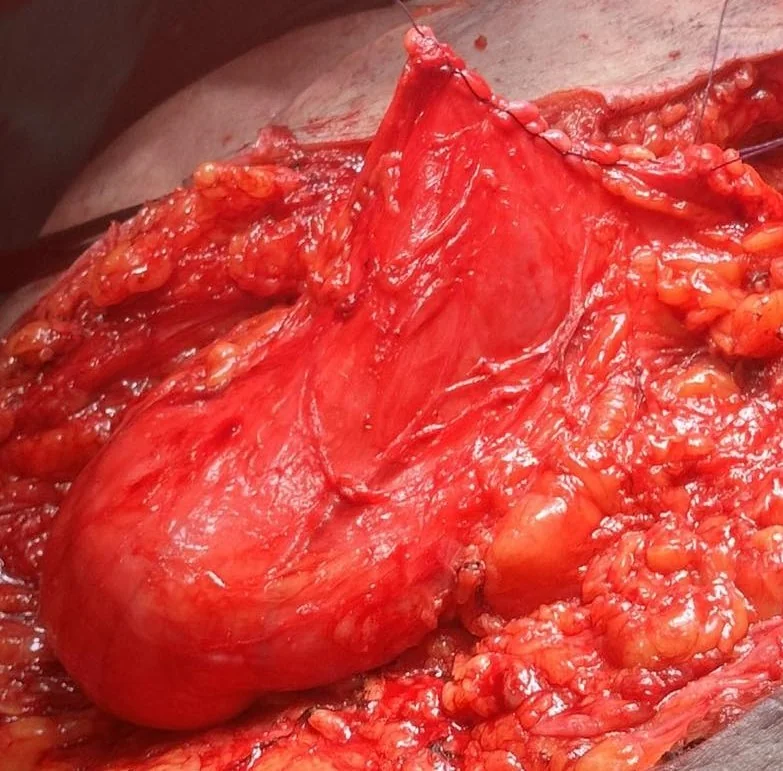
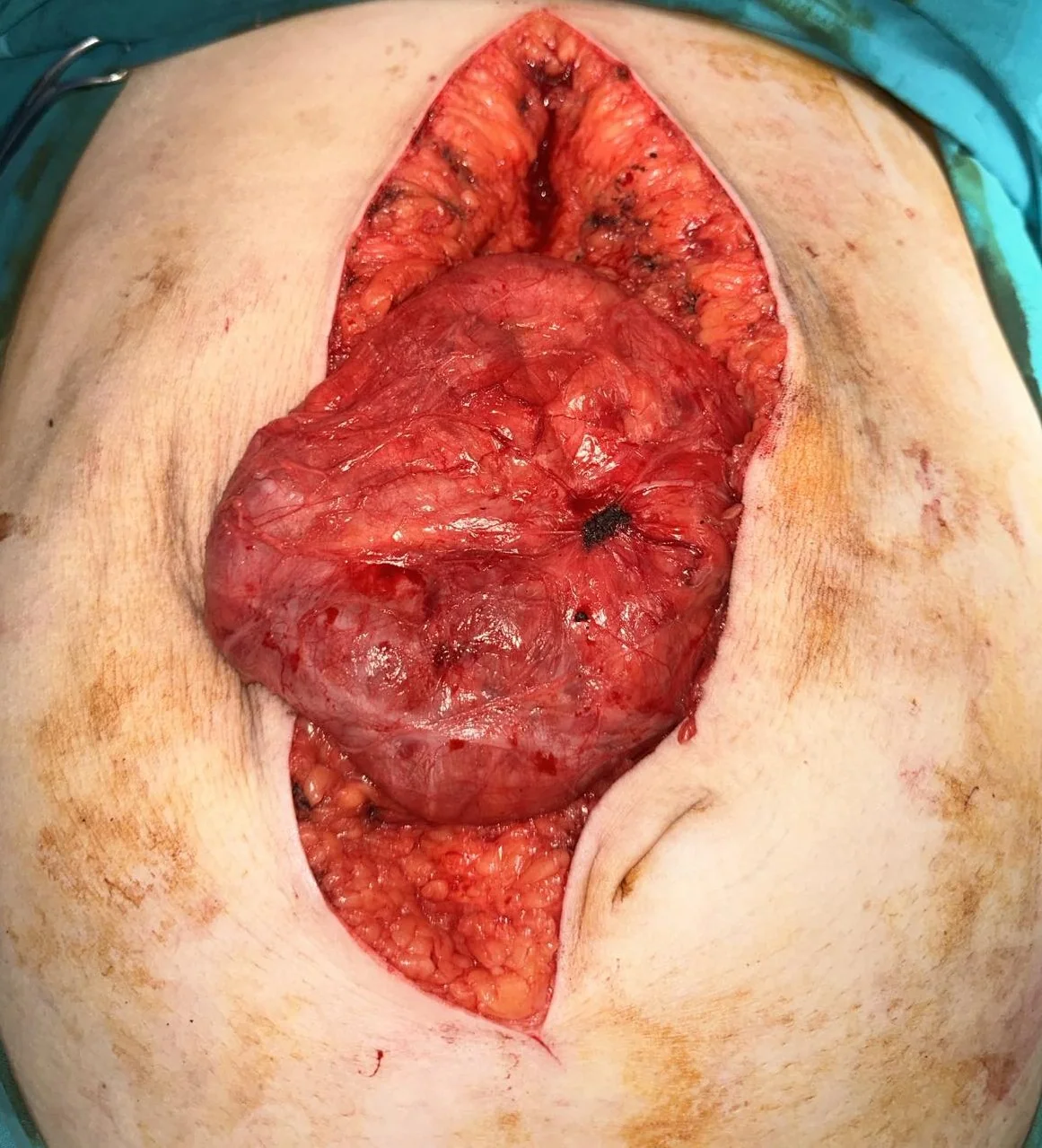
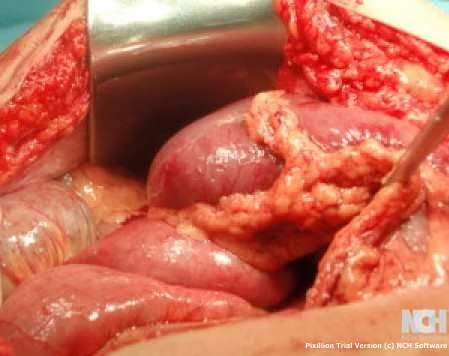
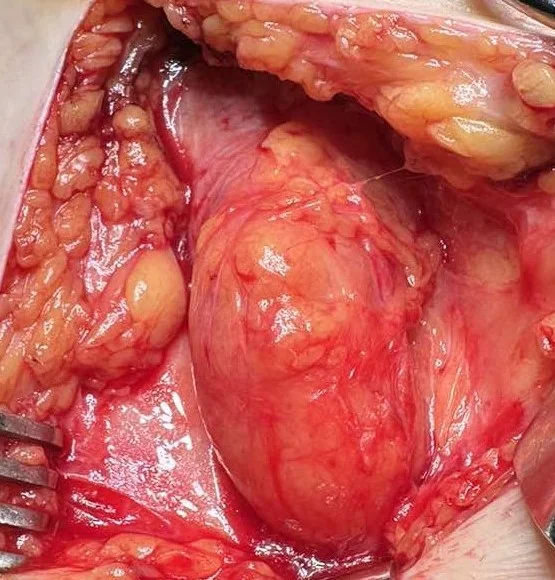
Operative view of the Spiegelian hernia . ( Courtesy Dr . V . Penopoulos ) (Courtesy Dr. V. Penopoulos).

