Endocrine Glands
Ενδοκρινείς Αδένες
513 images · 3 sub-chapters
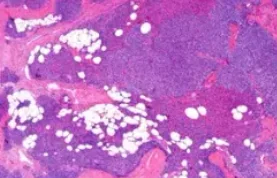
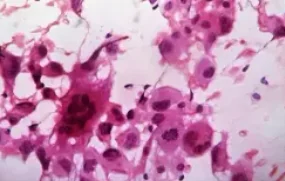
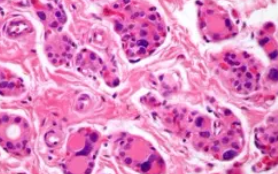
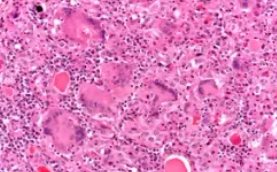
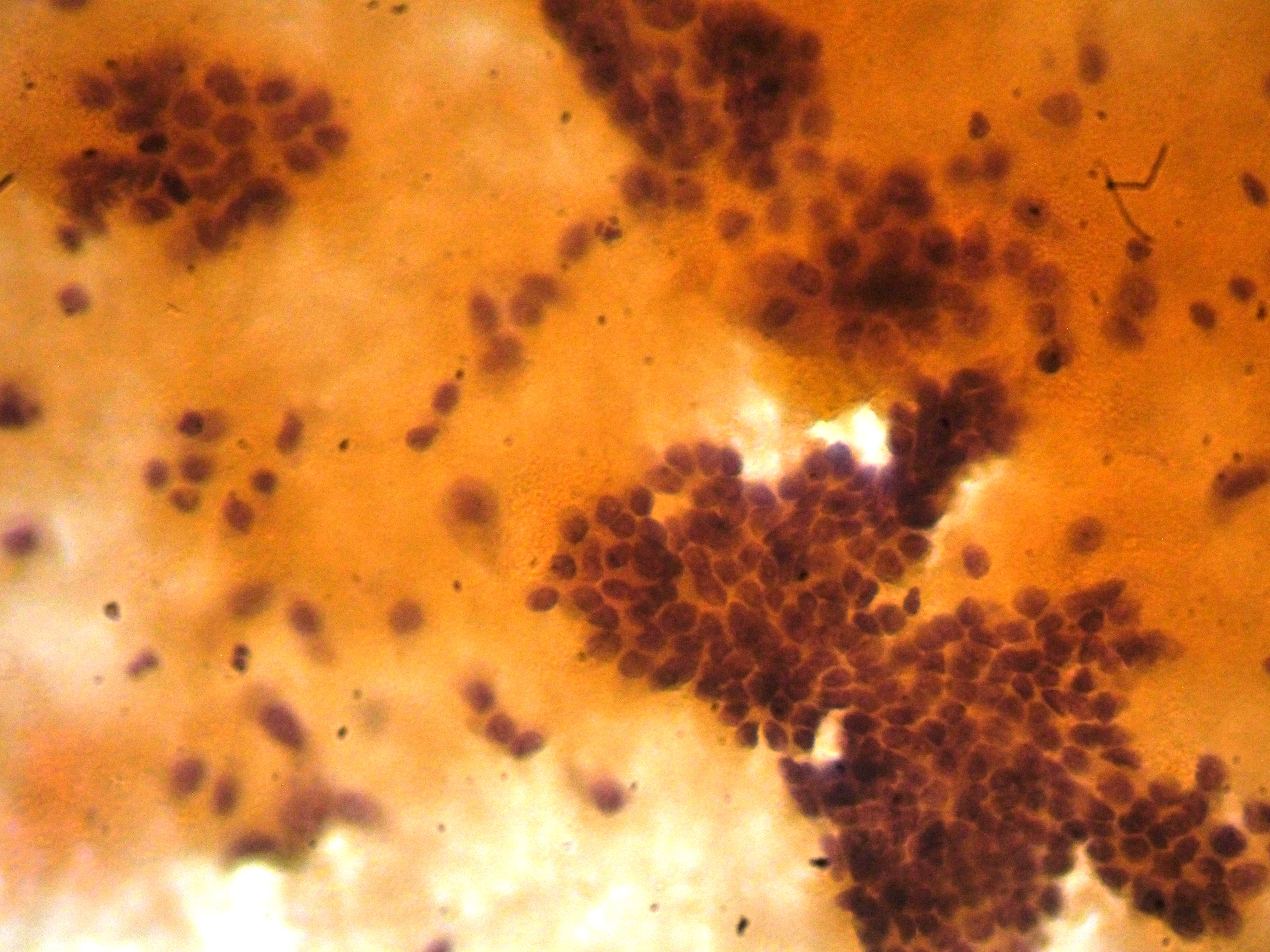
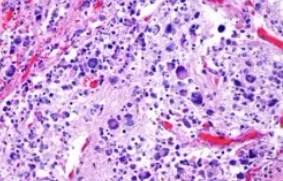
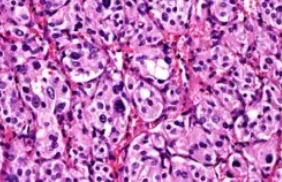
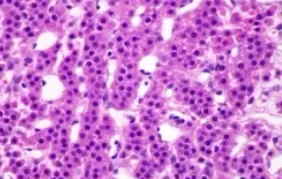
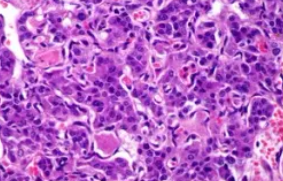
Hürthle cells, exhibiting the characteristic eosinophilic, granular cytoplasm.(Courtesy Dr.V.Penopoulos).

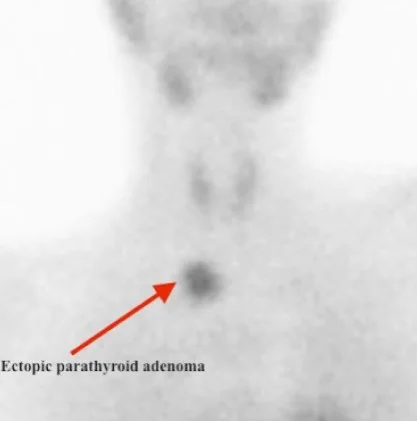
Negative Tc-99m sestamibi Scan for the demonstration of a parathyroid adenoma.(Courtesy Dr.V.Penopoulos).

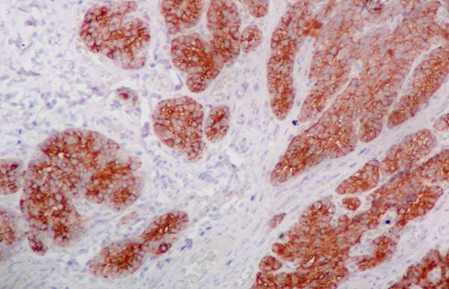
Immunohistochemical evaluation demonstrated positivity for parathyroid hormone and chromogranin, with low mitotic and proliferative activity (Courtesy Dr. V. Penopoulos)


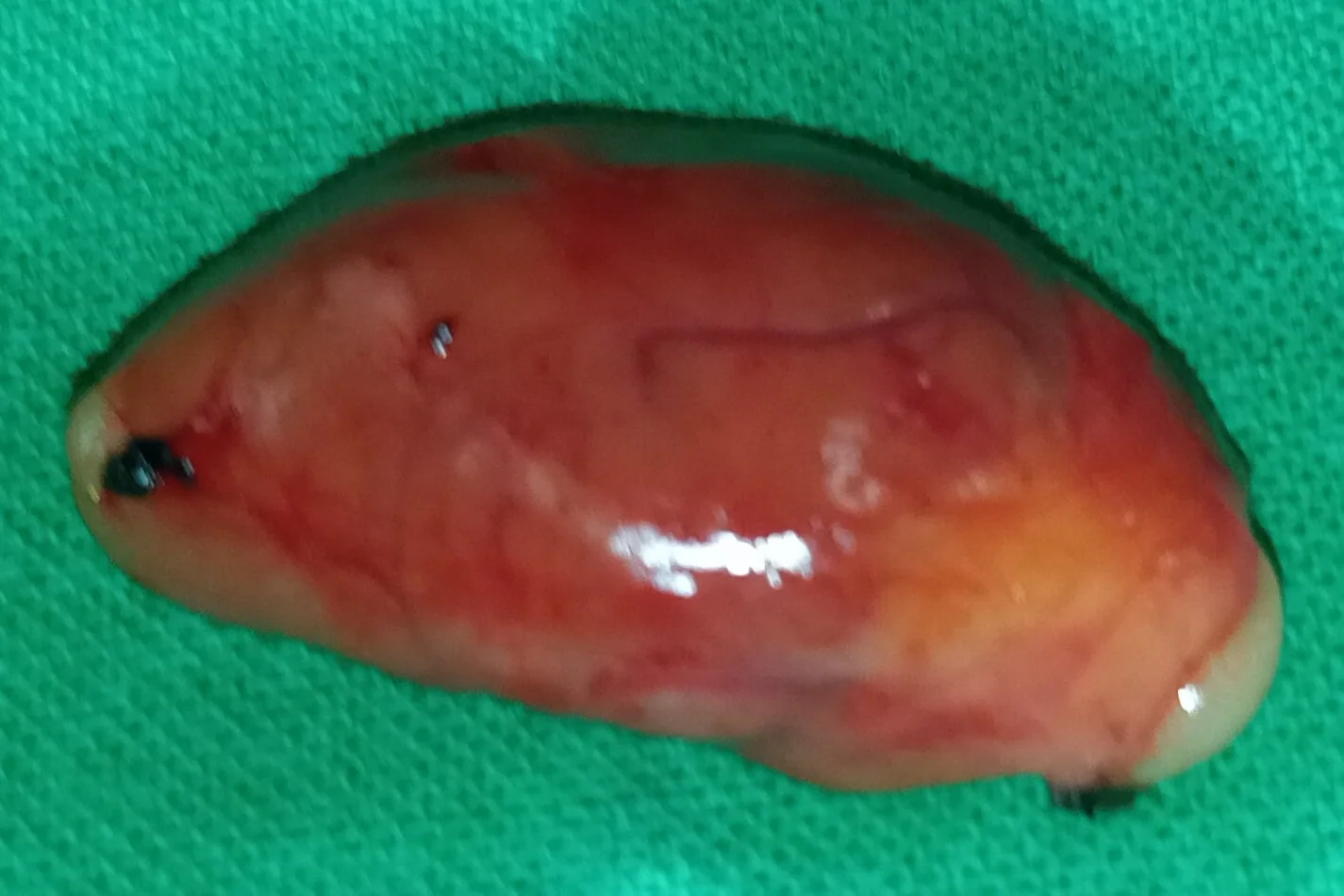
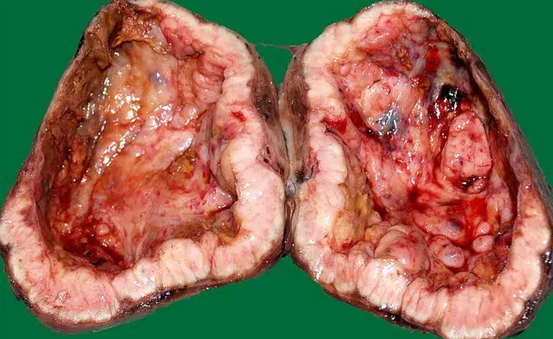
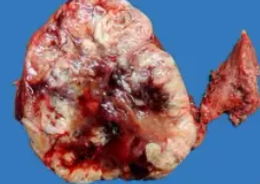
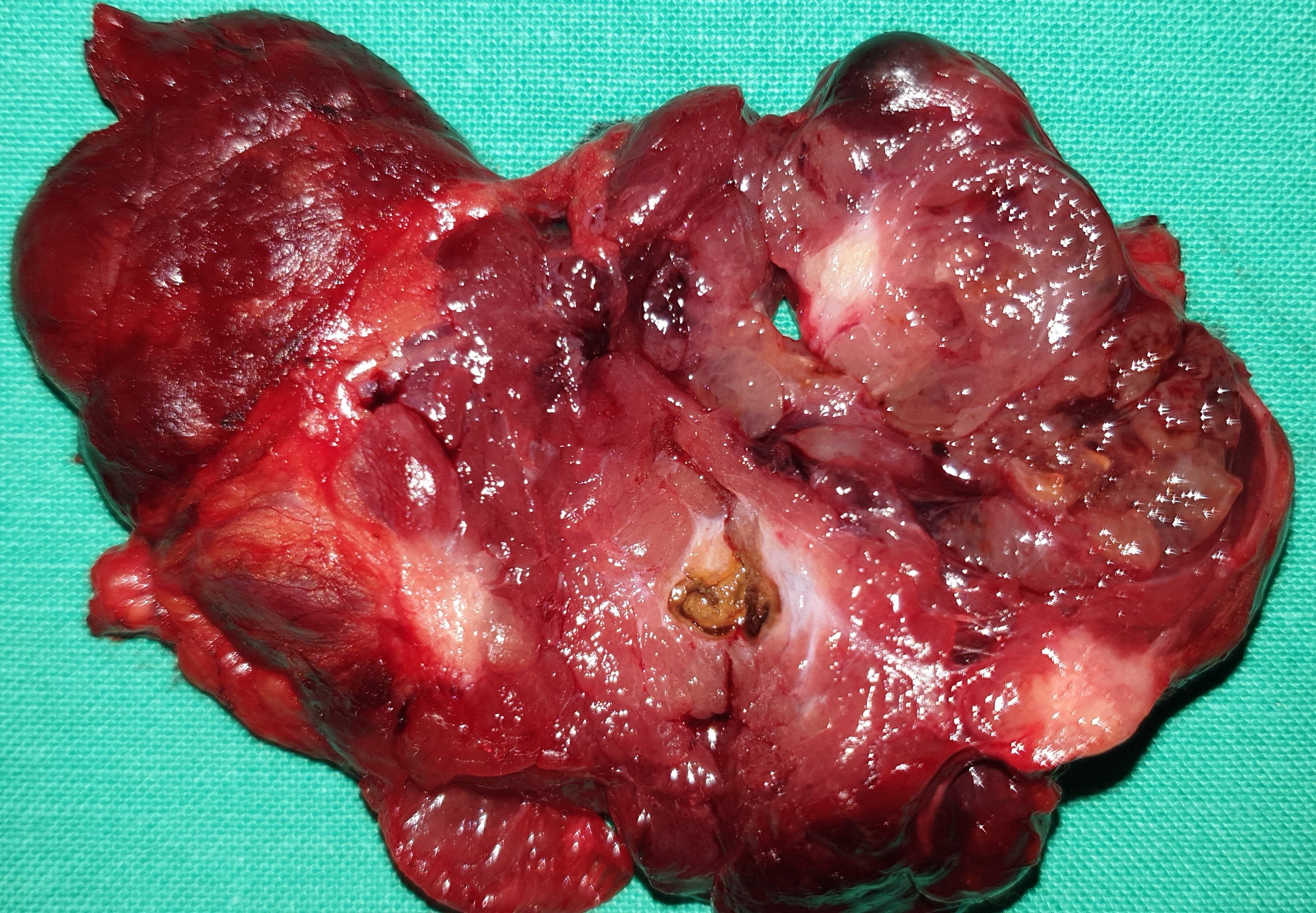
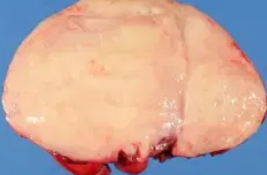
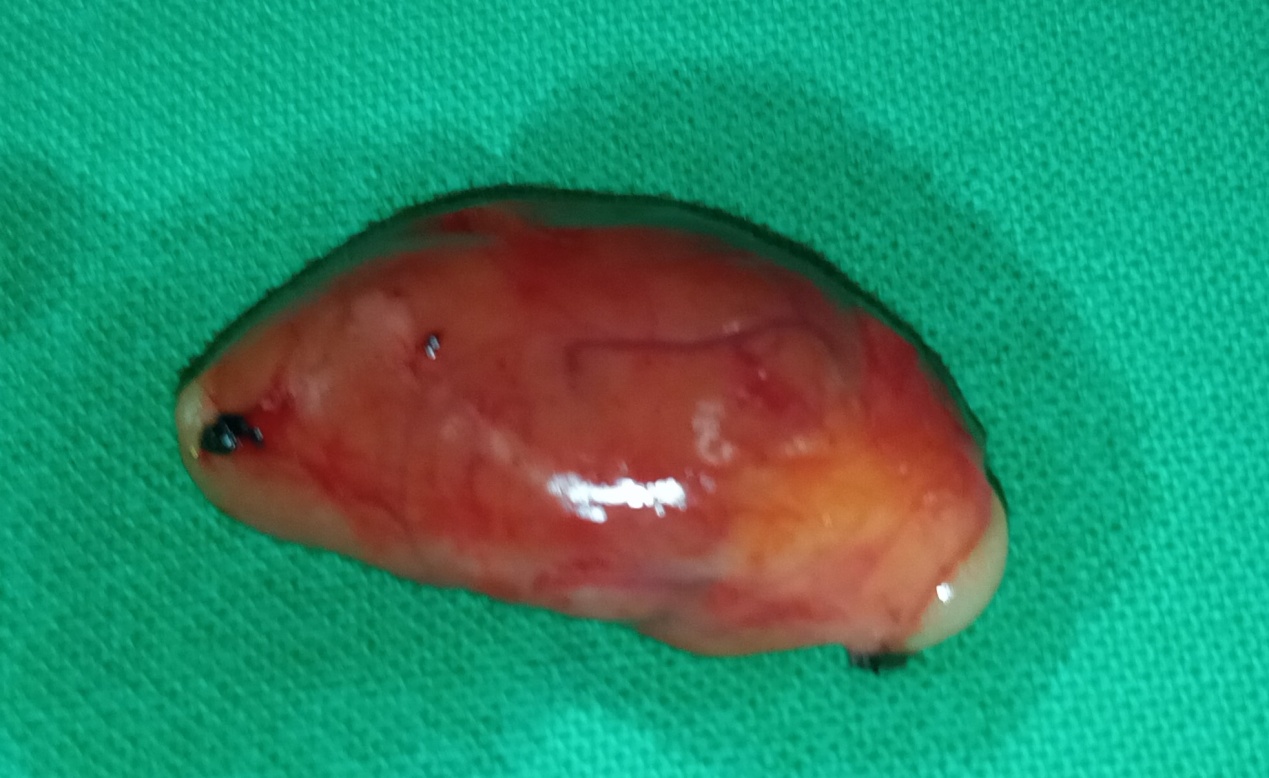
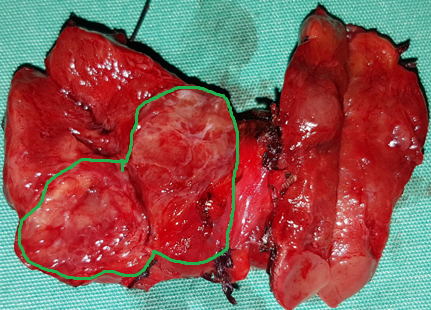
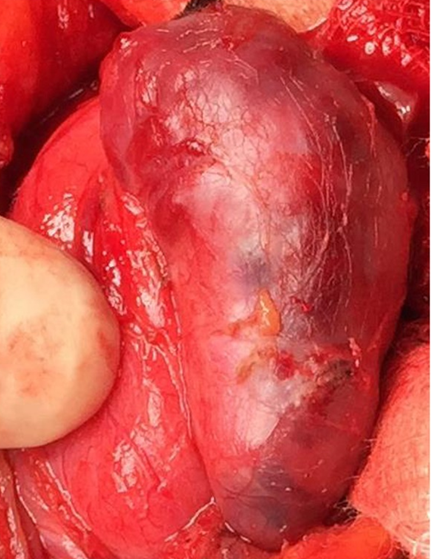
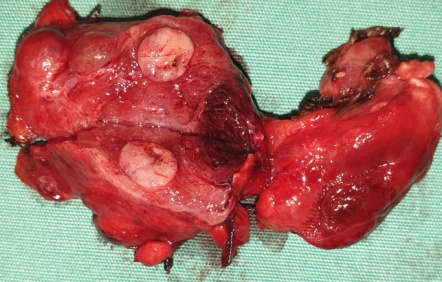
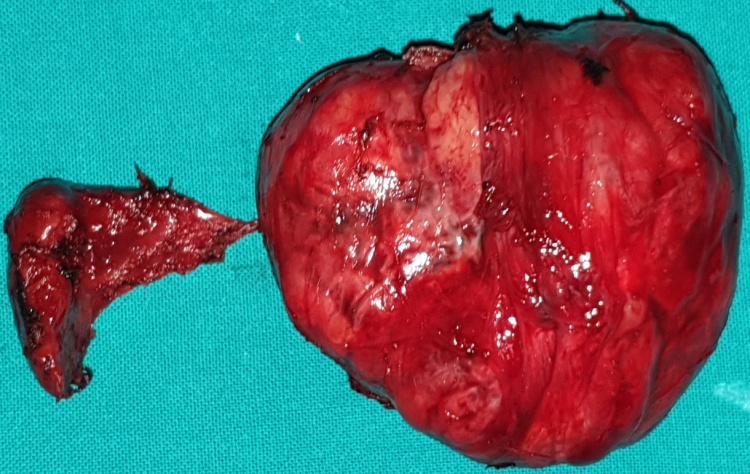
Specimen of an opened cystic parathyroid adenoma.The remaining turbid fluid within the opened cystic cavity is visible.(Courtesy Dr. V. Penopoulos).

Hürthle cells, exhibiting the characteristic eosinophilic, granular cytoplasm.(Courtesy Dr.V.Penopoulos).
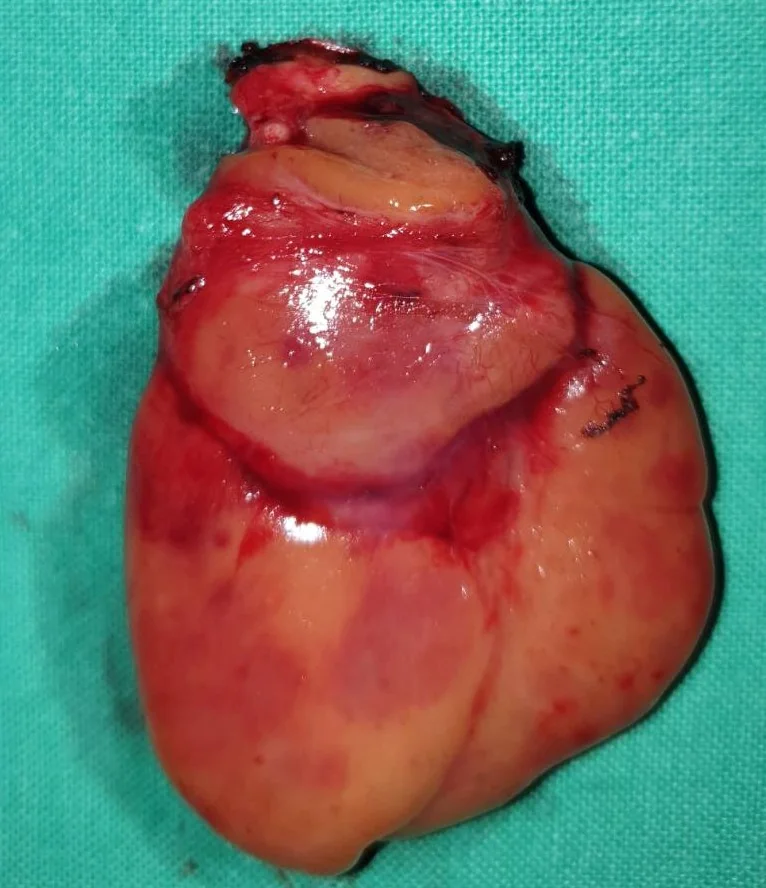
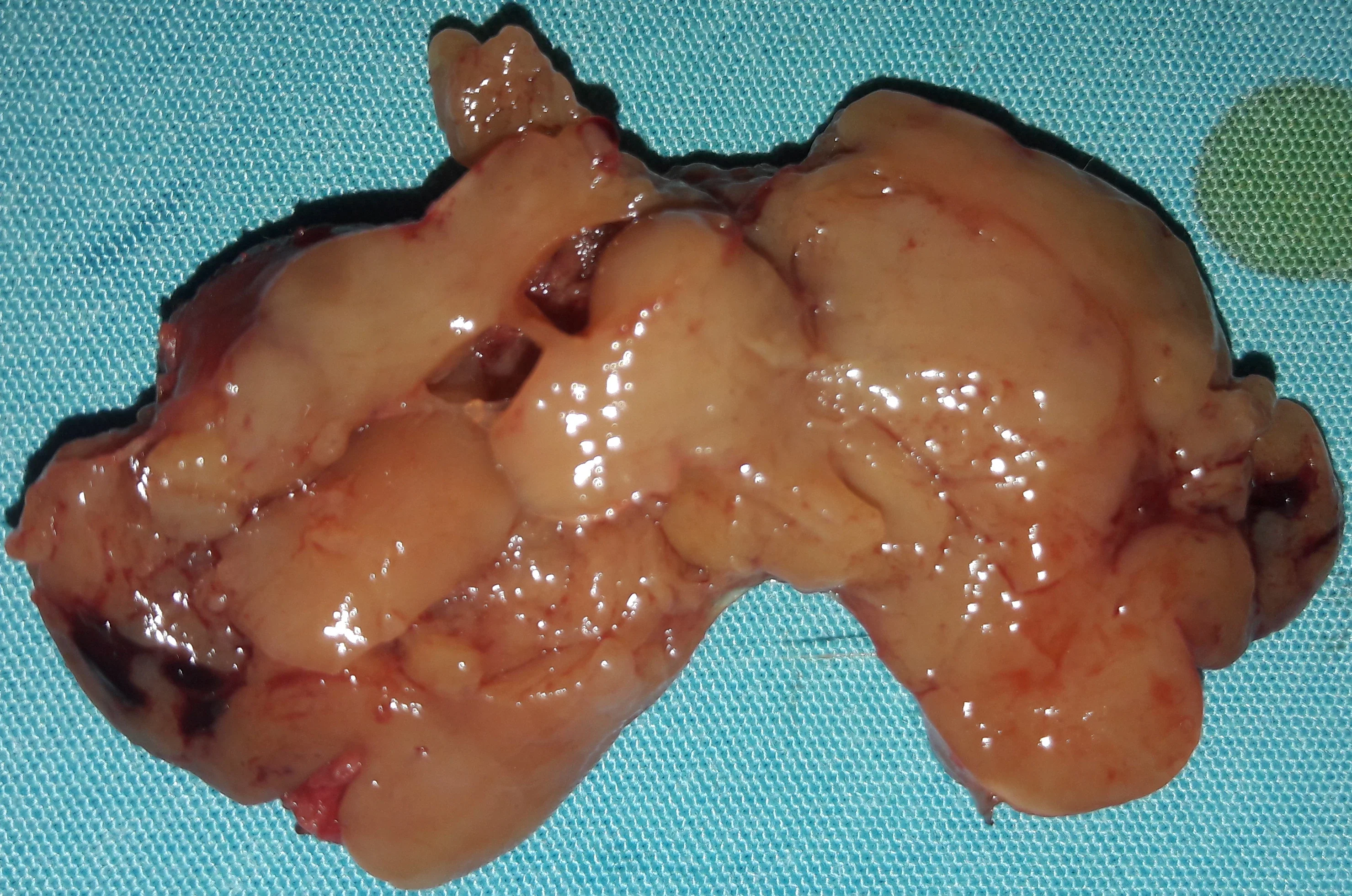
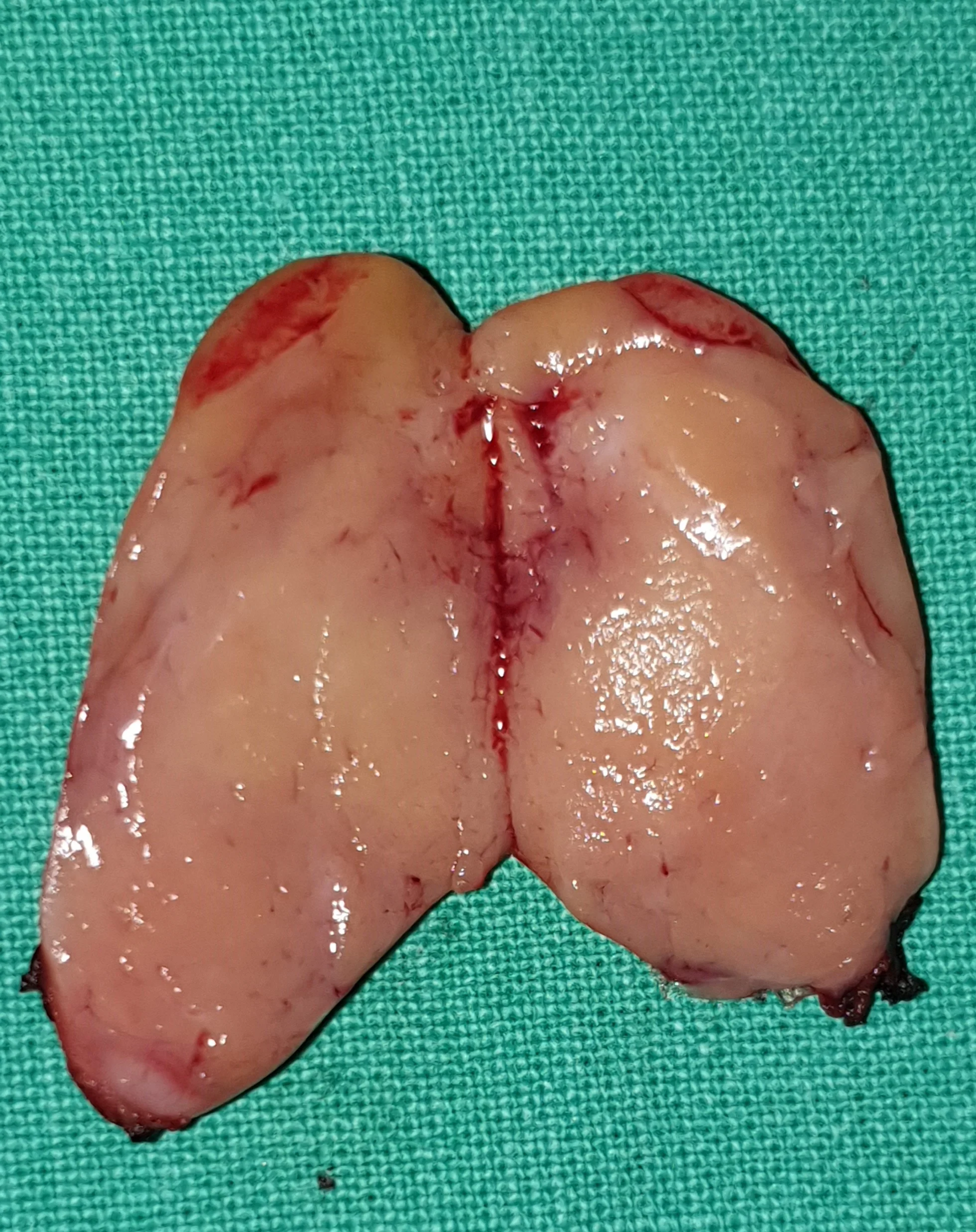
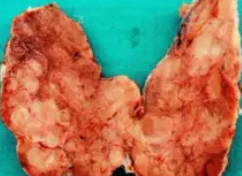
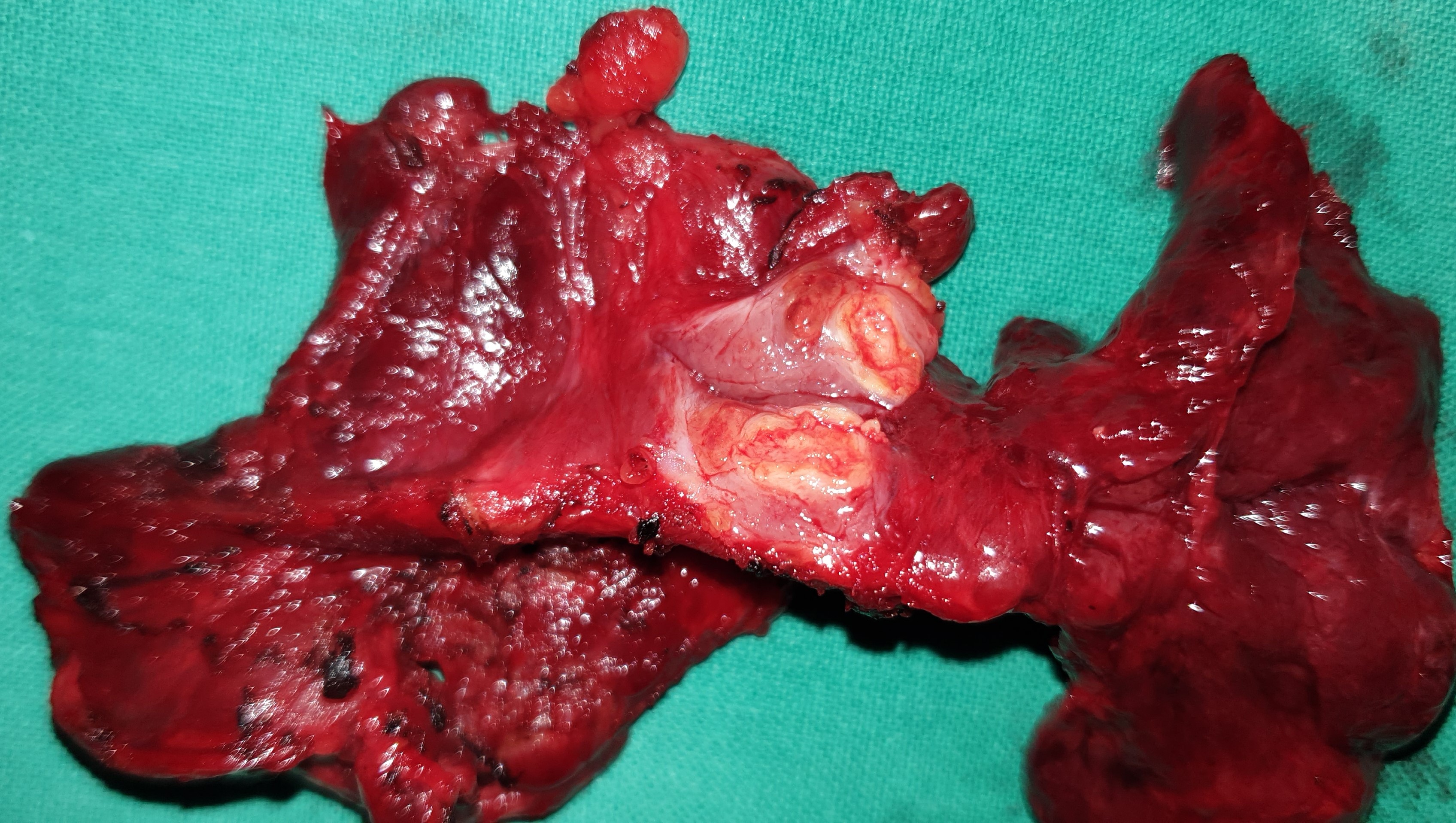
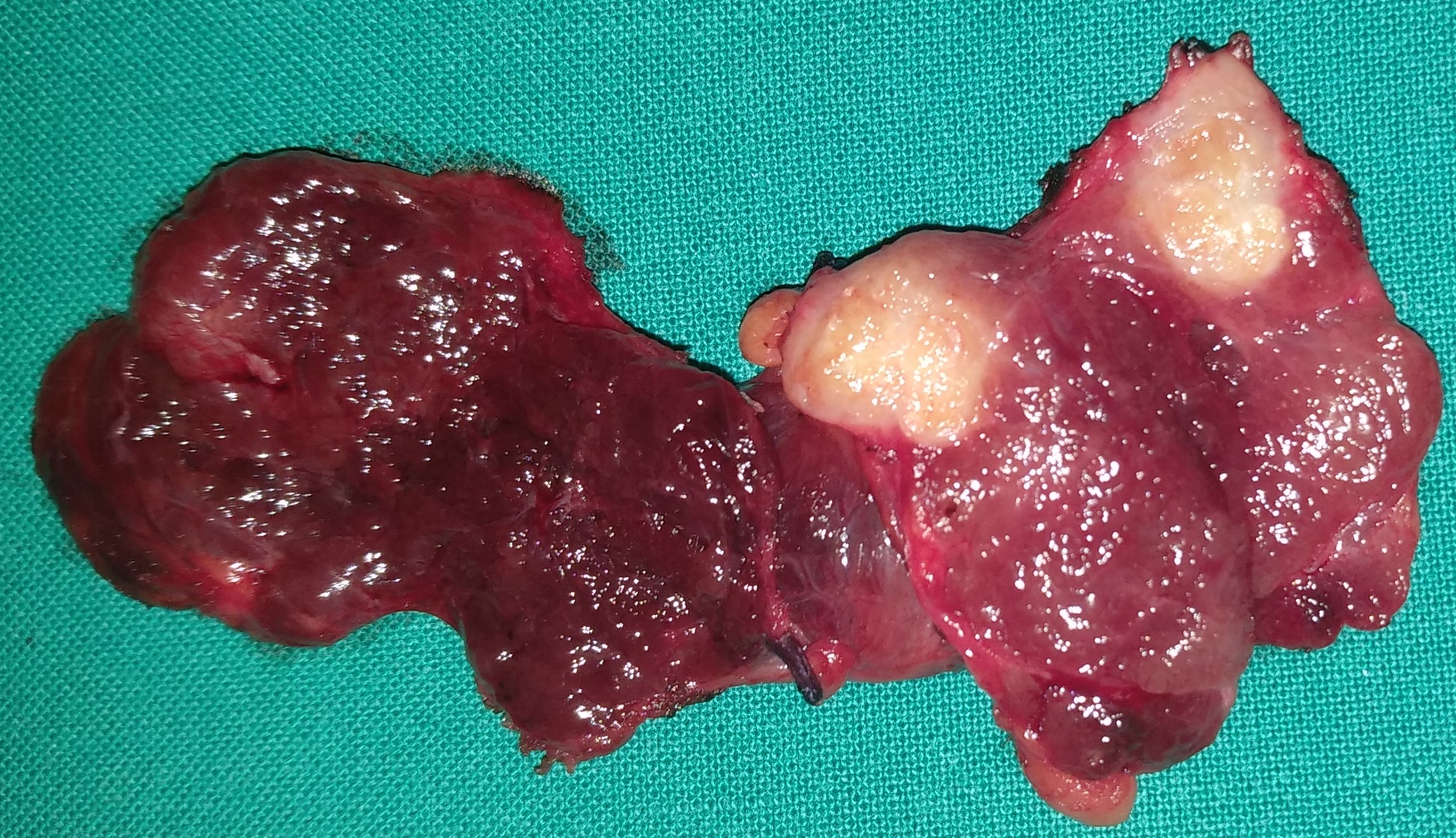
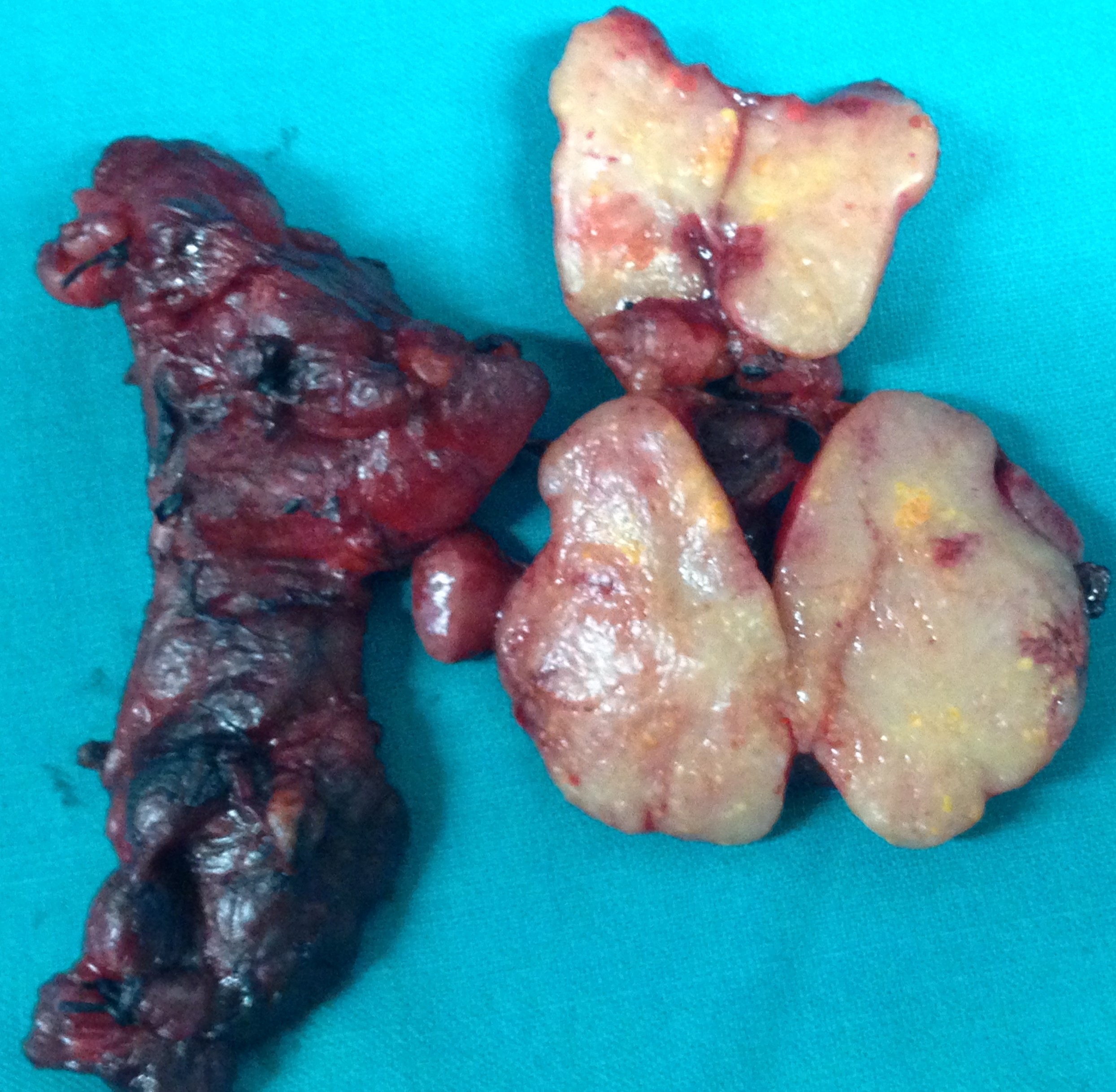
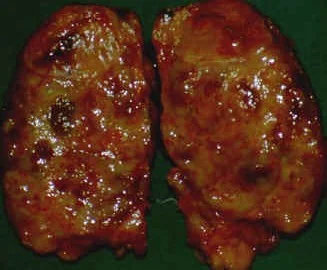
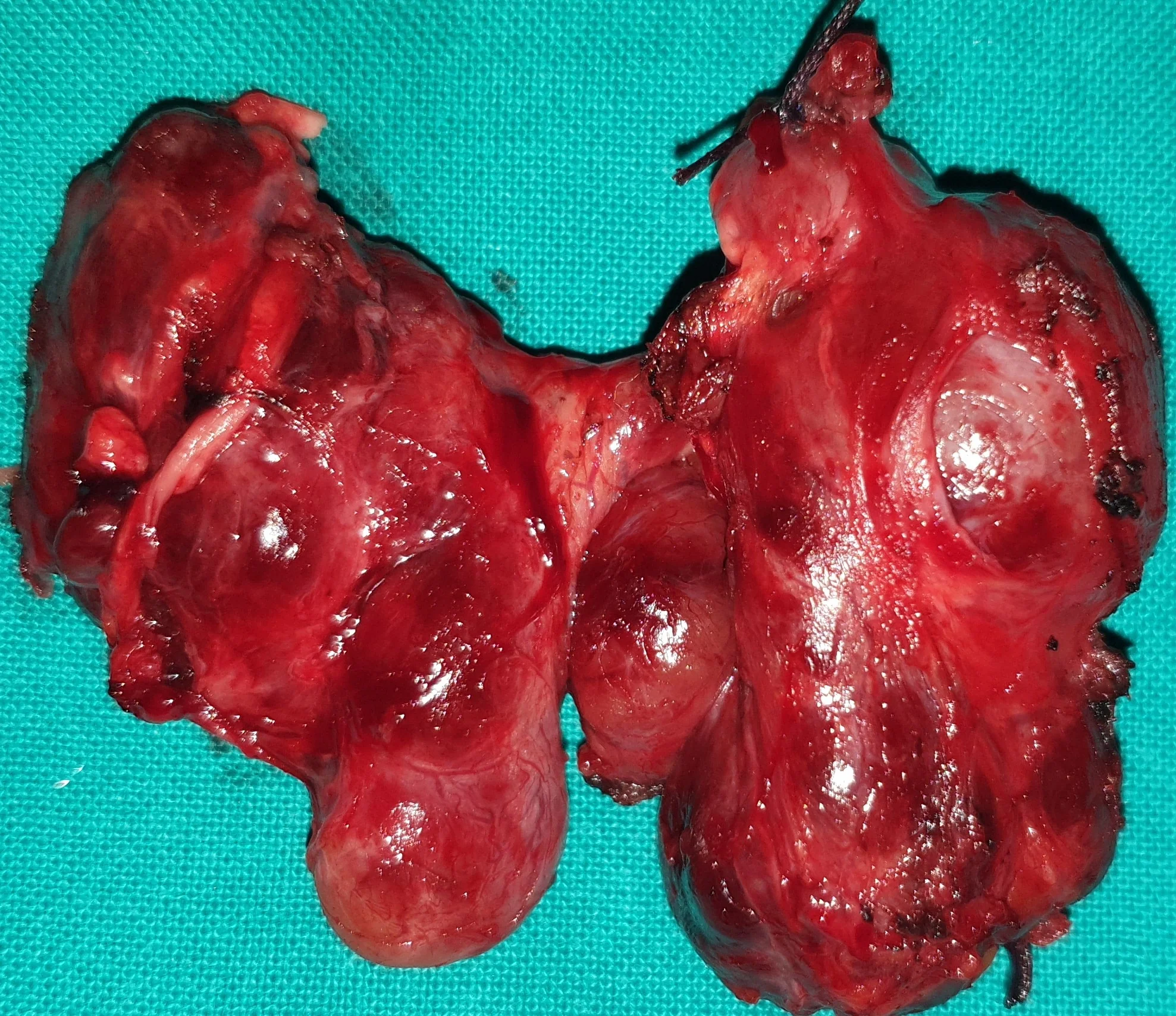
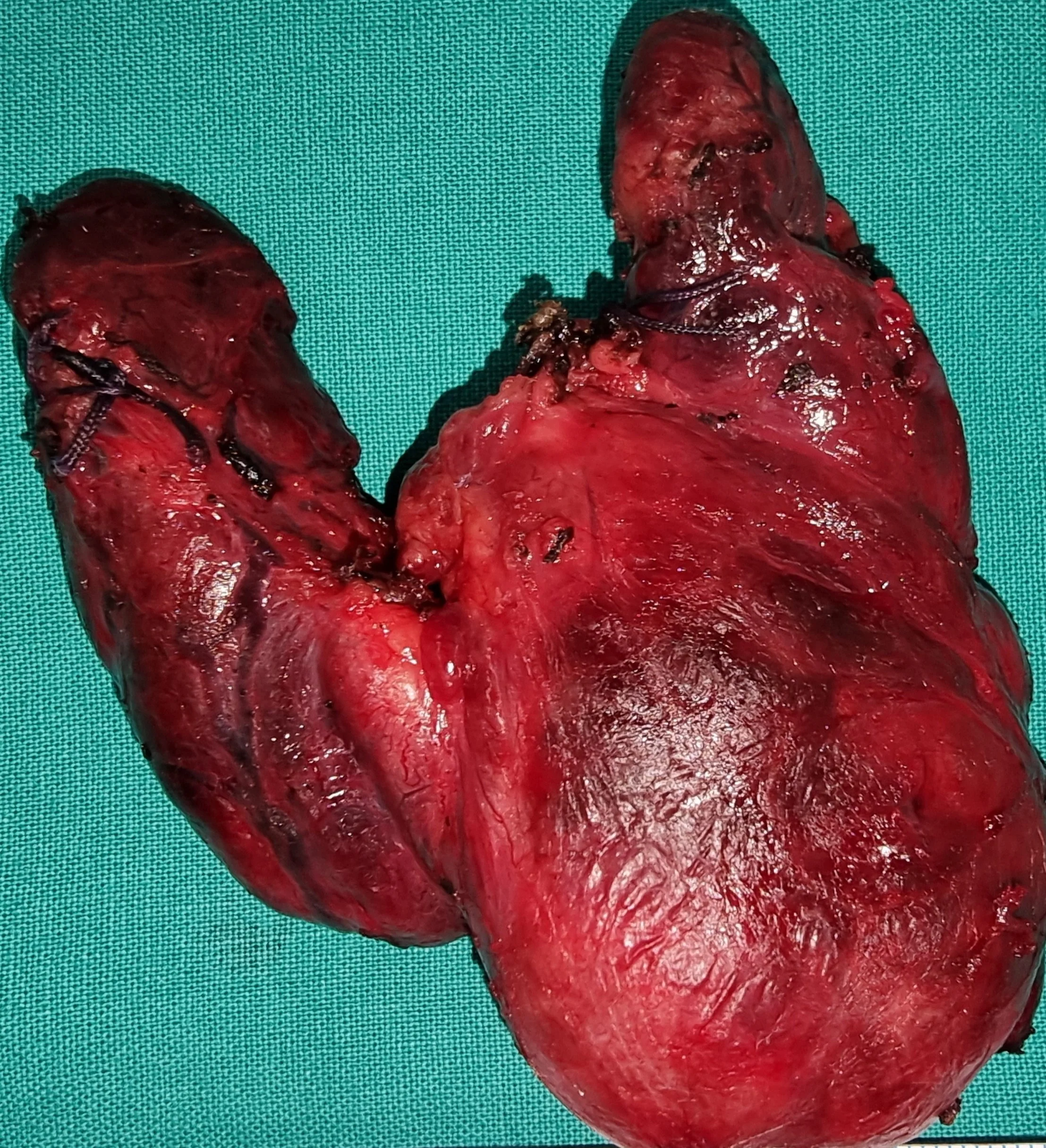
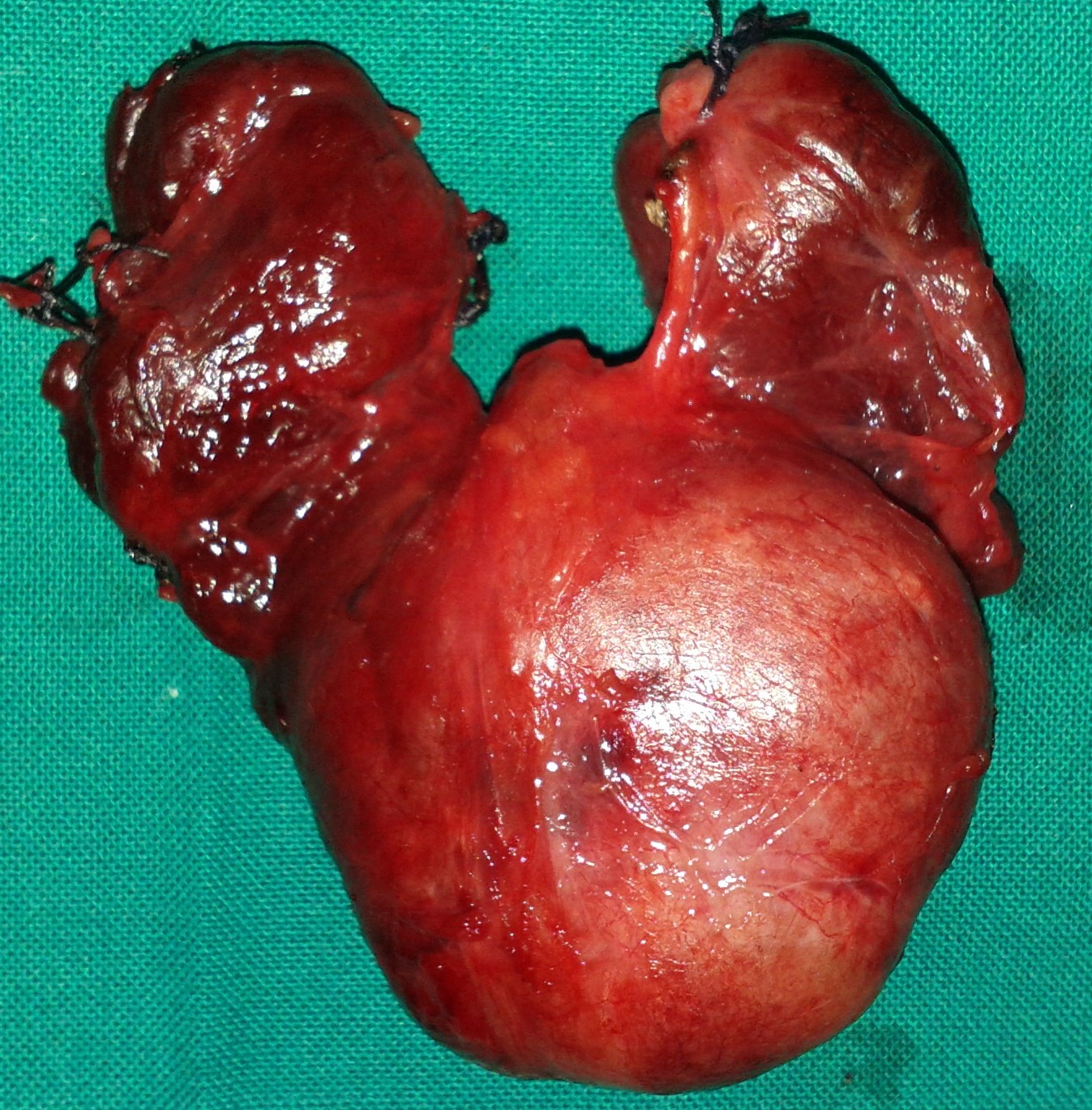
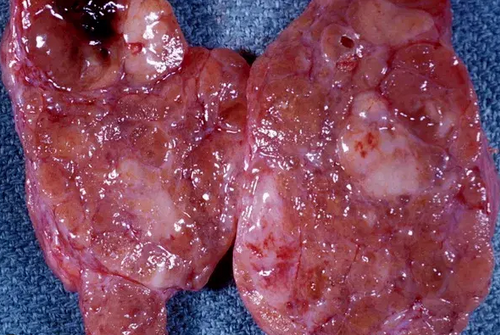
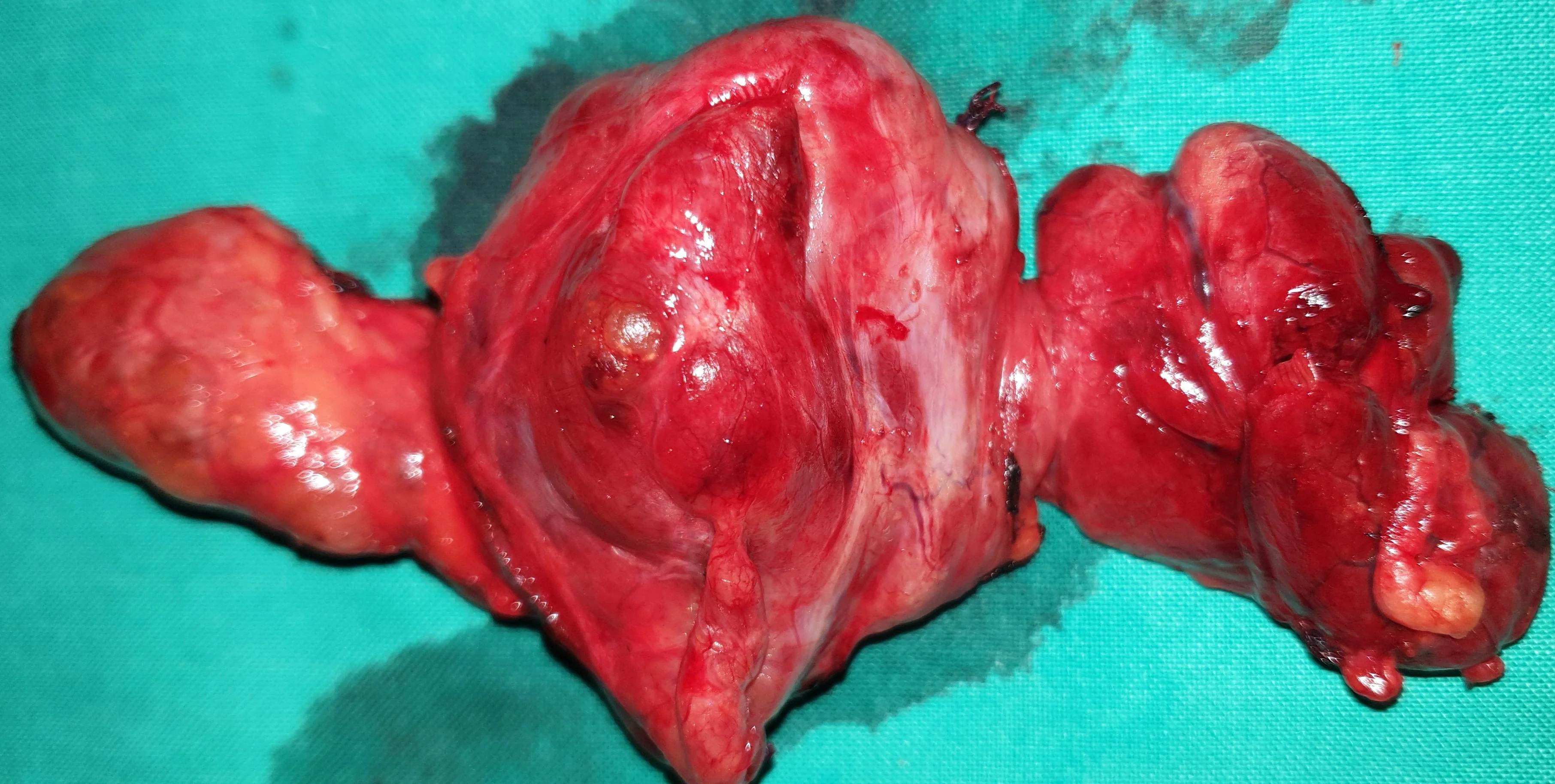
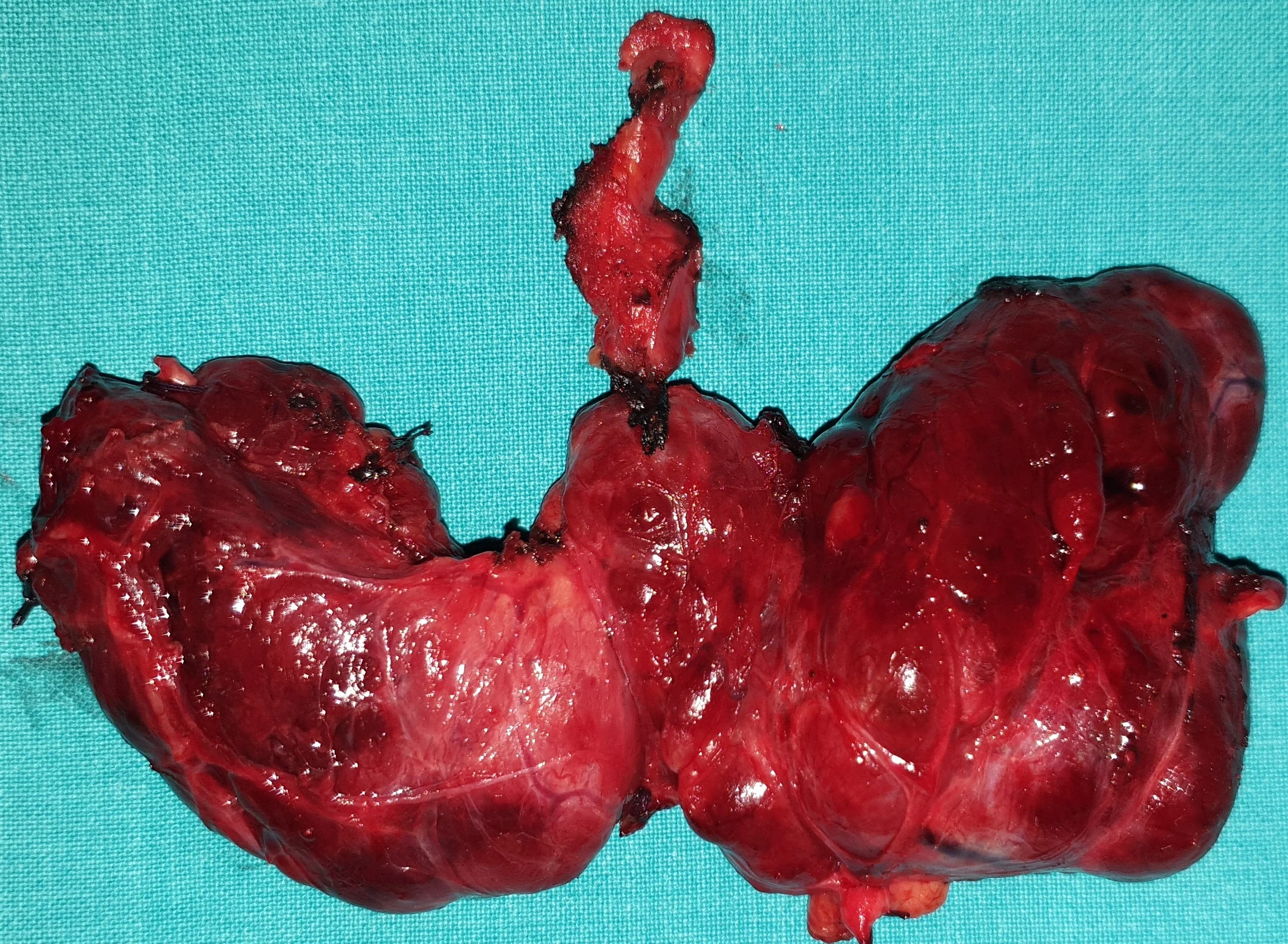
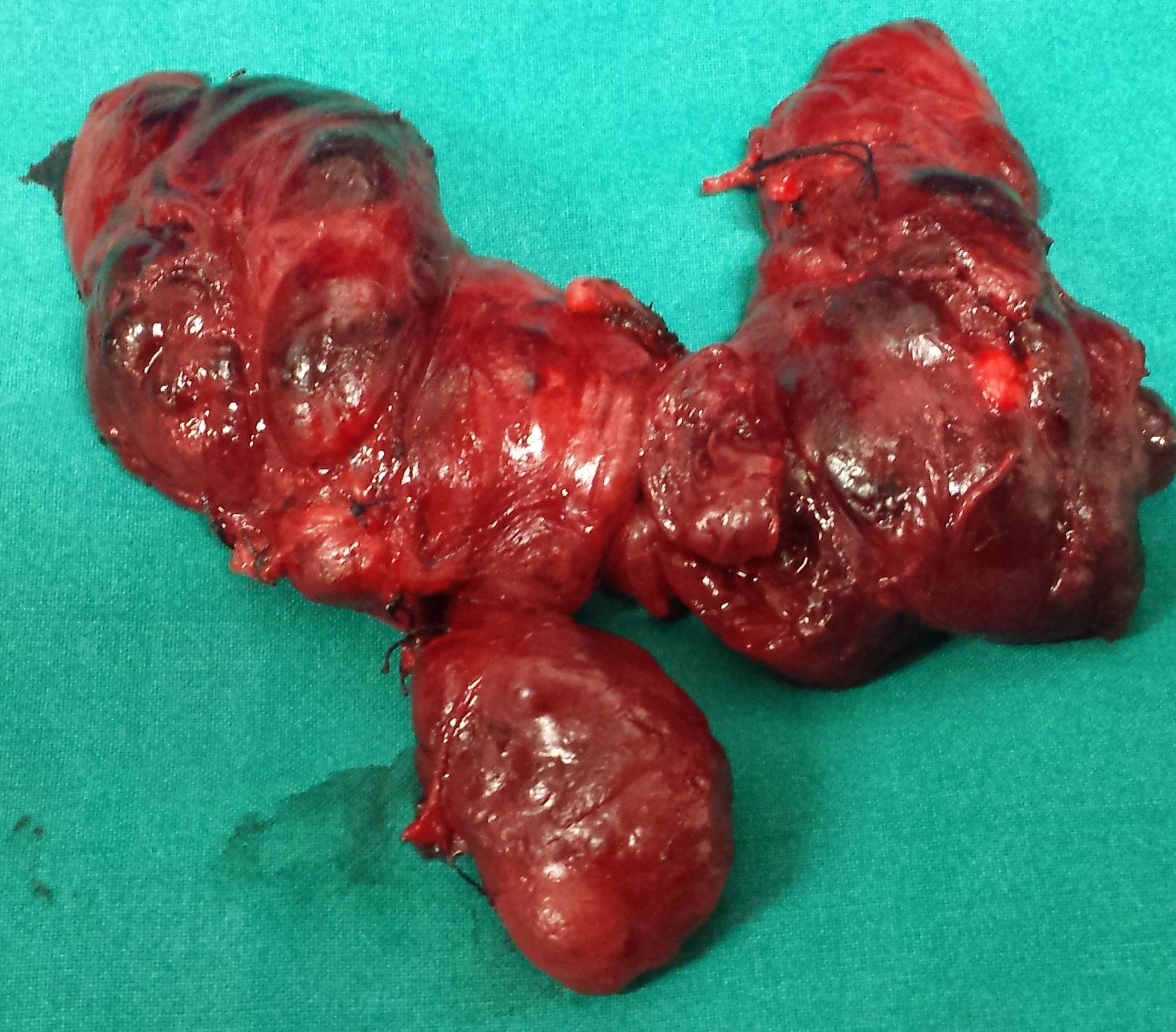
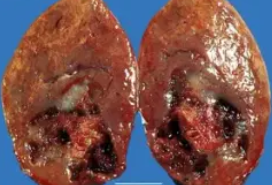
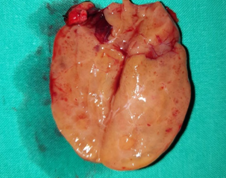
Total thyroidectomy specimen - Hürthle cell carcinoma . (Courtesy Dr. V. Penopoulos)