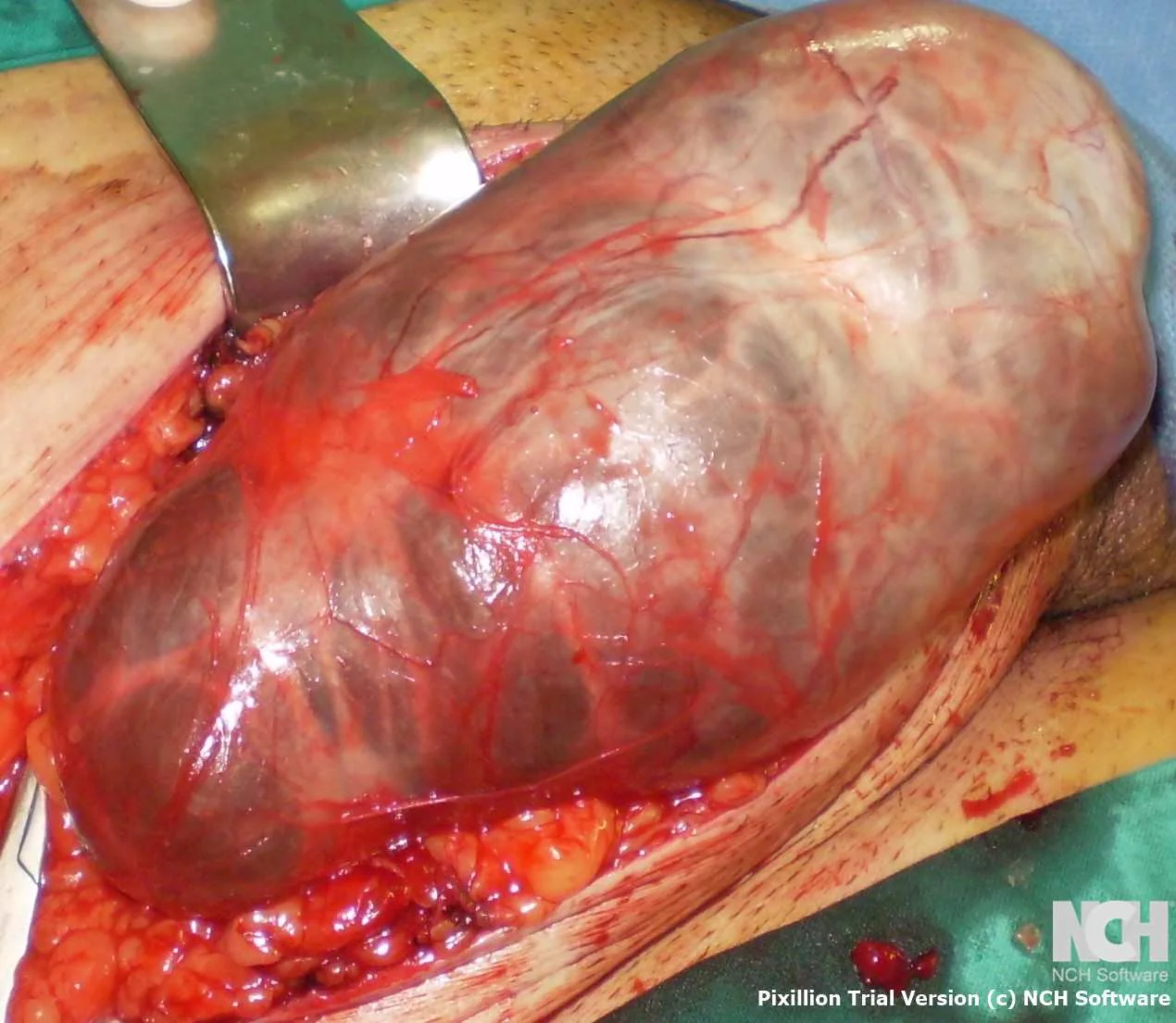
Figure 2 . Giant inguinoscrotal hernia , extending up to the knee joint . (Courtesy Dr . V . Penopoulos) .