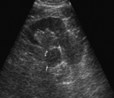
Ultrasound scan of the neck revealed heterogeneous parenchymal echotexture of both the thyroid lobes with multiple heterogeneous nodules seen




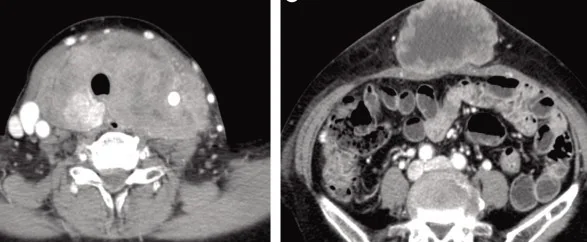
CT-Scan neck showed diffusely enlarged thyroid gland with heterogeneous enhancement but no calcification
Markedly decreased uptake of 99mTc-pertechnetate by the thyroid gland consistent with thyroiditis

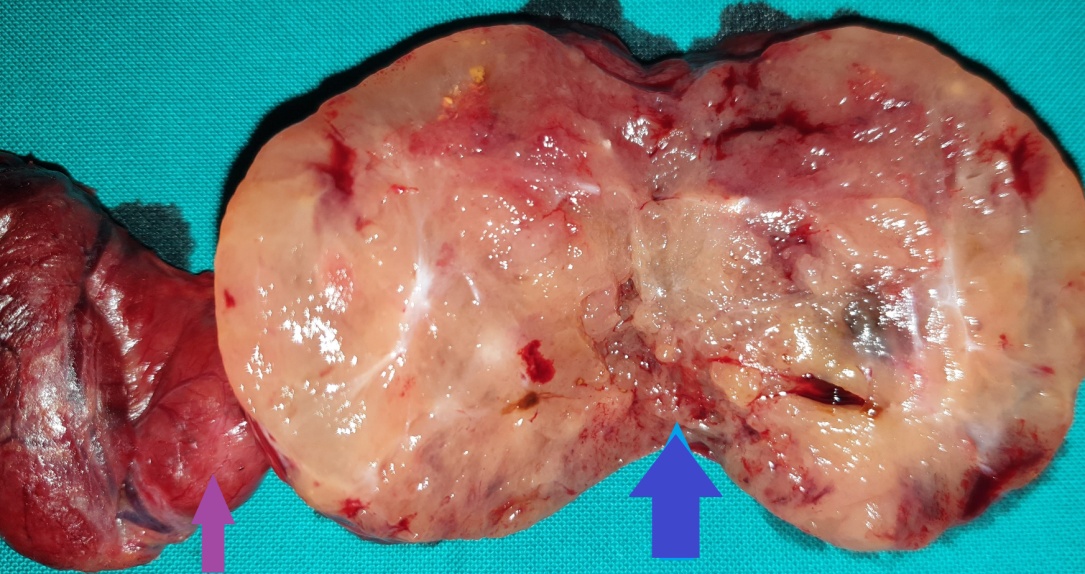
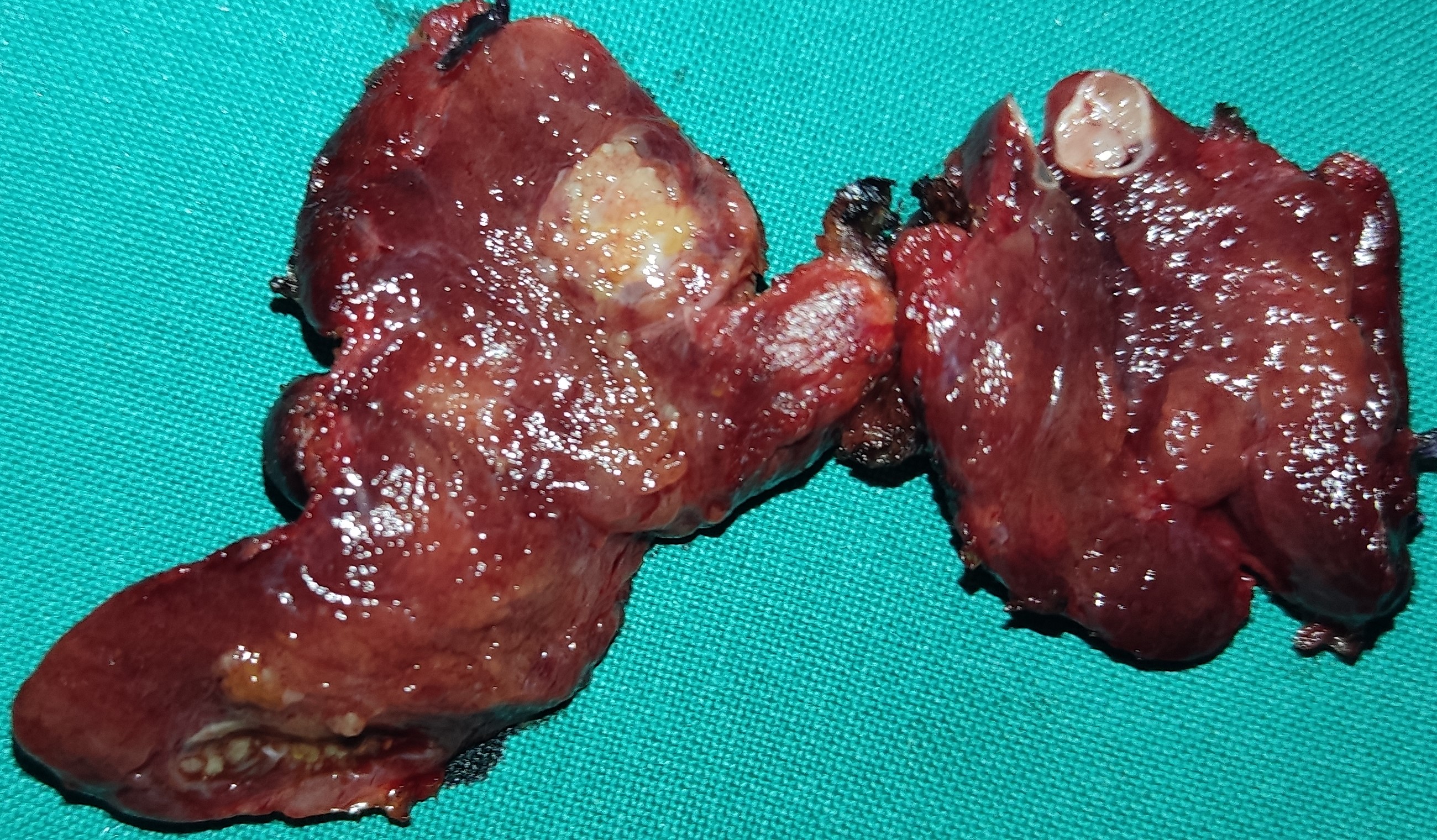
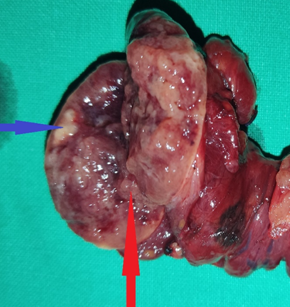
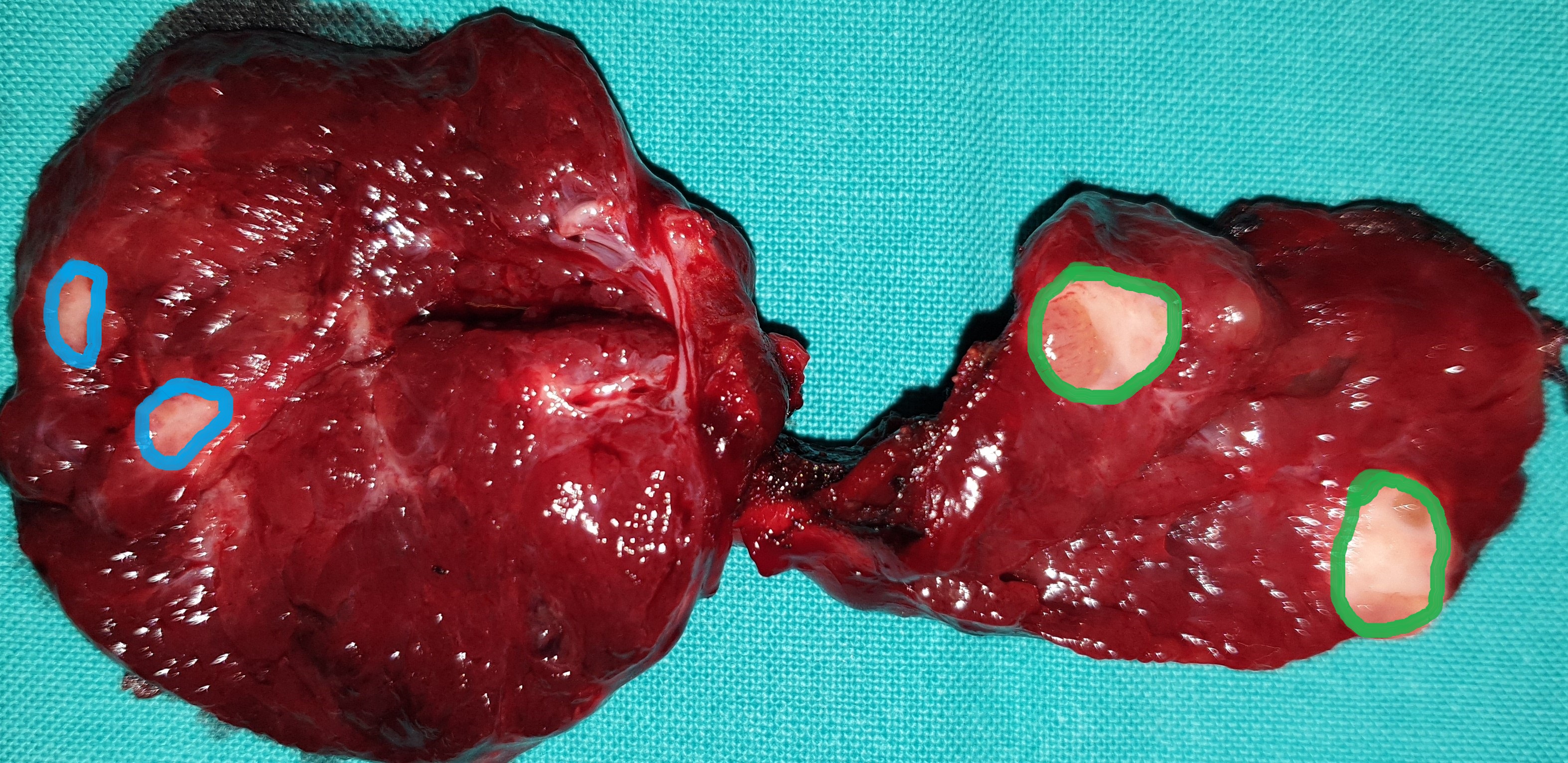
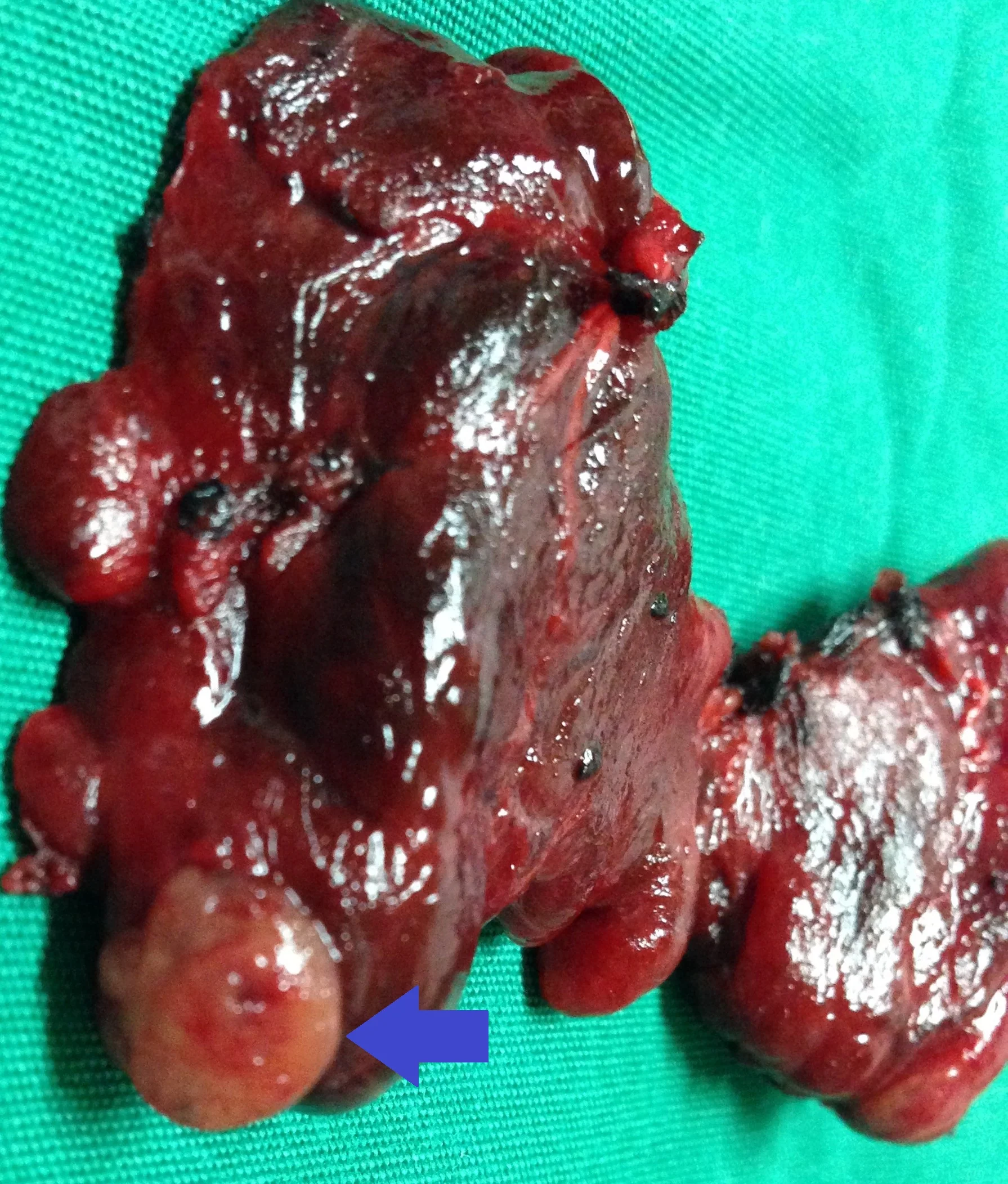
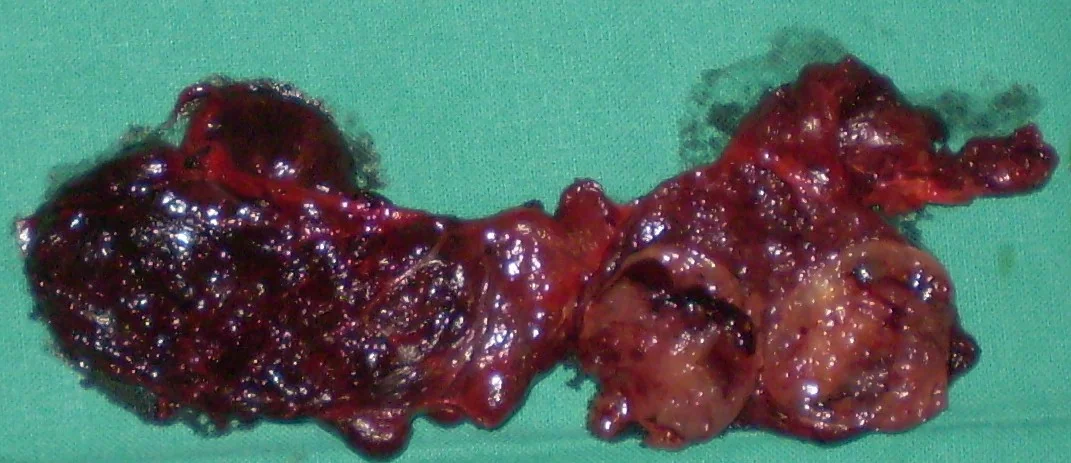
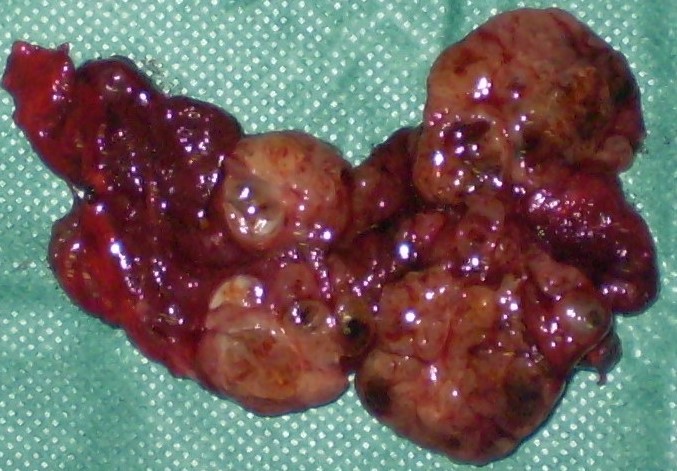
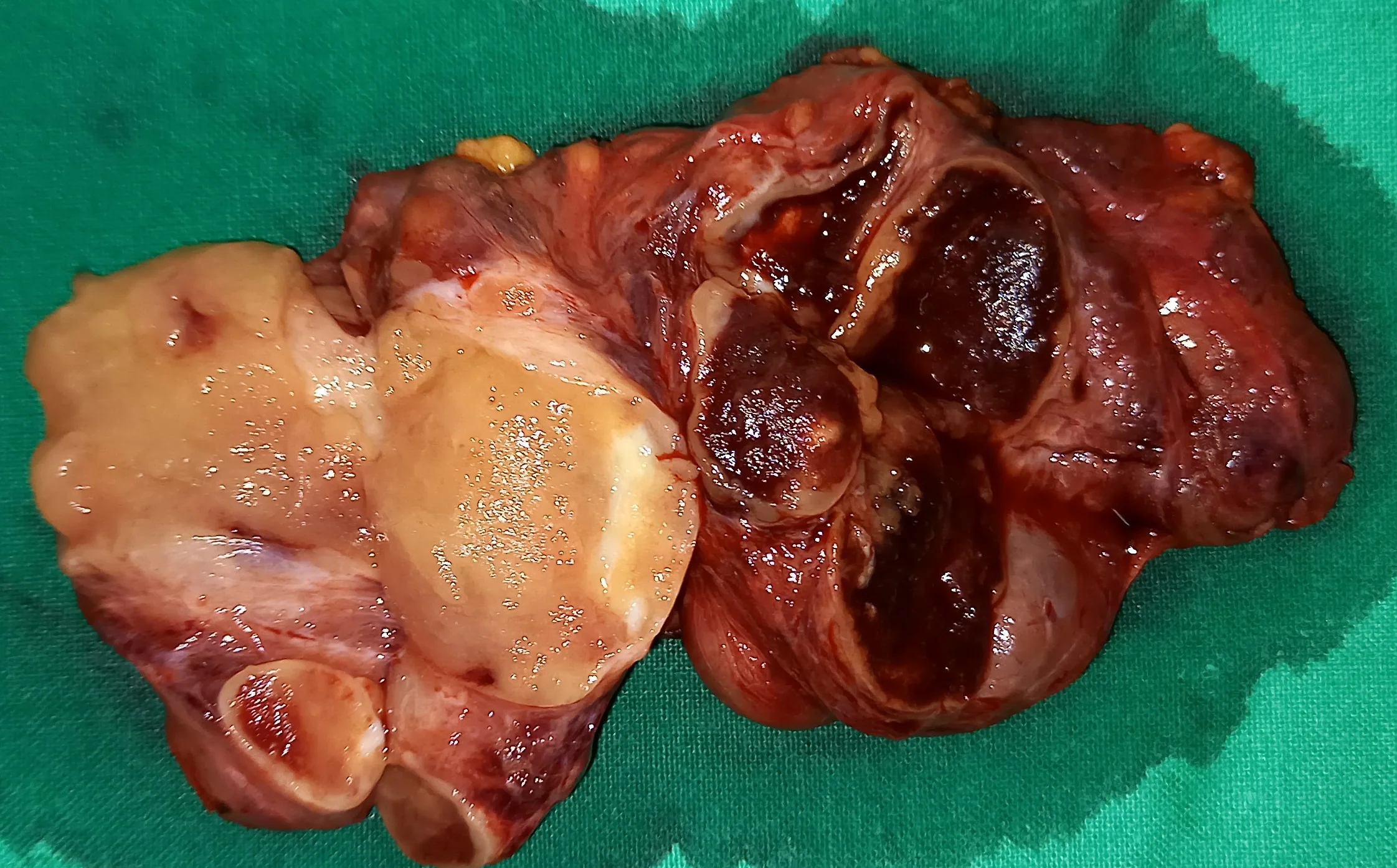
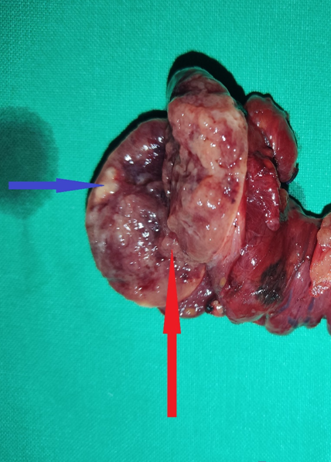
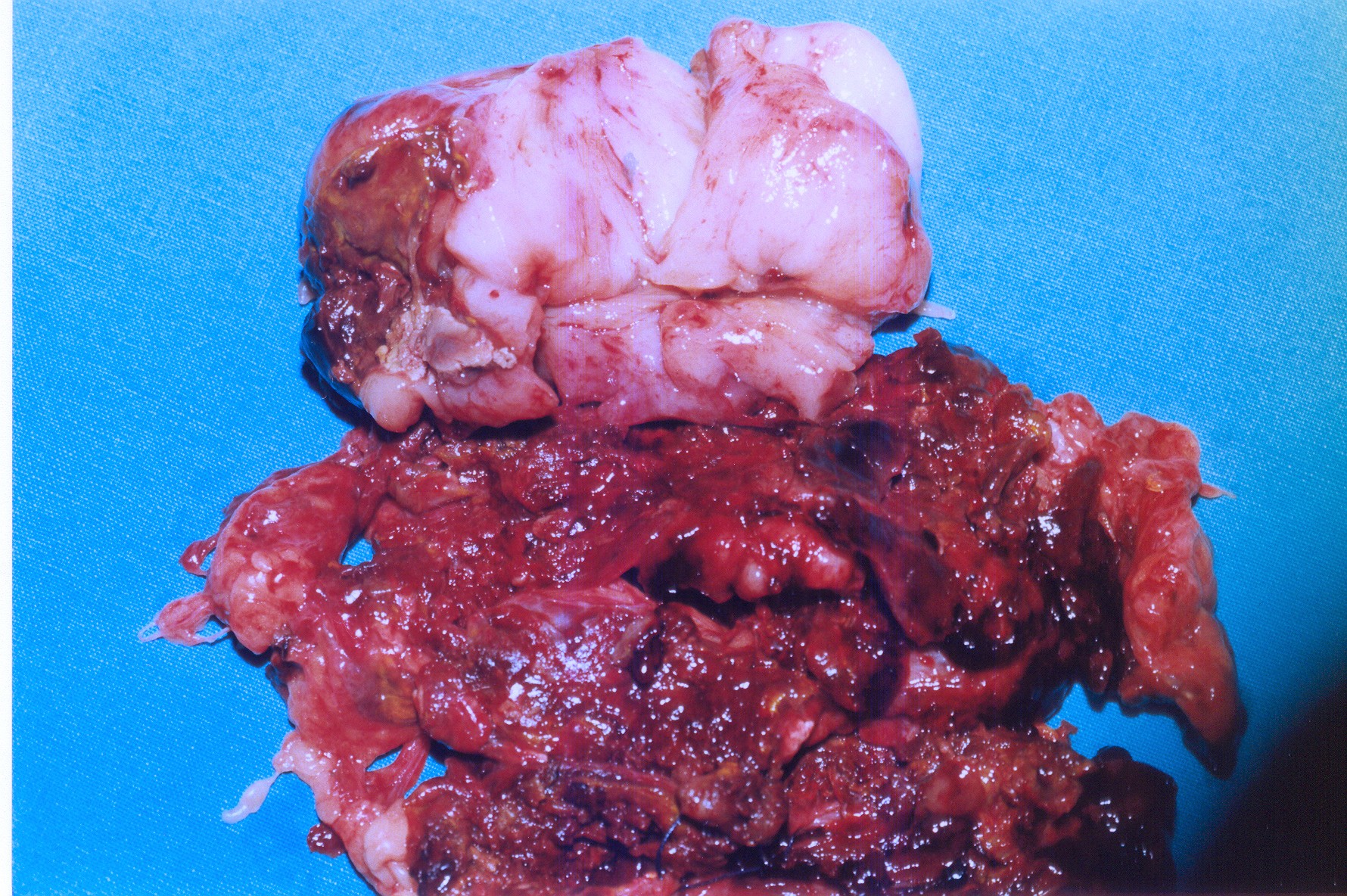
Purple arrow - Papillary thyroid carcinoma.Blue arrow - Follicular thyroid carcinoma.(Courtesy Dr. V. Penopoulos)

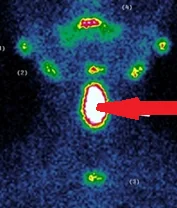
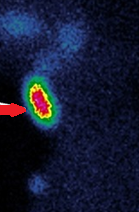
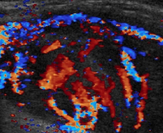
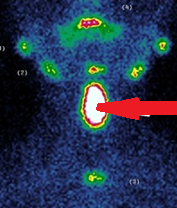
99mTc Sestamibi scintigraphy — Increased uptake of left inferior parathyroid gland (Courtesy Dr. V. Penopoulos)
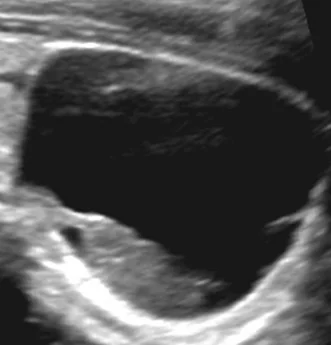
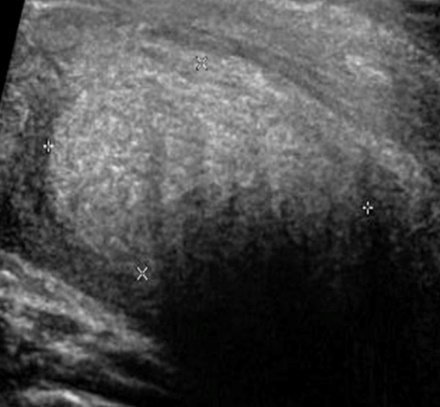
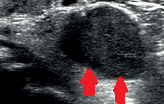
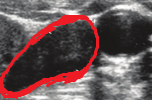
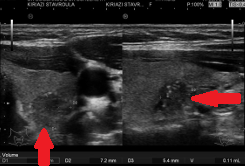
U/S Neck.Left sided, mixed echogenicity cervical nodule.(Courtesy Dr.V.Penopoulos).
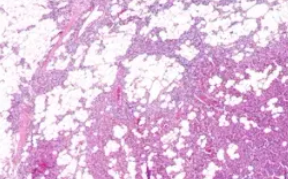
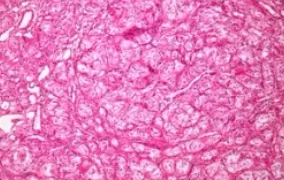
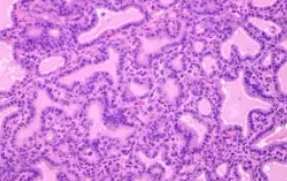
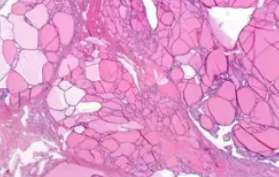
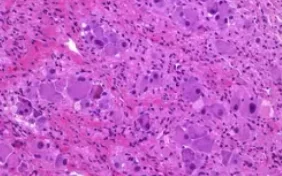
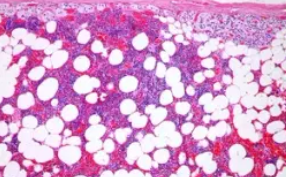
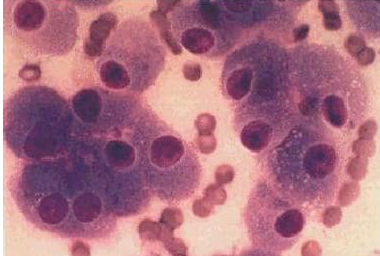
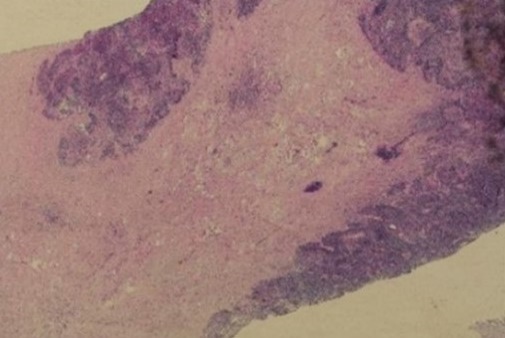
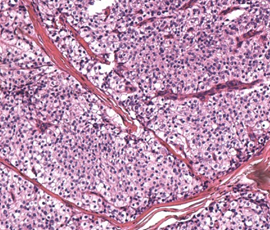
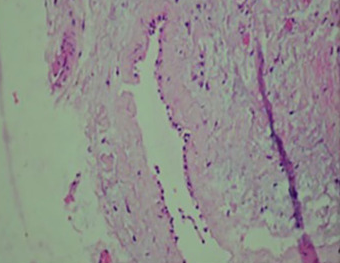
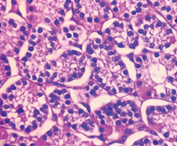
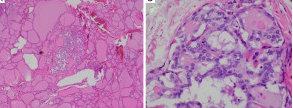
Water-clear cell parathyroid adenoma. The cells display minimal nuclear pleomorphism and have a uniform foamy cytoplasm (Courtesy Dr. V. Penopoulos)
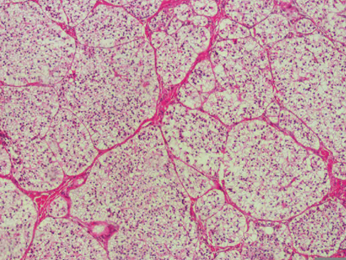
Water-clear cell parathyroid adenoma. The cells display minimal nuclear pleomorphism and have a uniform foamy cytoplasm (Courtesy Dr. V. Penopoulos)
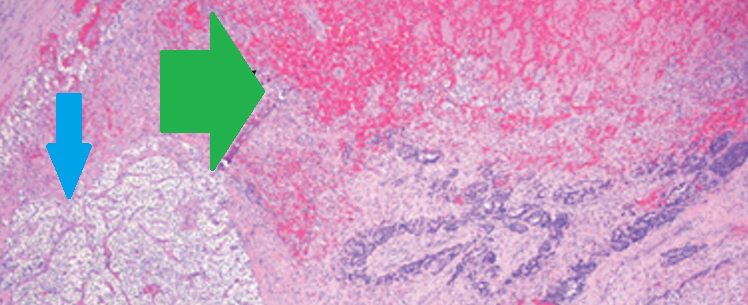
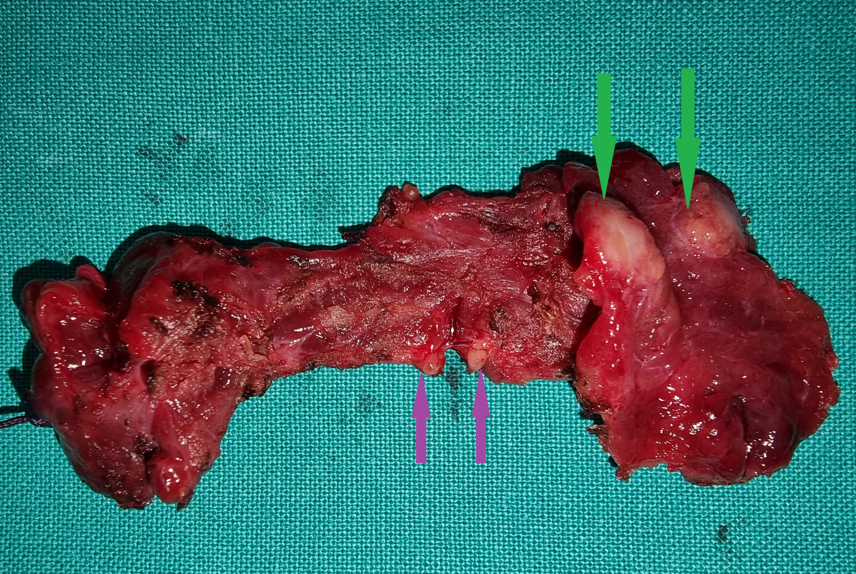
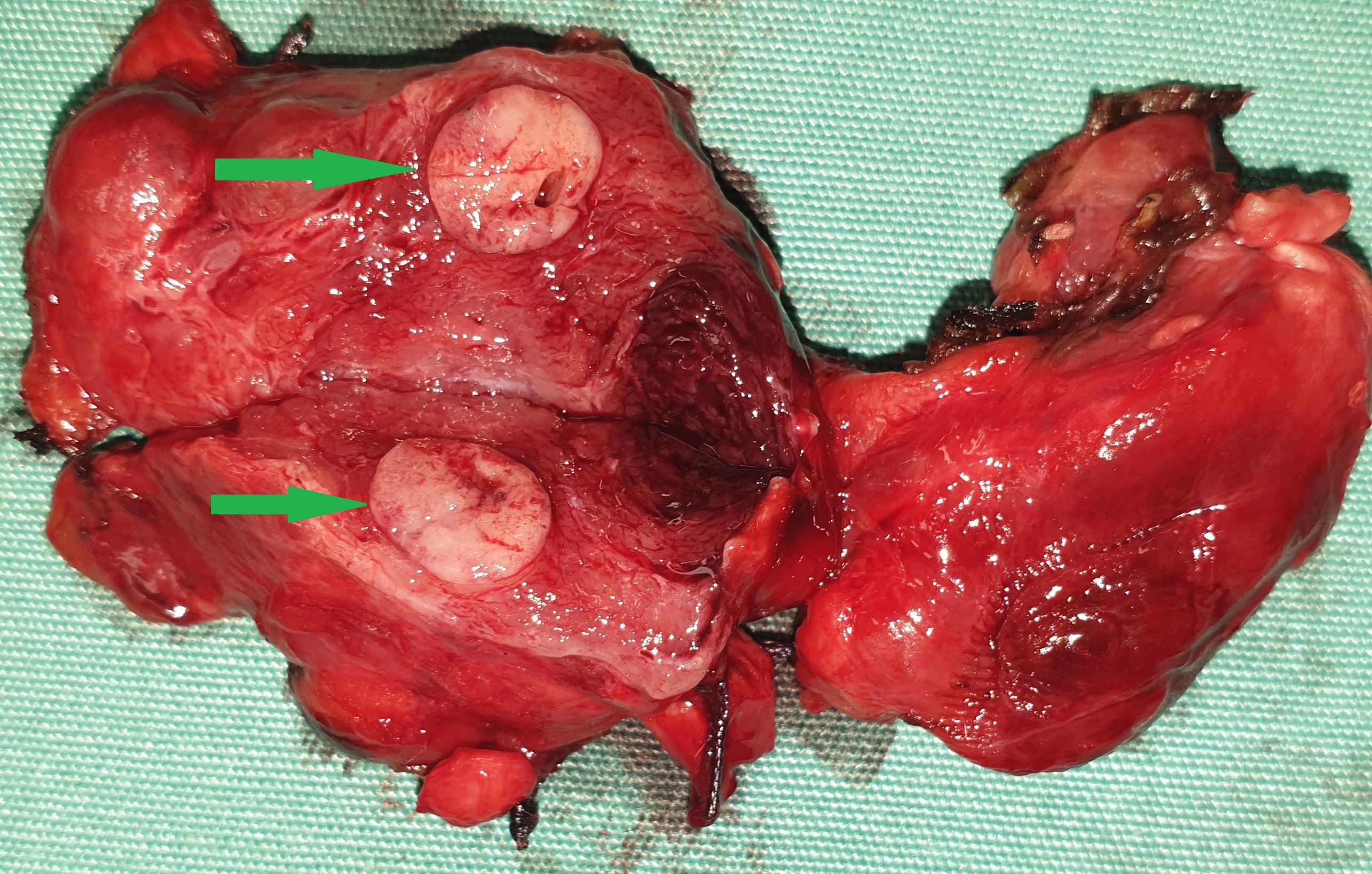
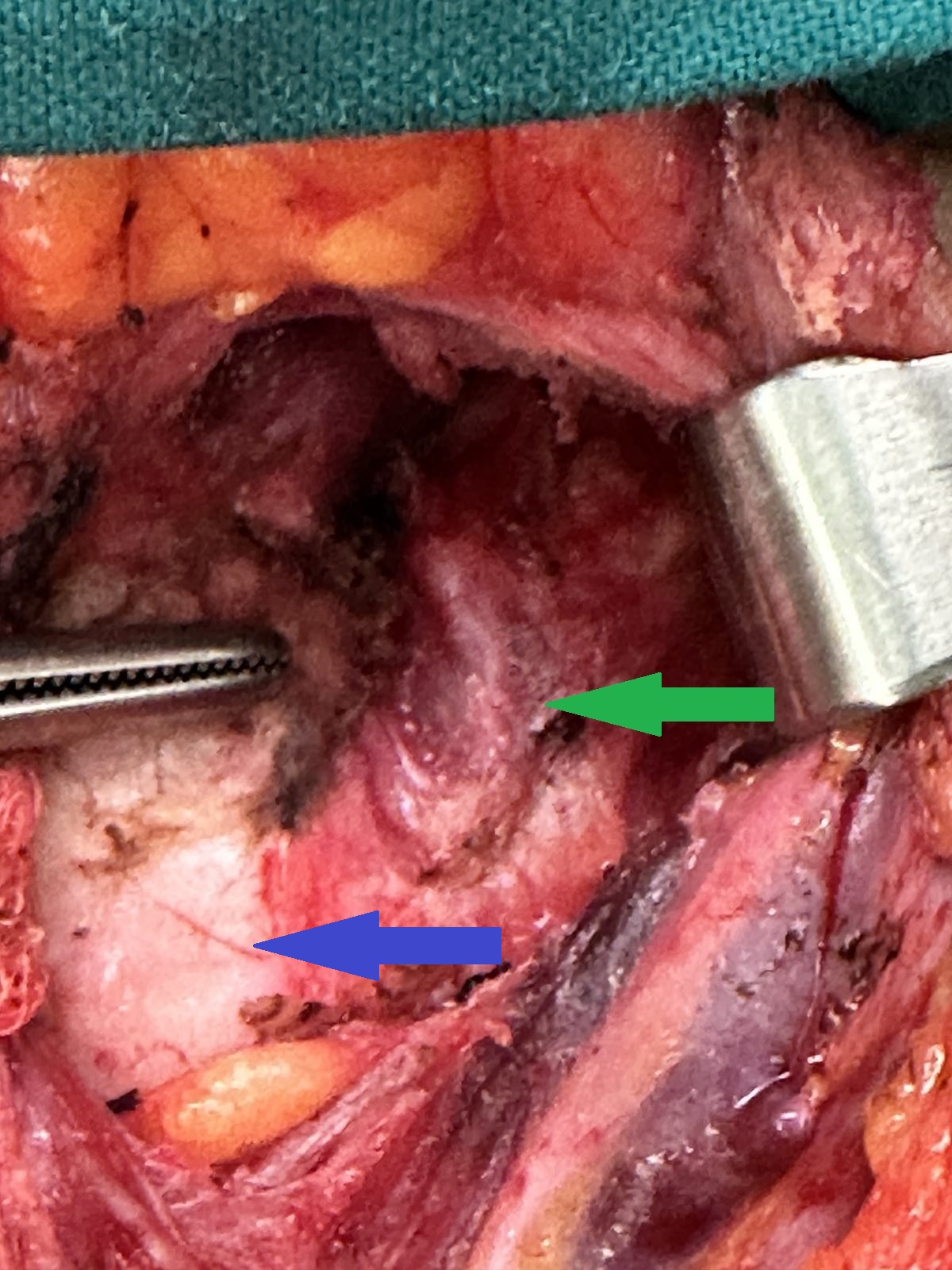
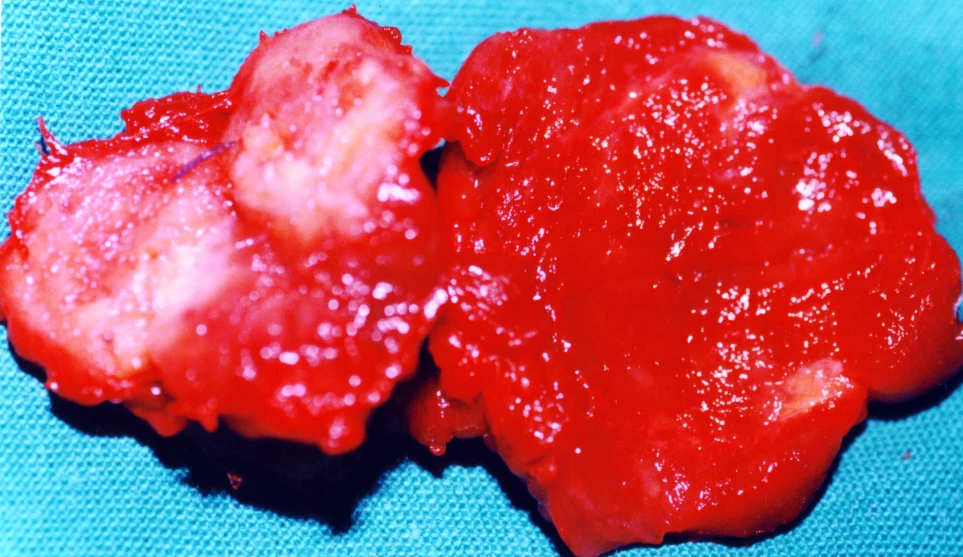
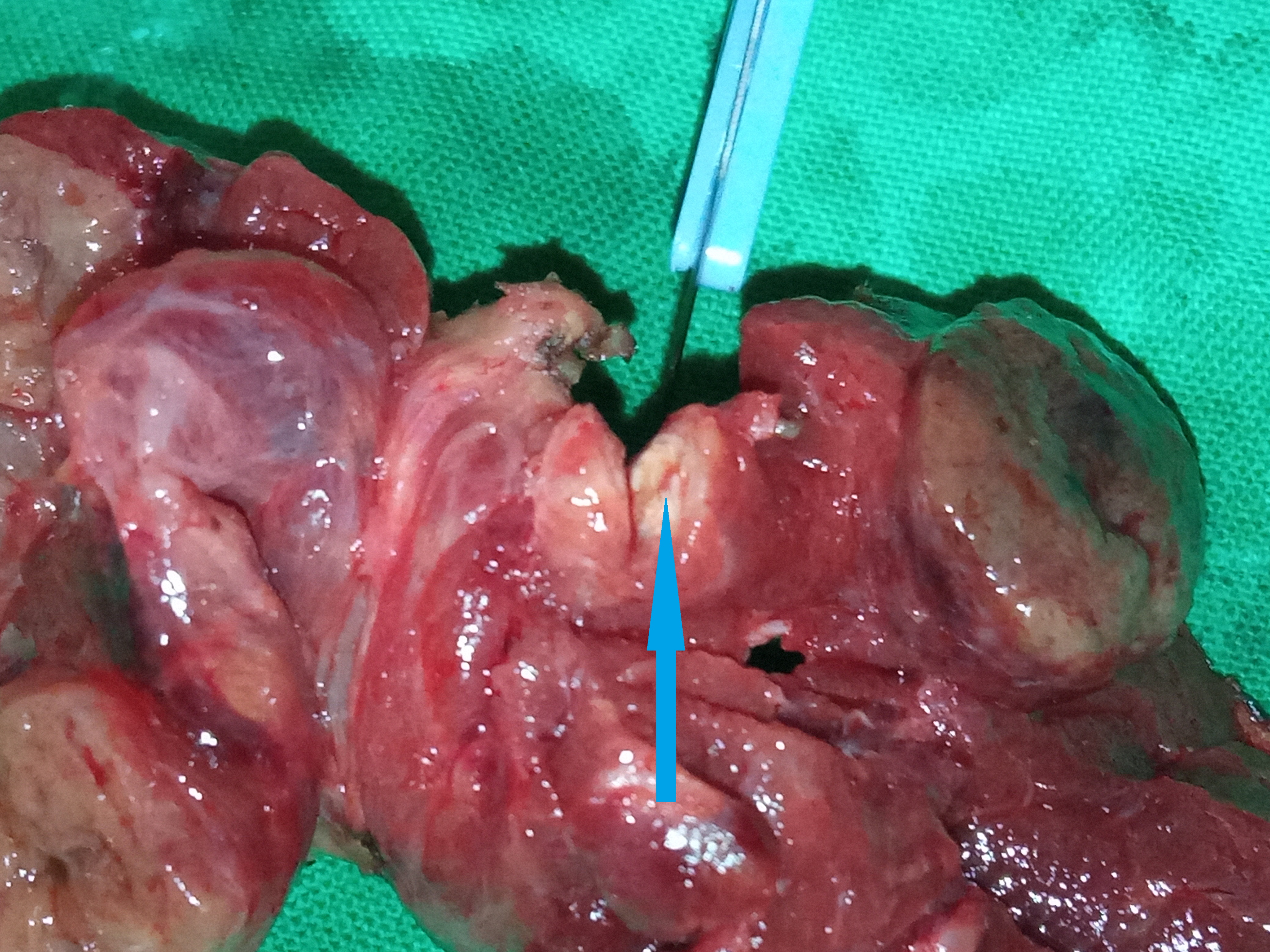
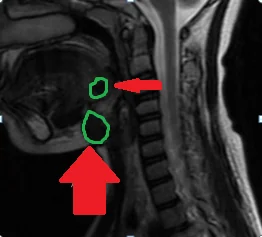
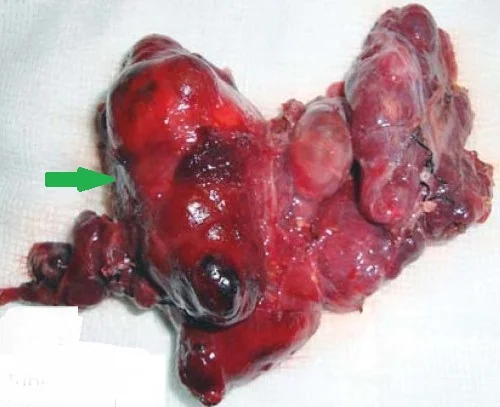
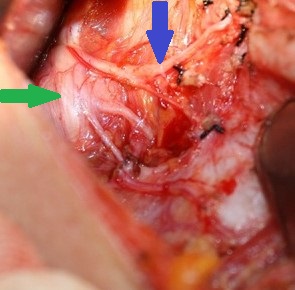
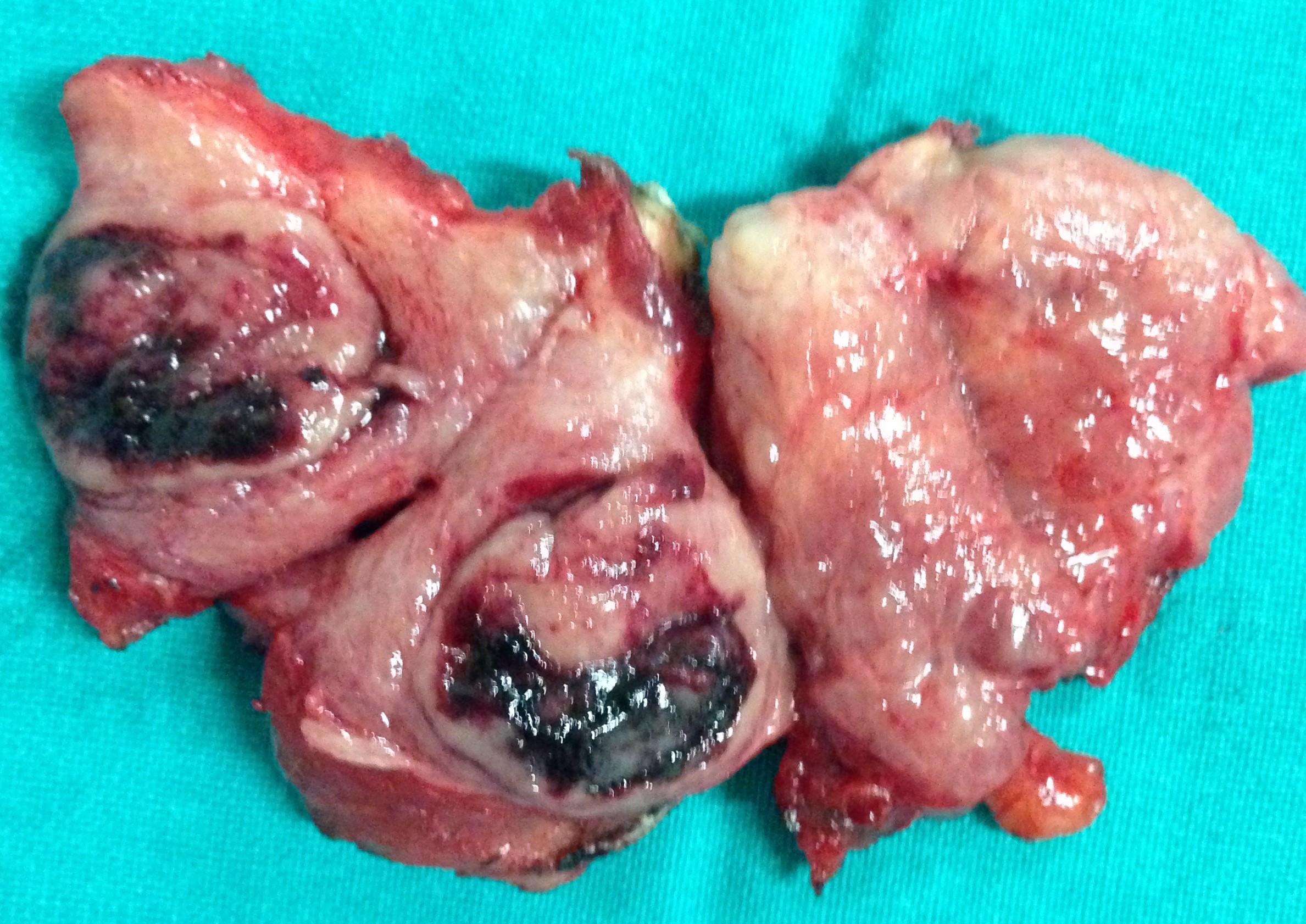
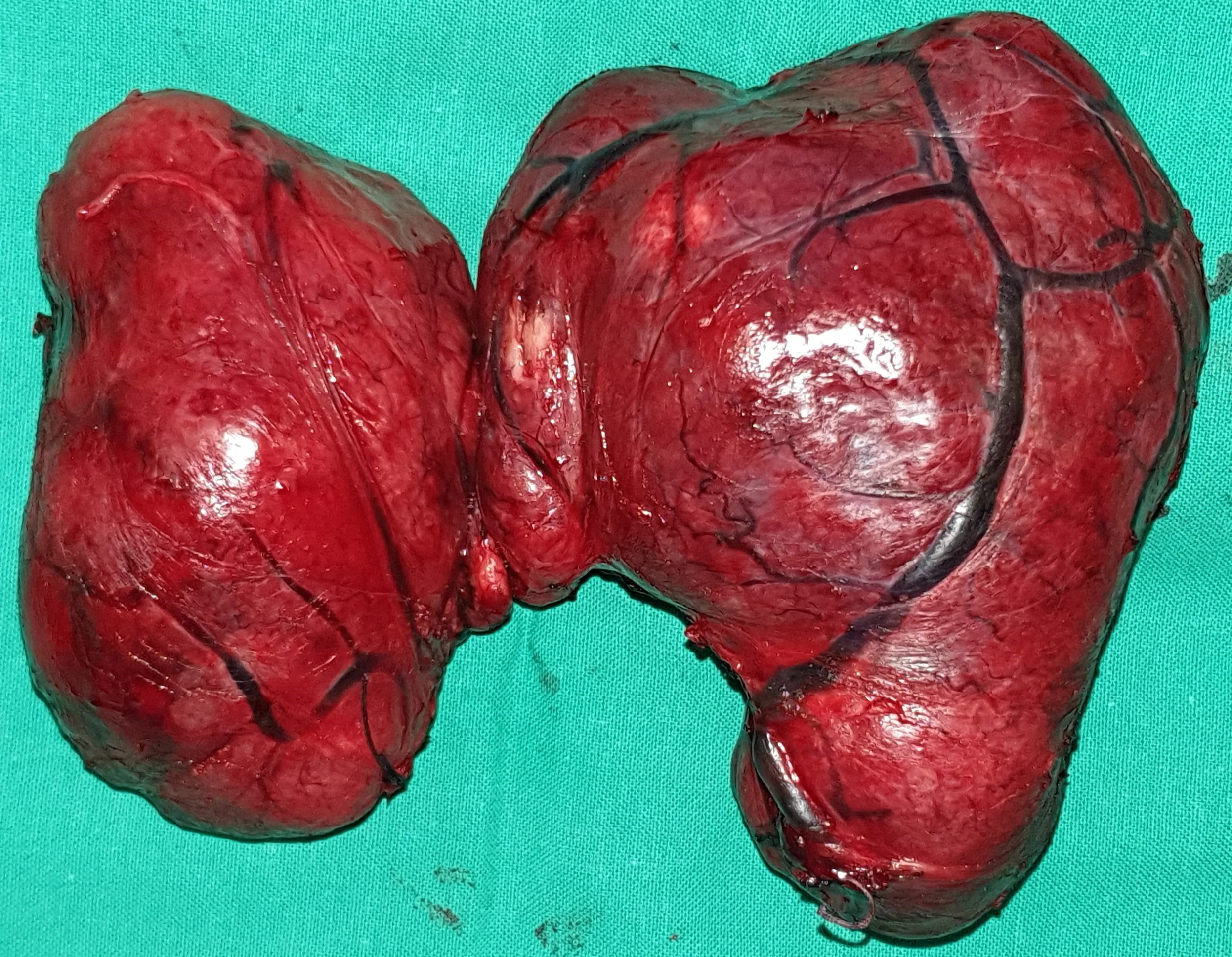
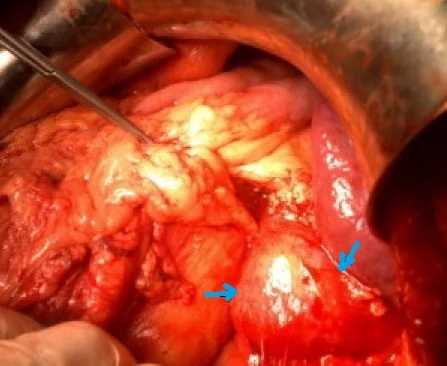
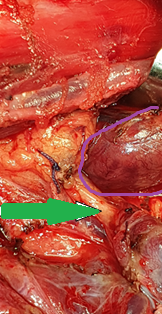
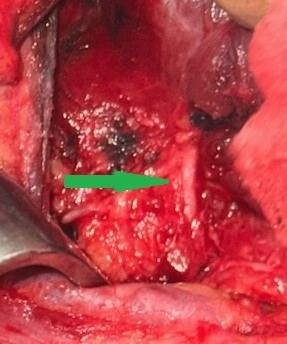
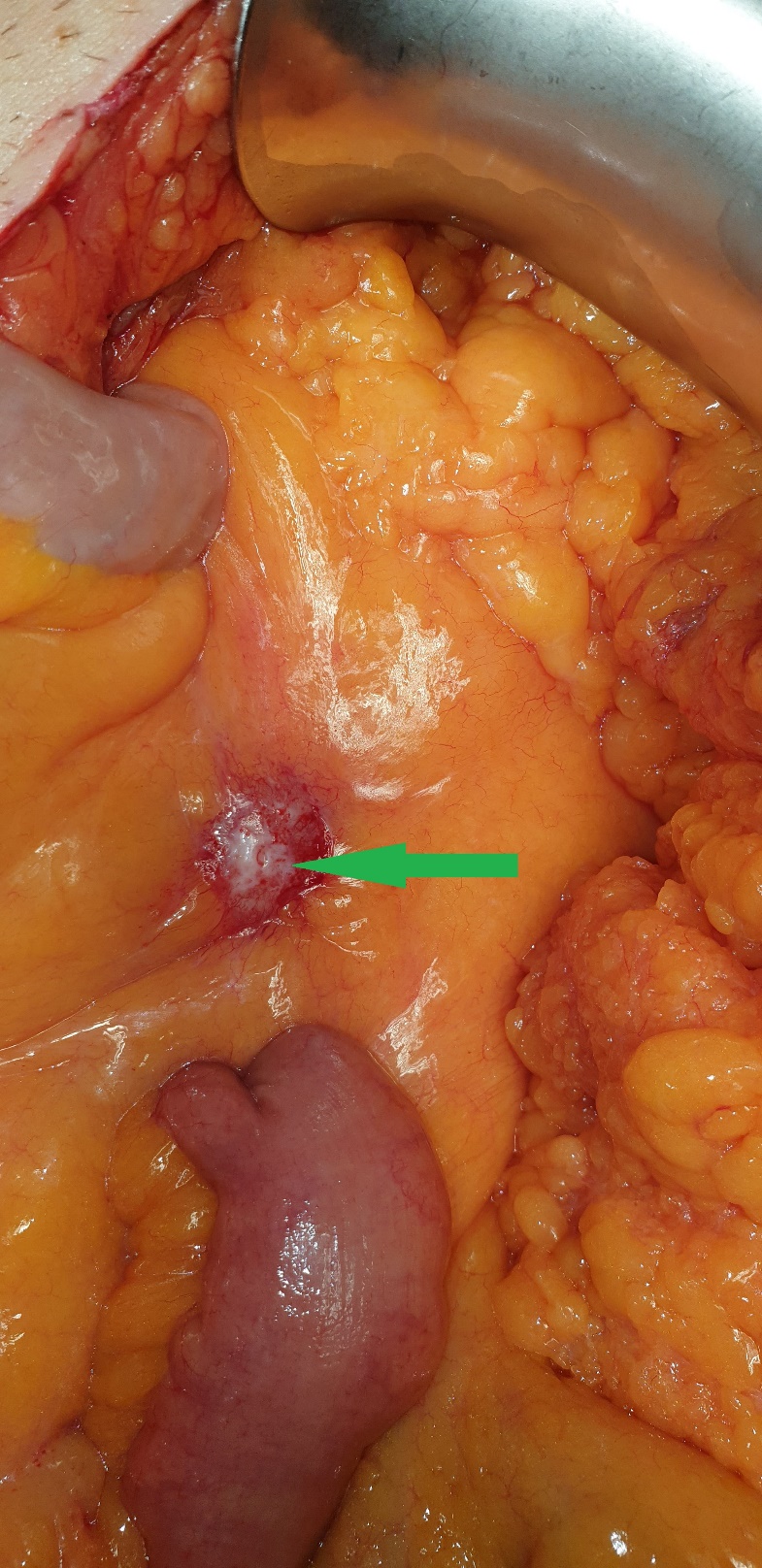
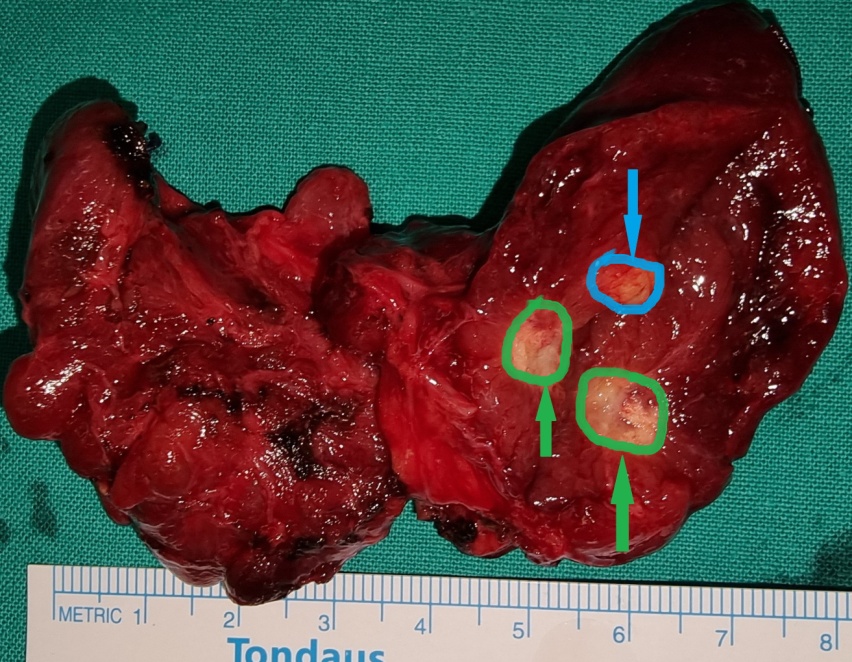
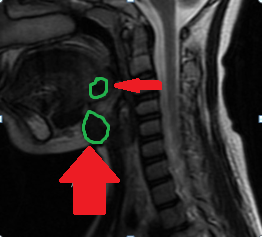
Blue arrow — Parathyroid adenoma. Green arrow — Area of necrosis and hemorrhage (Courtesy Dr. V. Penopoulos)
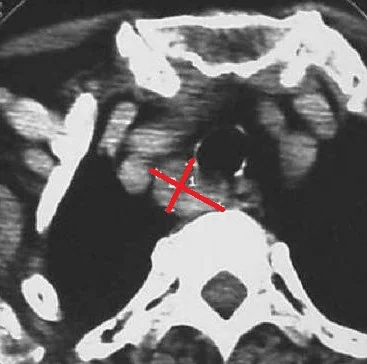
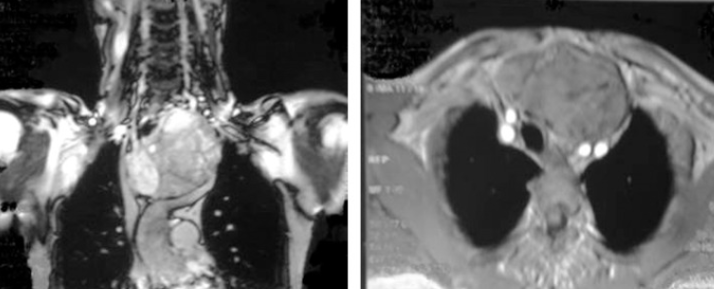
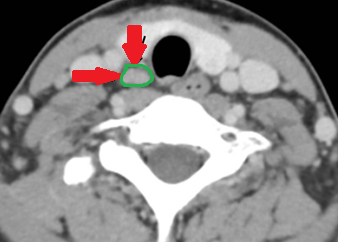
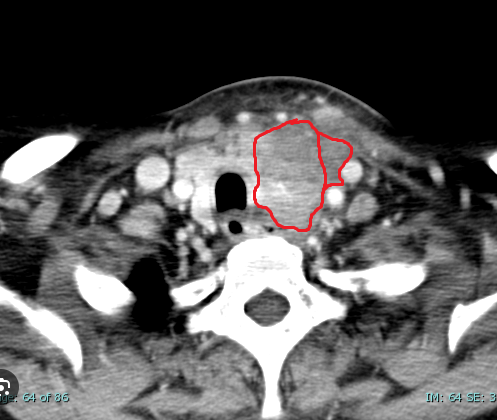
CT — Well-circumscribed nodule in contact with the lower pole of the left thyroid lobe (Courtesy Dr. V. Penopoulos)


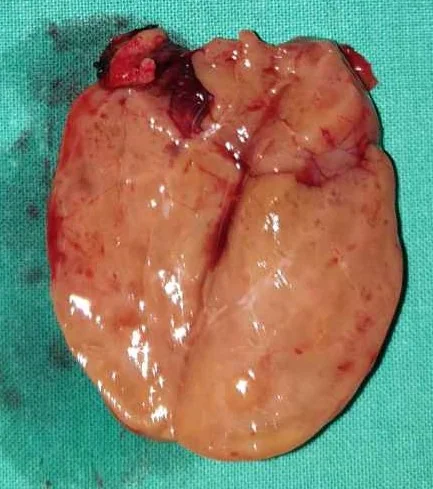
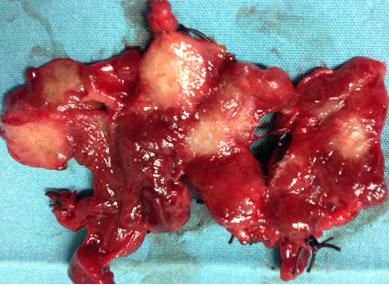
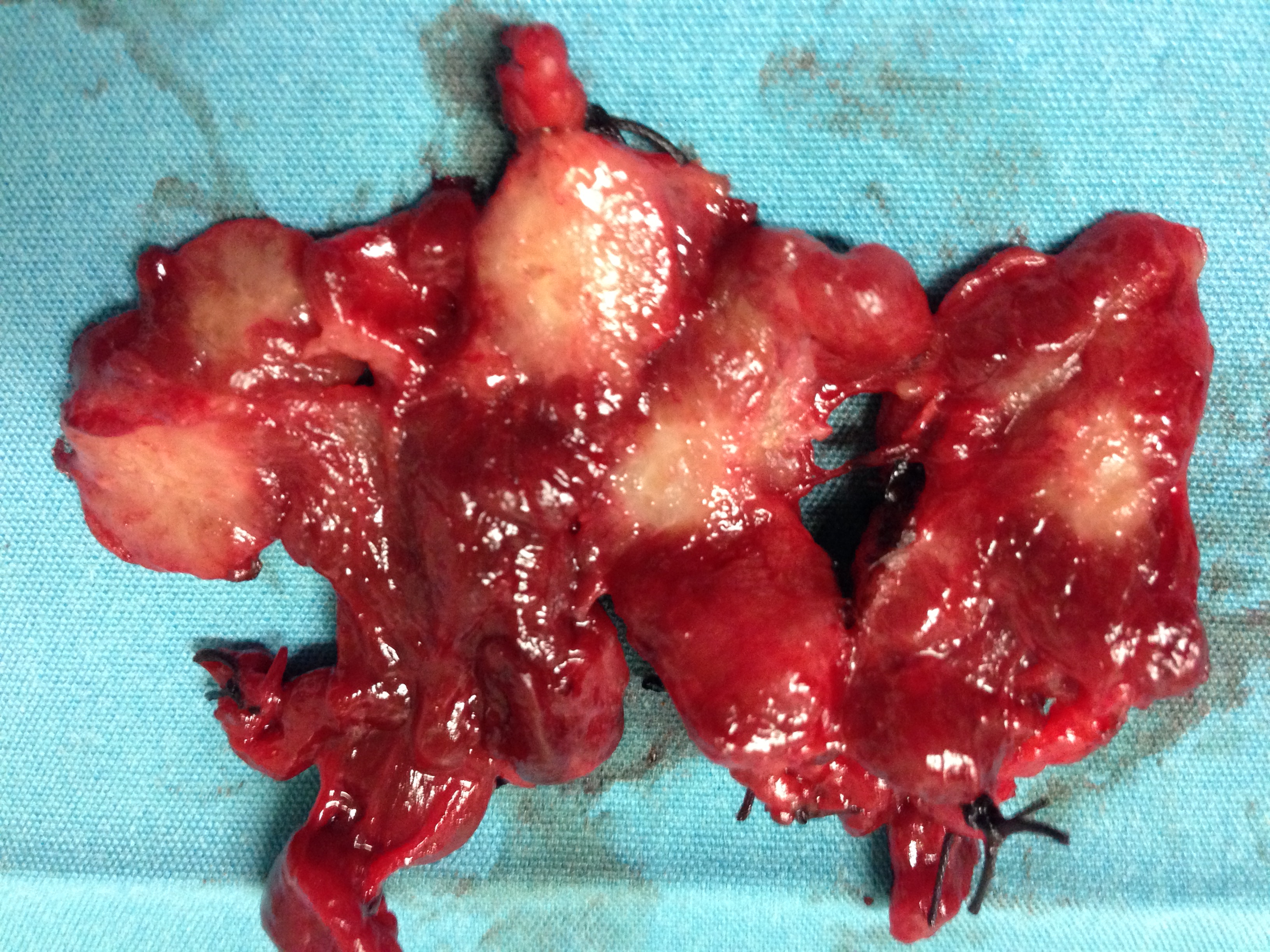
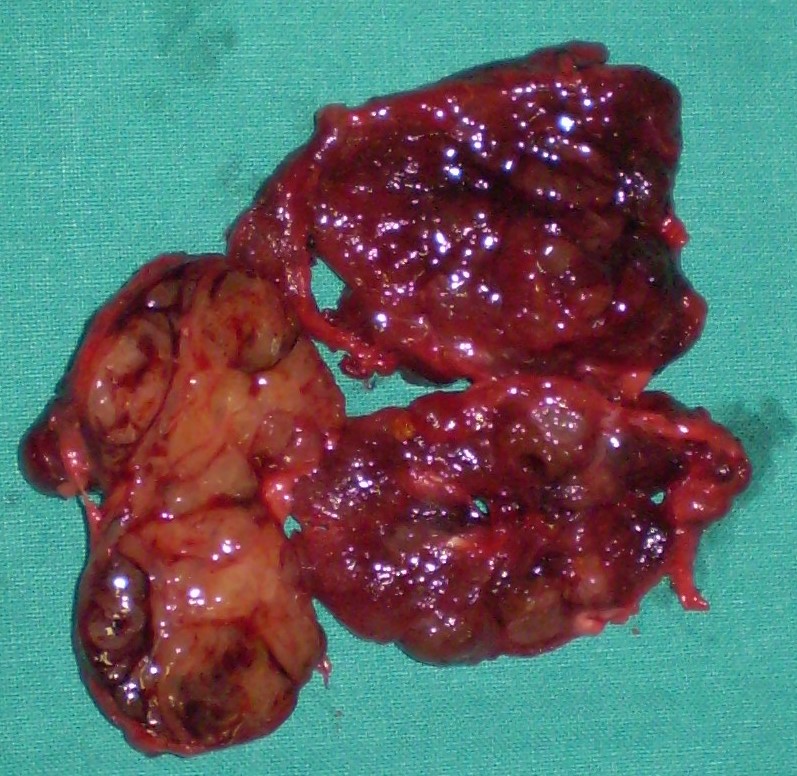
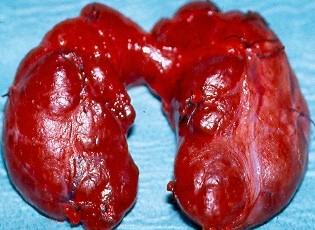
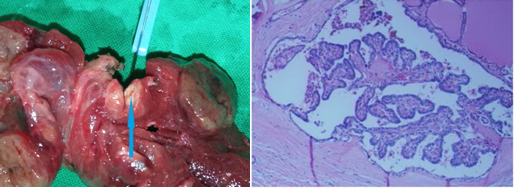
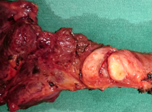
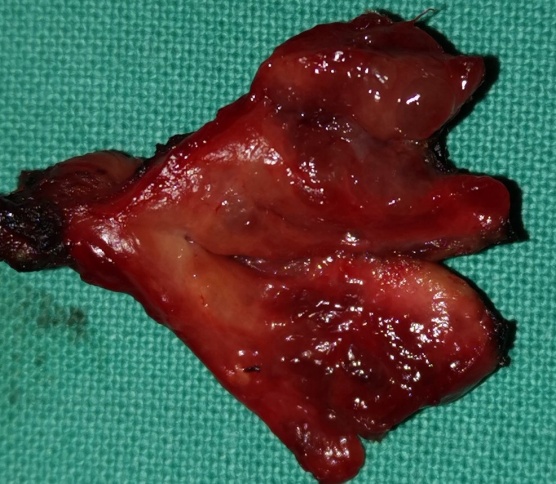
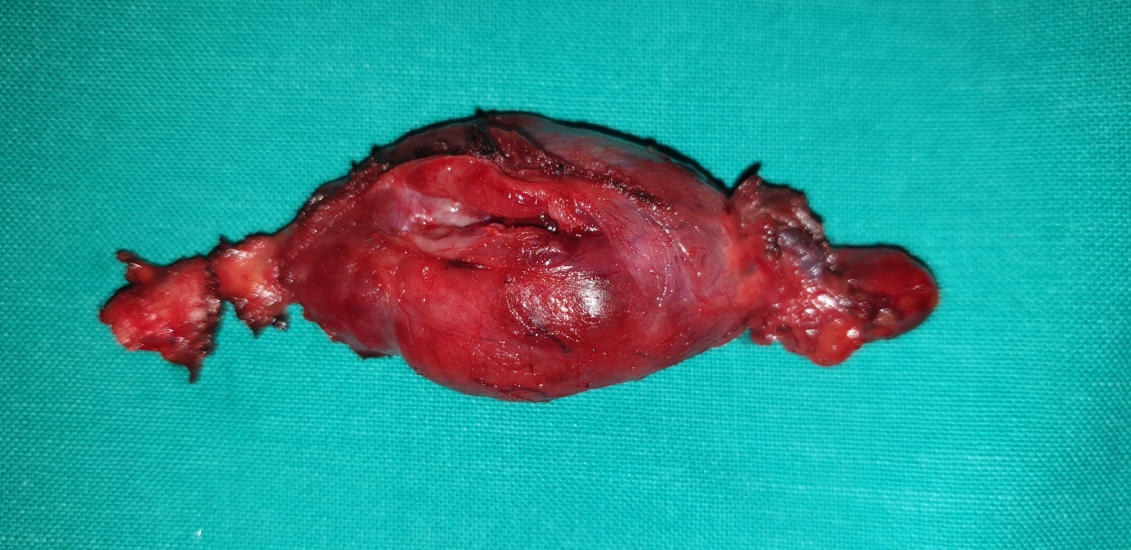
Right thyroid lobectomy and excision of parathyroid adenoma.(Courtesy Dr . V . Penopoulos ) .