Figure 1 . The extreme size of the scrotal “swelling” is obvious .( Courtesy Dr. V . Penopoulos ) .
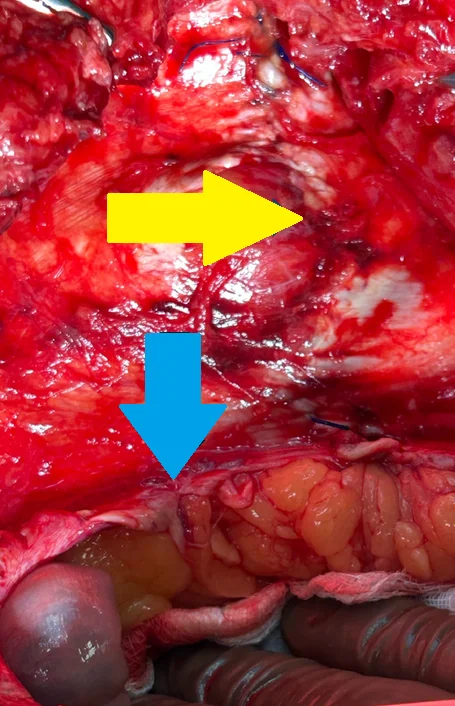
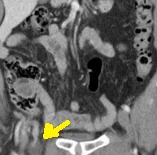
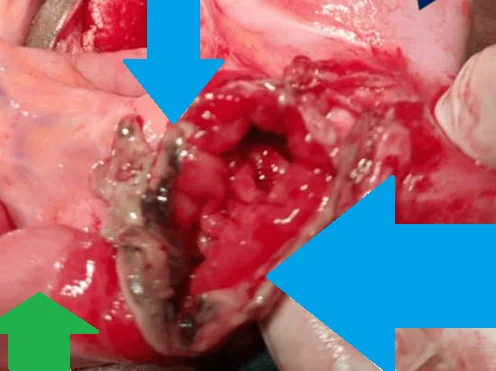
Blue arrow. The hernia orifice through which the ascitic fluid enters the intercostal hernia (Courtesy Dr. V. Penopoulos)
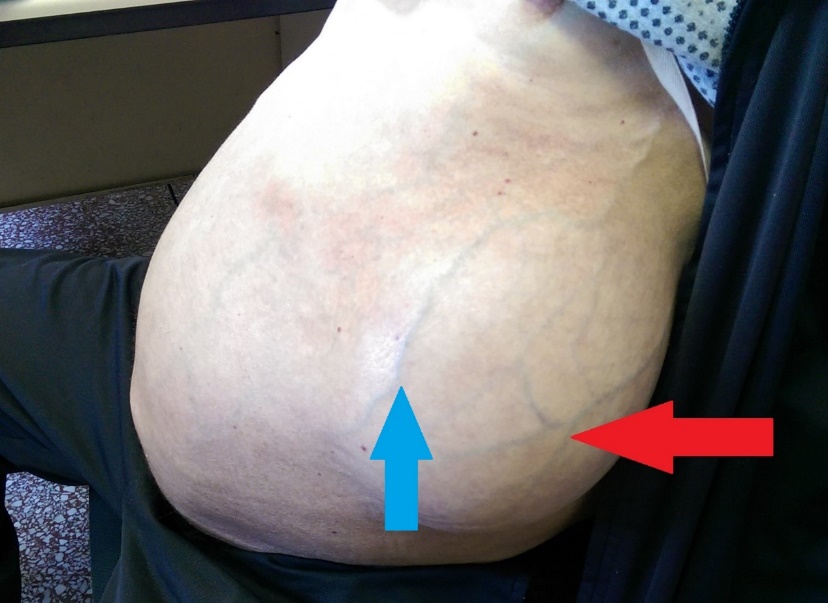
Blue arrow - Caput Medusae.Red arrow - Intercostal hernia.(Courtesy Dr. V. Penopoulos).
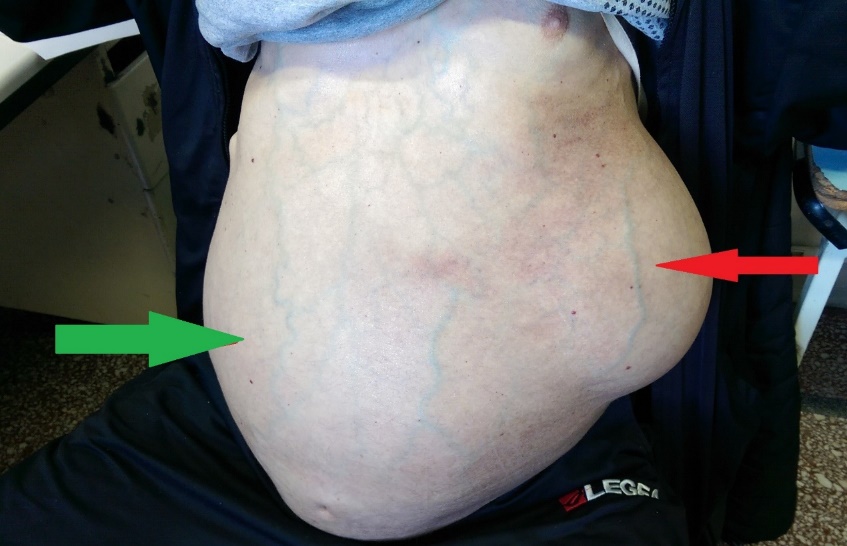
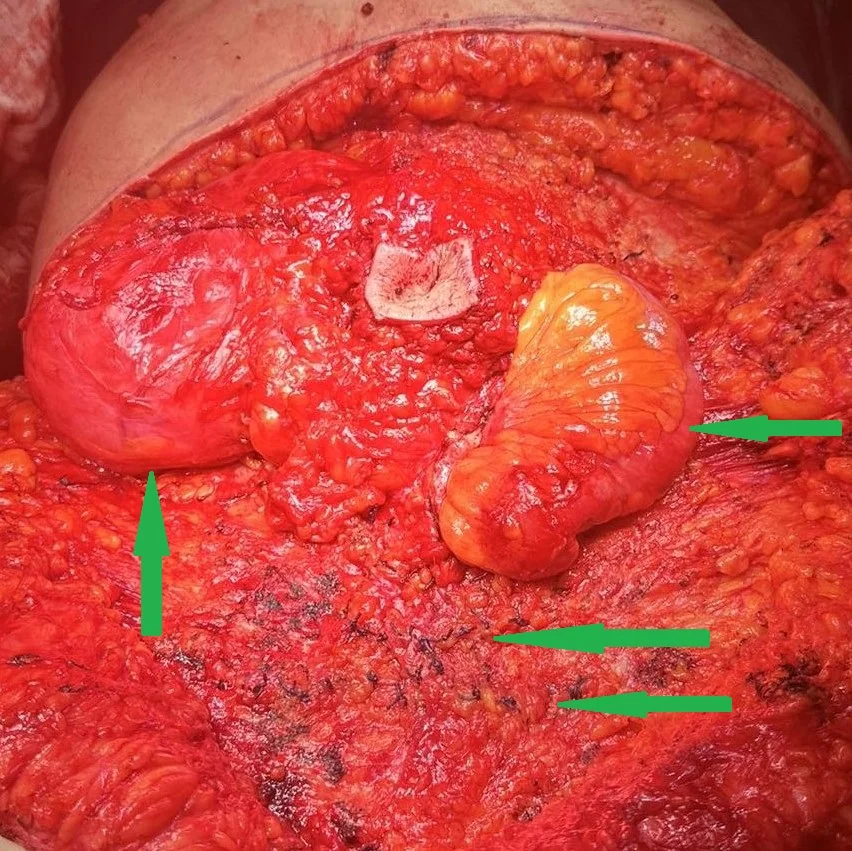
Green arrow - Ascites.Red arrow - Intercostal hernia.(Courtesy Dr. V. Penopoulos).
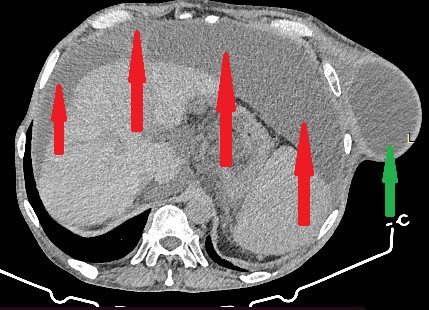
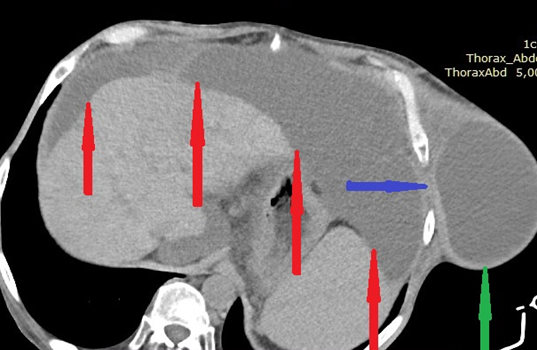
Red arrows - Ascites.Green arrow - Intercostal hernia.(Courtesy Dr. V. Penopoulos).
08.02
Umbilical Hernia
(16 images)
UMBILICAL HERNIA
Other2025