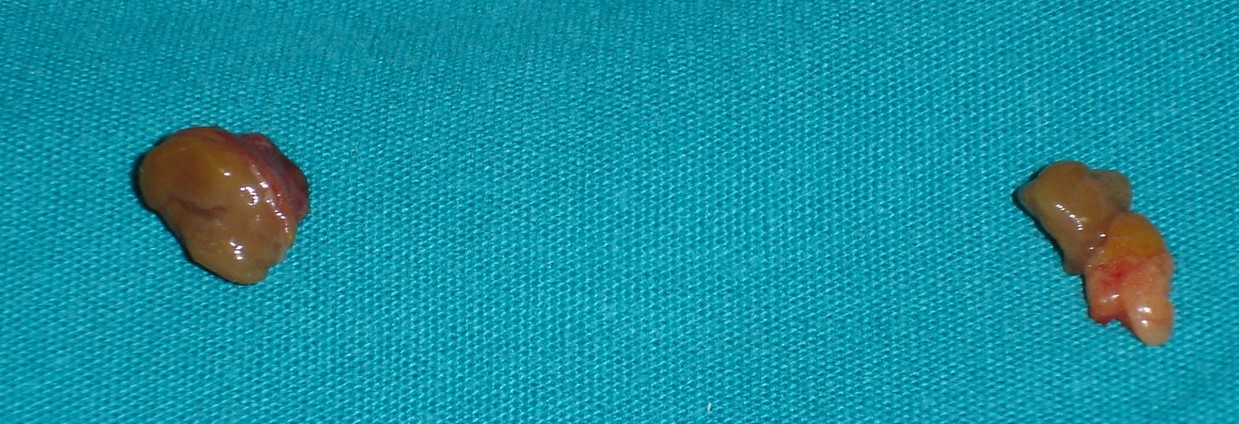
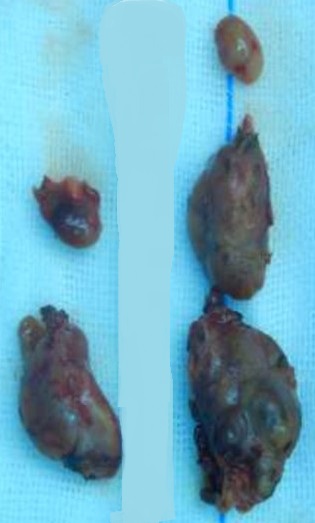
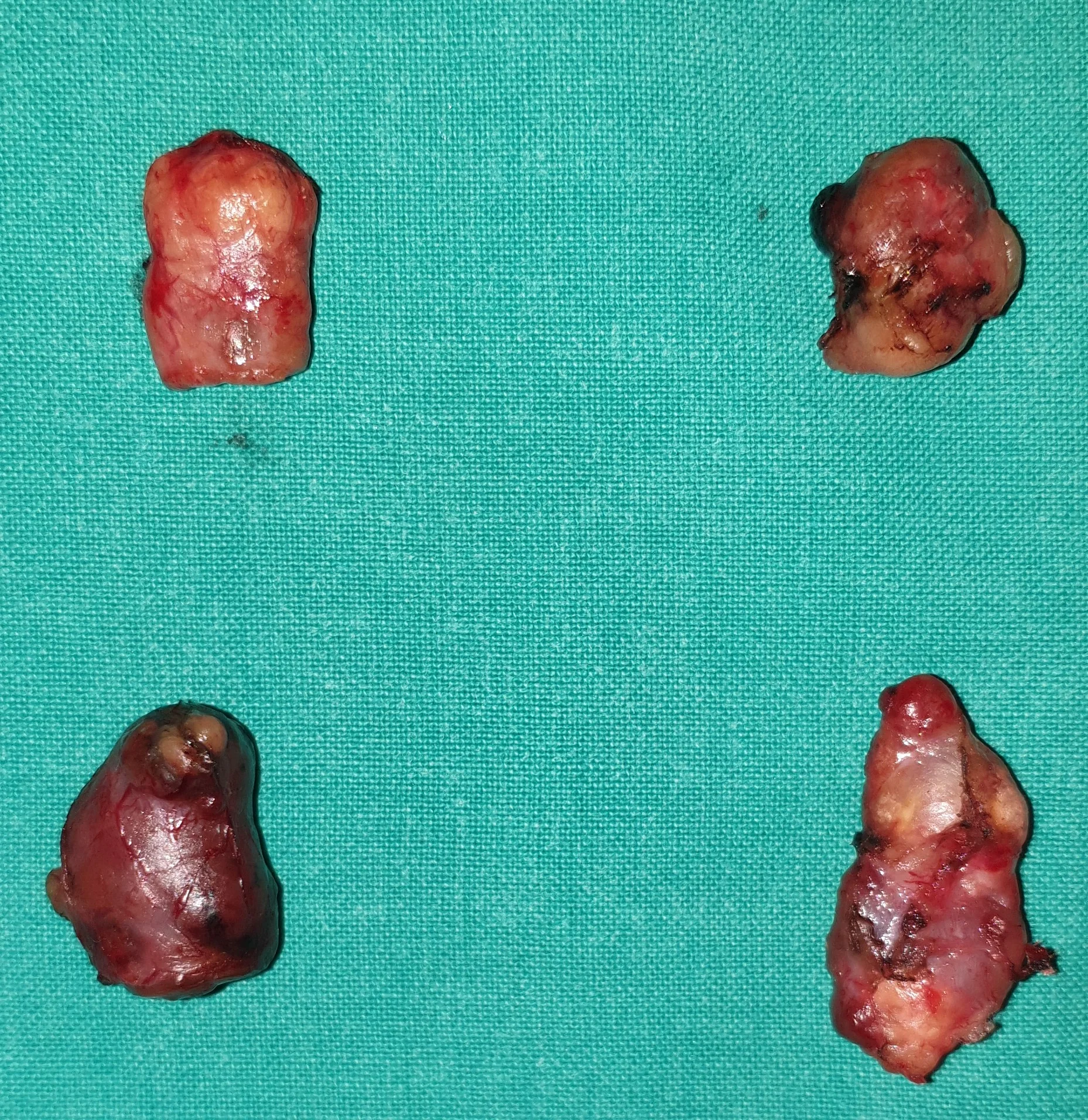
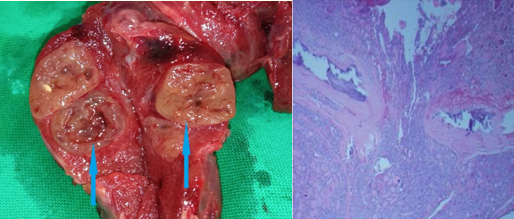
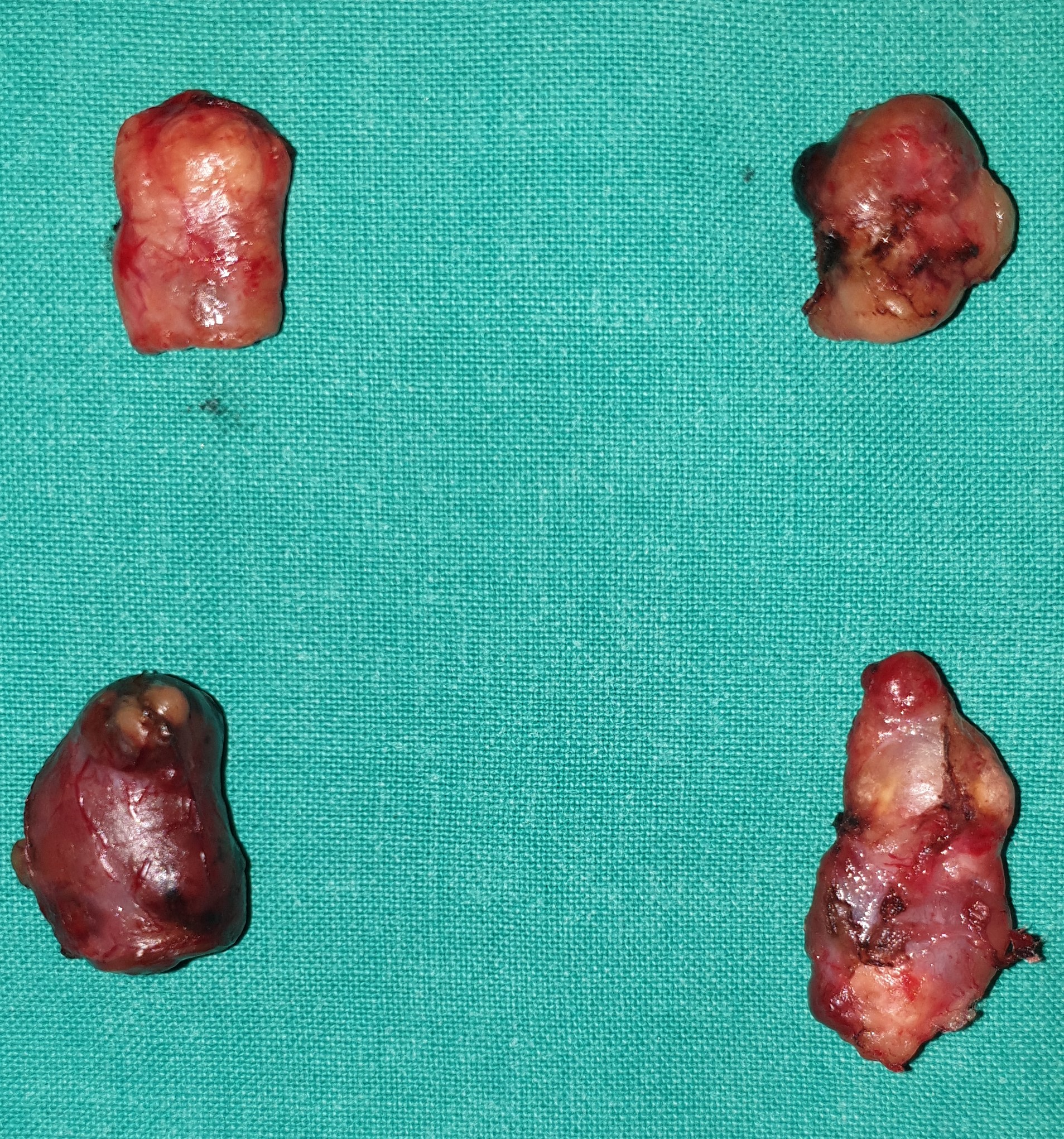
Red arrow - Left upper larger and harder parathyroid gland.Blue arrows - Rest three parathyroid glands.(Courtesy Dr.V.Penopoulos).

Subtraction scintigraphy suggestive of a right sided parathyroid adenoma and lack of thyroid perception (Courtesy Dr. V. Penopoulos)
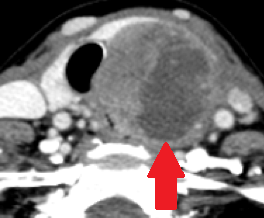
CT Scan indicating swollen right thyroid lobe with a sizable nodule in / adjacent to the right lower pole (Courtesy Dr. V. Penopoulos)


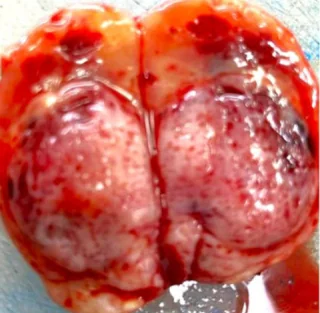
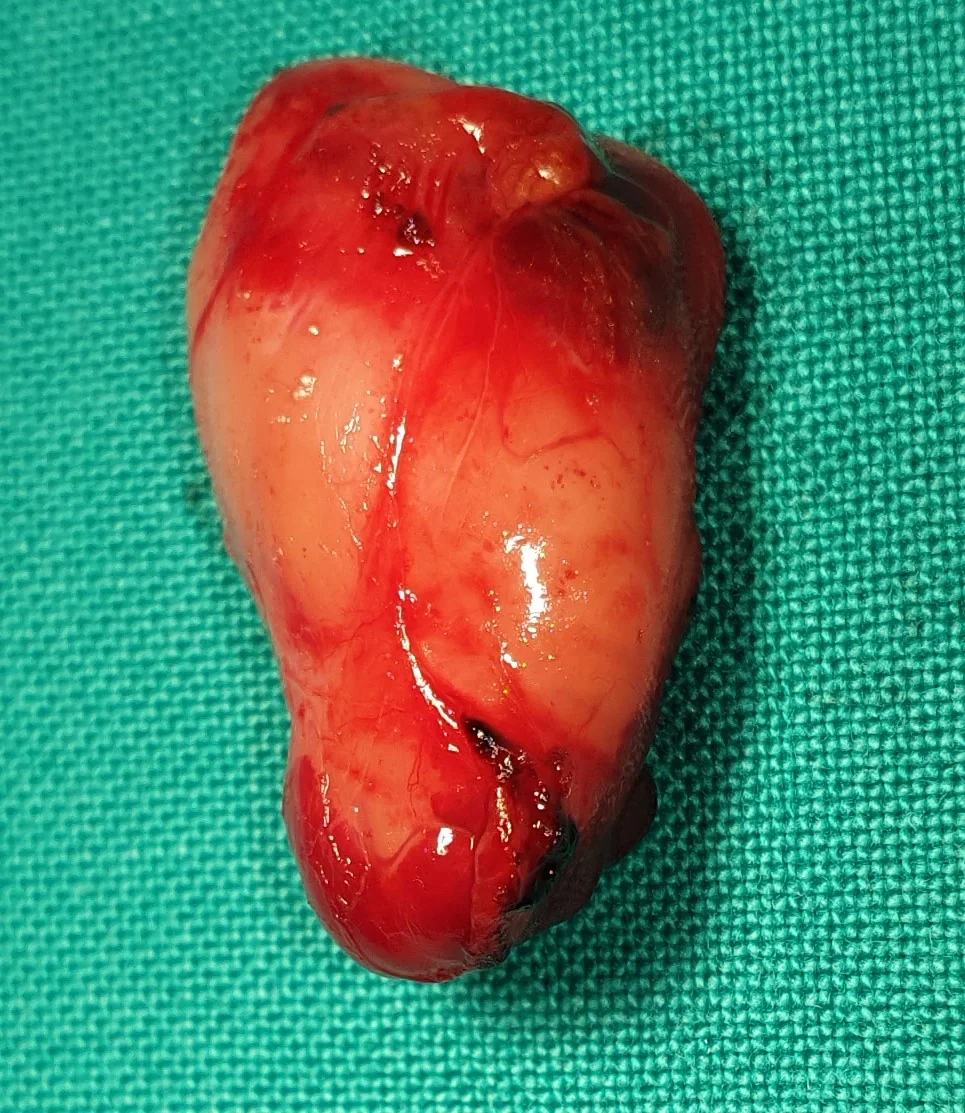
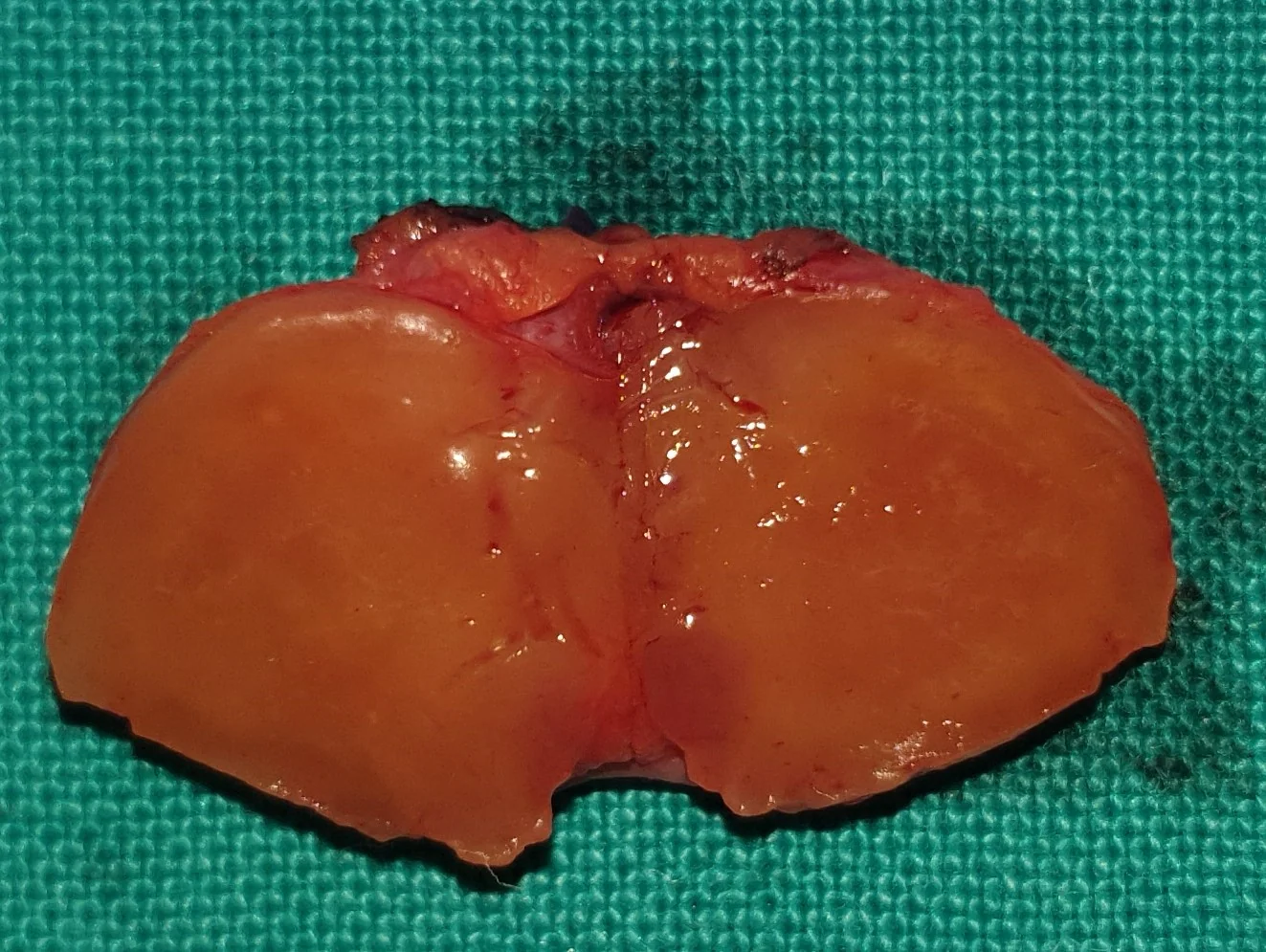
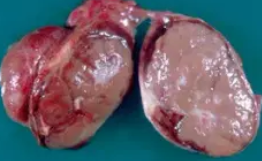
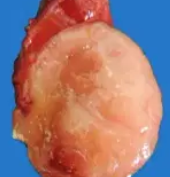
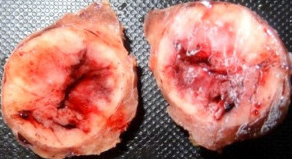
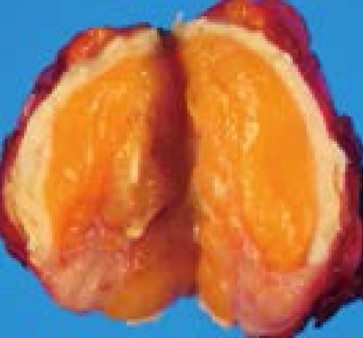
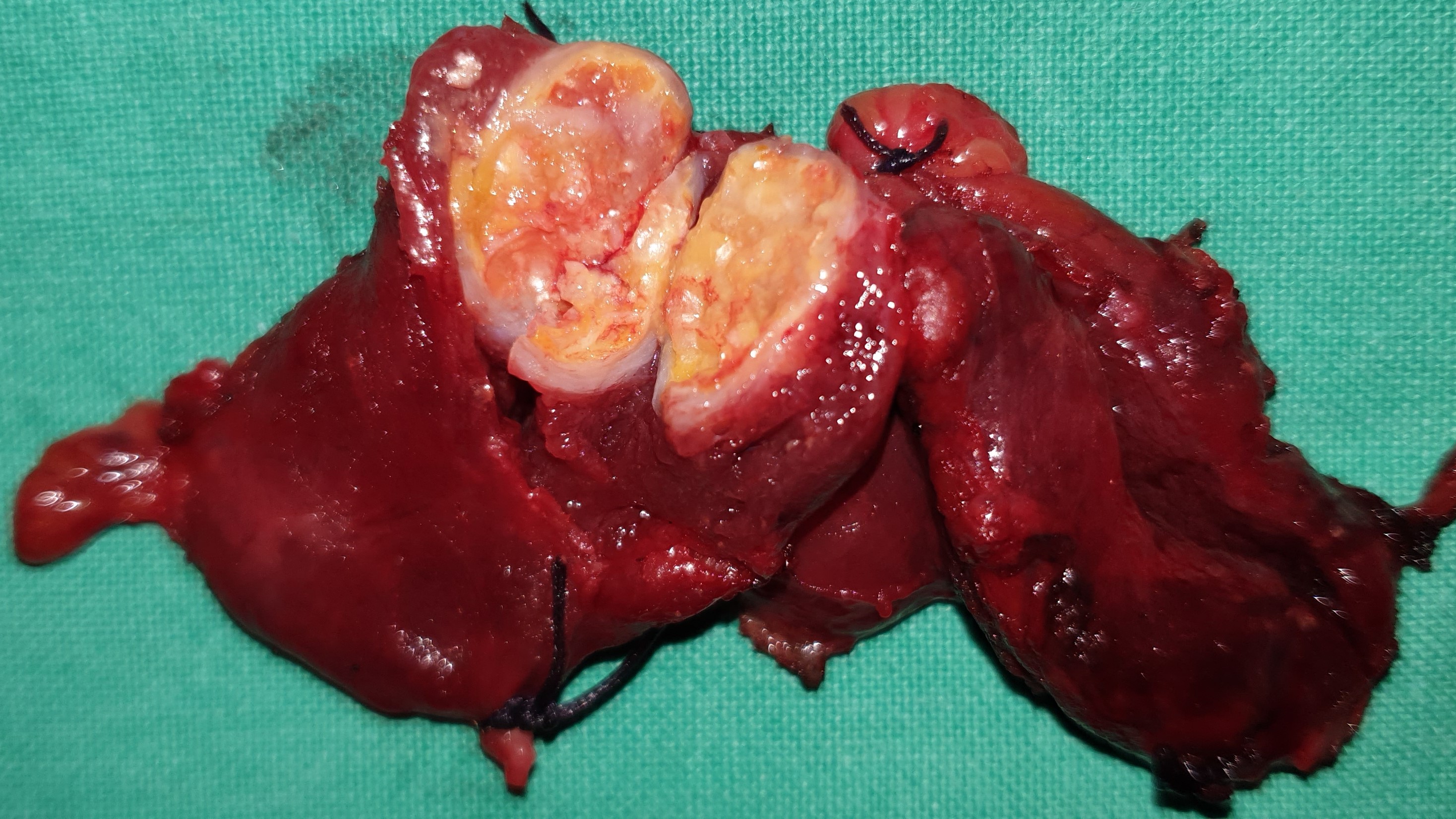
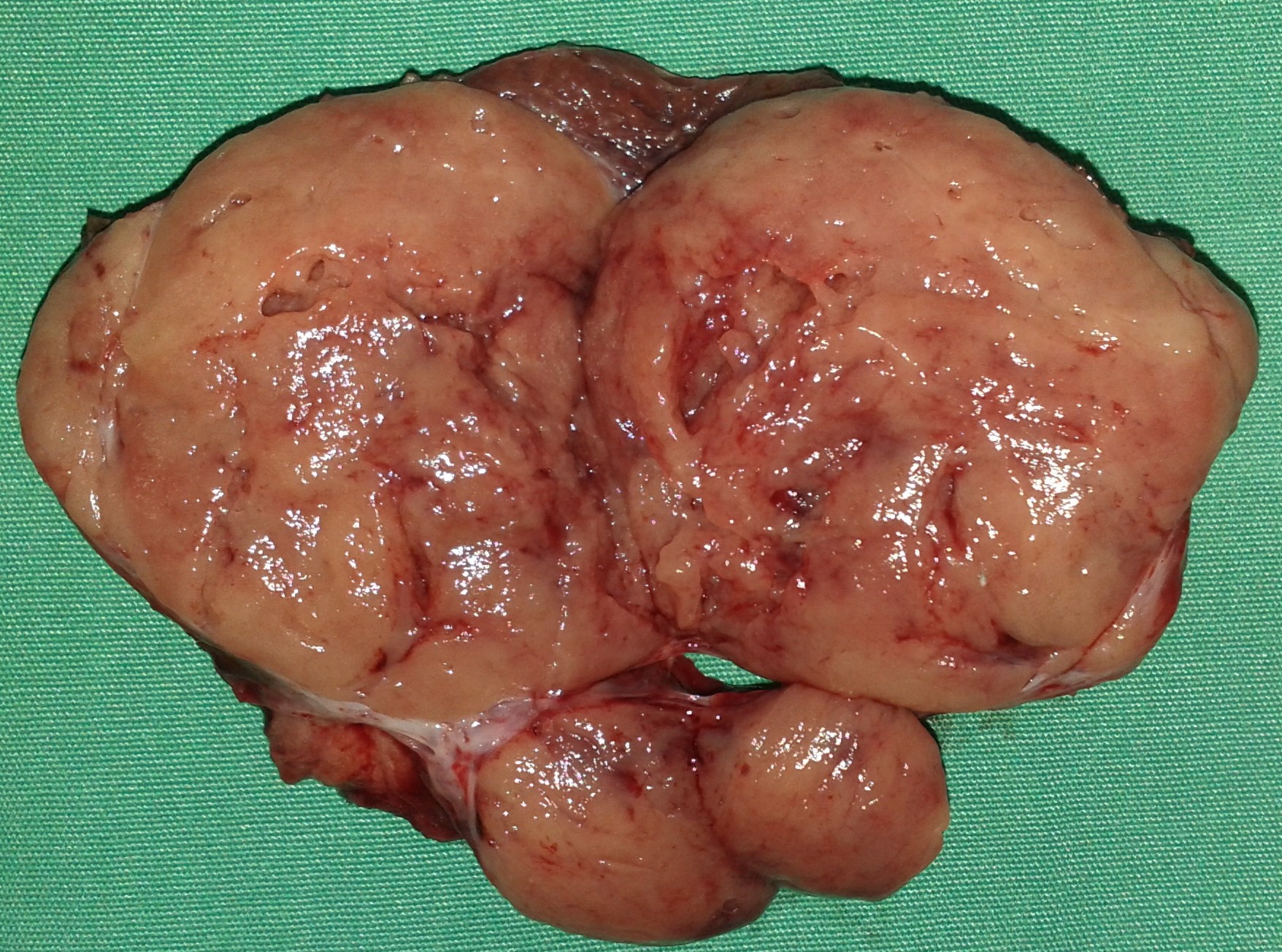
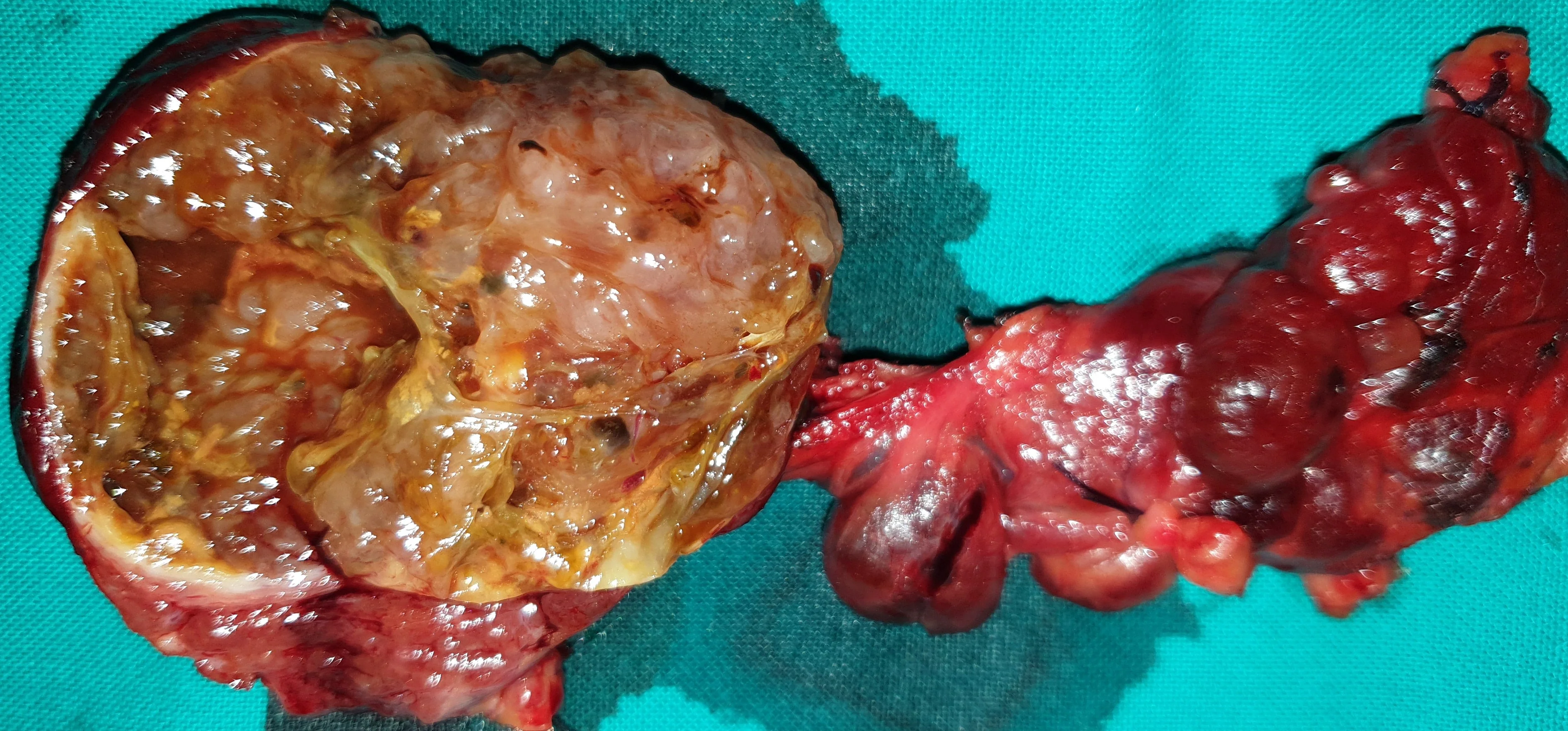
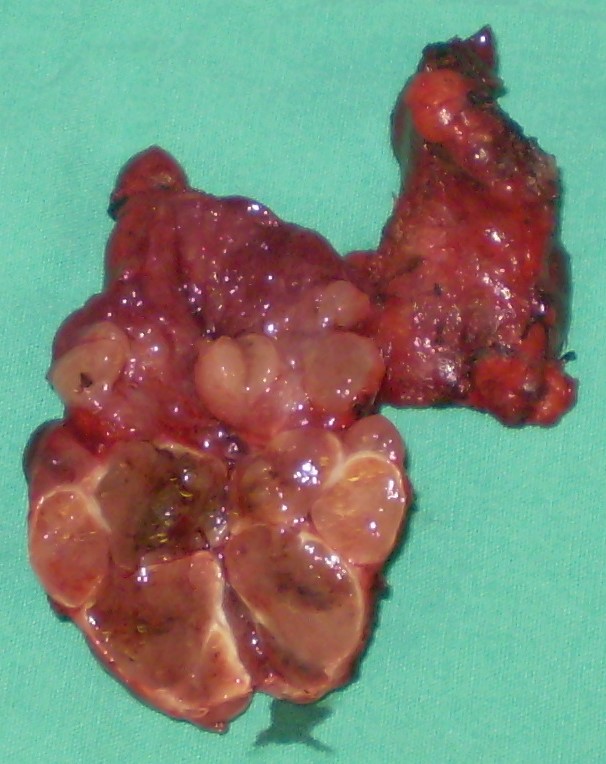
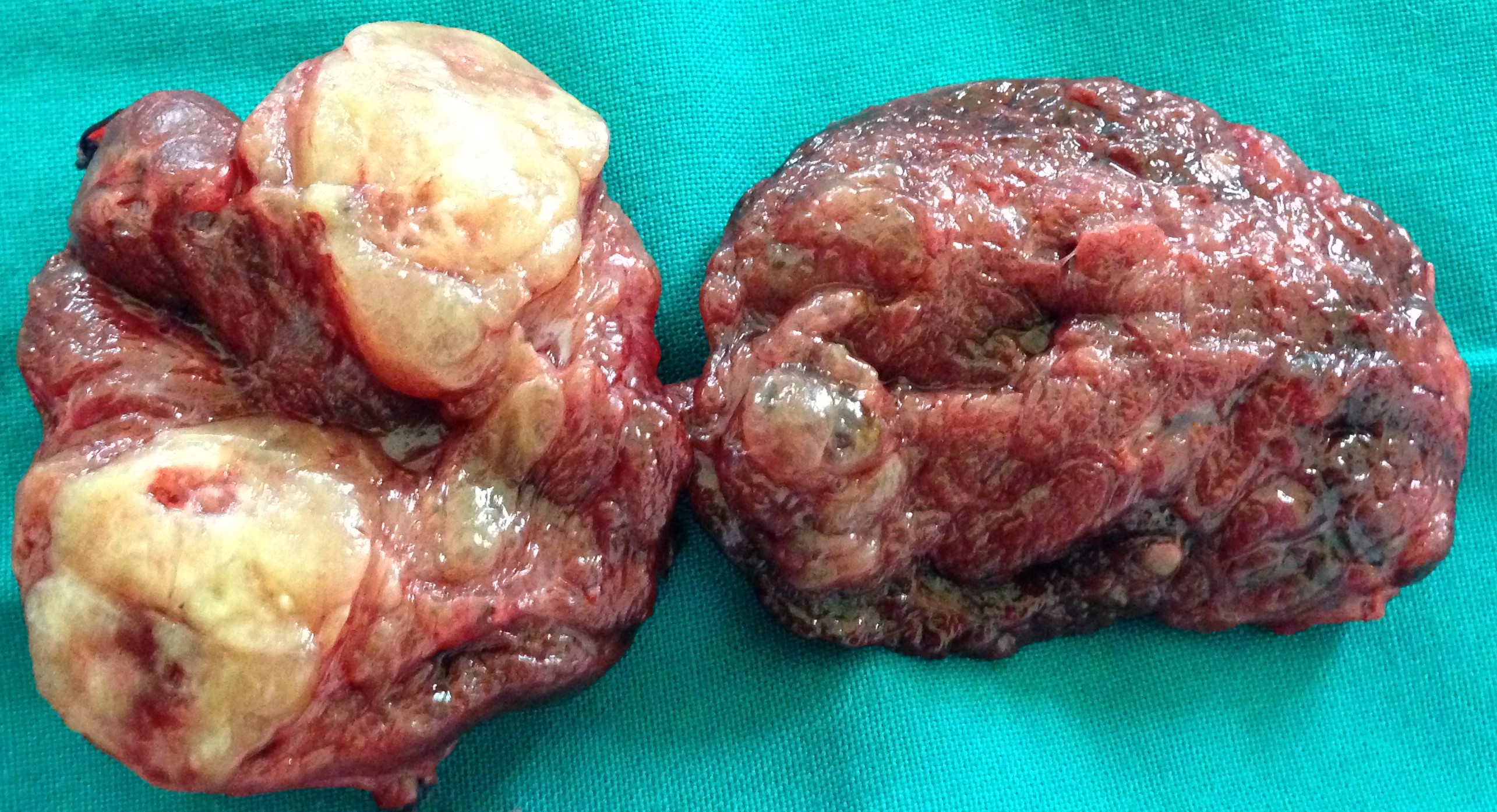
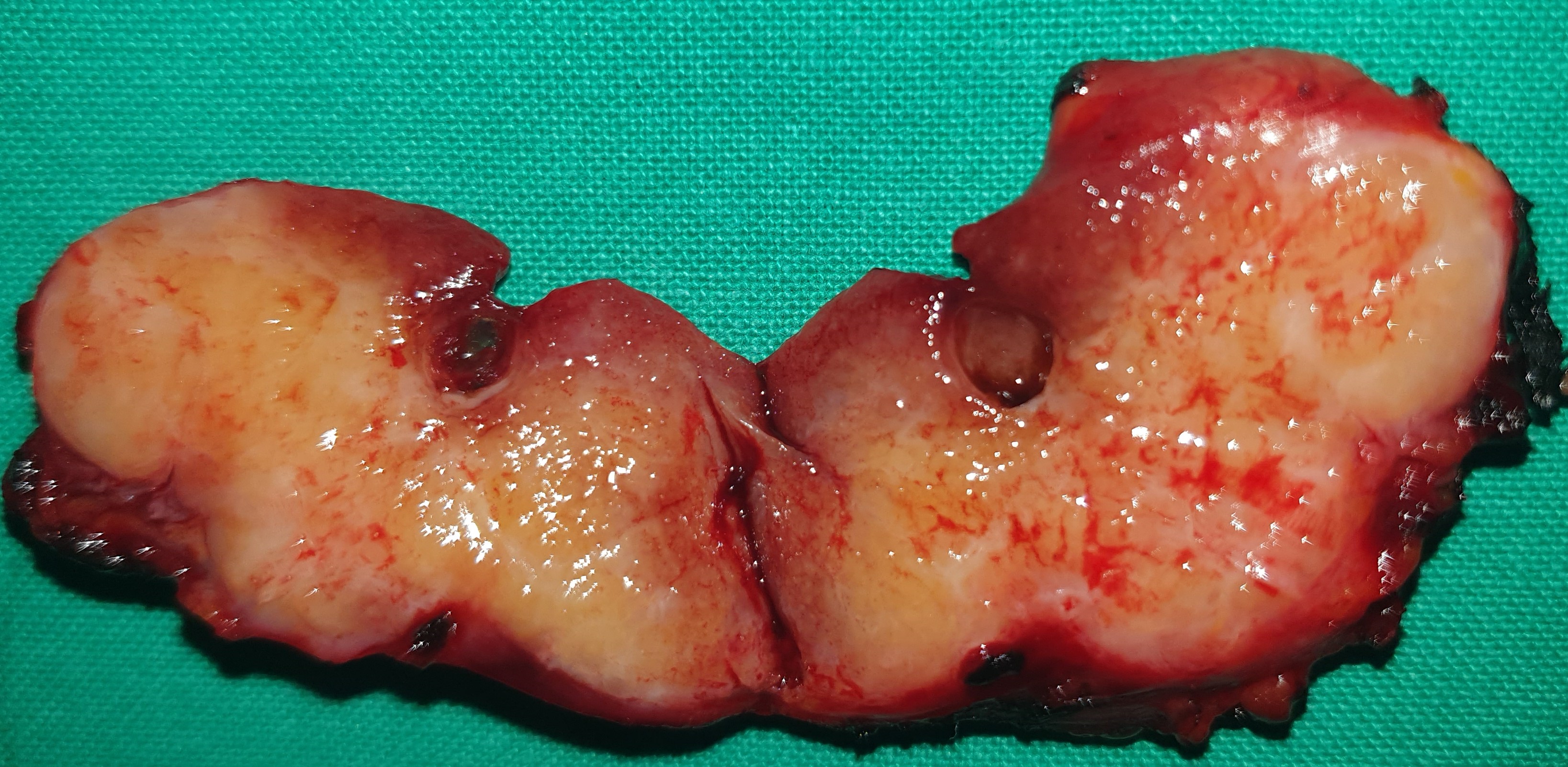
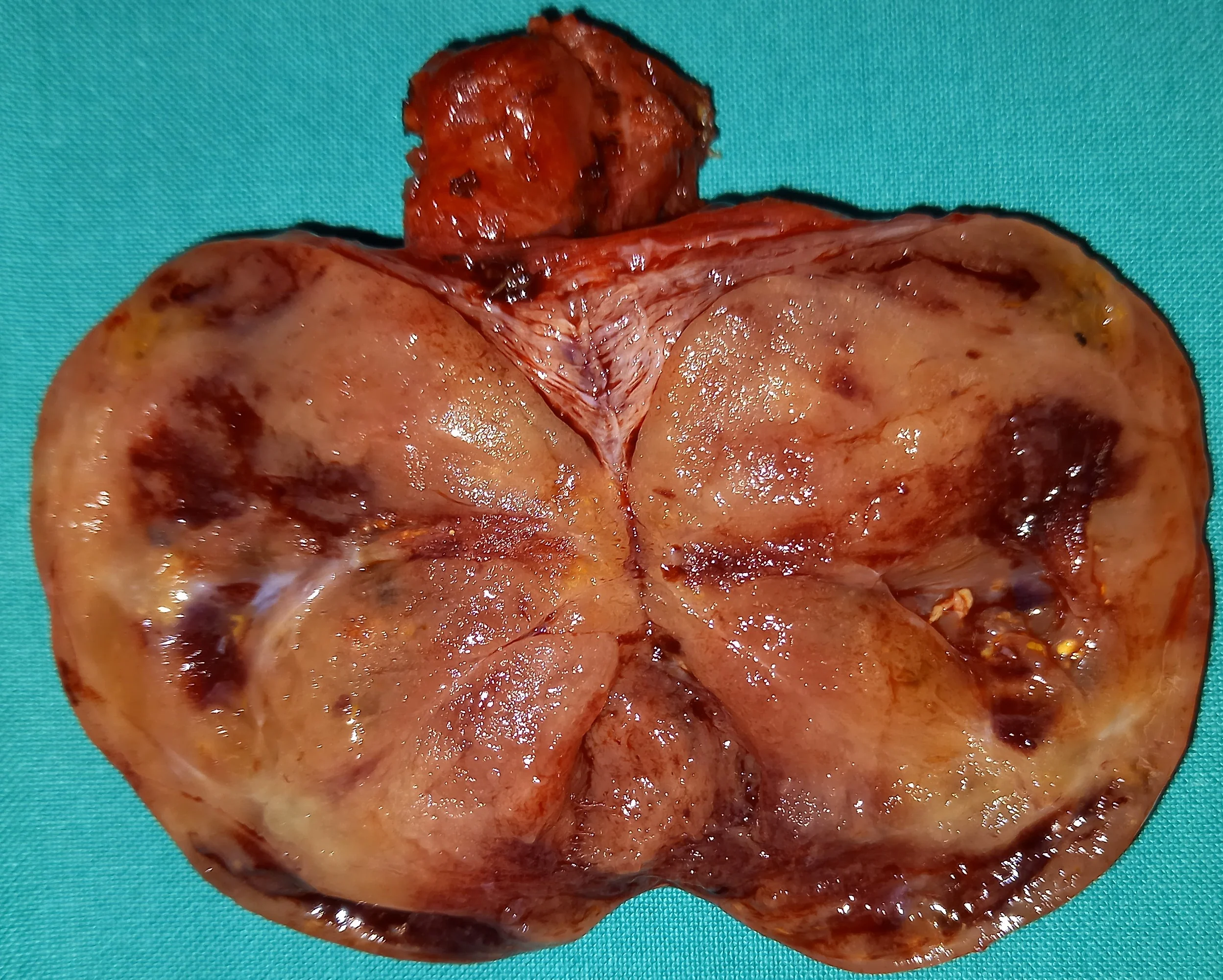
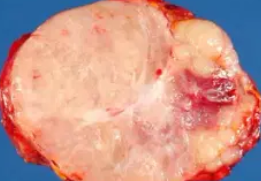
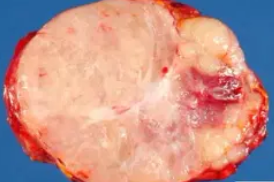
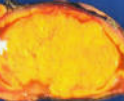
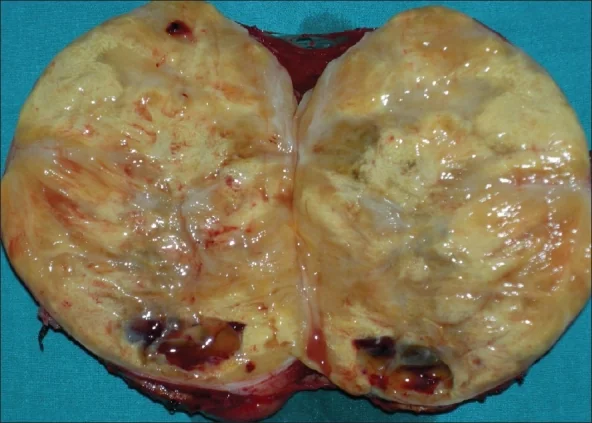
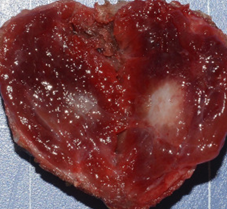
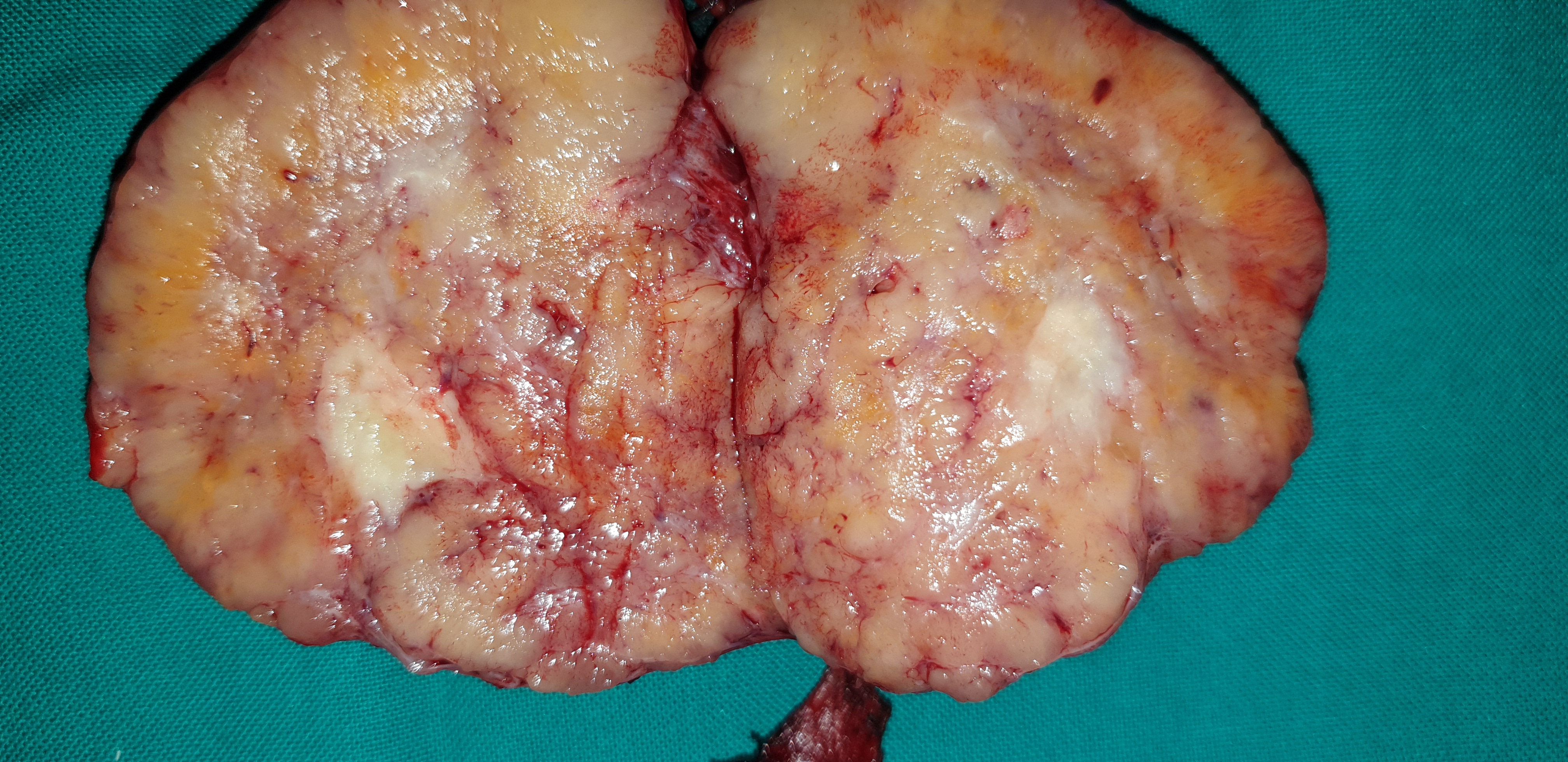
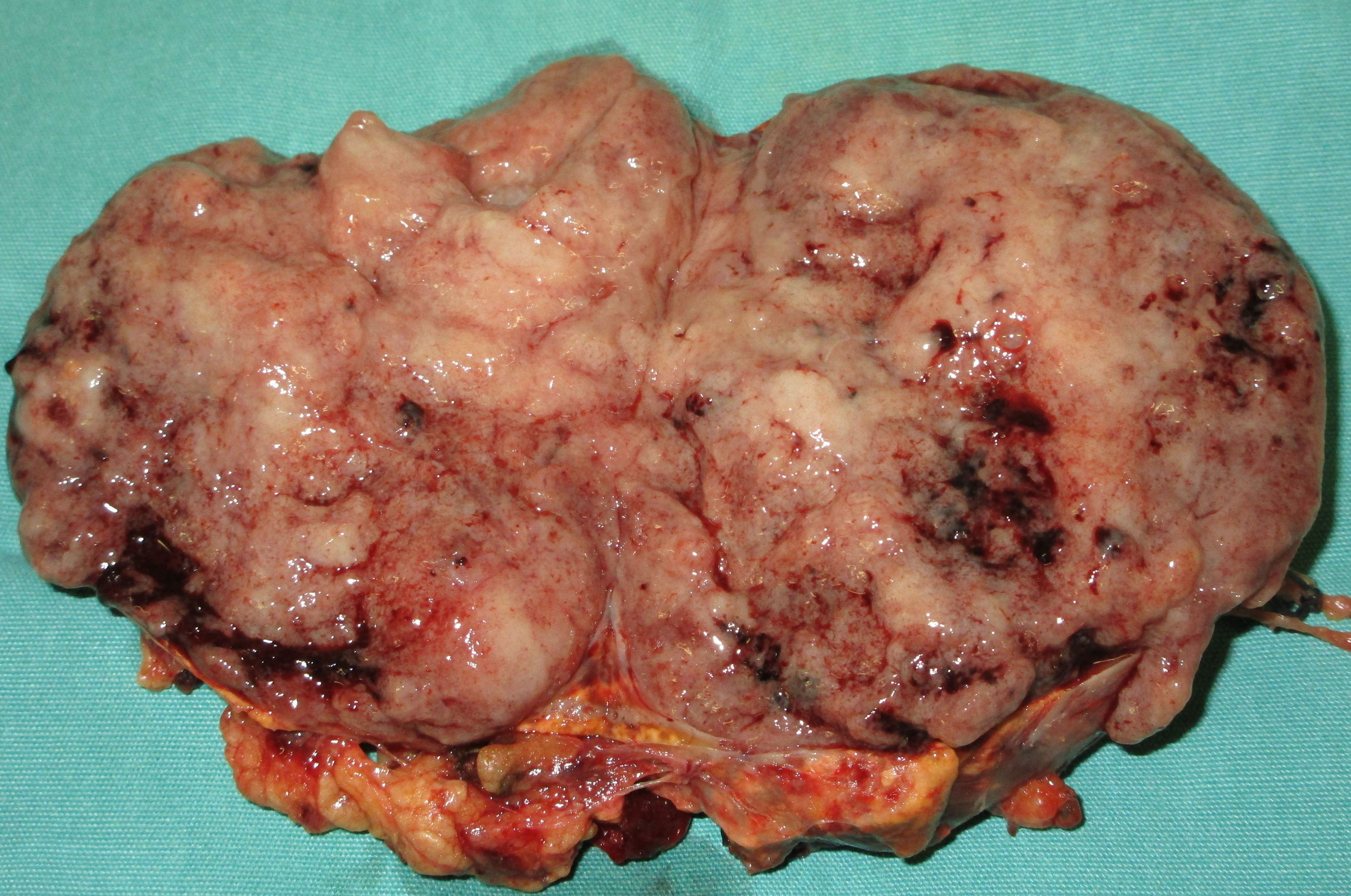
Cross section of large superior parathyroid adenoma.(Courtesy Dr. V. Penopoulos).
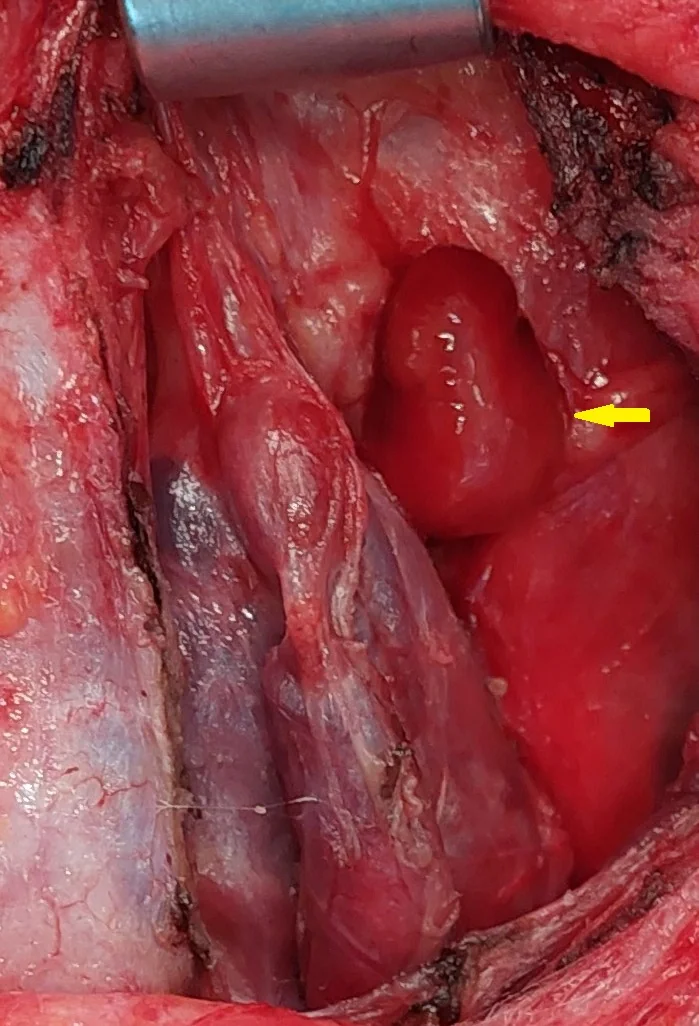
Purple arrow: over-descended large superior parathyroid adenoma. Yellow arrow: normal right inferior parathyroid gland found in the thymothyroid ligament (Courtesy Dr. V. Penopoulos)
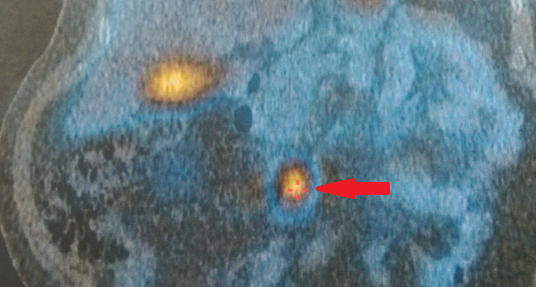
Sestamibi scintigraphy. Presence of a right inferior parathyroid adenoma.(Courtesy Dr. V. Penopoulos).

Purple arrow: over-descended large superior parathyroid adenoma. Yellow arrow: normal right inferior parathyroid gland found in the thymothyroid ligament (Courtesy Dr. V. Penopoulos)

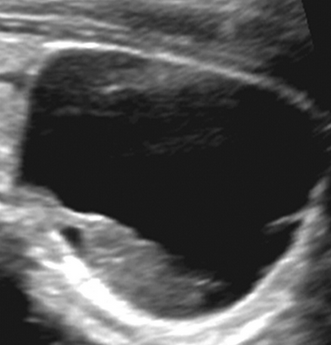
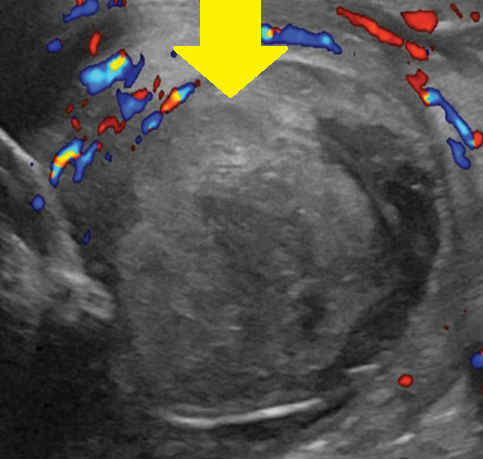
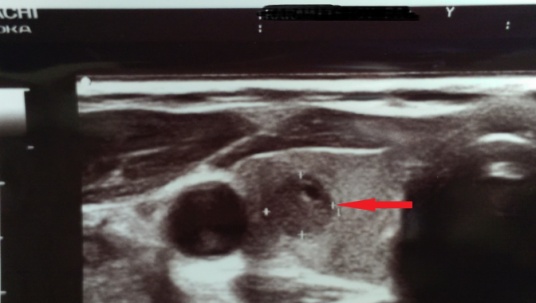
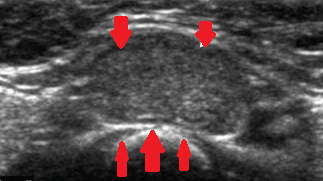
Neck ultrasound. Presence of a right inferior parathyroid adenoma (Courtesy Dr. V. Penopoulos)
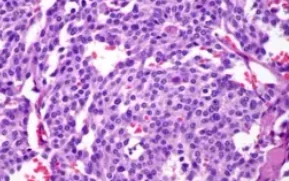
Papillary thyroid carcinoma,with characteristic nuclear features(nuclear crowding, overlapping, clearing, membrane irregularities and inclusions). (Courtesy Dr . V . Penopoulos) .
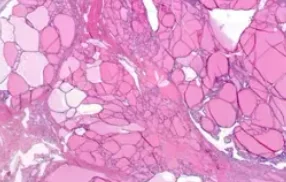
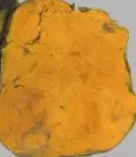
Thyroid follicular carcinoma widely invading the thyroid capsule.(Courtesy Dr.V.Penopoulos).
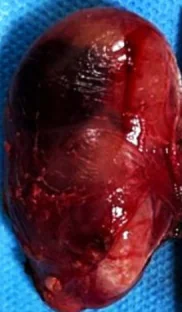
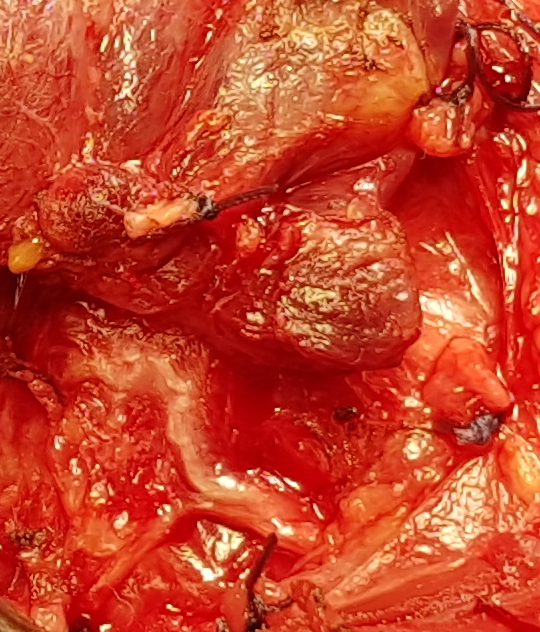
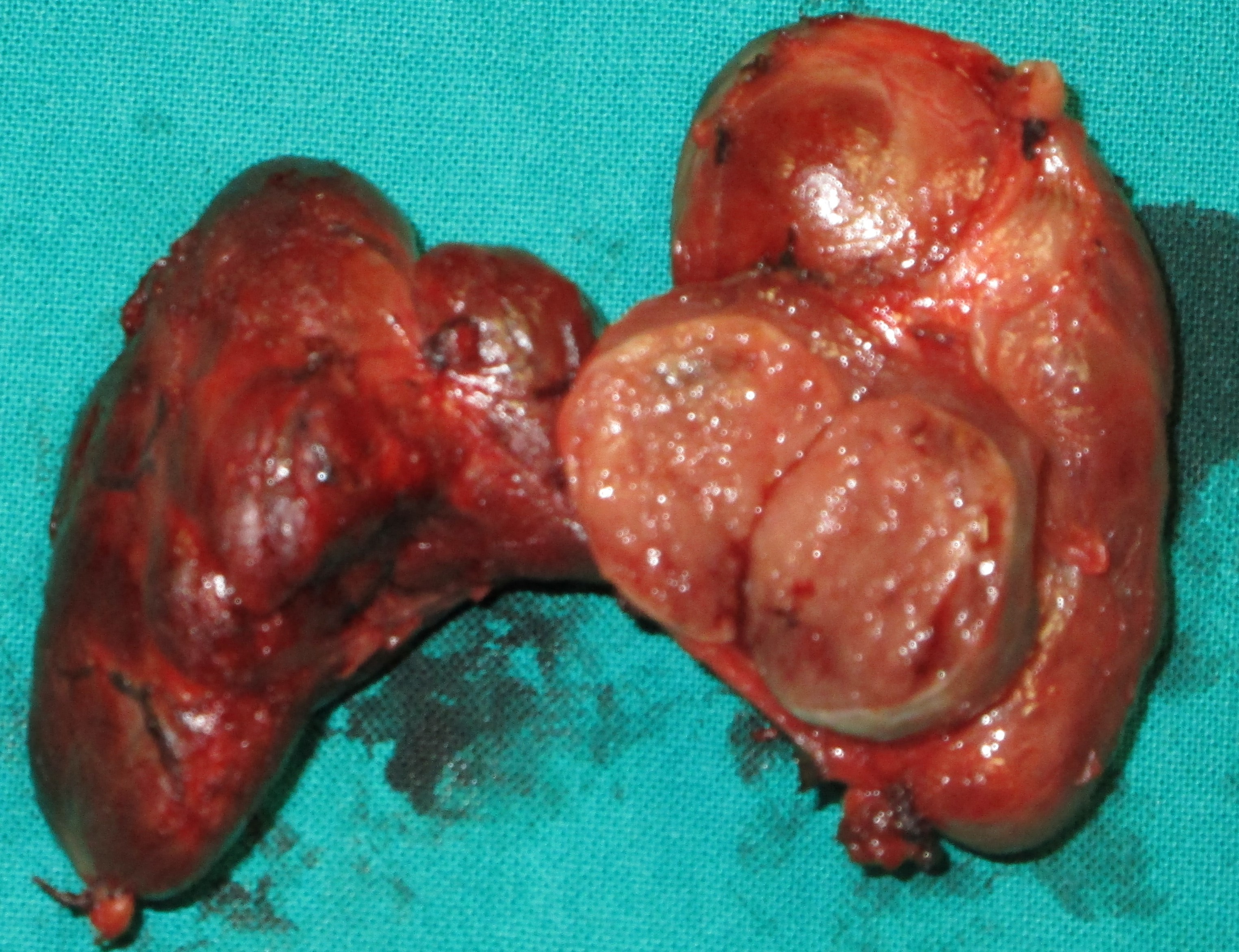
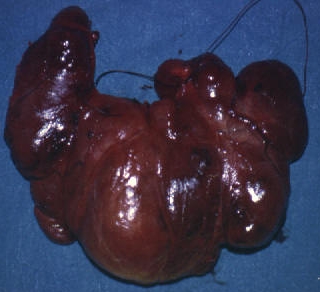
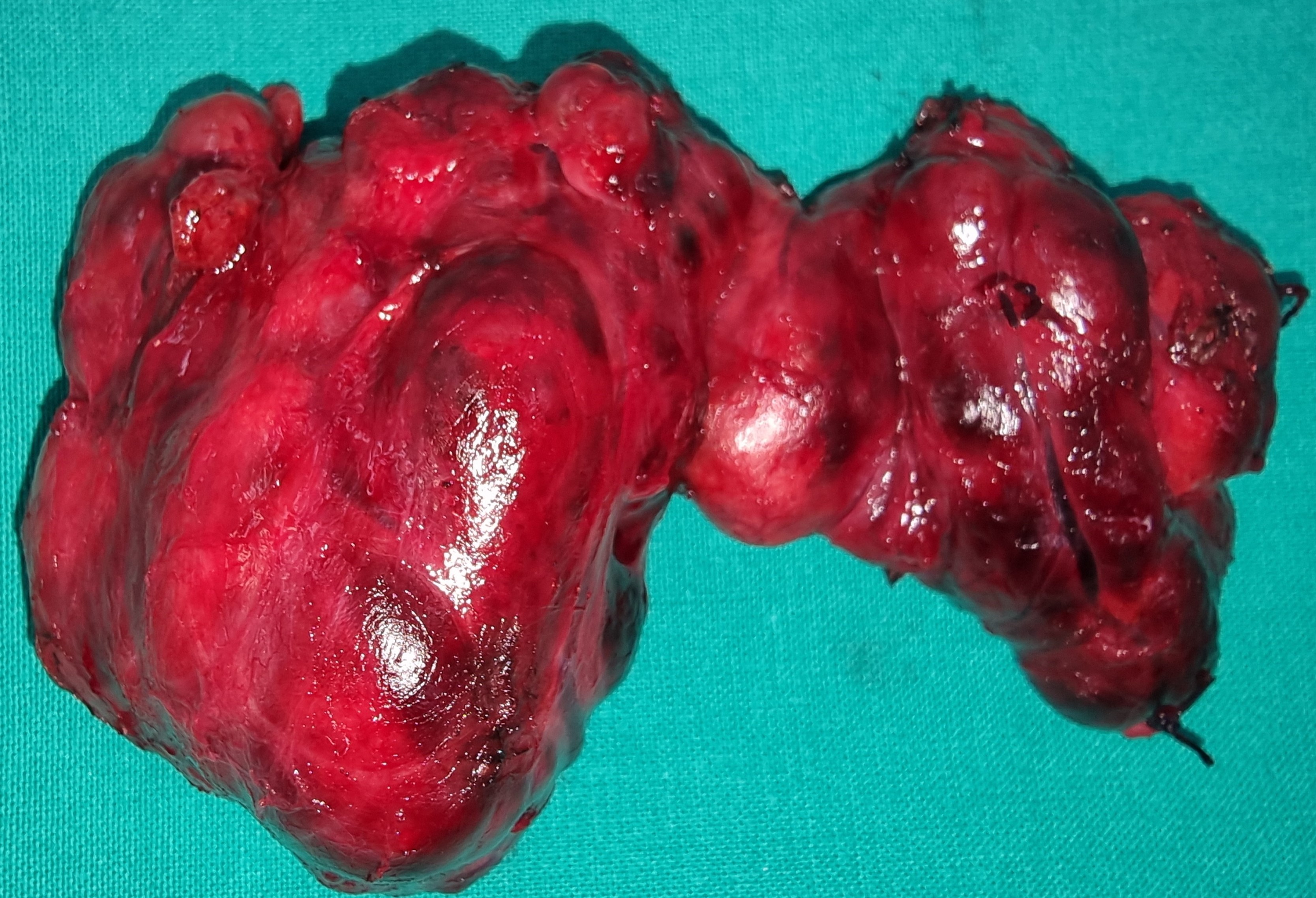
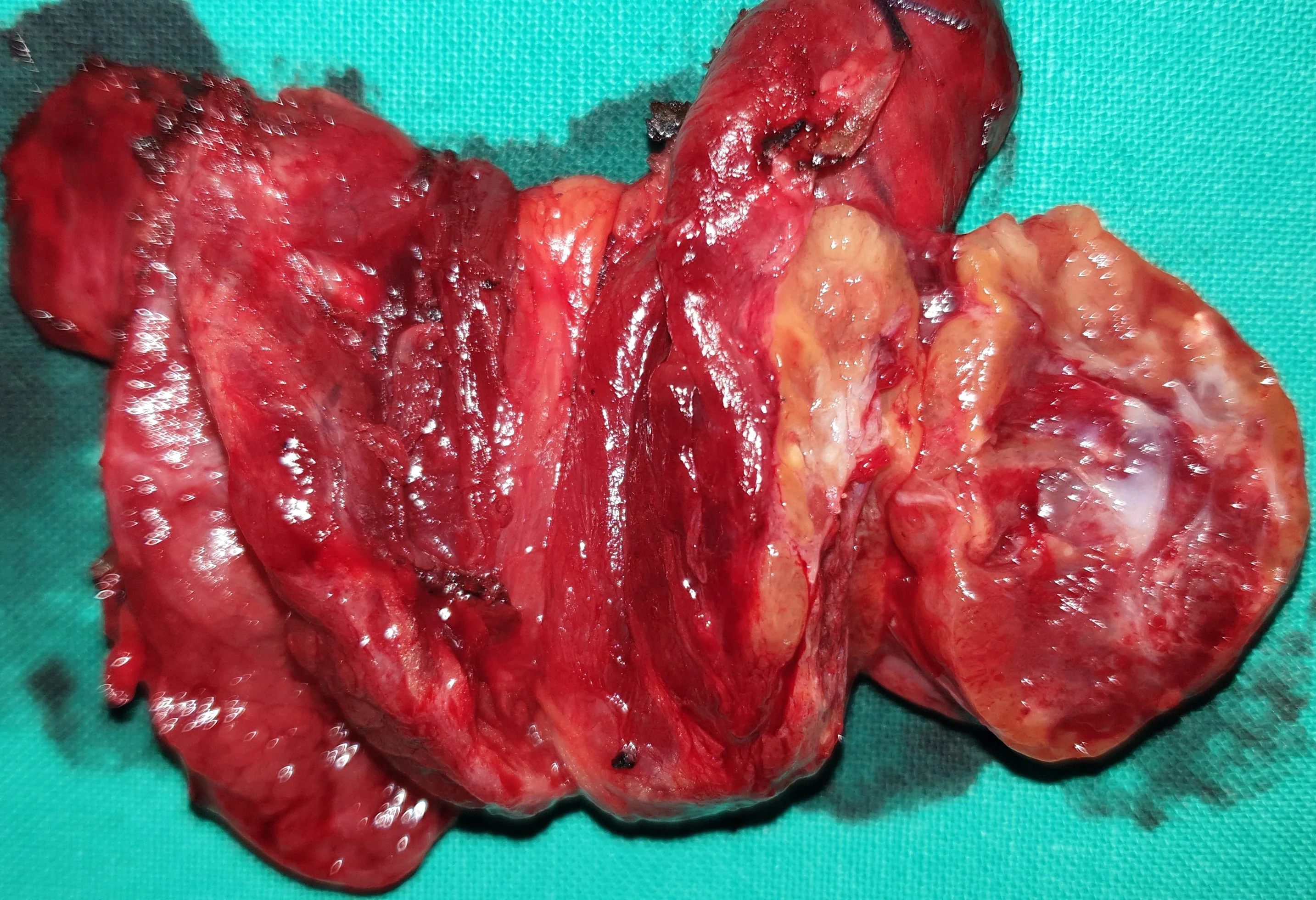
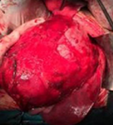
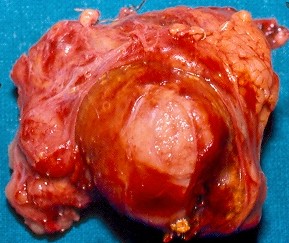
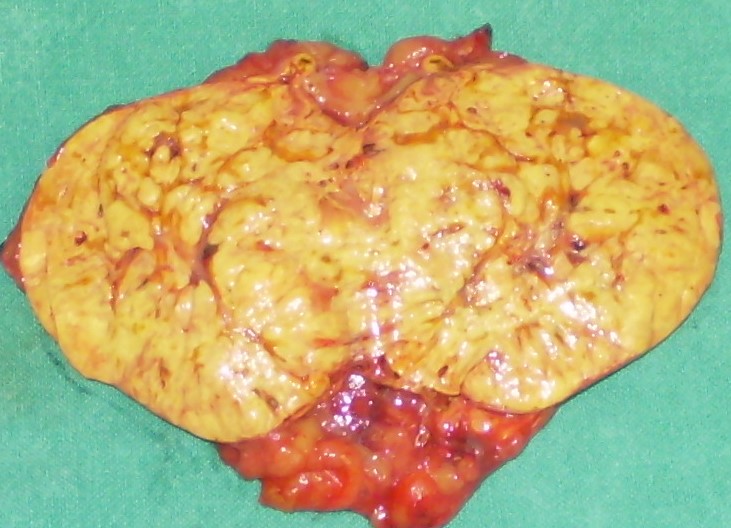
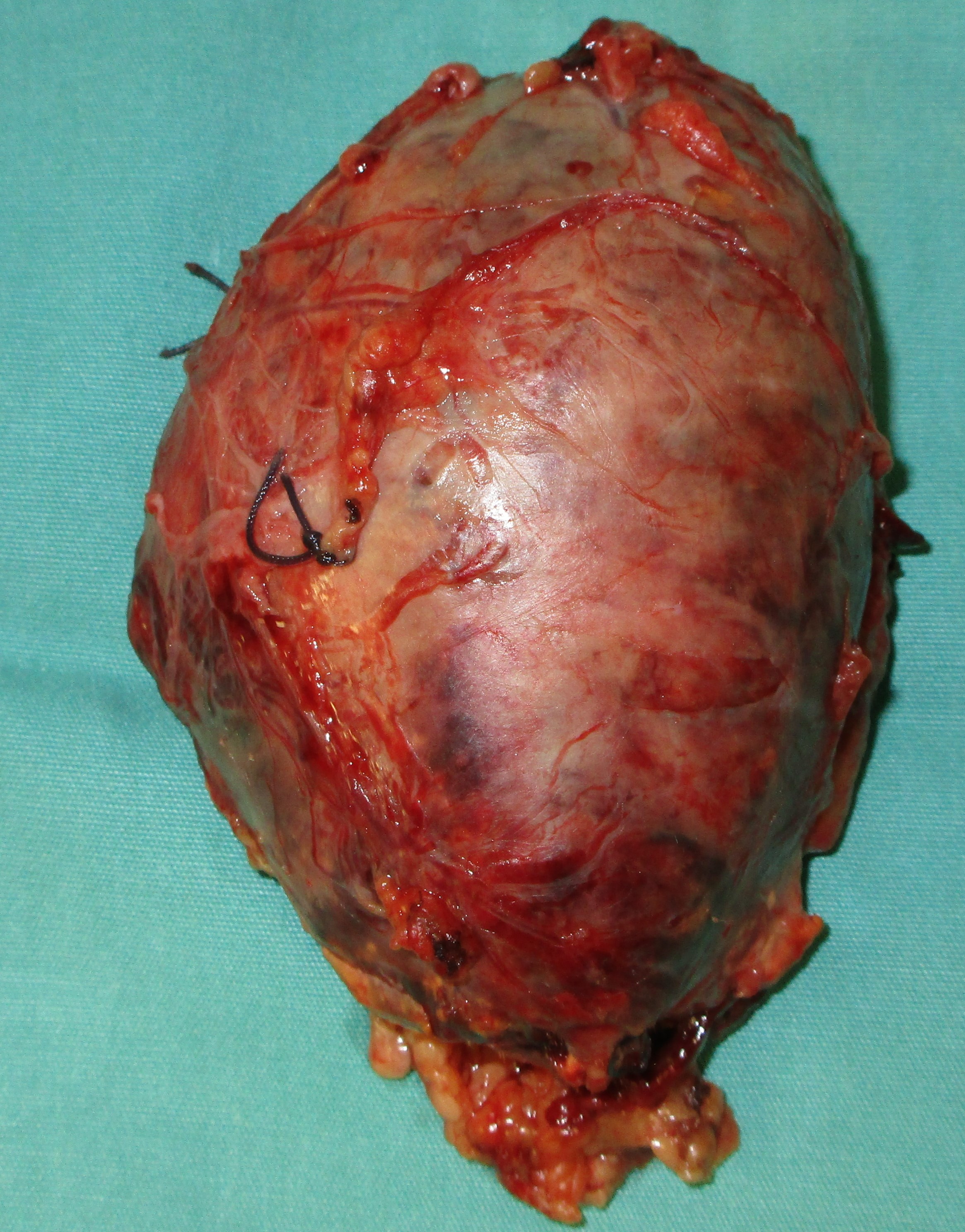
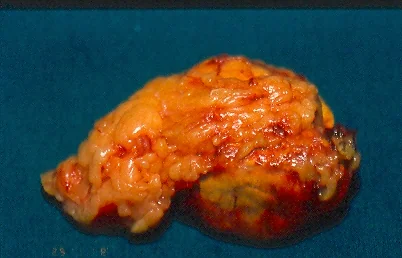
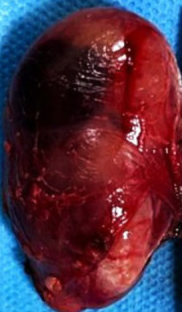
Surgical specimen of cystic phaeochromocytoma .Intratumoral hemorrhage.( Courtesy Dr . V . Penopoulos ).

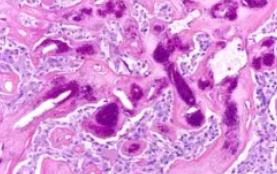
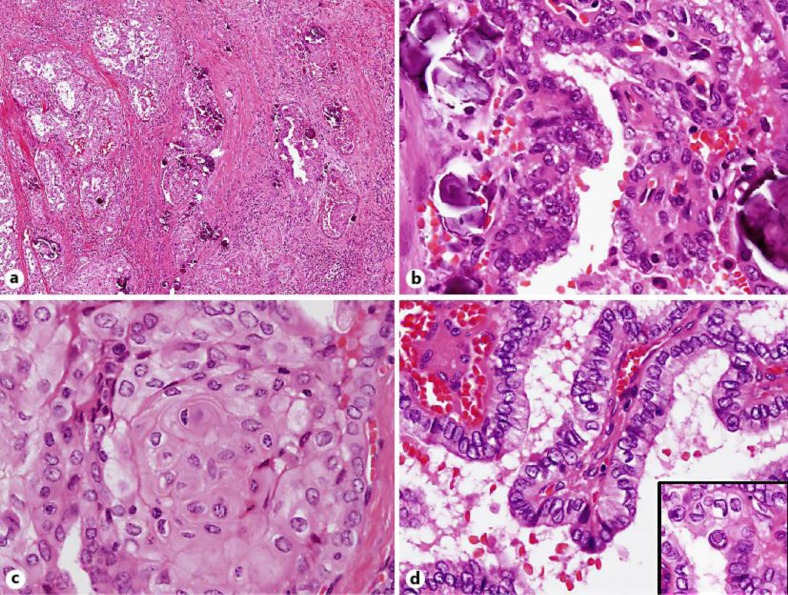
Histopathological examination of parathyroid adenocarcinoma (Courtesy Dr. V. Penopoulos)


PET scan. Findings consistent with parathyroid carcinoma (Courtesy Dr. V. Penopoulos)



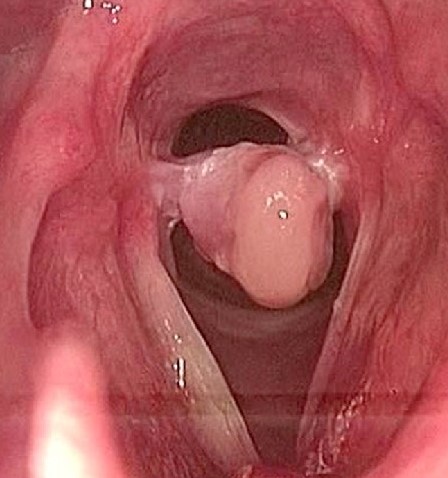
Endoscopic image of downhill varices, below the upper esophageal sphincter.(Courtesy Dr. V. Penopoulos).
Histopathological examination of parathyroid adenocarcinoma (Courtesy Dr. V. Penopoulos)

The diffuse sclerosing papillary carcinoma of the right lobe is evident . Two groups of infiltrated lymph nodes are also seen (Courtesy Dr. V. Penopoulos)
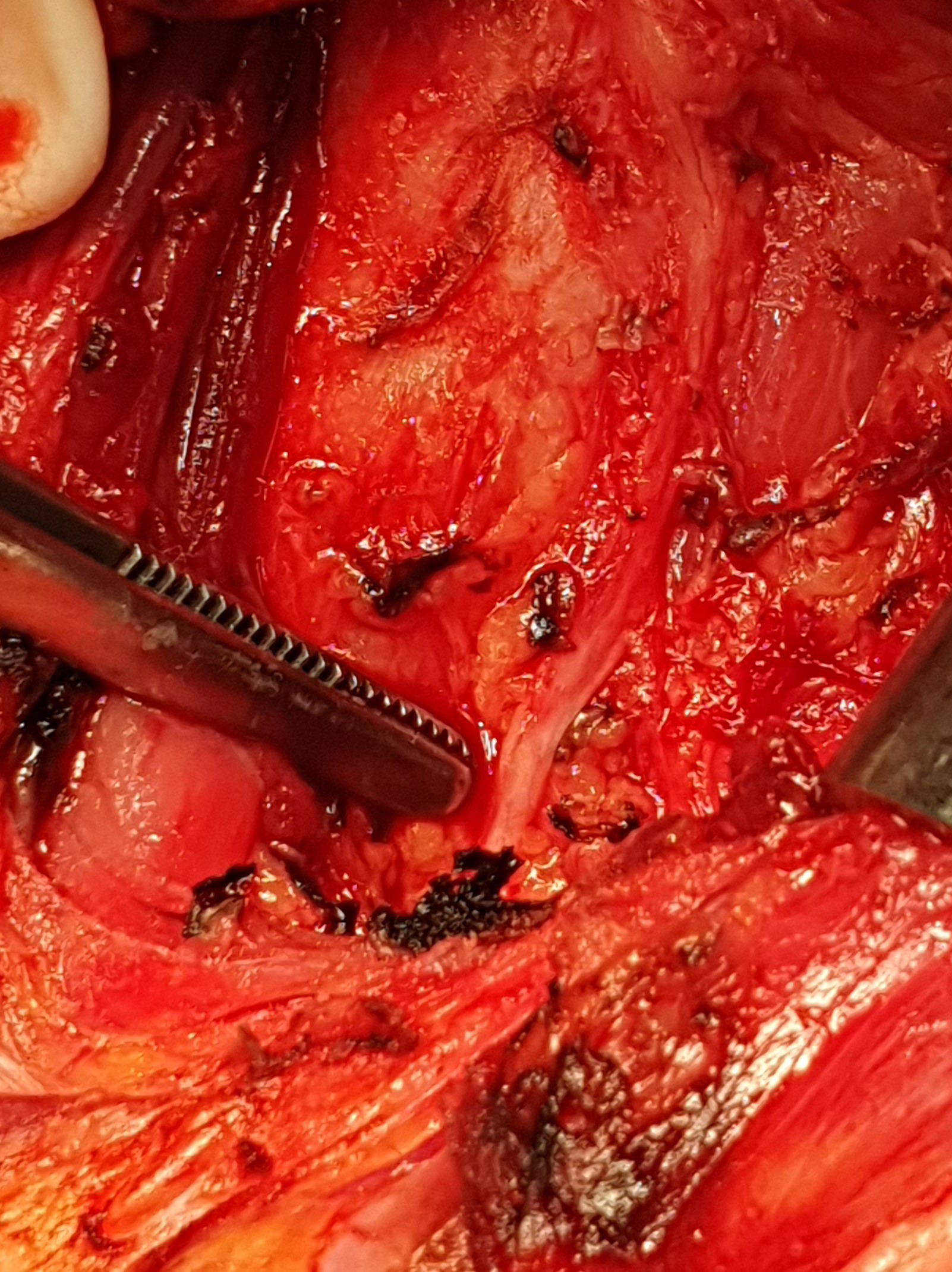
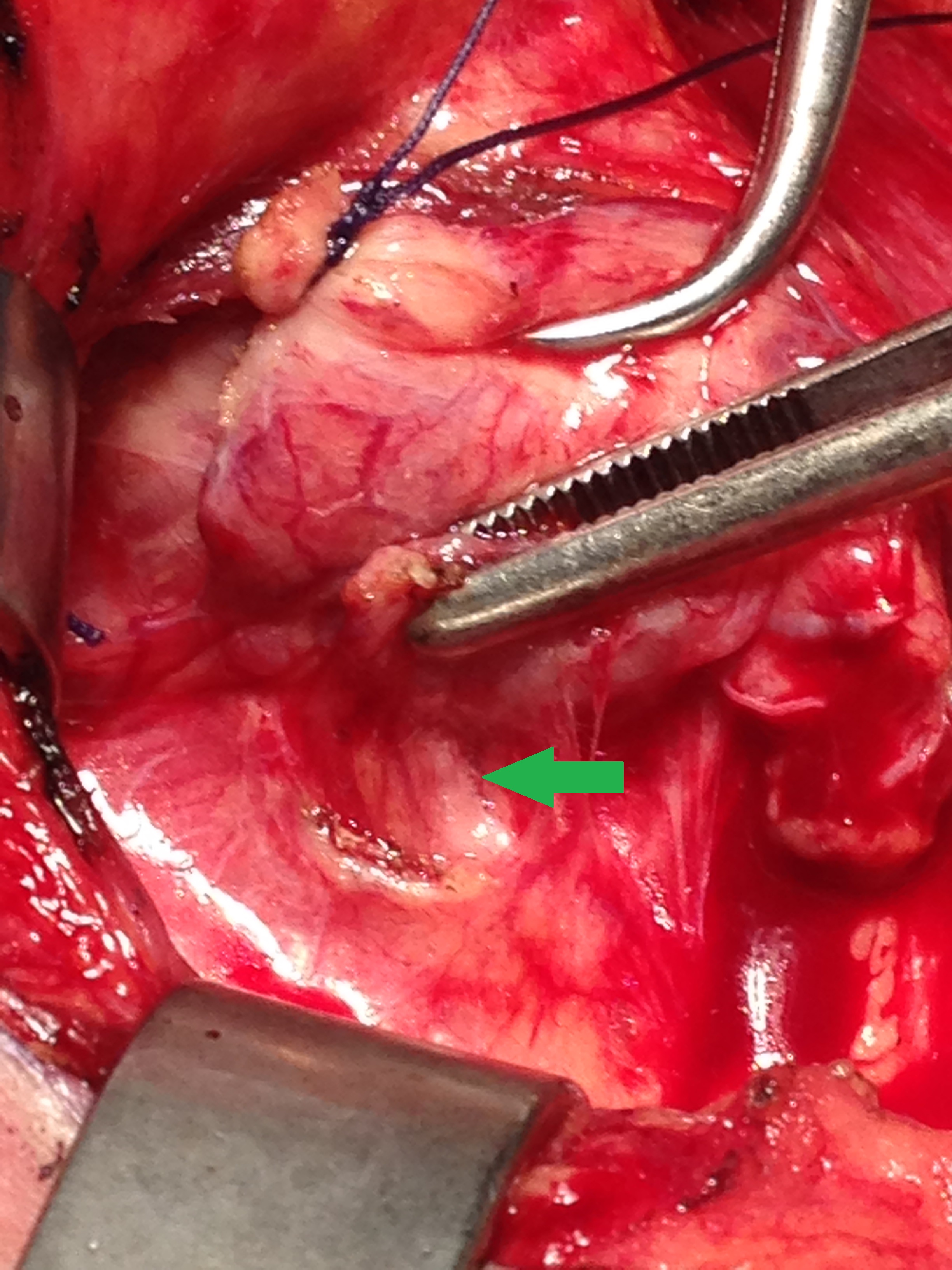
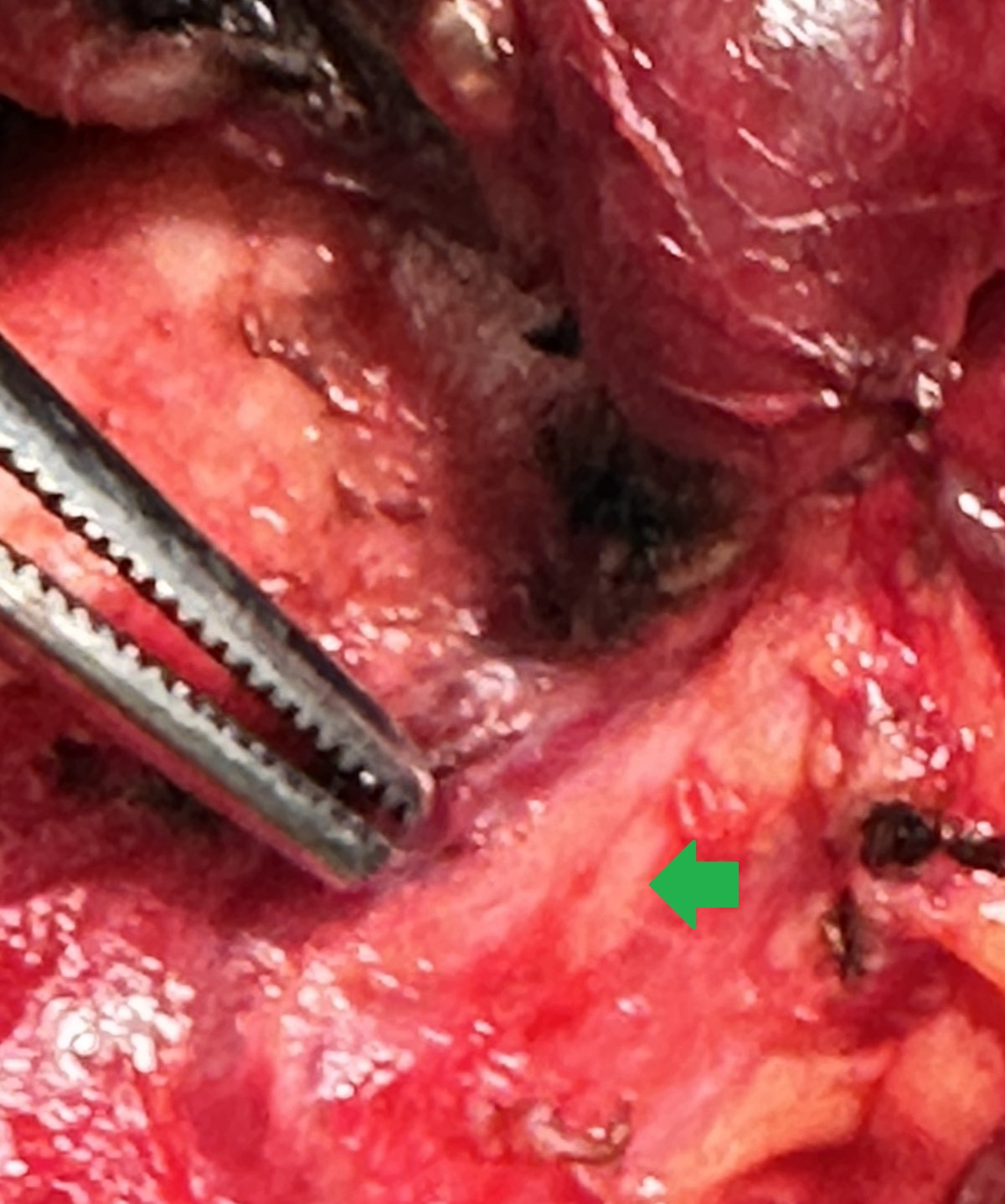
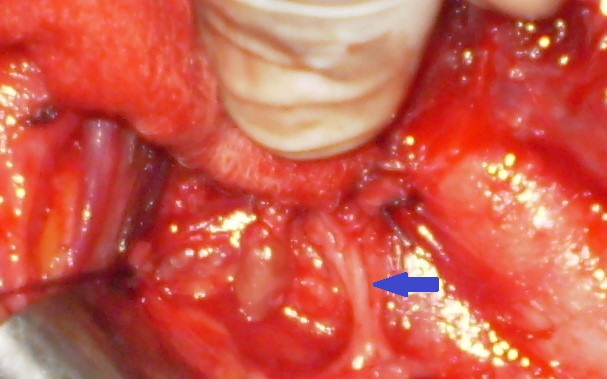
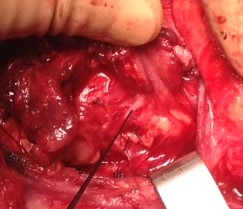
The right inferior laryngeal nerve was densely adherent to the papillary tumor (Courtesy Dr. V. Penopoulos)


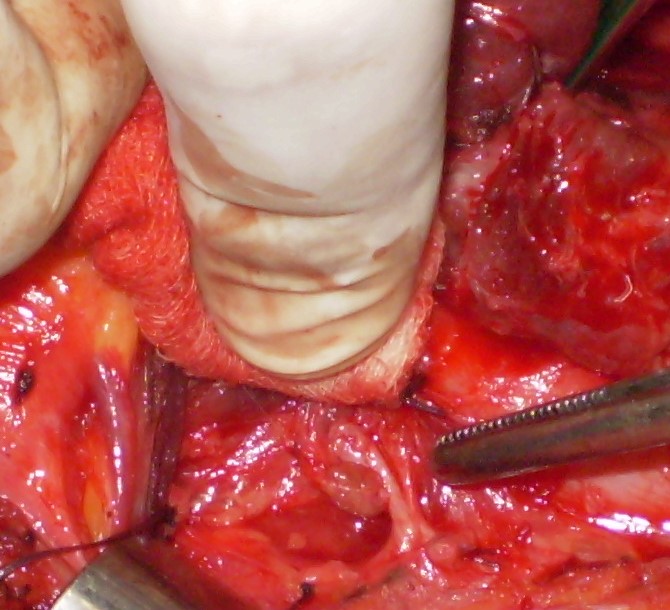
Right recurrent laryngeal nerve adherent to parathyroid cyst.(Courtesy Dr.V.Penopoulos).
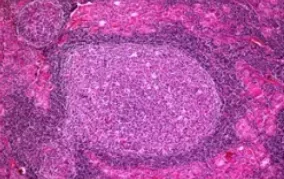
A growing papillary tumor with remarkable fibrosis and lymphocytic infiltration is clearly seen (Courtesy Dr. V. Penopoulos)