UMBILICAL HERNIA
Other2010

UMBILICAL HERNIA
Other2017

UMBILICAL HERNIA
Other2022

UMBILICAL HERNIA
Other2019

UMBILICAL HERNIA
Other2017

UMBILICAL HERNIA
Other2015

UMBILICAL HERNIA
Other2011

UMBILICAL HERNIA
Other2013

UMBILICAL HERNIA
Other2011

UMBILICAL HERNIA
Other2006

UMBILICAL HERNIA
Other2003

UMBILICAL HERNIA
Imaging2002

TRANSMESENTERIC HERNIA
Open1995

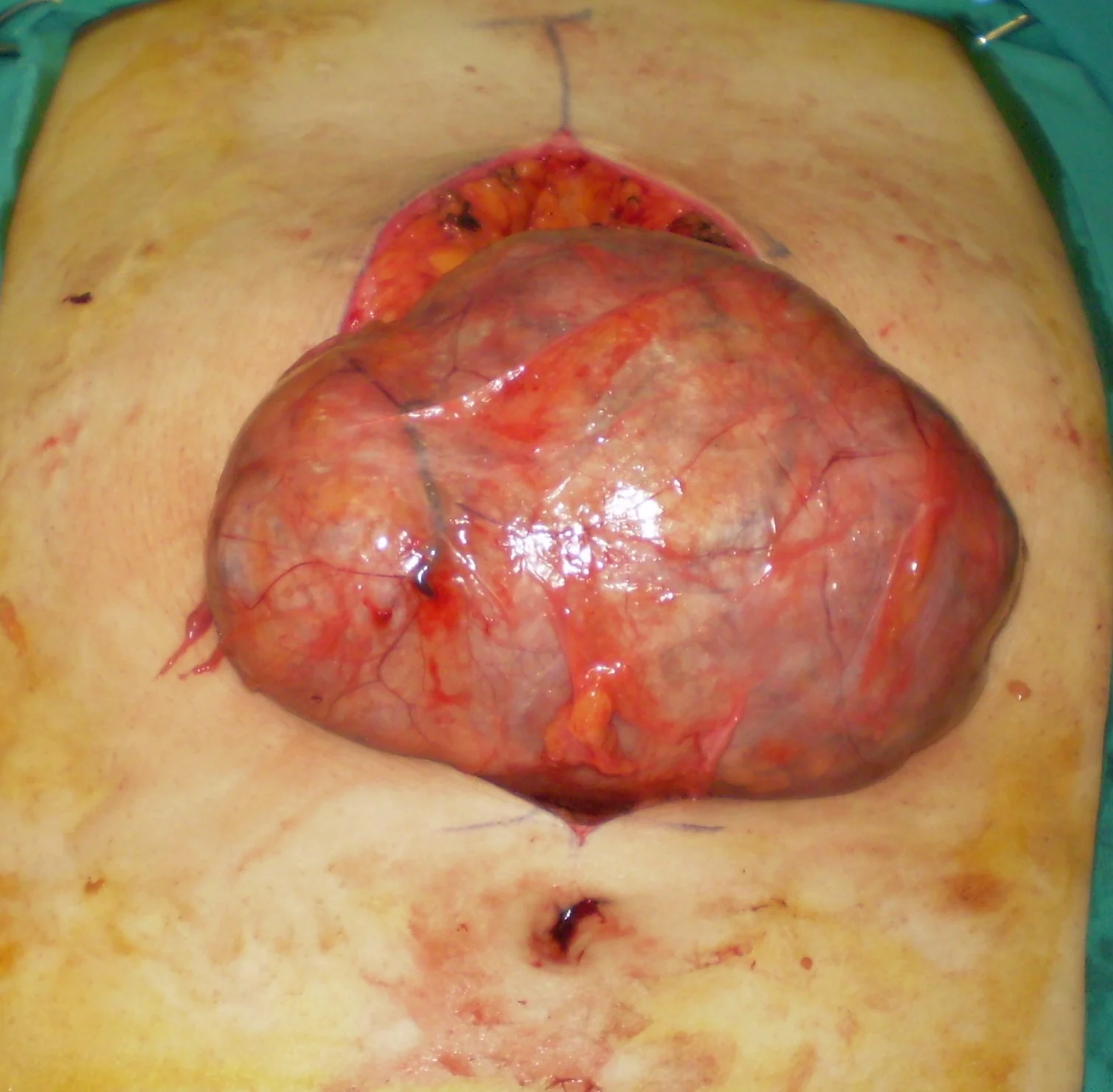
HUGE UMBILICAL HERNIA
Open1996
08.03
Rare Hernias
(48 images)
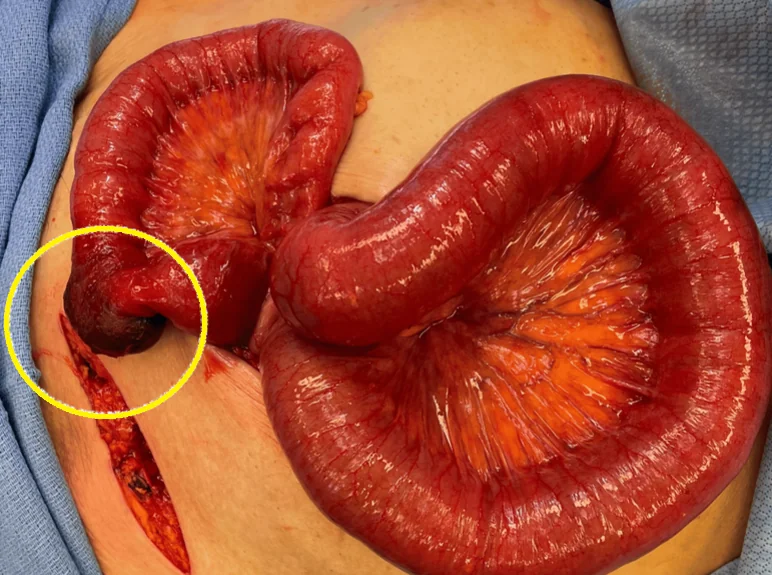
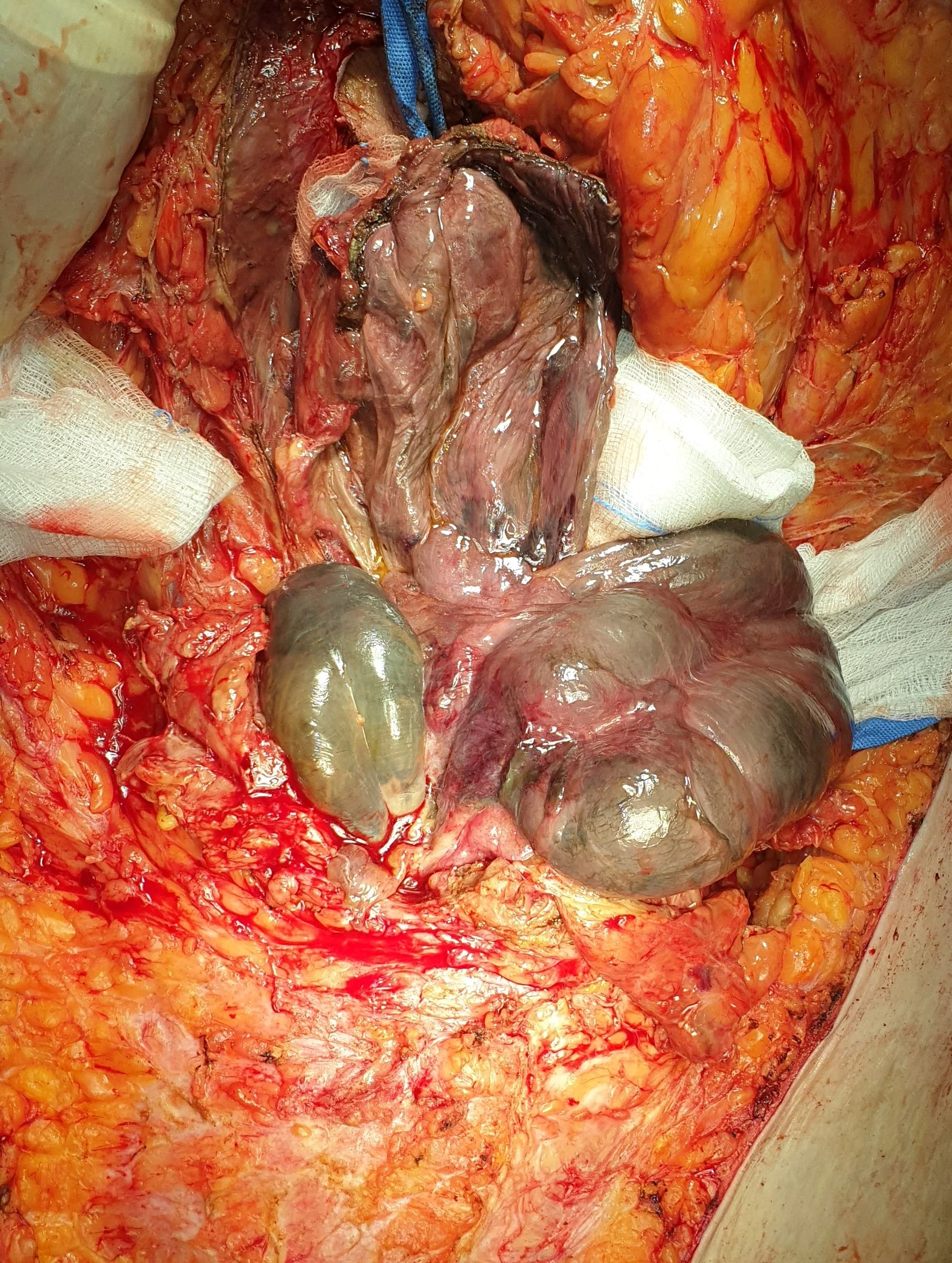
PERINEAL HERNIA - INTESTINAL NECROSIS
Open2005