Postoperative endoscopy and chest-neck CT. Complete disappearance of the esophageal varices (Courtesy Dr. V. Penopoulos)

Postoperative chest-neck CT. Complete disappearance of the esophageal varices (Courtesy Dr. V. Penopoulos)

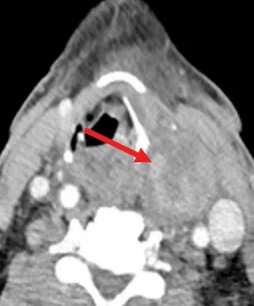
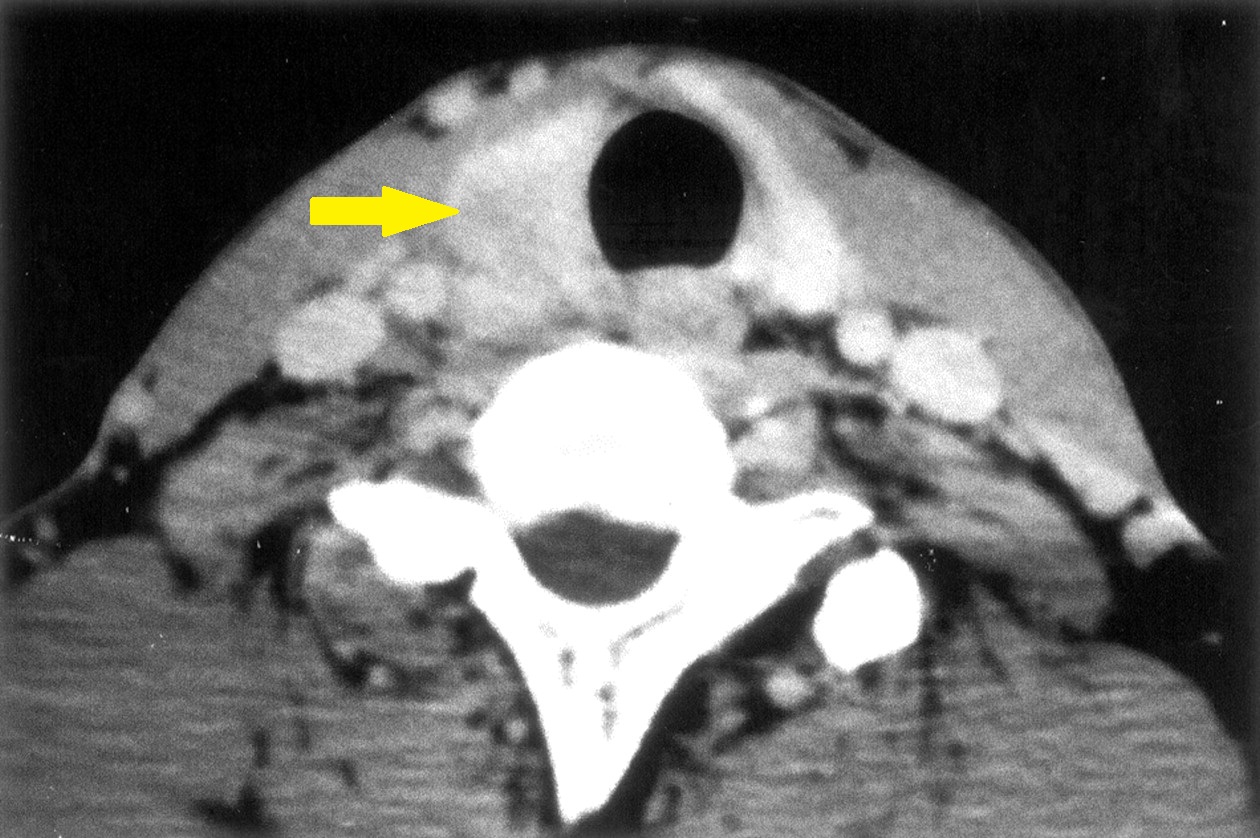
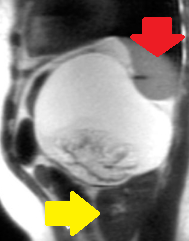
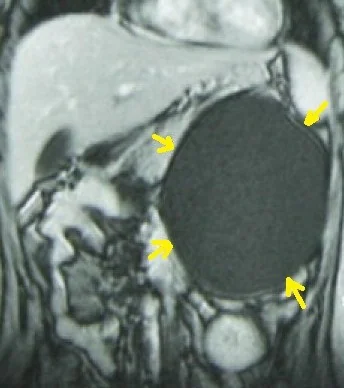
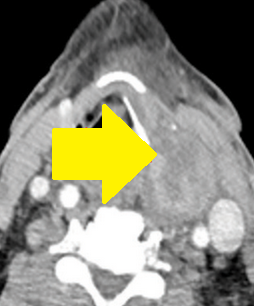
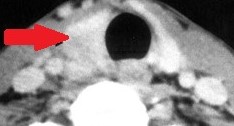
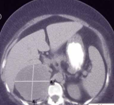
Neck CT. Red arrow — Large cyst on the right, compressing the esophagus, with well-defined margins and colloid content (Courtesy Dr. V. Penopoulos)


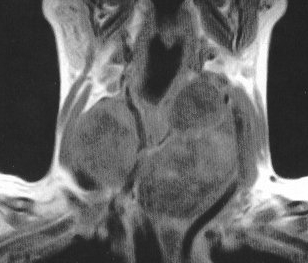
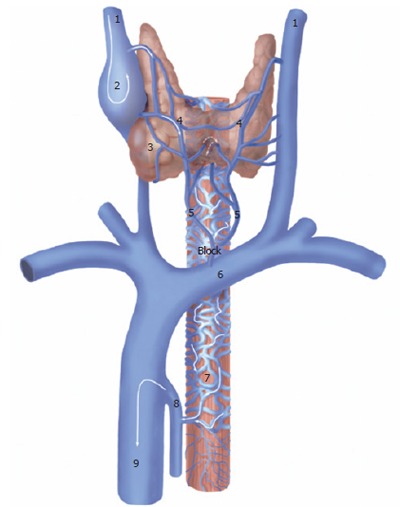
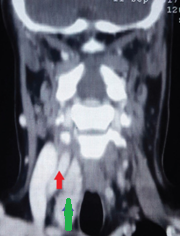
Yellow arrow: dilated venous plexus. Green arrow: trachea. Purple arrow: enlarged right thyroid lobe with central cystic degeneration (Courtesy Dr. V. Penopoulos)

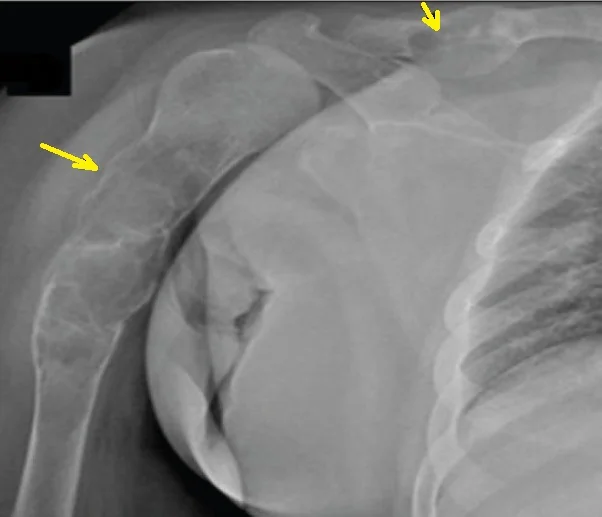
Chest-neck CT. Red outline: enlarged right thyroid lobe. Green arrow: mild pressure on the trachea. Red arrow: downhill esophageal varices (Courtesy Dr. V. Penopoulos)

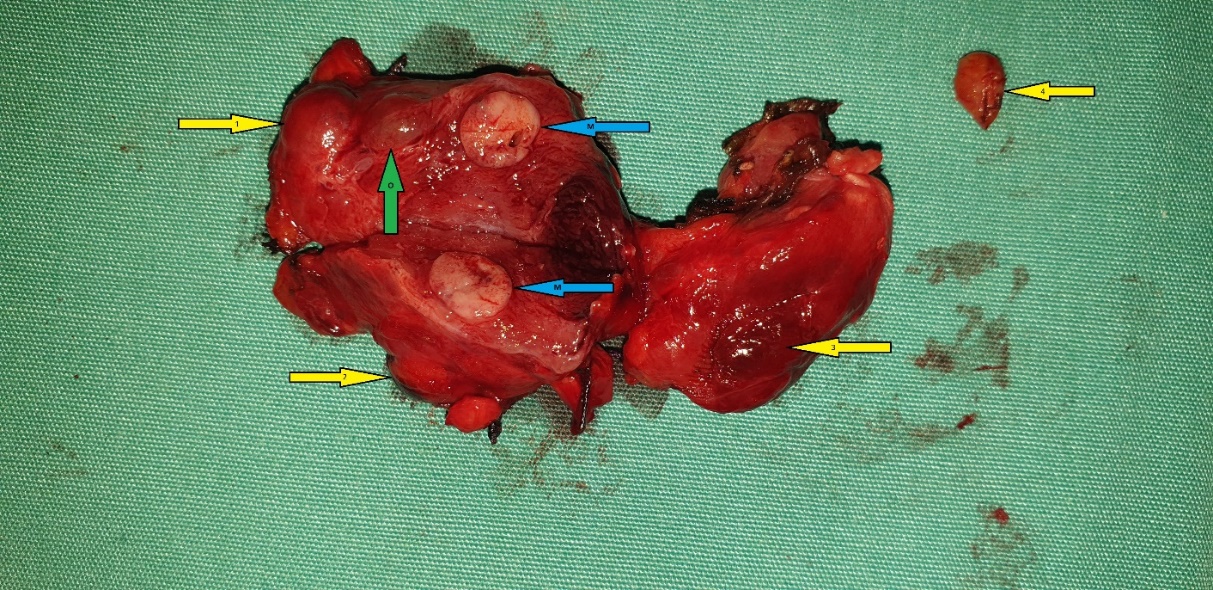
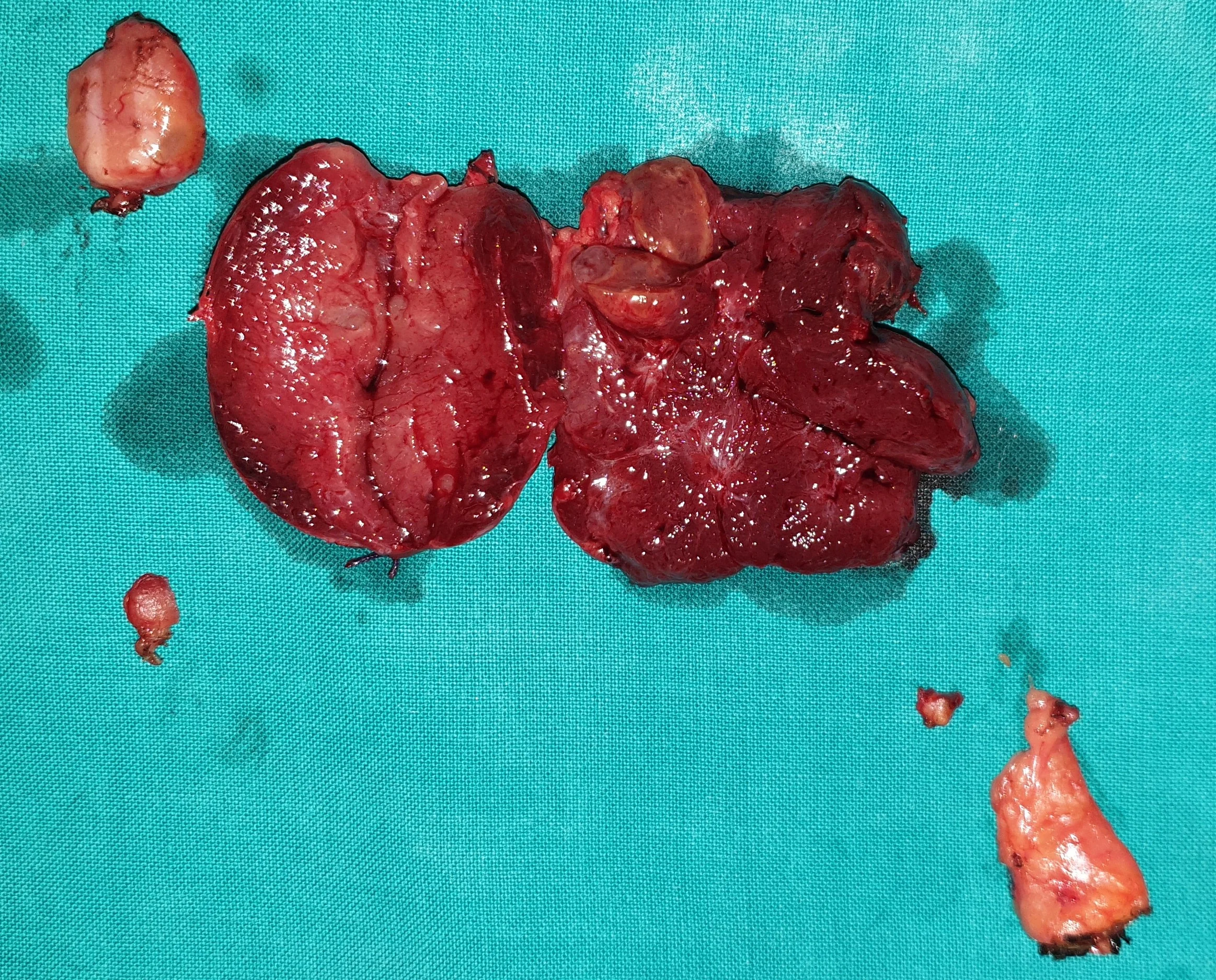
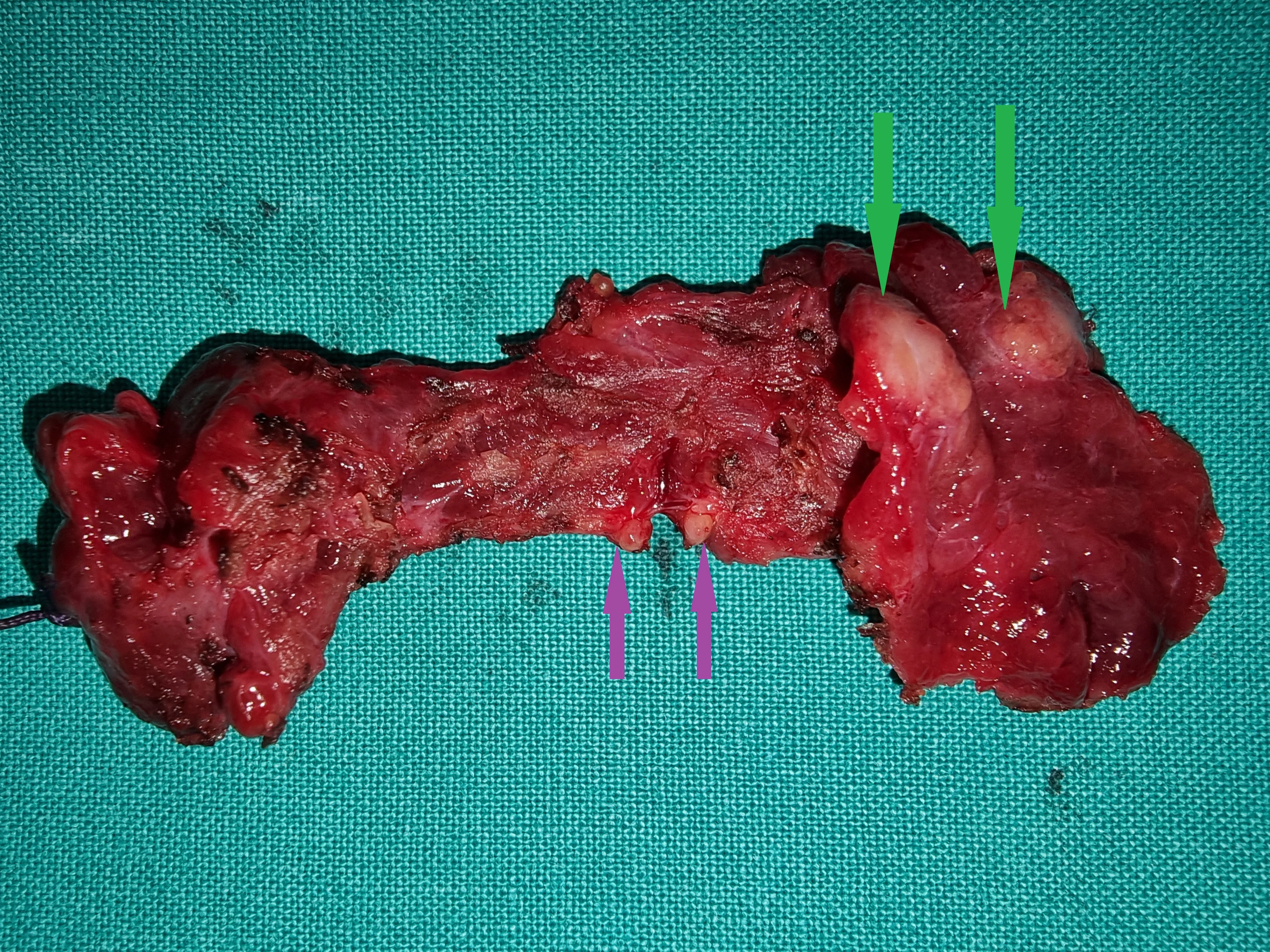
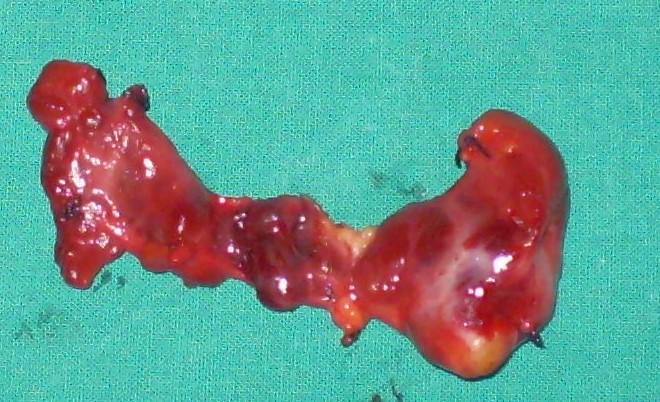
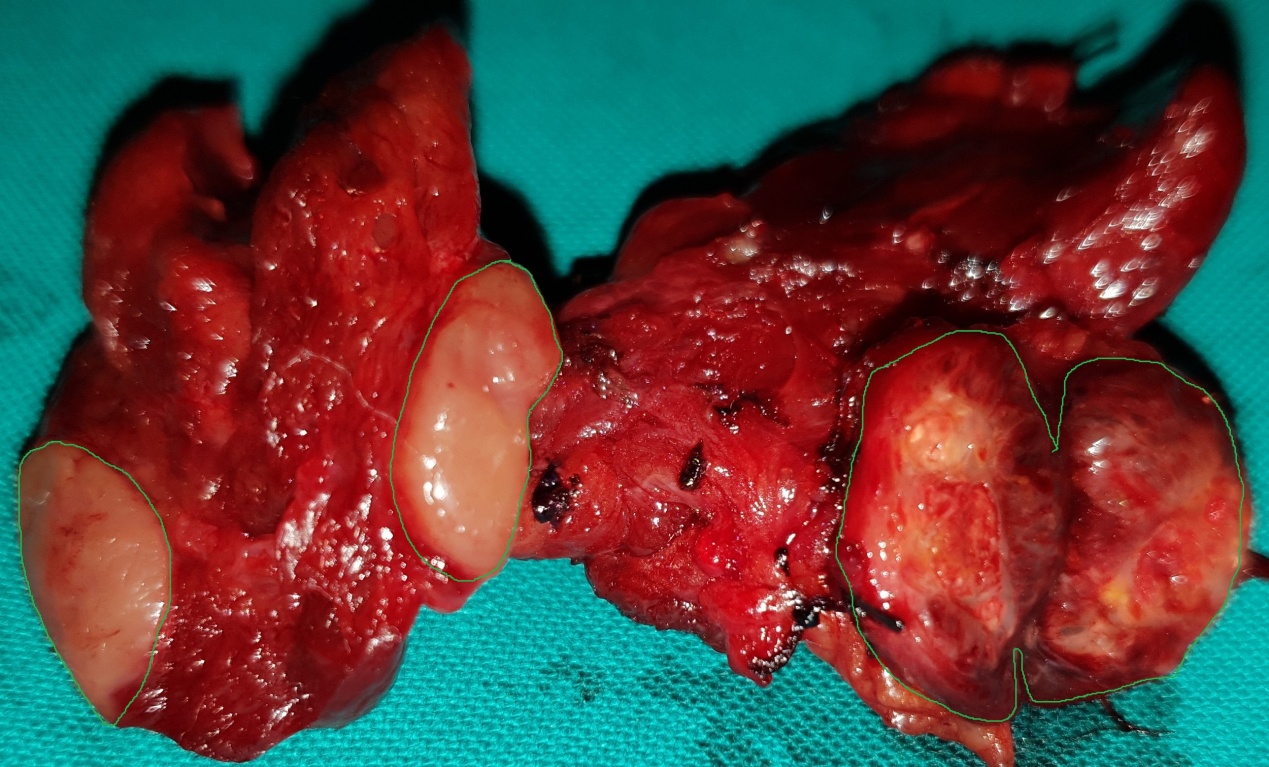
Figure 5 . Surgical specimen a) Blue arrows: encapsulated medullary microcarcinoma b) Yellow arrows : parathyroid glands . c) Green arrow : Benign thyroid nodule . ( Courtesy Dr . V . Penopoulos ) .
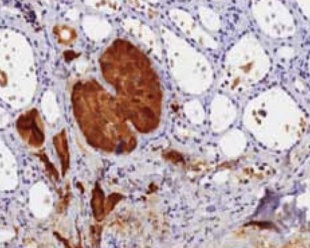
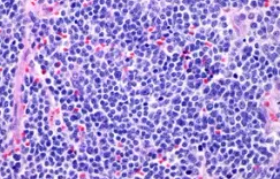
Figure 7 . Epithelial cells with an organoid and trabecular pattern with positive immunohystochemical staining for calcitonin .

Thyroid U/S . Encapsulated medullary microcarcinoma . (Courtesy Dr . V . Penopoulos) .

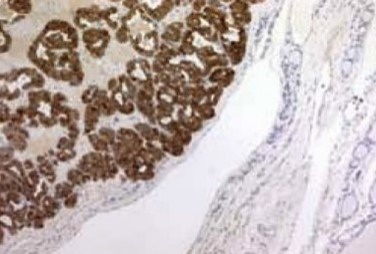
Figure 6 . Epithelial cells with an organoid and trabecular pattern with positive immunohystochemical staining for chromogranin .

Figure 1 . Signaling pathways implicated in medullary thyroid carcinoma tumorigenesis .