PERINEAL HERNIA REPAIR - MESH
Open2002

PERINEAL HERNIA
Imaging2009

PERINEAL HERNIA
Imaging2006

PERINEAL HERNIA
Imaging2002

PERINEAL HERNIA
Imaging1997

PERINEAL HERNIA - URINARY BLADDER
Imaging2004
INTERPARIETAL HERNIA
Open2007
INTERPARIETAL HERNIA
Open2005
INTERPARIETAL HERNIA
Imaging2007
INTERPARIETAL HERNIA
Imaging2005
DE GARENGEOT'S HERNIA
Laparoscopic2013
DE GARENGEOT'S HERNIA
Imaging2011

DE GARENGEOT'S HERNIA
Imaging2004

REDUCED DE GARENGEOT'S HERNIA
Laparoscopic2004
DE GARENGEOT'S HERNIA
Laparoscopic2004

OGILVIE'S HERNIA - URINARY BLADDER
Open2006

OBTURATOR FORAMEN HERNIA
Open2000
RICHTER'S HERNIA - ILEUM PERFORATION
Open2009
RICHTER'S HERNIA
Imaging2009

RICHTER'S HERNIA
Imaging2015
REDUCED RICHTER'S HERNIA
Laparoscopic2015

RICHTER'S HERNIA - OBTURATOR FORAMEN
Open2005

RICHTER'S HERNIA
Imaging2002

RICHTER'S HERNIA
Imaging1998

LITTRE'S HERNIA
Laparoscopic2022

LITTRE'S HERNIA
Imaging1999

LITTRE'S HERNIA
Imaging2000

LITTRE'S HERNIA
Imaging1997

AMYAND'S HERNIA
Imaging2022
AMYAND'S HERNIA
Imaging2008

AMYAND'S HERNIA
Imaging2011

AMYAND'S HERNIA
Imaging2011

INCARCERATED AMYAND'S HERNIA
Laparoscopic2014

AMYAND'S HERNIA
Laparoscopic2011
AMYAND'S HERNIA
Laparoscopic2008
08.01
Inguinal Hernias-Epigastric Hernias-Abdominal Hernias
(52 images)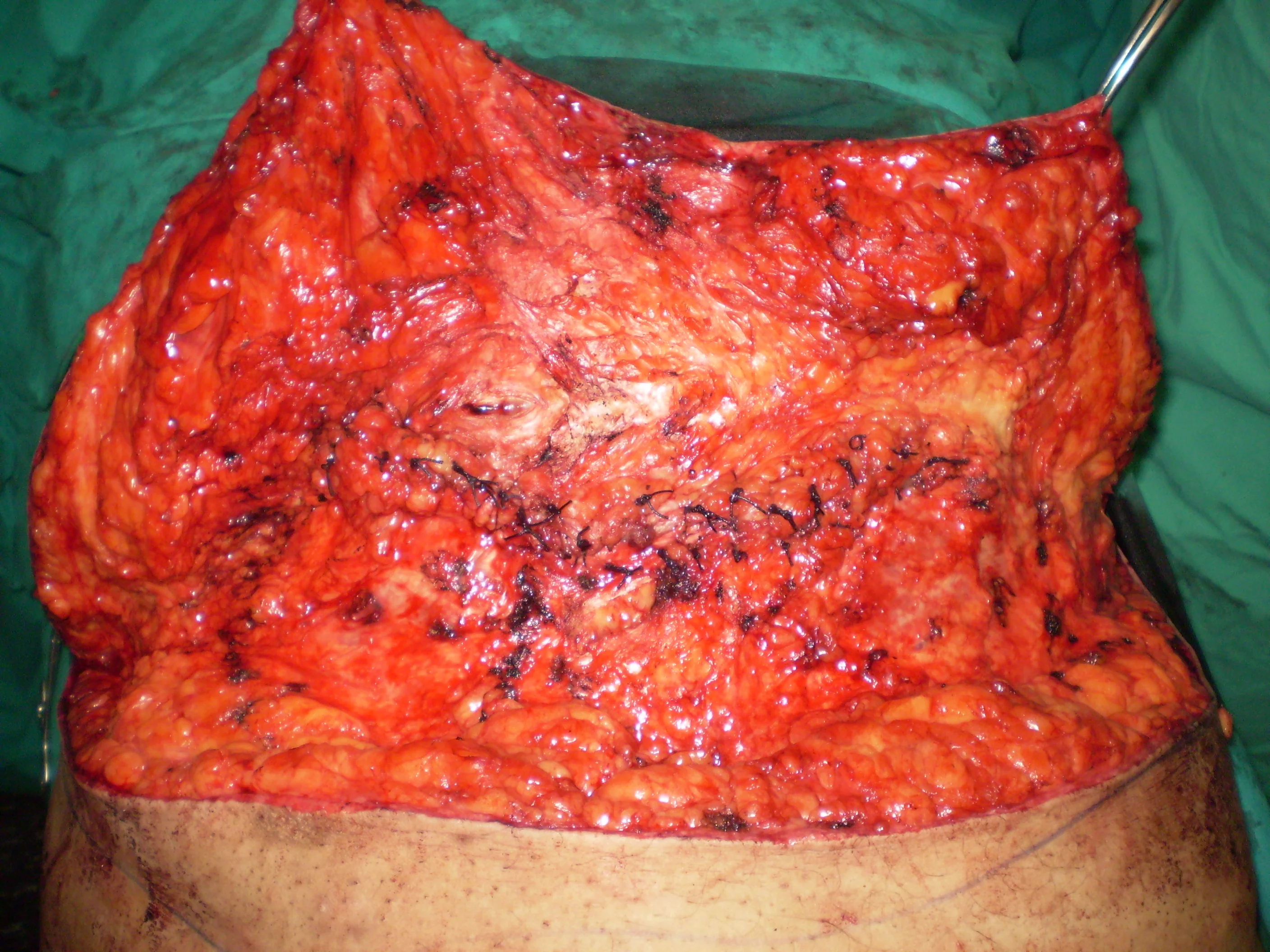
HERNIAL DEFECT CLOSURE
Open2001
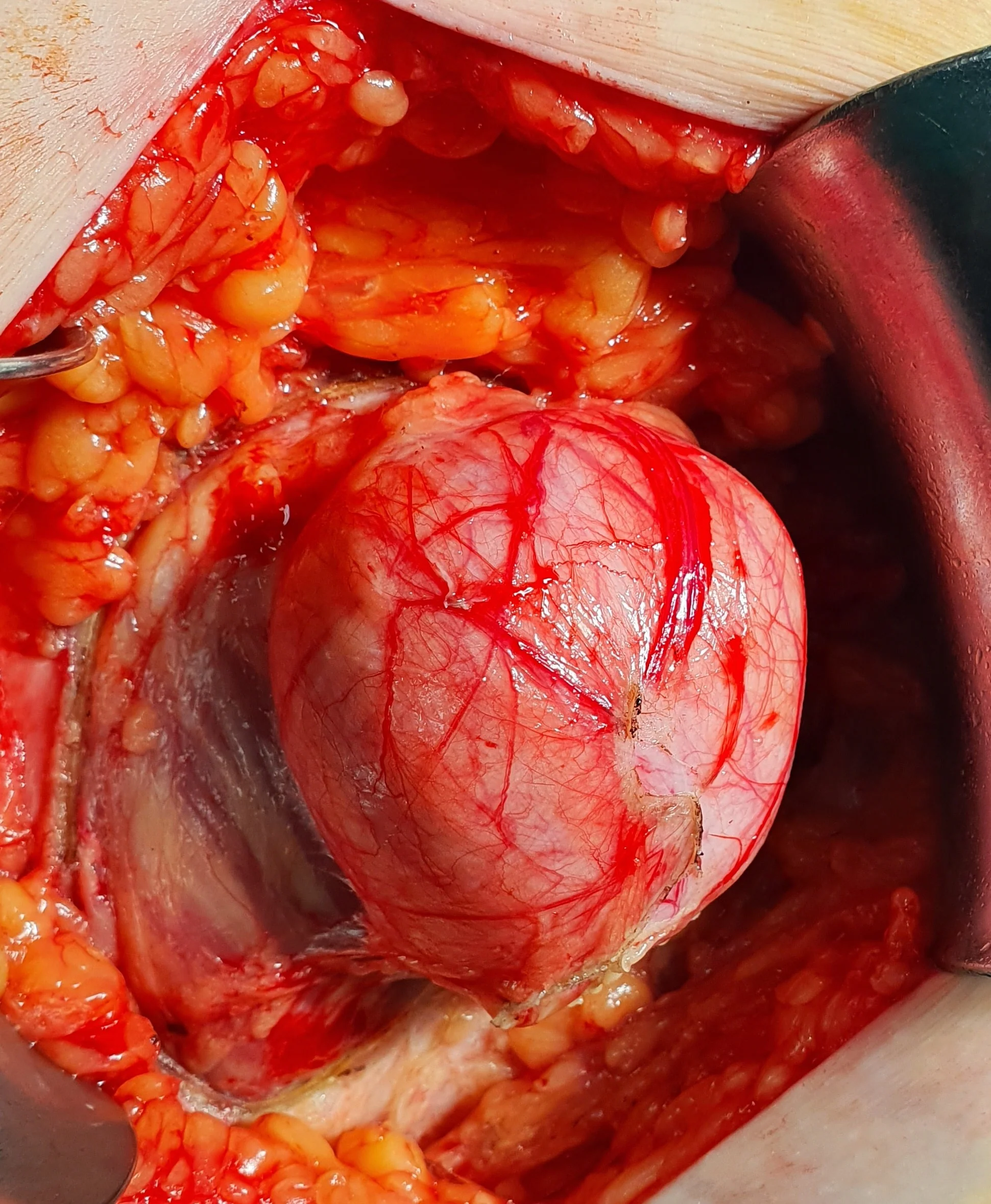
SIZEABLE HERNIAL SAC
Open2000
MULTIPLE ABDOMINAL HERNIAS
Open2000
RECURRENT ABDOMINAL HERNIA REPAIR
Open1999