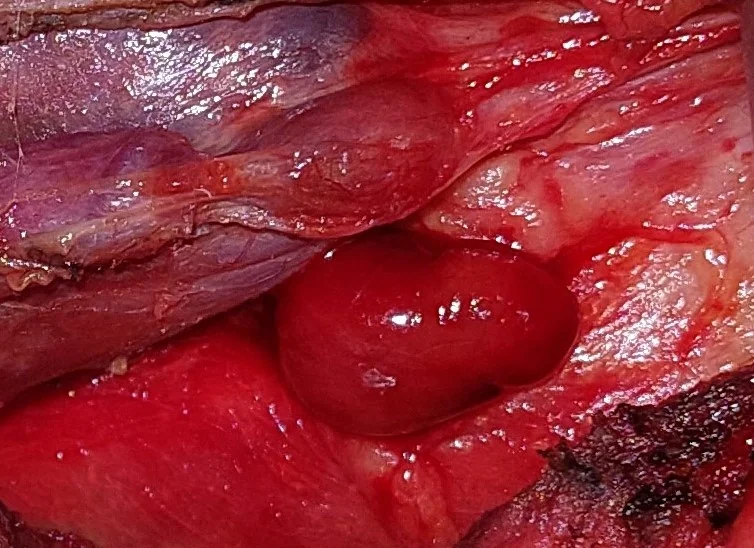
Parathyroid adenoma lying posteriorly of the right common carotid artery.(Courtesy Dr.V.Penopoulos).
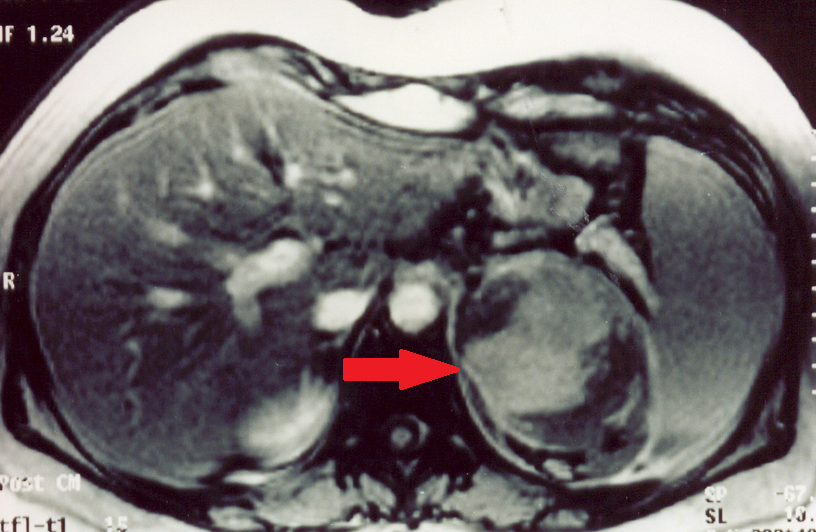
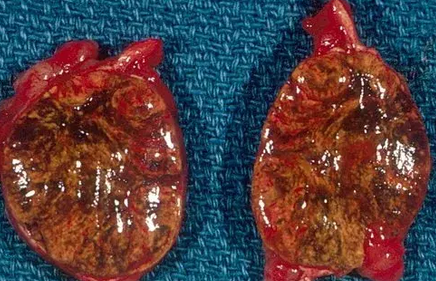
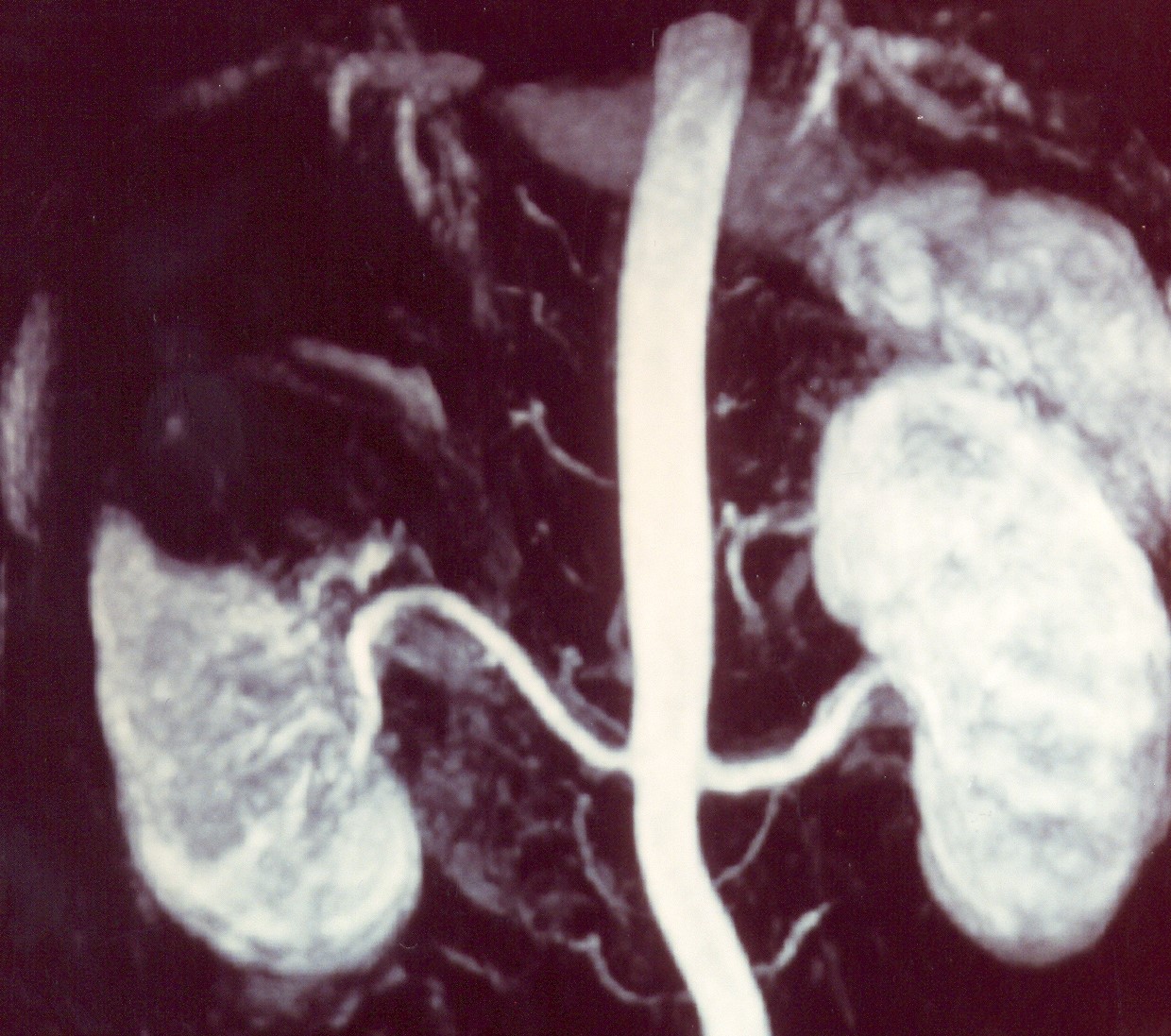
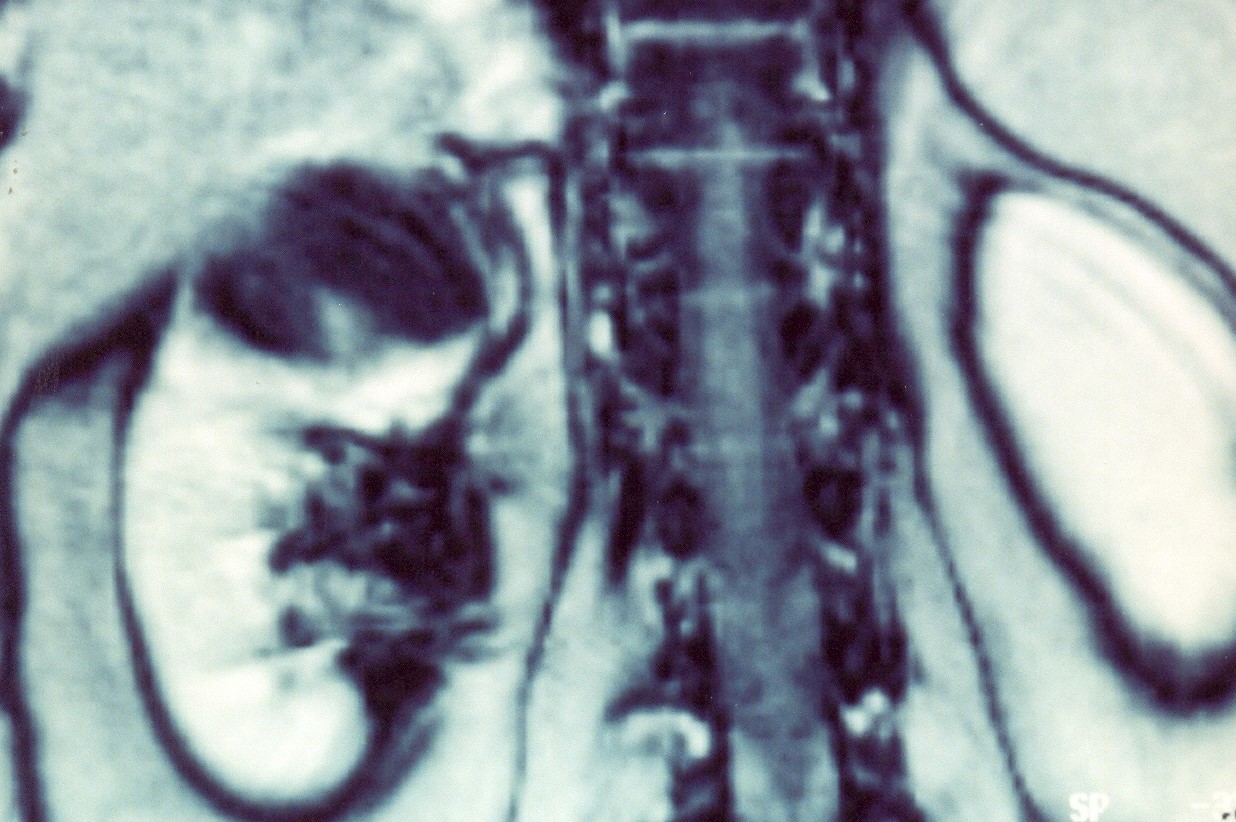
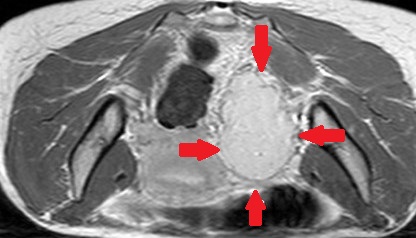
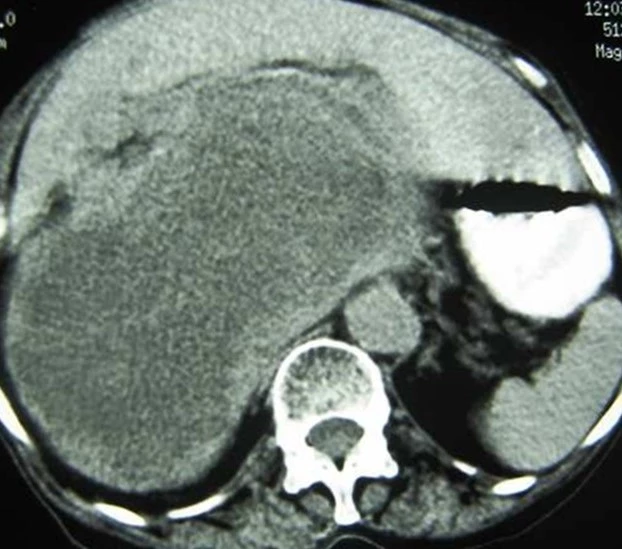
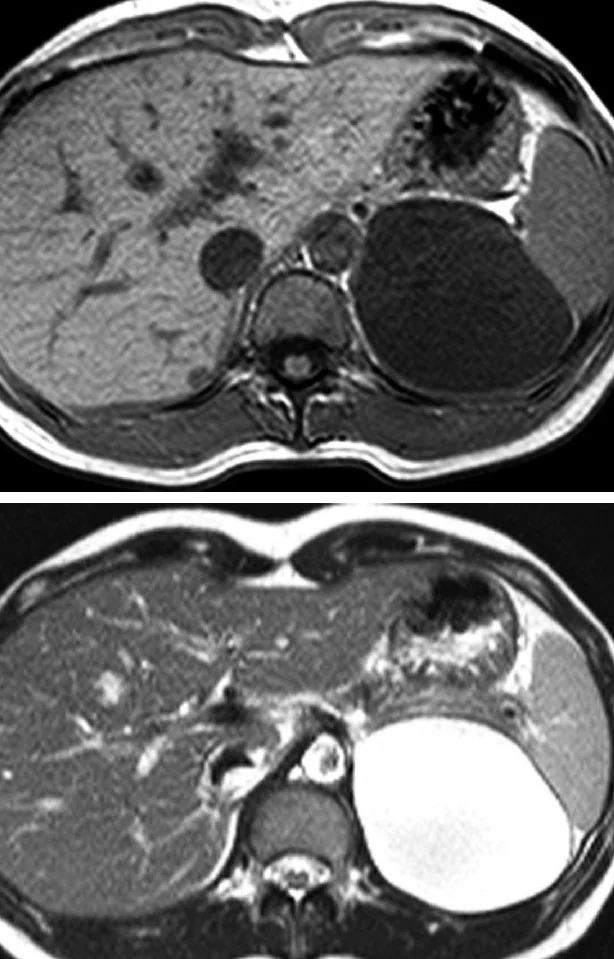
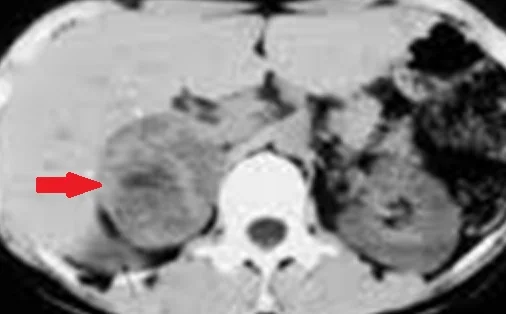
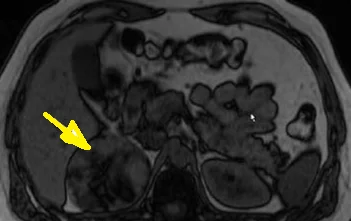
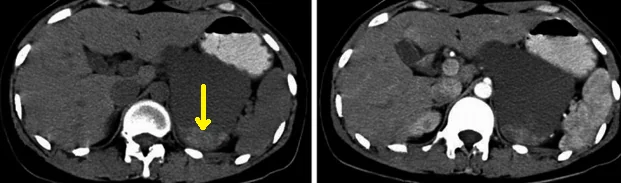
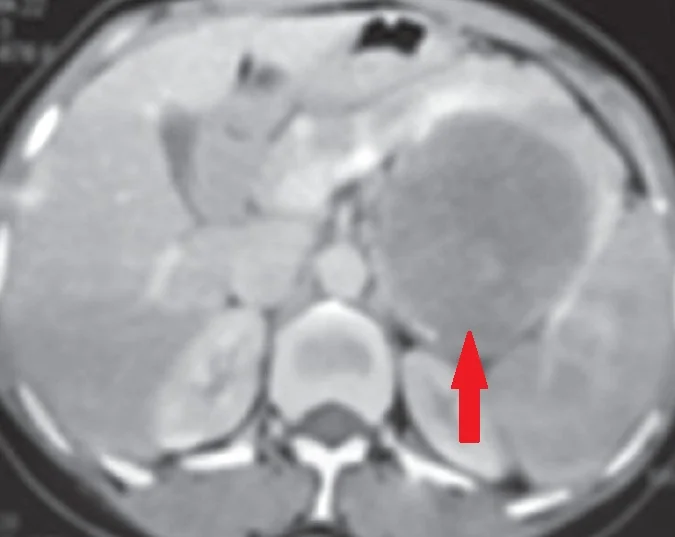
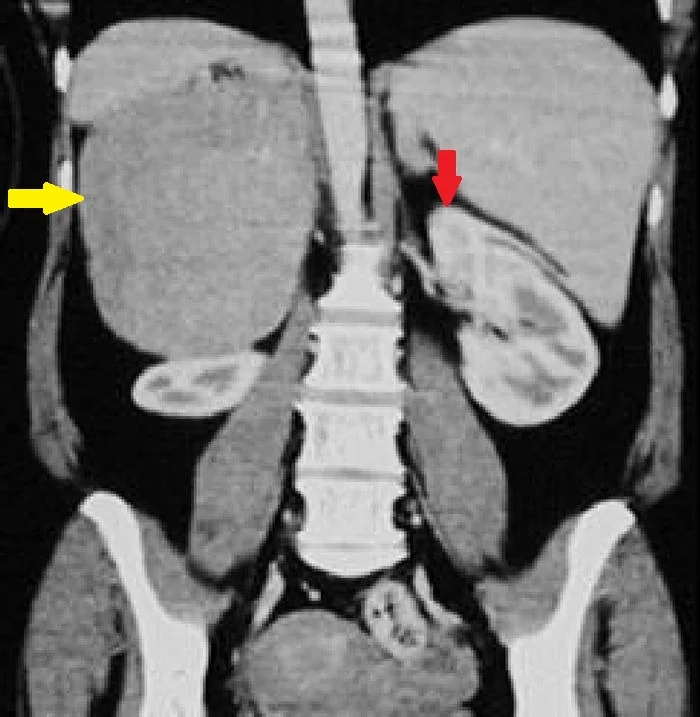
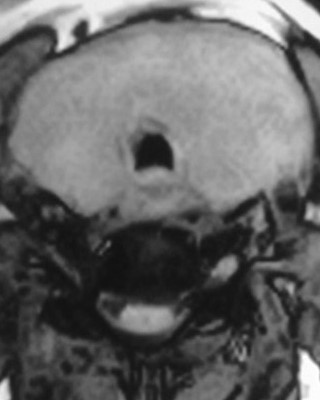
Abdominal MRI.Spontaneous left adrenal haemorrhage.(Courtesy Dr.V.Penopoulos).
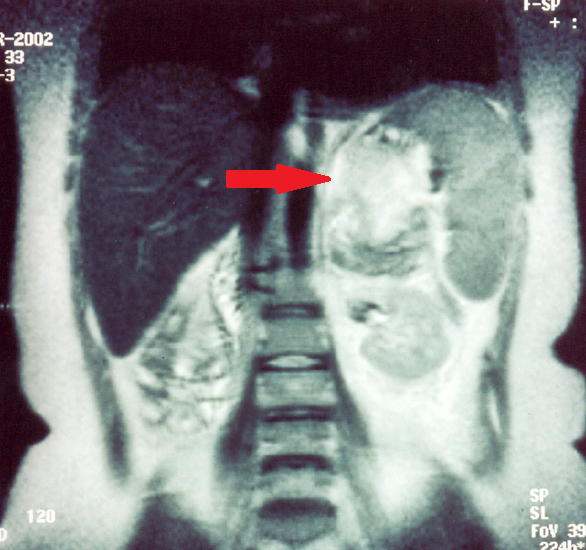
Abdominal MRI.Spontaneous left adrenal haemorrhage.(Courtesy Dr.V.Penopoulos).
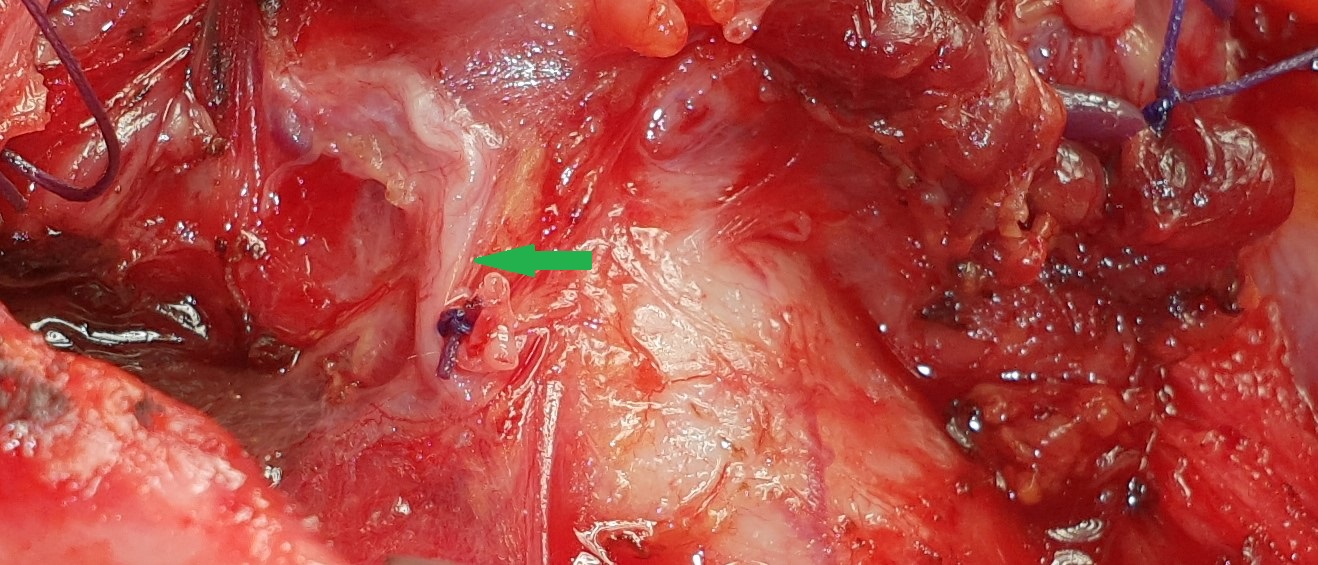
Green arrow-Ectopic parathyroid adenoma.Red arrow-Right common carotid artery.(Courtesy Dr. V. Penopoulos).
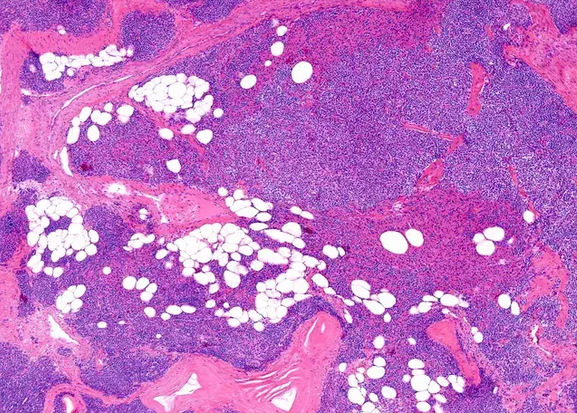
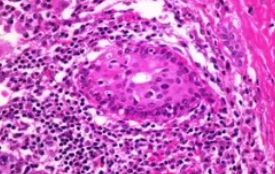
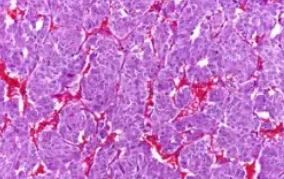
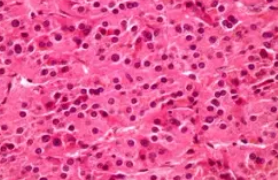
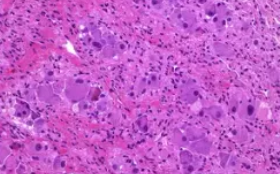
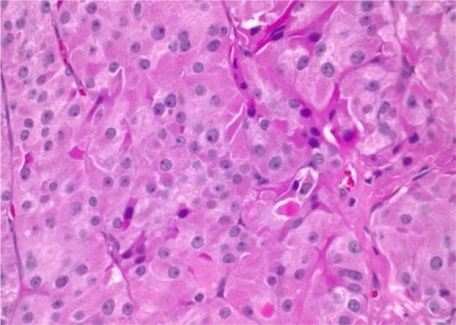
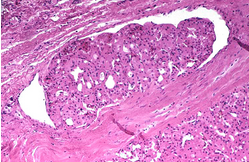
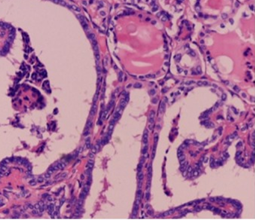
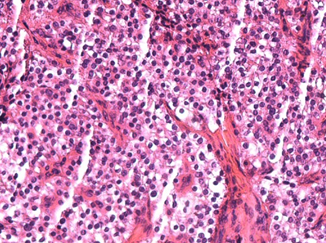
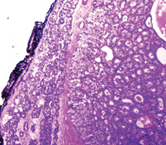
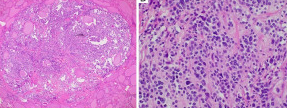
Parathyroid adenoma. The cells demonstrate moderate pleomorphism, with centrally located round nuclei and clear/eosinophilic cytoplasm, without cellular atypia or mitotic activity (Courtesy Dr. V. Penopoulos)
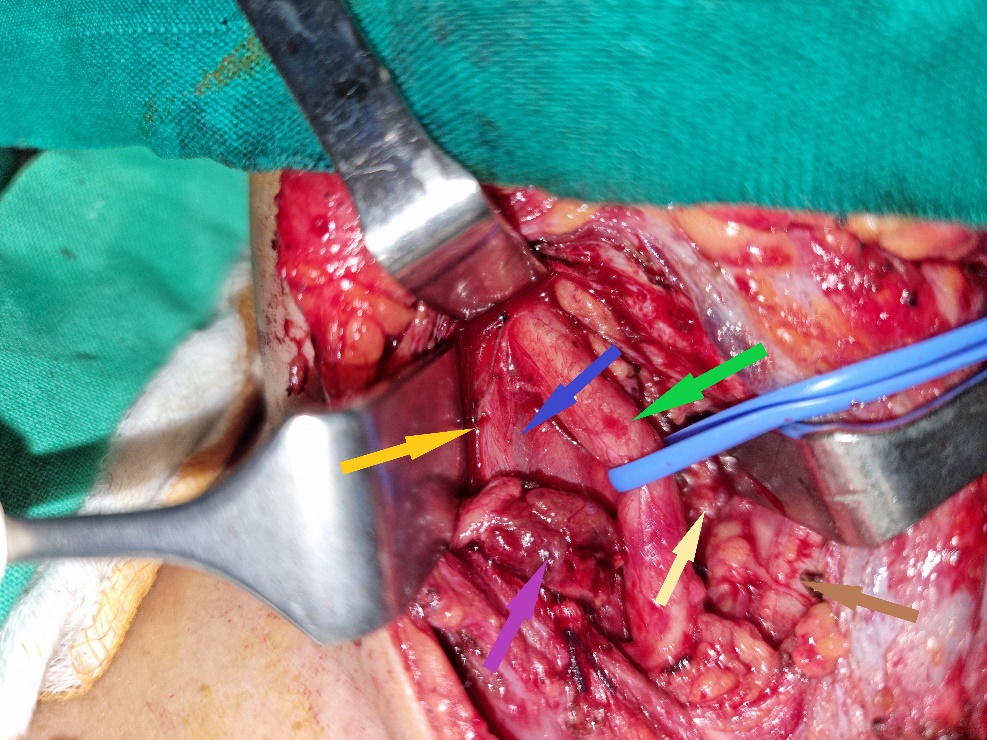
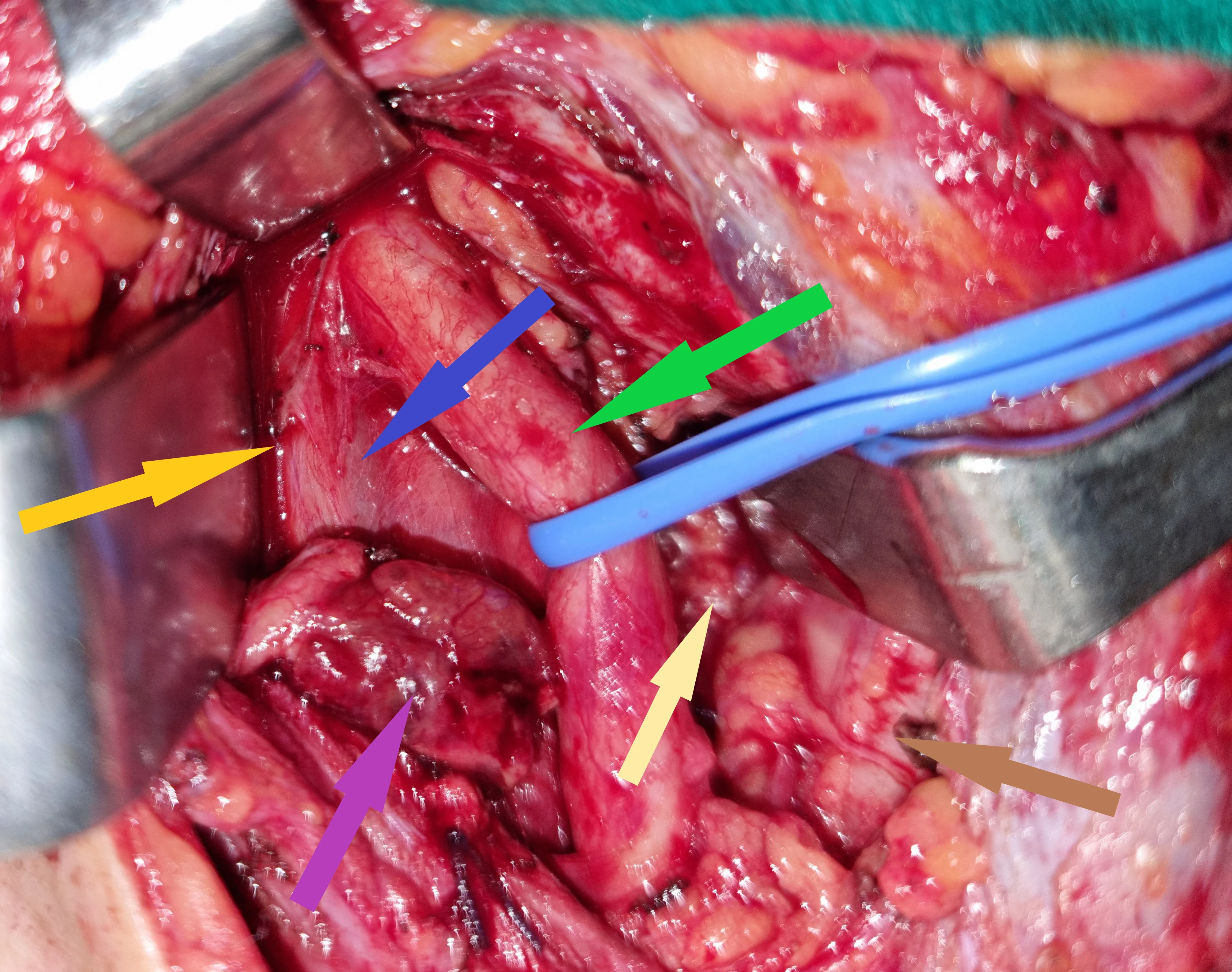
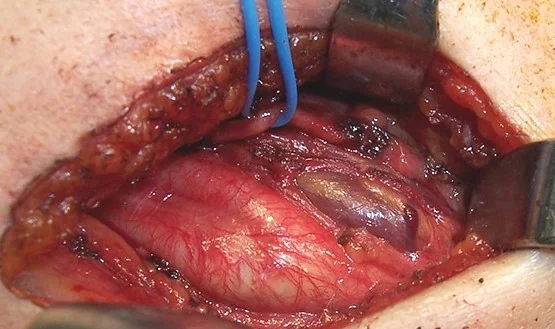
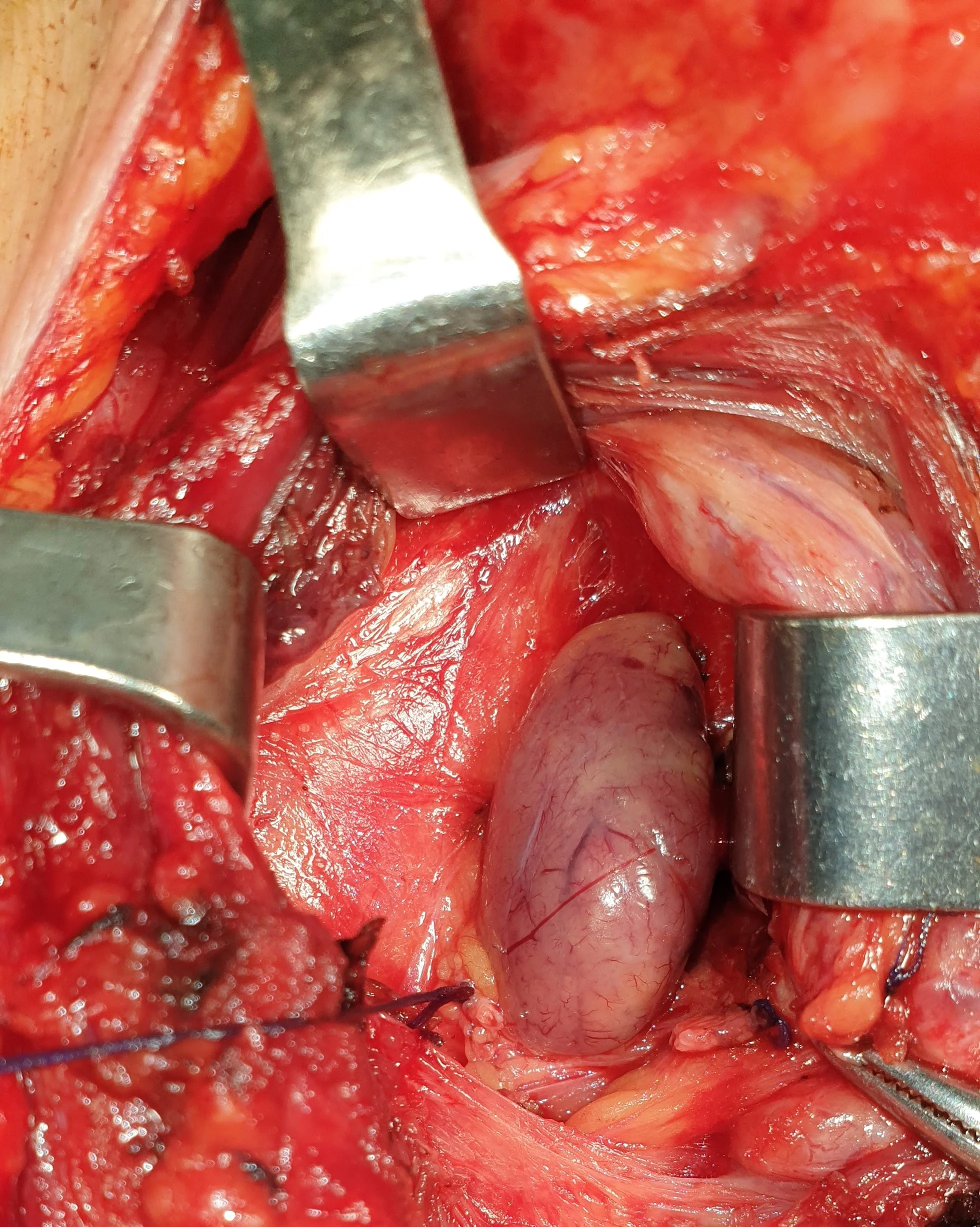
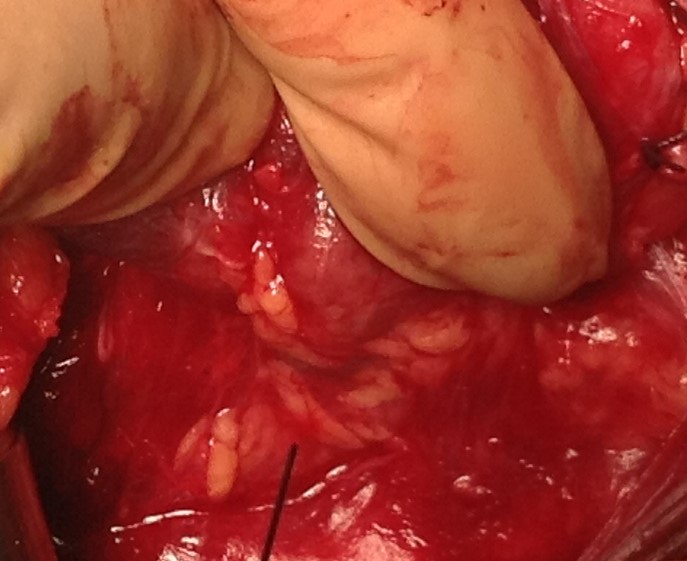
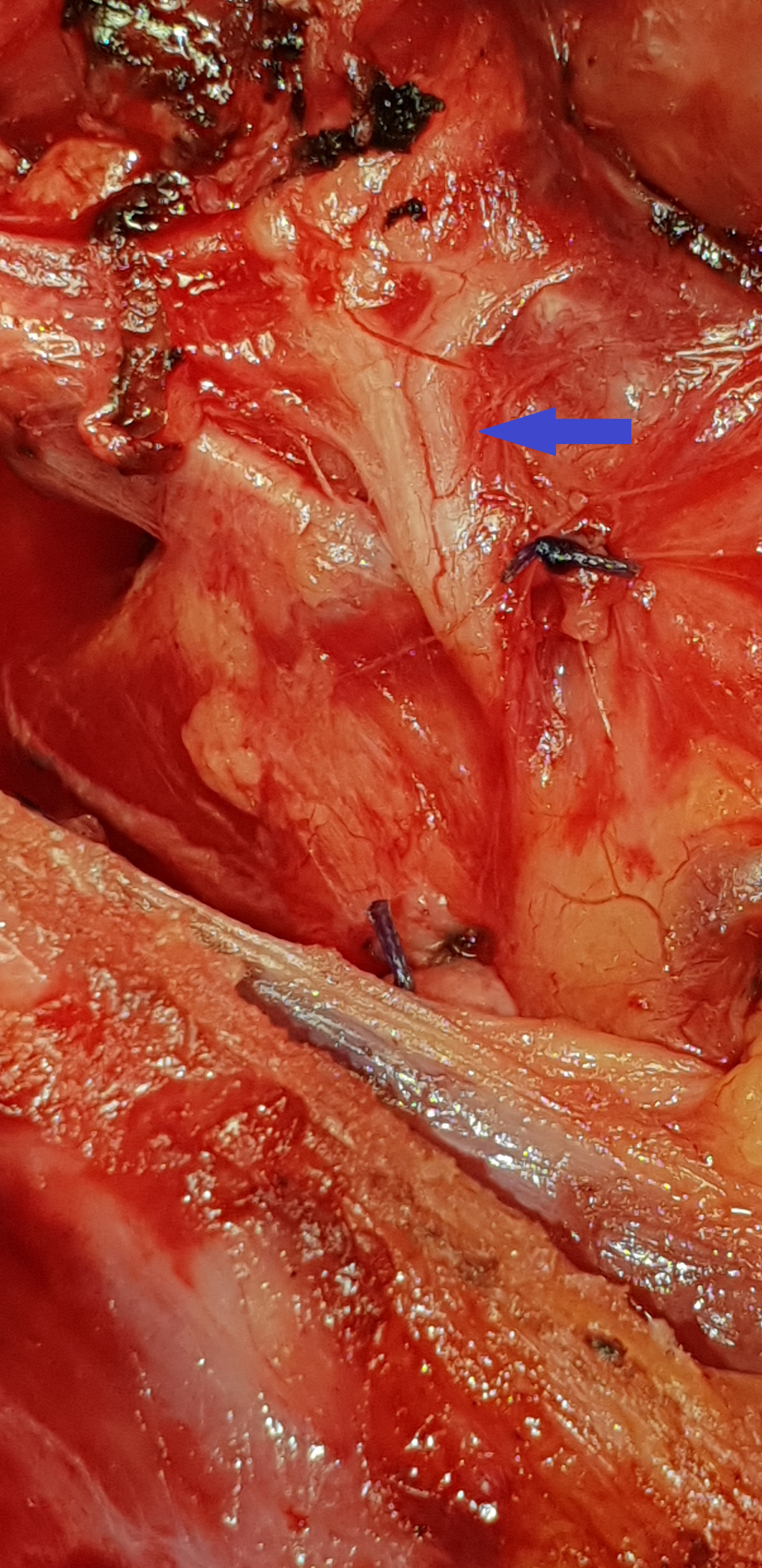
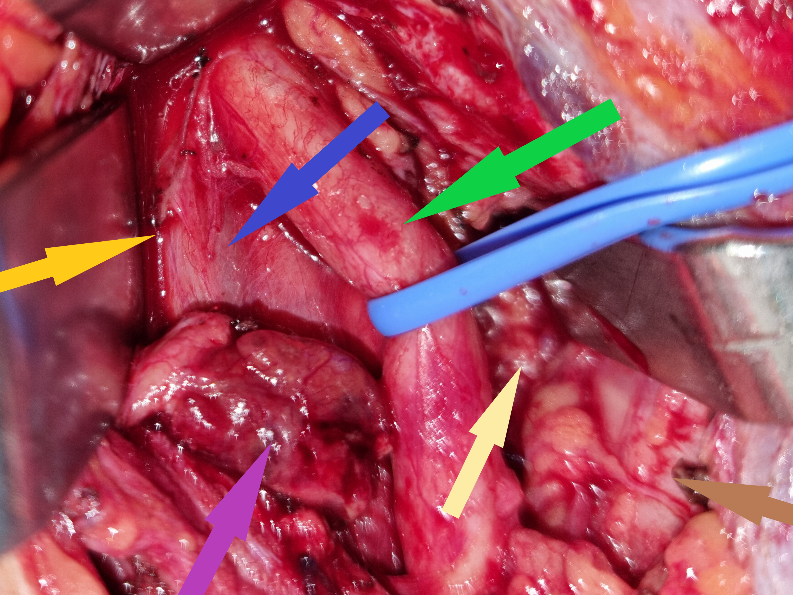
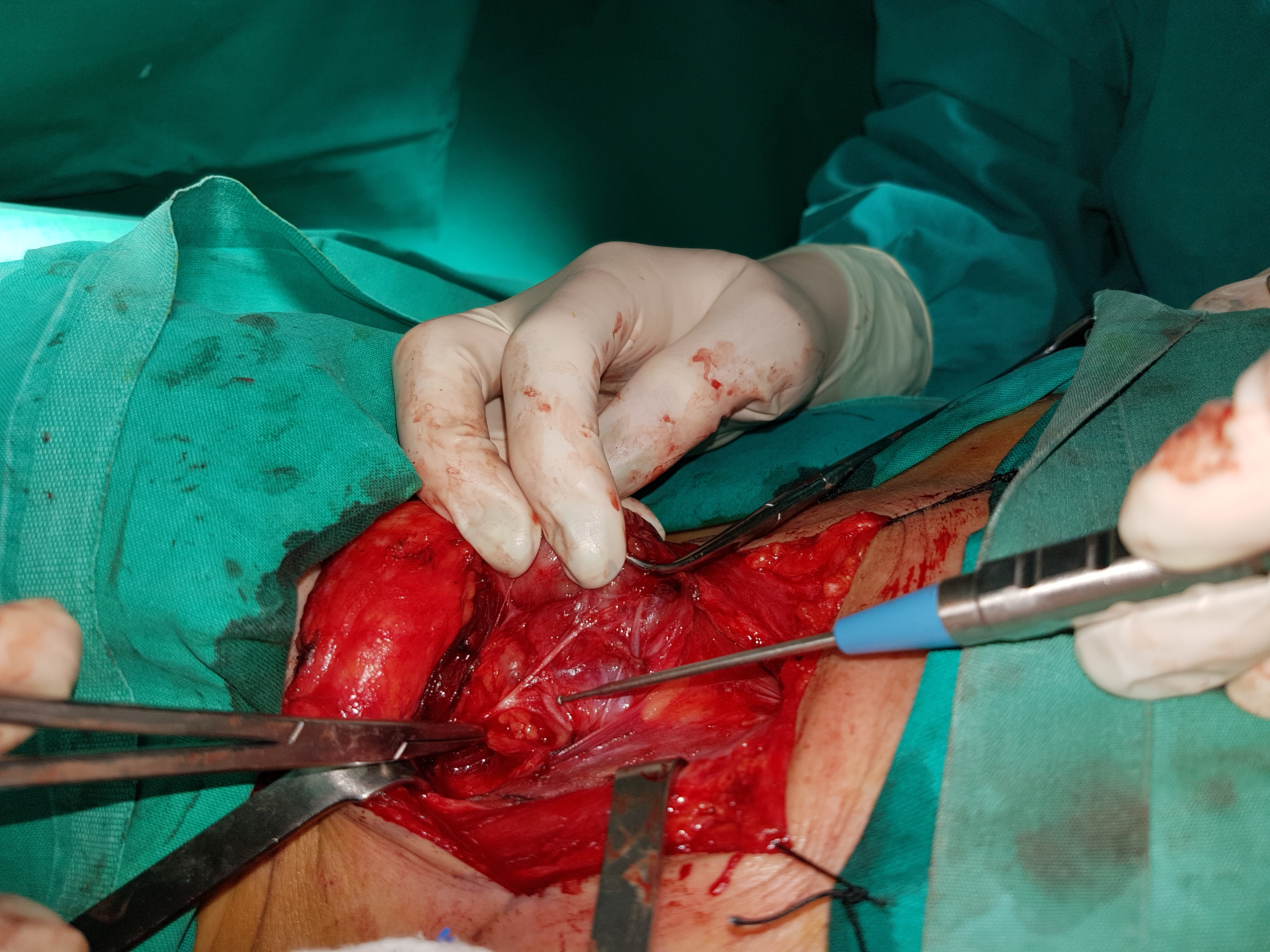
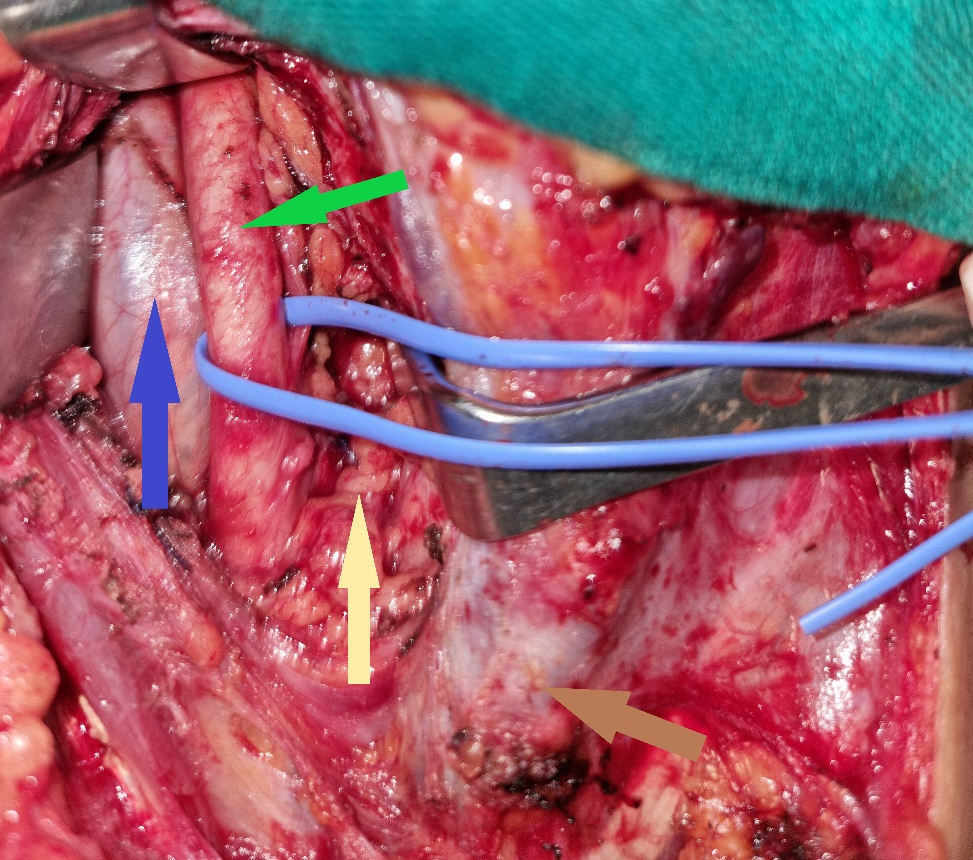
Green arrow — Right common carotid artery. Blue arrow — Right internal jugular vein. Purple arrow — Parathyroid adenoma. Yellow arrow — Right vagus nerve. Brown arrow — Trachea. Light brown arrow — Right recurrent laryngeal nerve (Courtesy Dr. V. Penopoulos)


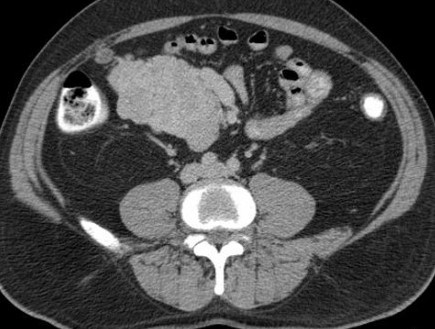
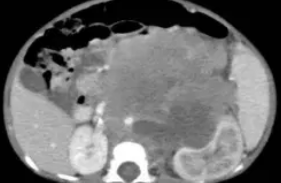
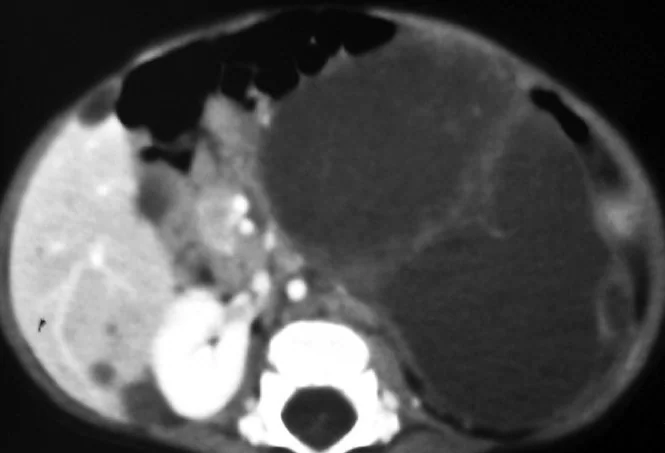
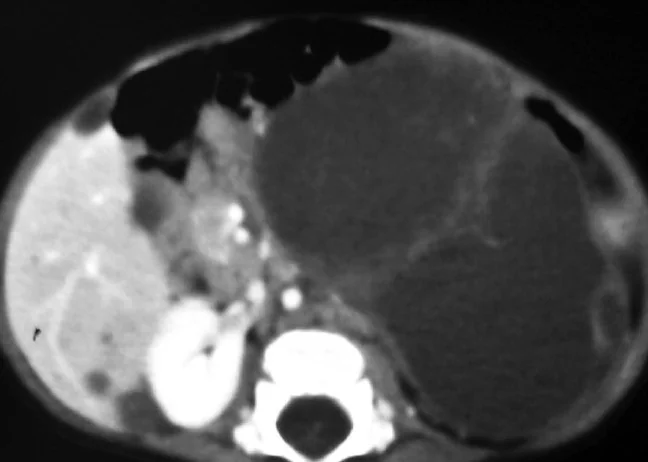
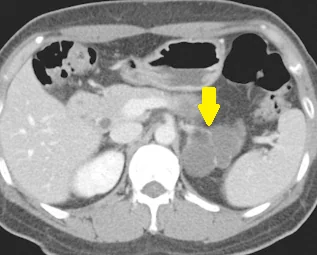
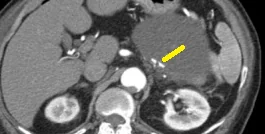
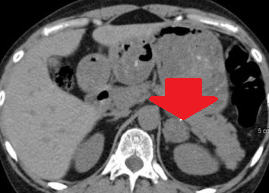
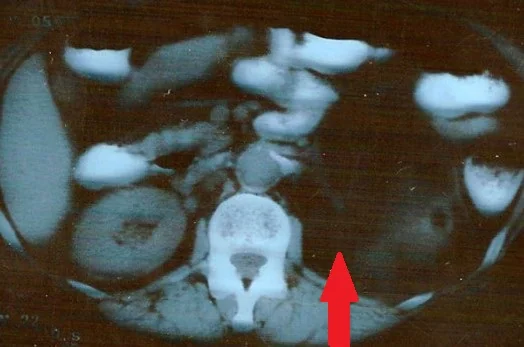
Abdominal CT Scan.The suspicious nodule at the root of the mesentery is clearly visible.(Courtesy Dr. V. Penopoulos).

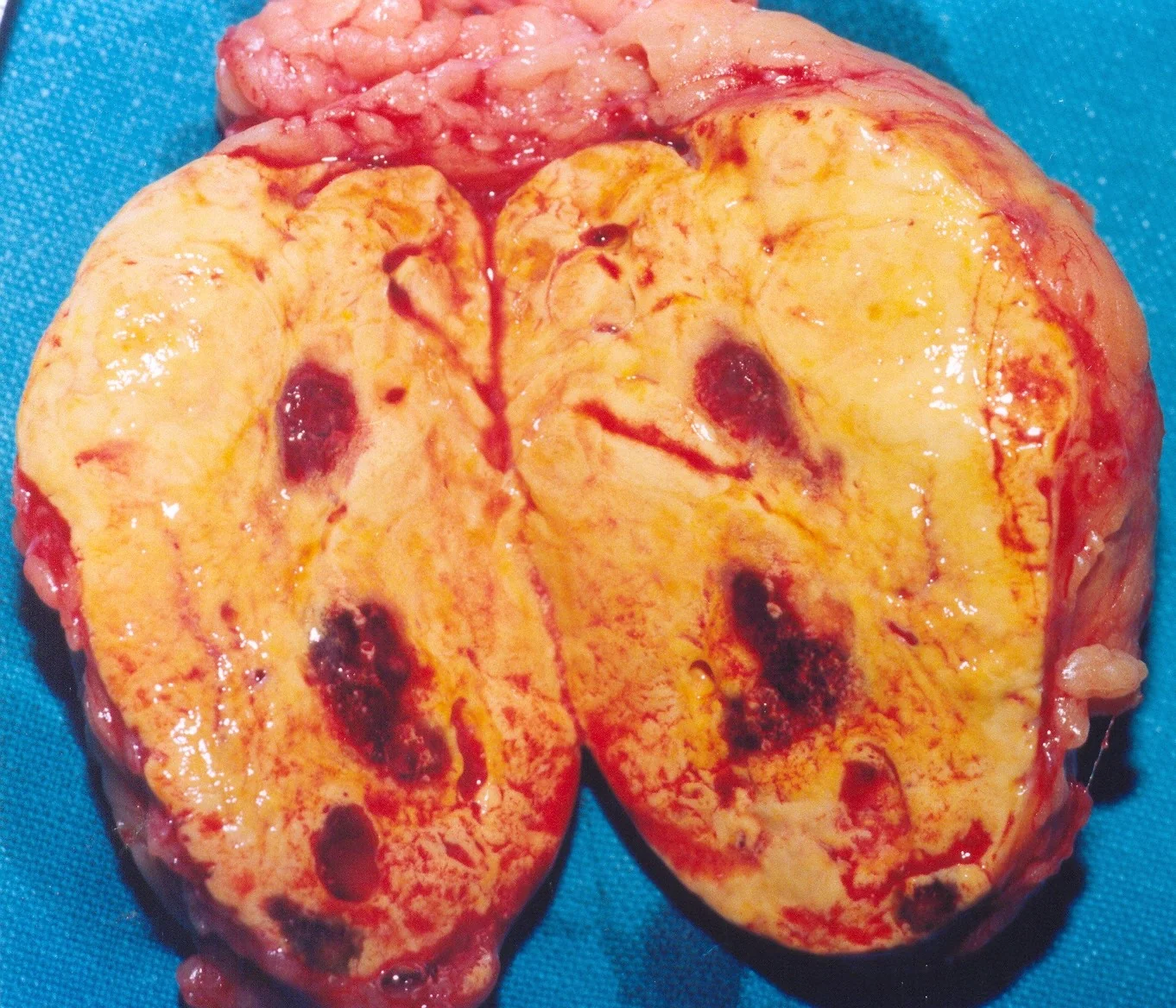
T scan.13 years after the initial identification of a non-functional incidentaloma of the right adrenal gland.Presence of a heterogeneous tumor – adrenocortical carcinoma of the right adrenal gland (Courtesy Dr. V. Penopoulos)
Cervical ultrasound. Medullary carcinoma. Visible microcalcifications (Courtesy Dr. V. Penopoulos)


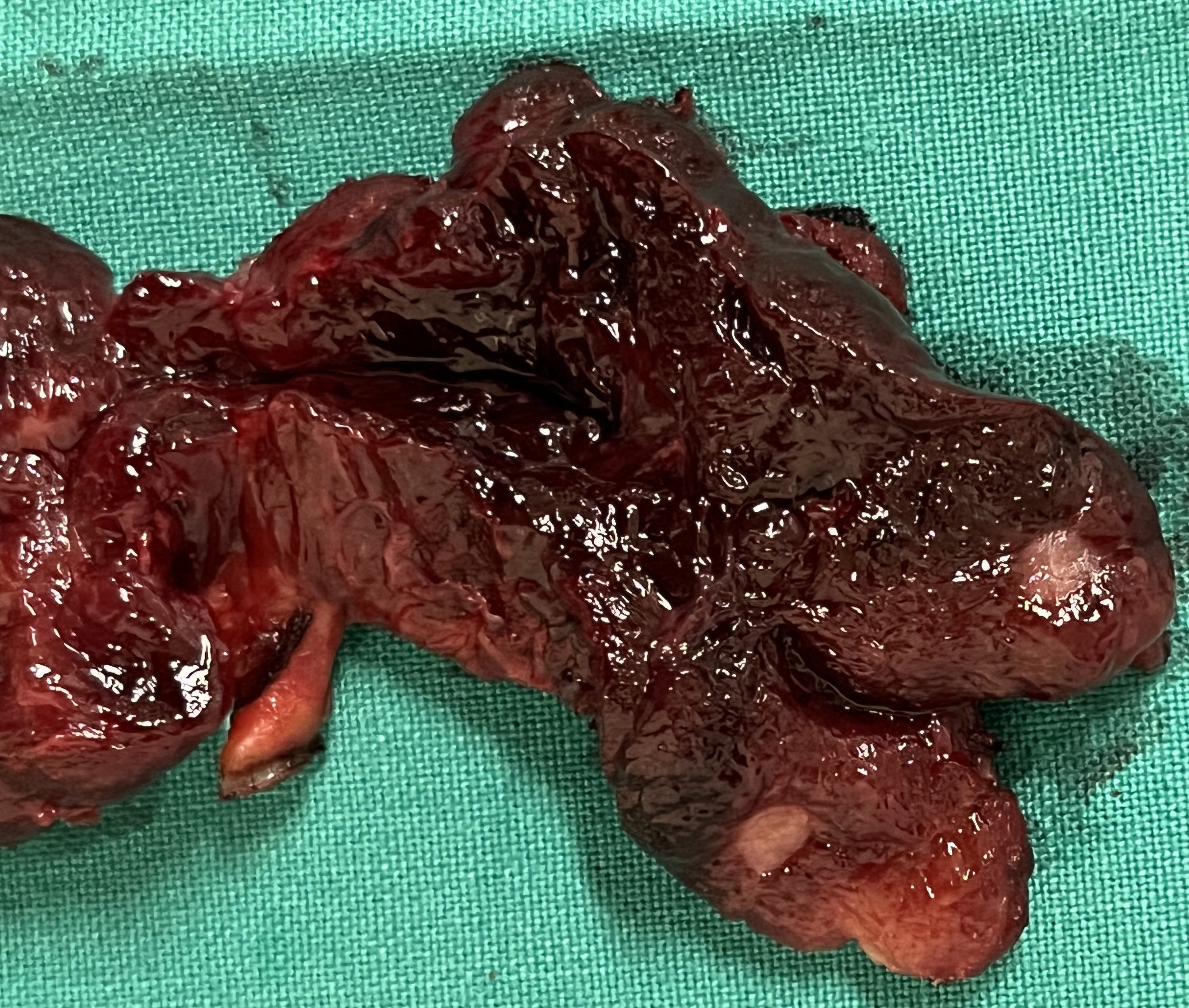
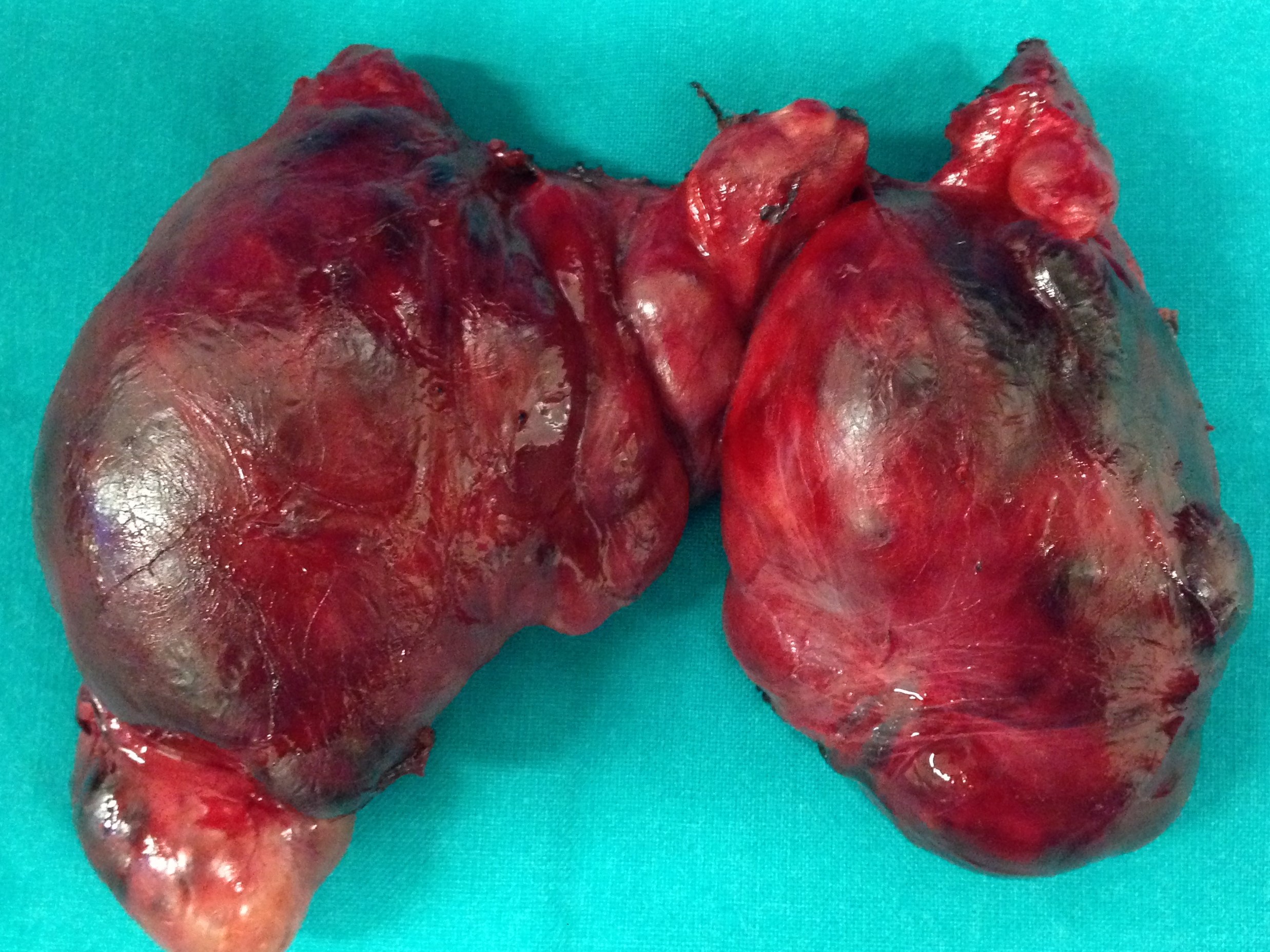
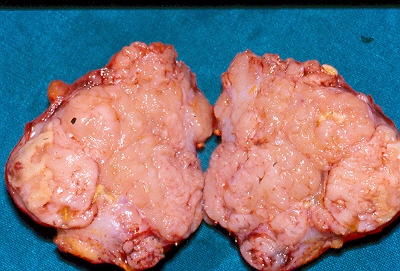
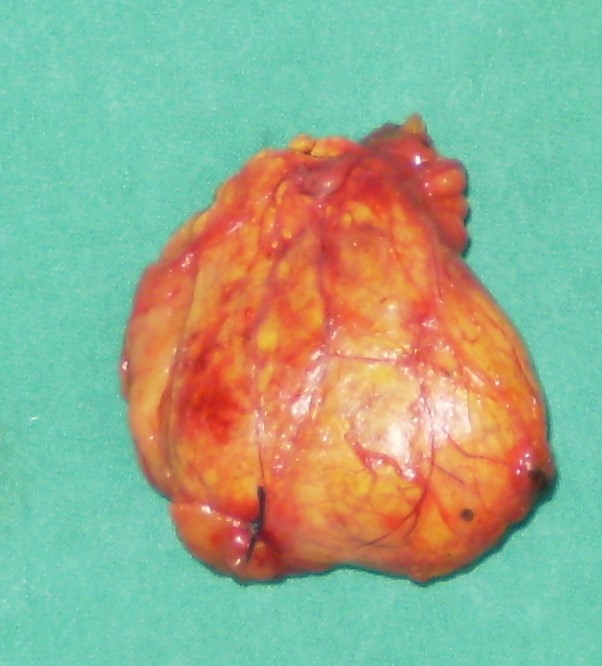
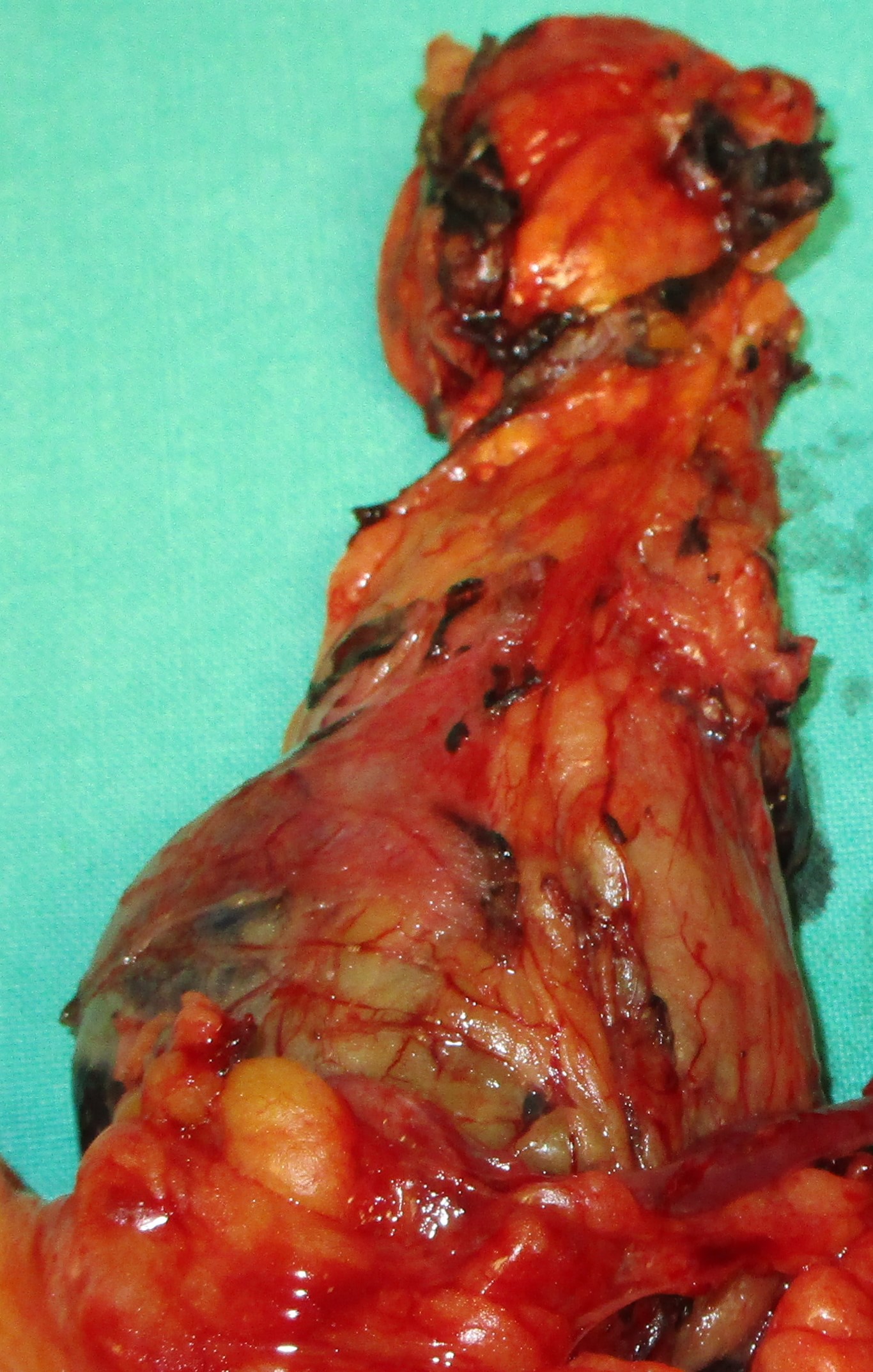
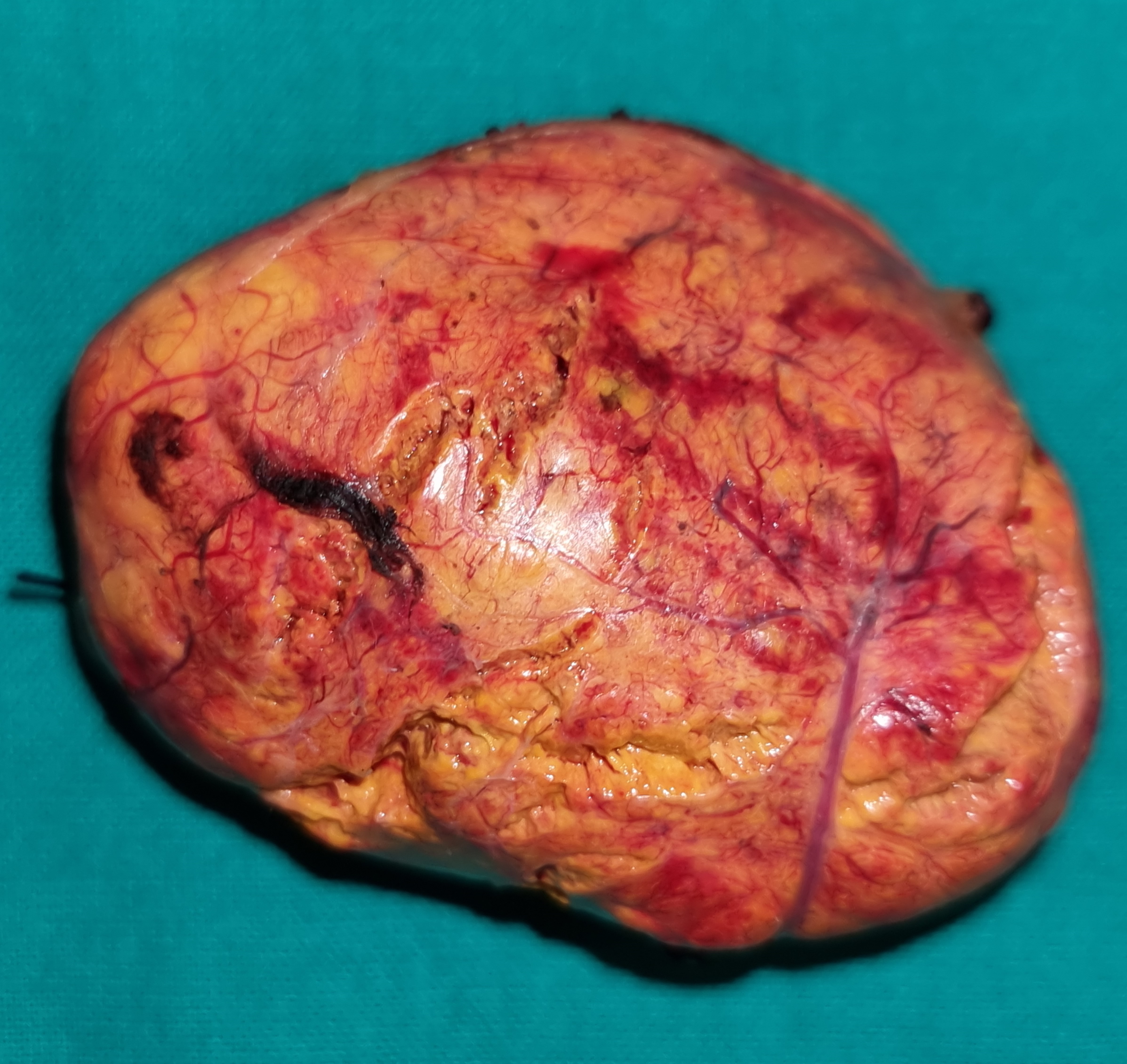
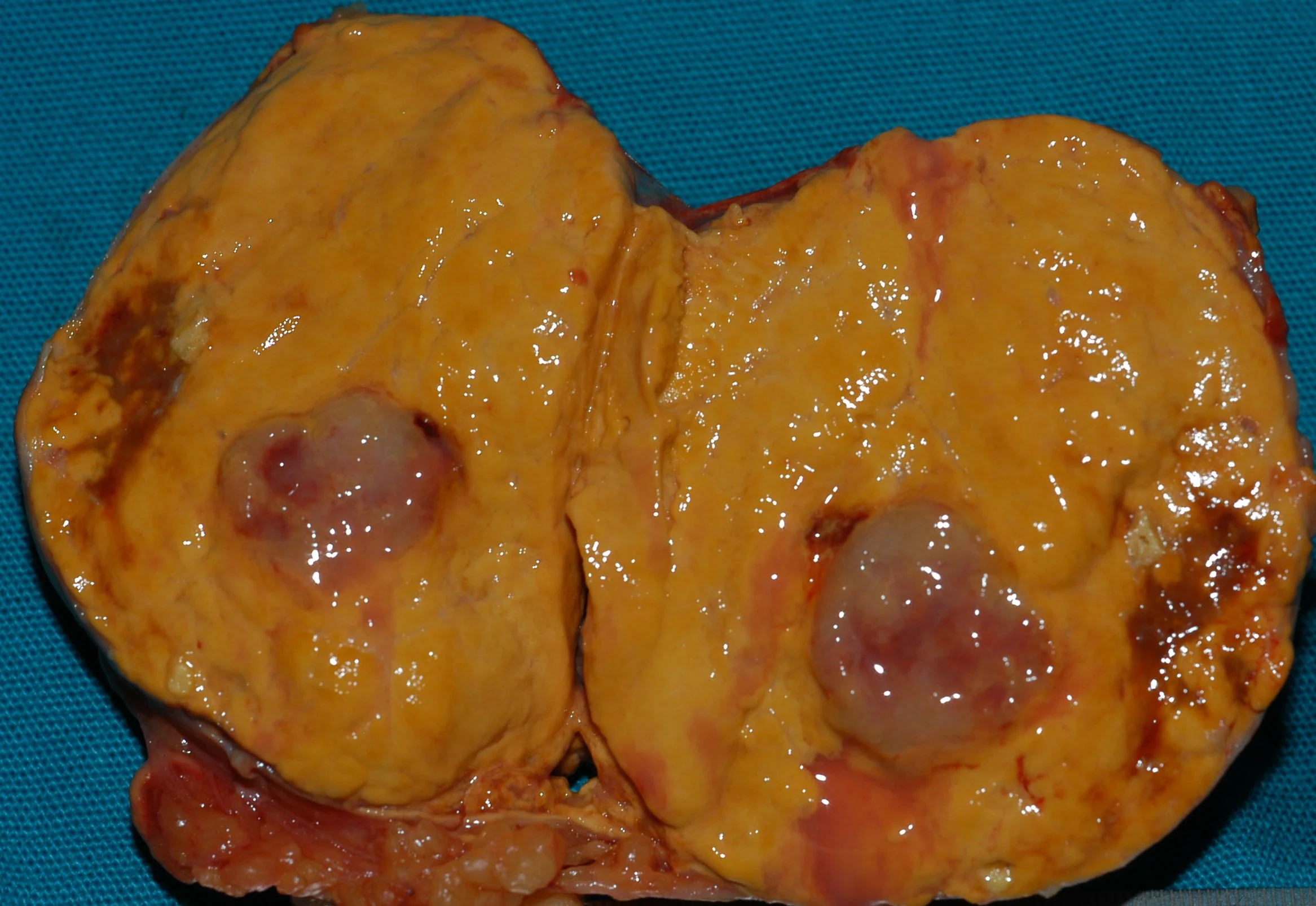
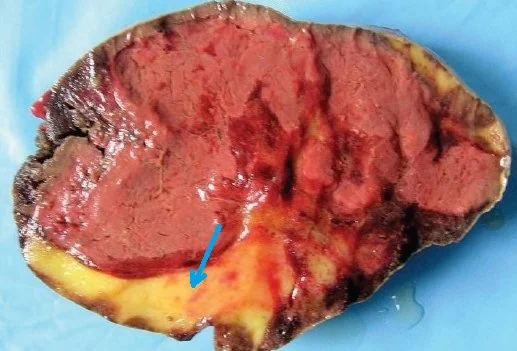
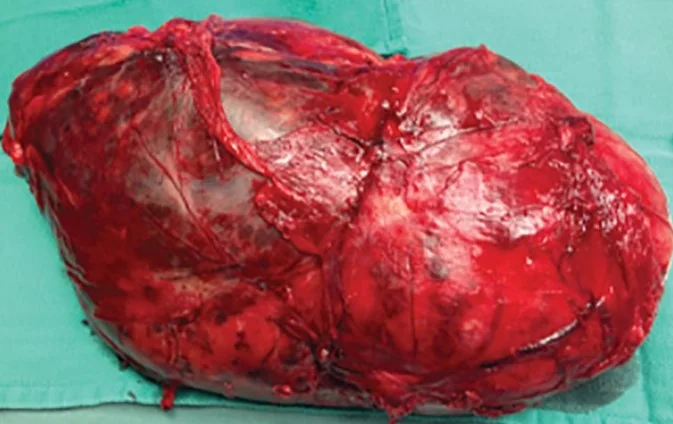
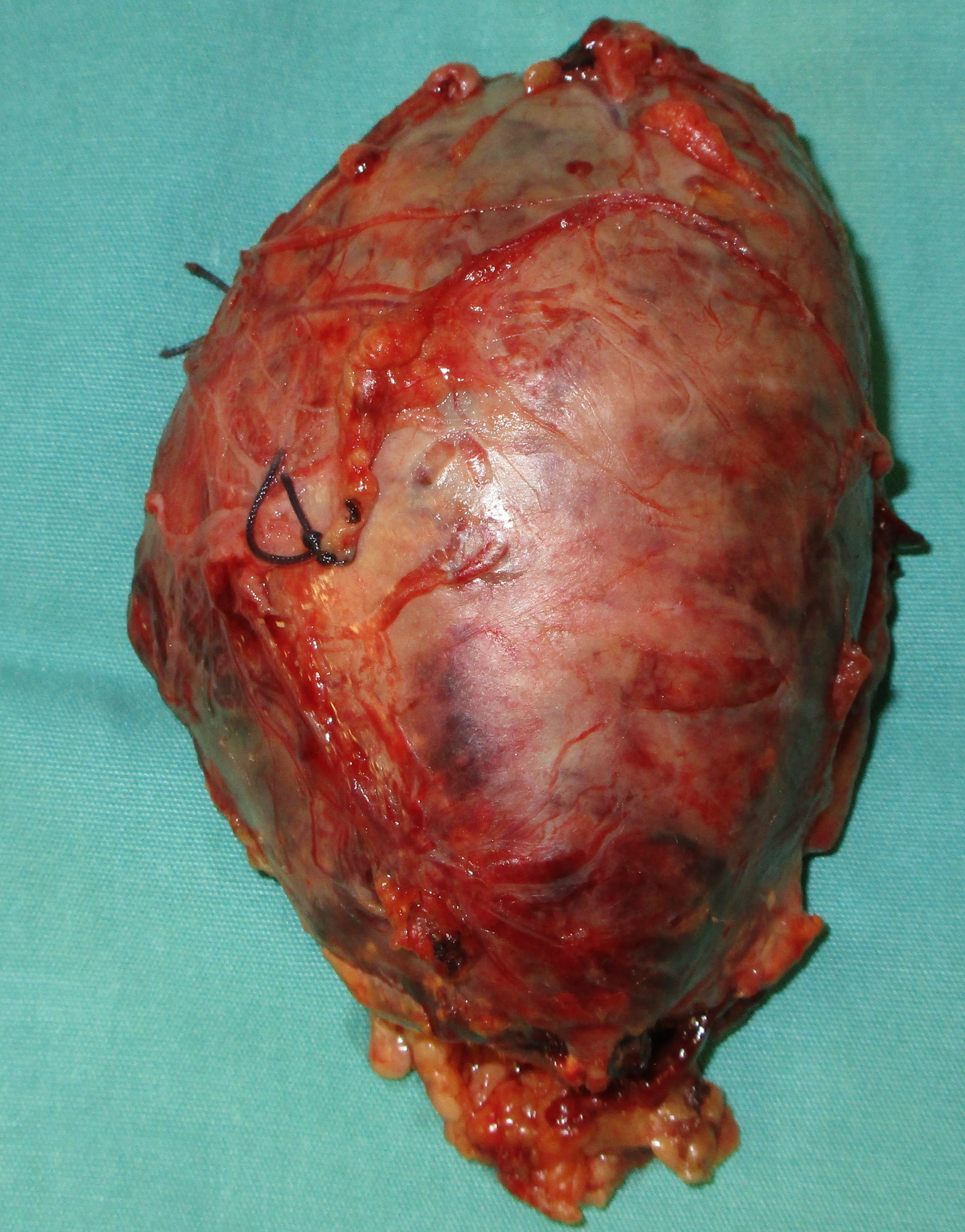
Primary adrenal leiomyosarcoma .Adrenalectomy specimen.(Courtesy Dr.V.Penopoulos).
Type III. Green arrows: Sectioned papillary carcinoma of the right thyroid lobe. Blue arrow: Medullary carcinoma of the right thyroid lobe. The two cancers are clearly separated by normal thyroid parenchyma (Courtesy Dr. V. Penopoulos)