STRANGULATED HERNIA
Imaging1994
NO TENSION INGUINAL HERNIA REPAIR
Open1991

POST INGUINAL HERNIA REPAIR HEMATOMA
Laparoscopic

ABDOMINAL HERNIA REPAIR - ABDOMINOPLASTY
Open2000

ABDOMINAL HERNIA - ABDOMINAL APRON
Open2000
INCISIONAL HERNIA
Open2000

STRANGULATED INCISIONAL HERNIA - ΙΝΤΕΣΤΙΝΑΛ ΝΕΨΡΟΨΙΣ
Open2003

STRANGULATED INCISIONAL HERNIA - NECROTIC BOWEL
Open2000
STRANGULATED INCISIONAL HERNIA - NECROTIC BOWEL
Open2003

STRANGULATED INCISIONAL HERNIA
Open2003
PETERSEN SPACE HERNIA
Open2000

PETERSEN SPACE HERNIA
Imaging2000

STRANGULATED RICHTER'S HERNIA
1995

STRANGULATED RICHTER'S HERNIA
Open1995

EPIGASTRIC HERNIA
Open1990
SYNCHRONOUS INGUINAL HERNIA + HYDROCELE
Open1995

GIANT INGUINOSCROTAL HERNIA
Open1994
DOUBLE LAYER MESH
Other1996
INGUINAL HERNIA - DISSECTION OF HERNIAL SAC
Open1994
NO TENSION INGUINAL HERNIA REPAIR WITH MESH
Open1994
SYNCHRONOUS INDIRECT + DIRECT HERNIAS
Open1994
INGUINAL HERNIA REPAIR
Open1991

INGUINAL HERNIA - BOWEL IN THE SCROTUM
Imaging1991

INGUINAL HERNIA - AIR IN THE SOFT TISSUES
Imaging1990

INGUINAL HERNIA - HERNIA TRUSS
Open1993

SIZEABLE INGUINOSCROTAL HERNIA
Open2000

INGUINAL HERNIA - BOWEL IN THE CANAL
Imaging1997
INGUINAL HERNIA REPAIR
Laparoscopic2002

INFLAMMED INGUINAL HERNIA
Open2000

GIANT INGUINOSCROTAL HERNIA - SCROTAL ULCER
Open2001

GIANT INGUINOSCROTAL HERNIA - POST OP SEROMA
Open2000

GIANT INGUINOSCROTAL HERNIA
Open1998

ENORMOUS INGUINAL HERNIA
Open1997

ENORMOUS INGUINAL HERNIA
Open1995