Cervical ultrasound. Green arrow: Papillary carcinoma. Red arrow: Medullary carcinoma (Courtesy Dr. V. Penopoulos)
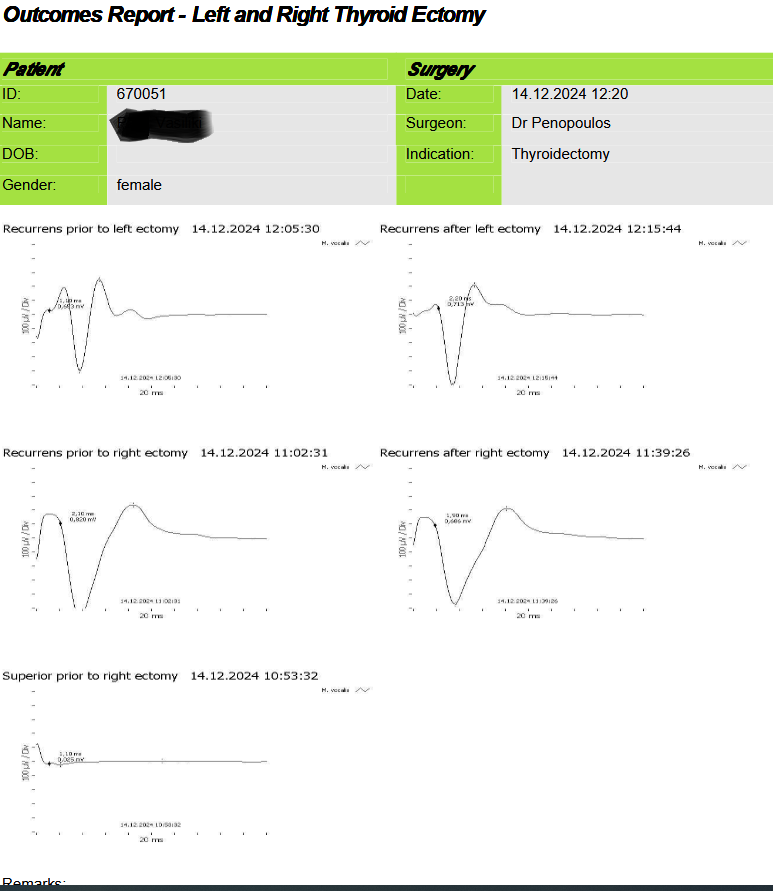
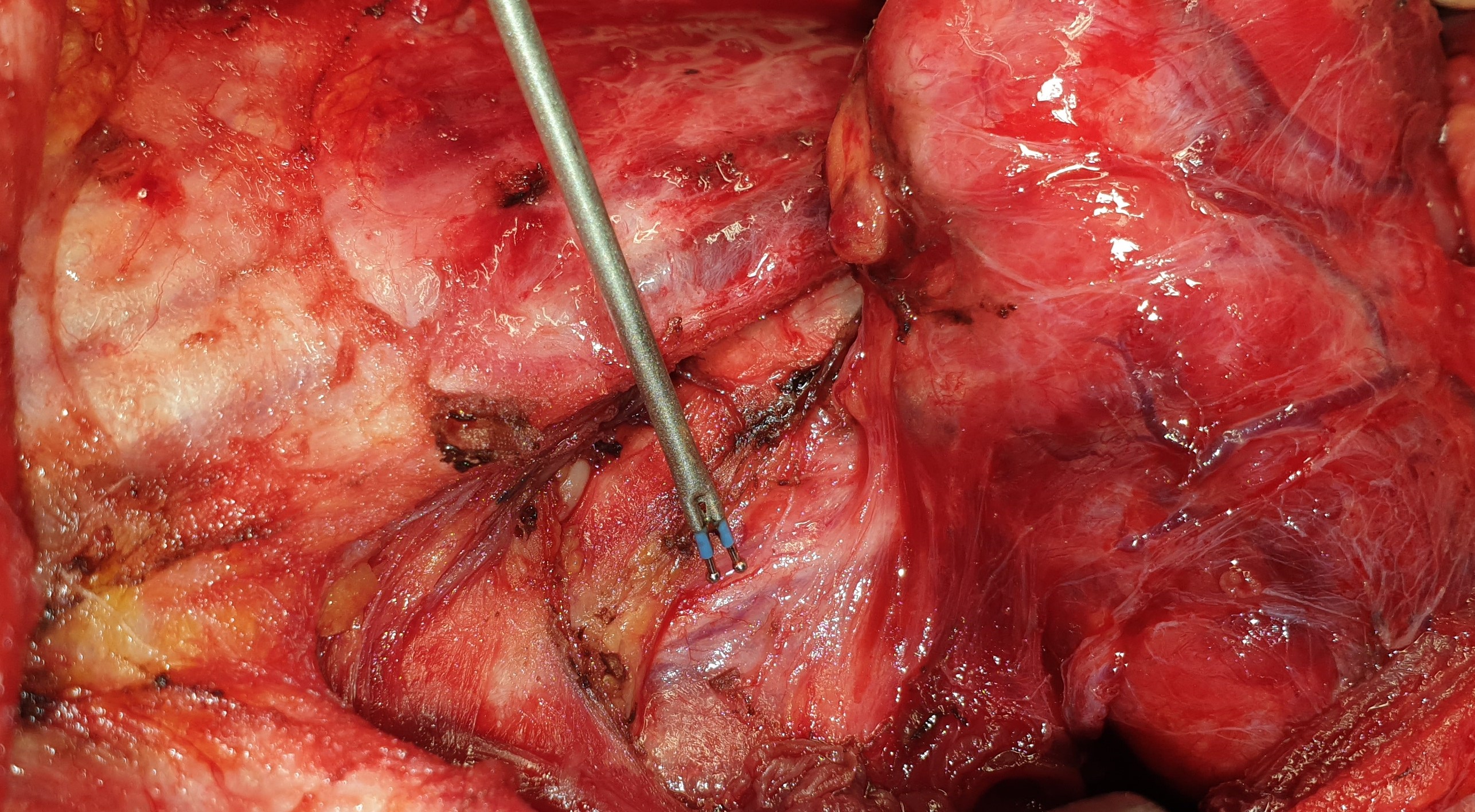
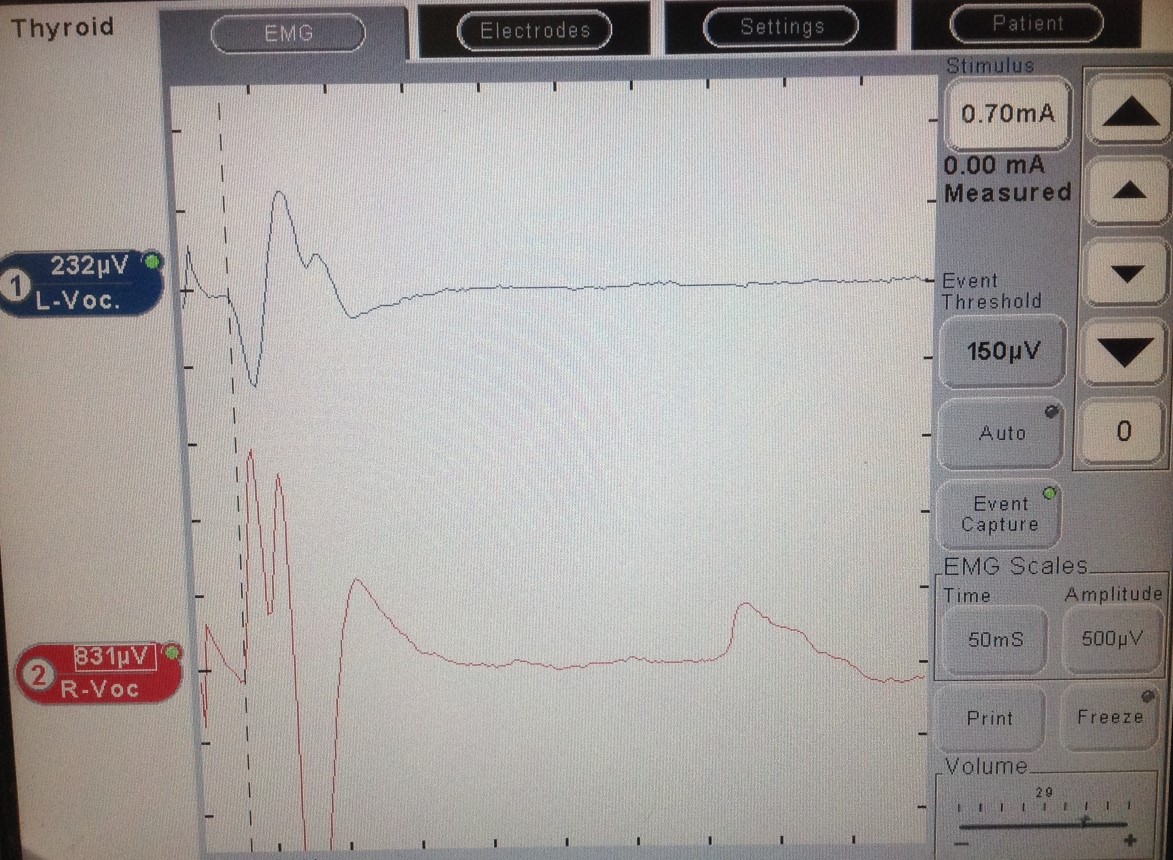
Inferior laryngeal nerve monitoring before and after total thyroidectomy (Courtesy Dr. V. Penopoulos)

The whole-body scintigraphy (Octreoscan) also revealed another focus in the thyroid gland, which was due to a known benign nodule of the organ (Courtesy Dr. V. Penopoulos)
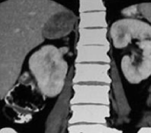
CT scan, 13 years after the initial identification of a non-functional incidentaloma of the right adrenal gland. Presence of a heterogeneous tumor – adrenocortical carcinoma of the right adrenal gland (Courtesy Dr. V. Penopoulos)
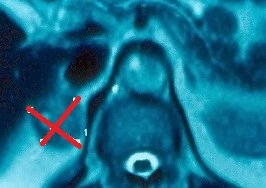
Whole-body scintigraphy (Octreoscan). A pathological focus is clearly visible at the root of the mesentery.(Courtesy Dr.V.Penopoulos).
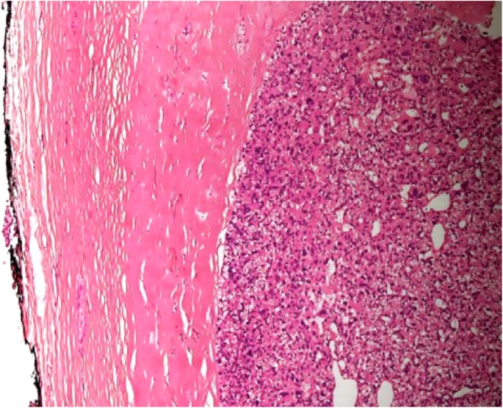
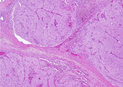
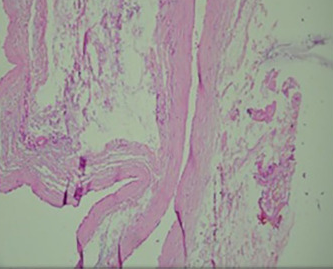
Thick capsule. A characteristic feature of both atypical parathyroid adenoma and parathyroid carcinoma (Courtesy Dr. V. Penopoulos)
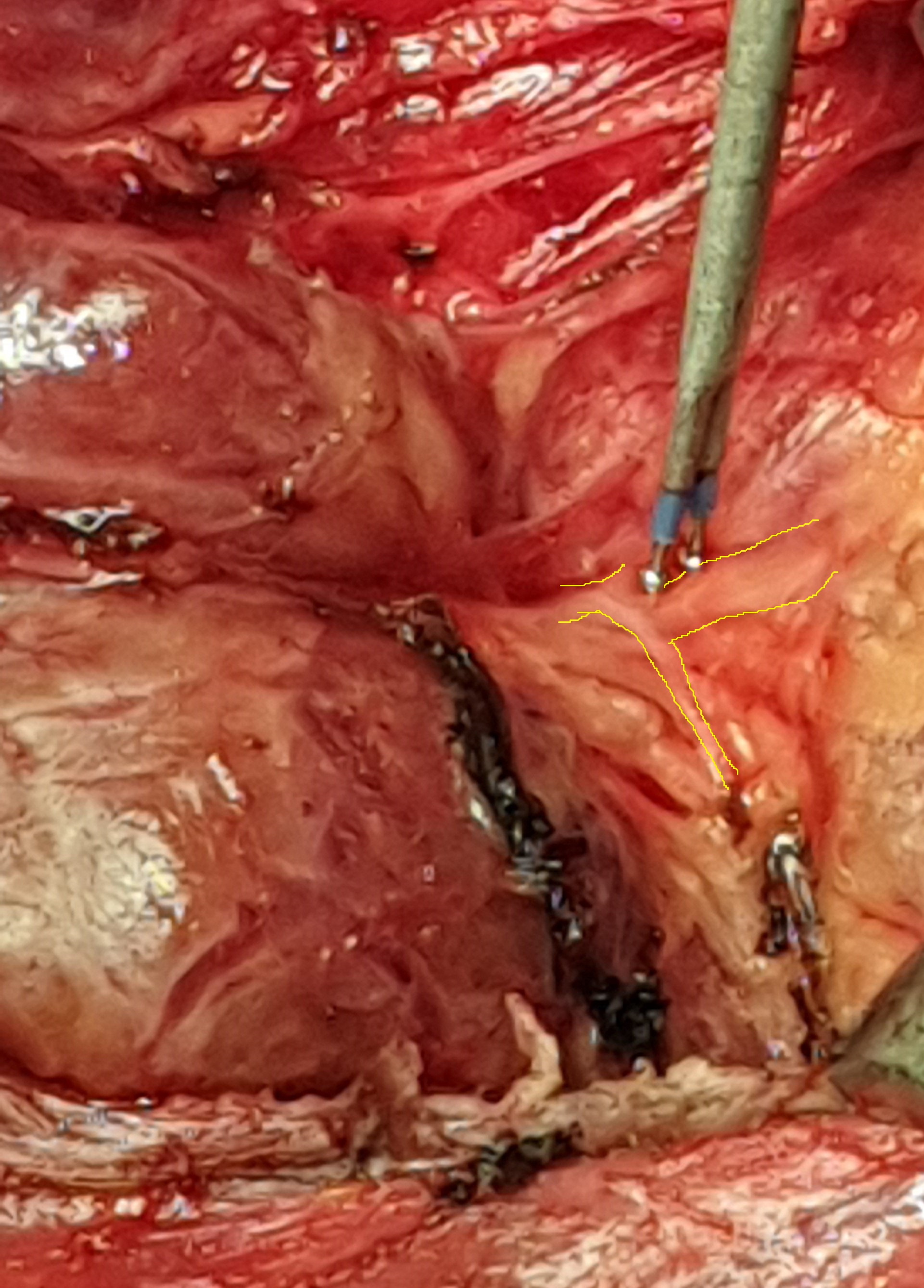
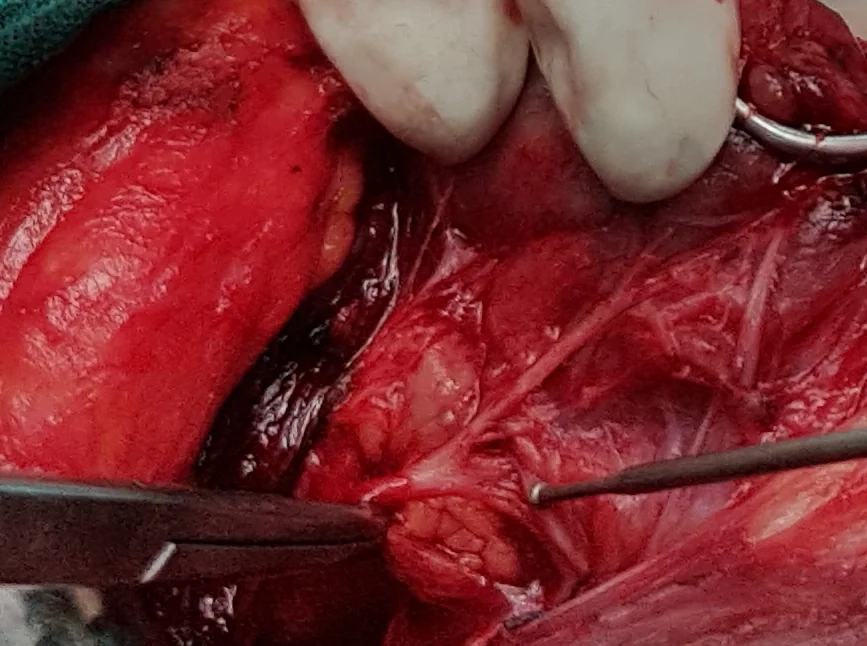
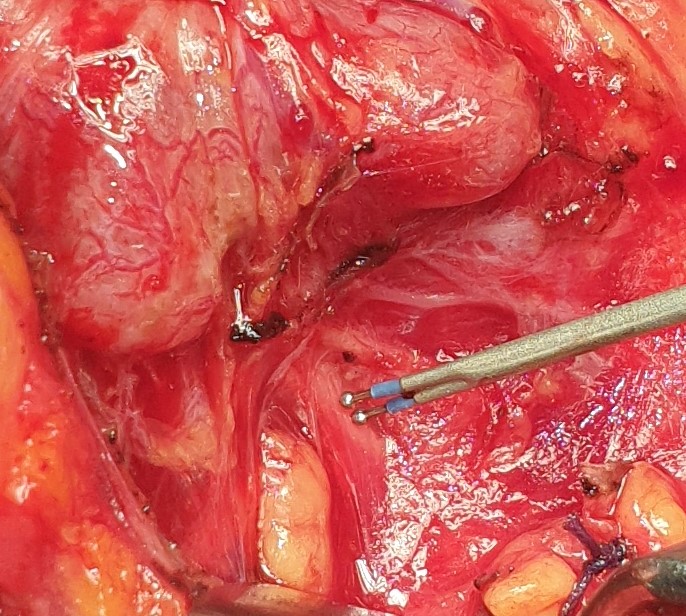
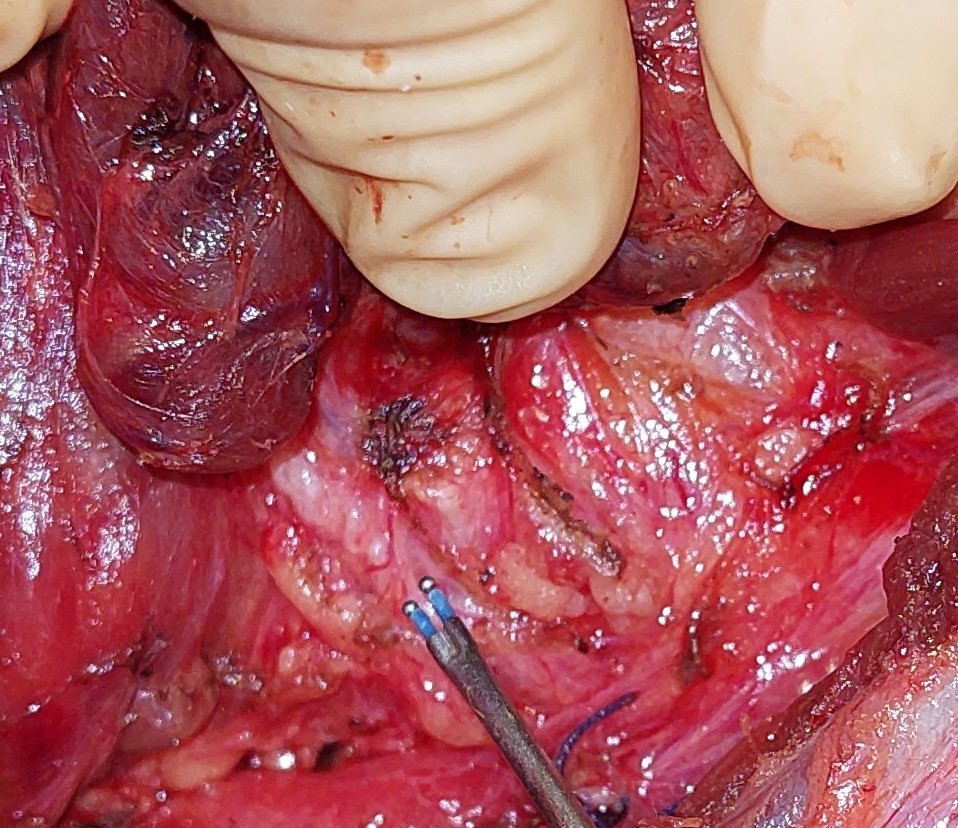
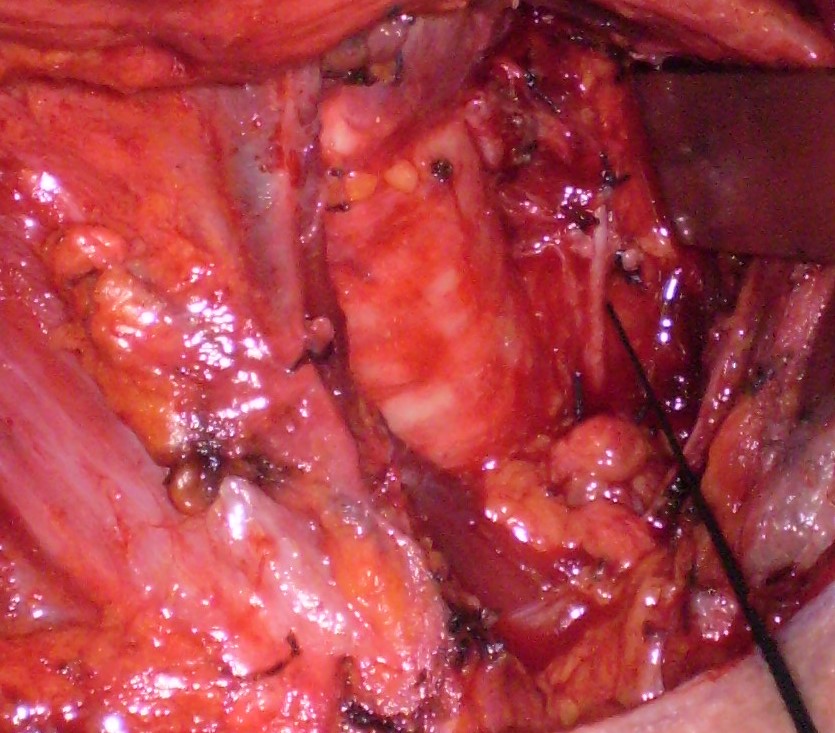
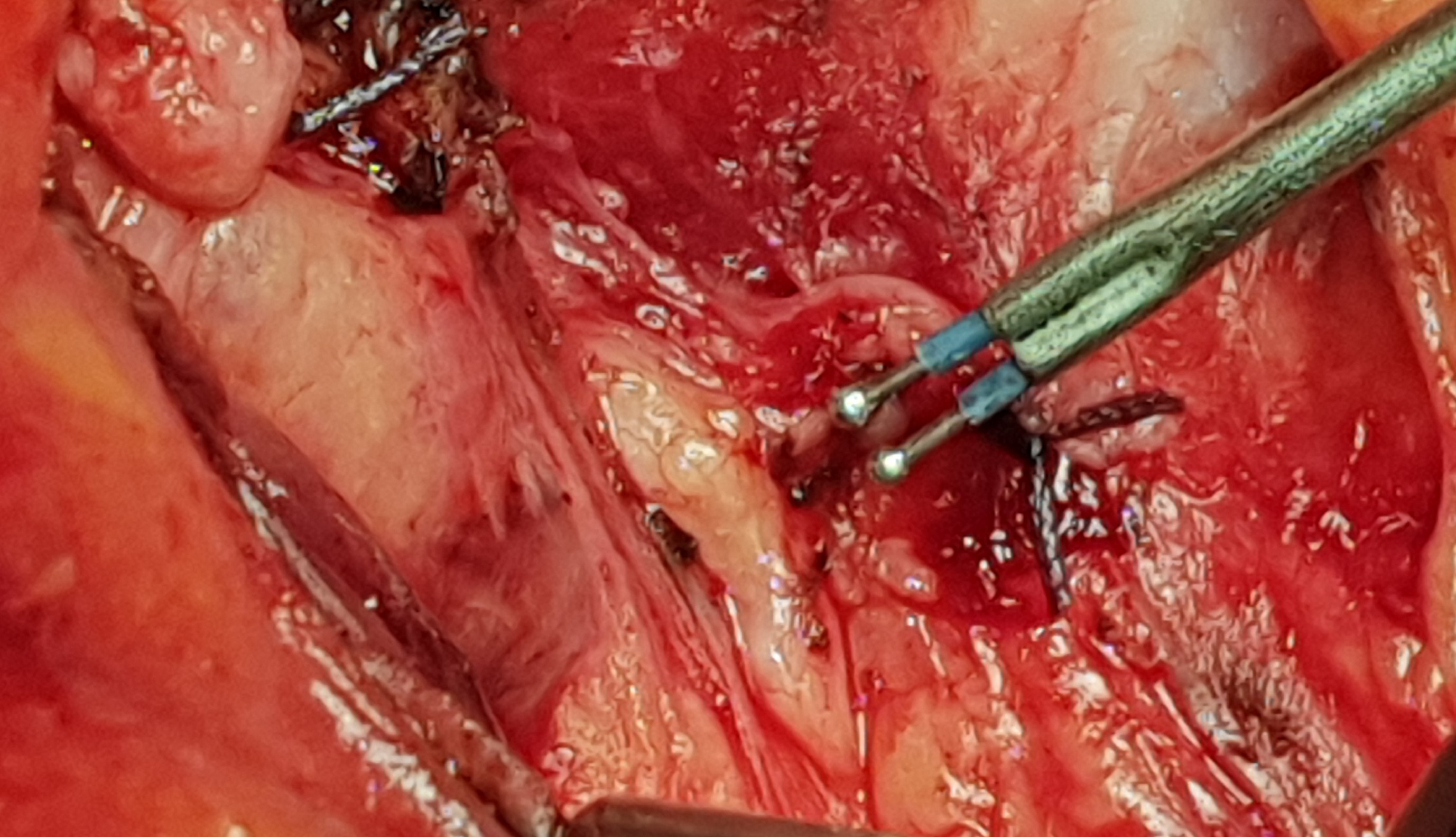
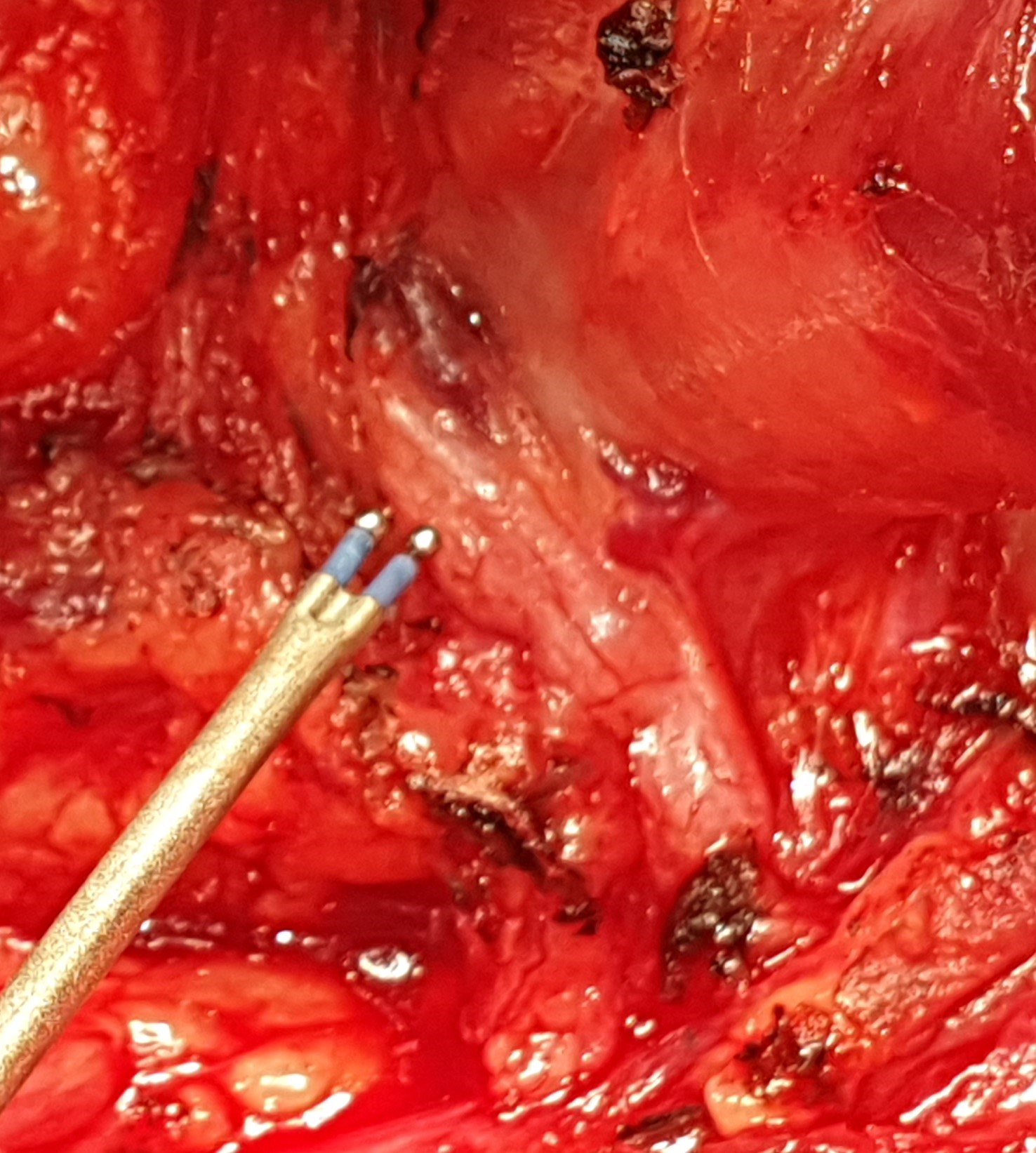
Identification and protection of the recurrent laryngeal nerve. Outline of the nerve — application of the nerve stimulator (Courtesy Dr. V. Penopoulos)
Sestamibi Scan . Sizeable right inferior parathyroid adenoma.(Courtesy Dr.V.Penopoulos).


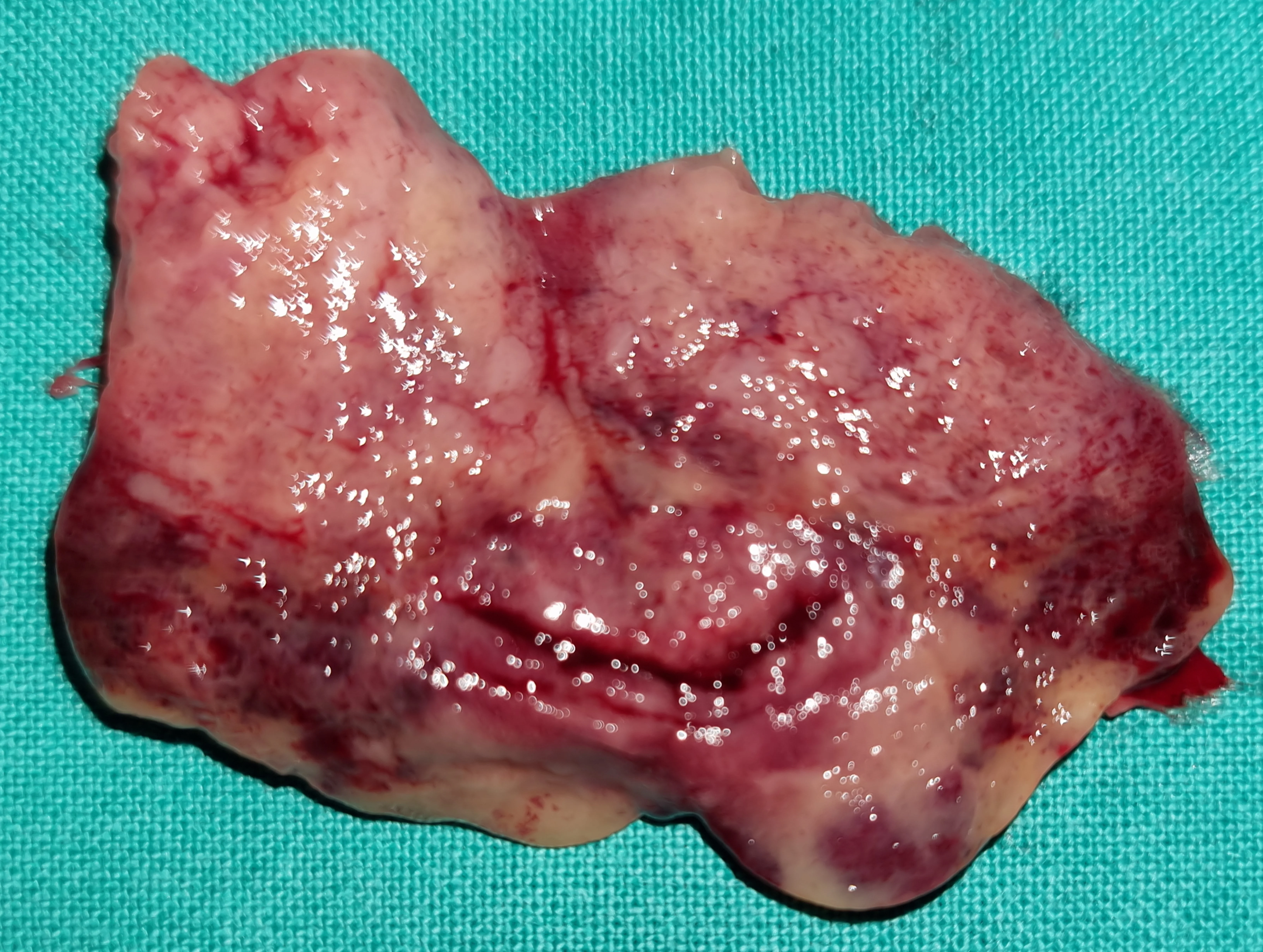
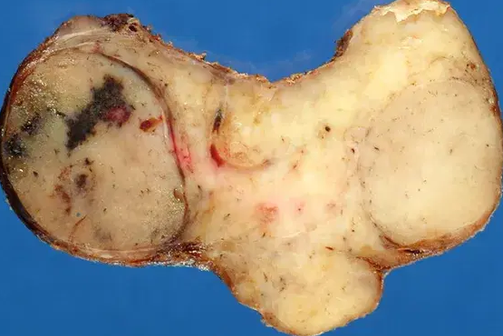
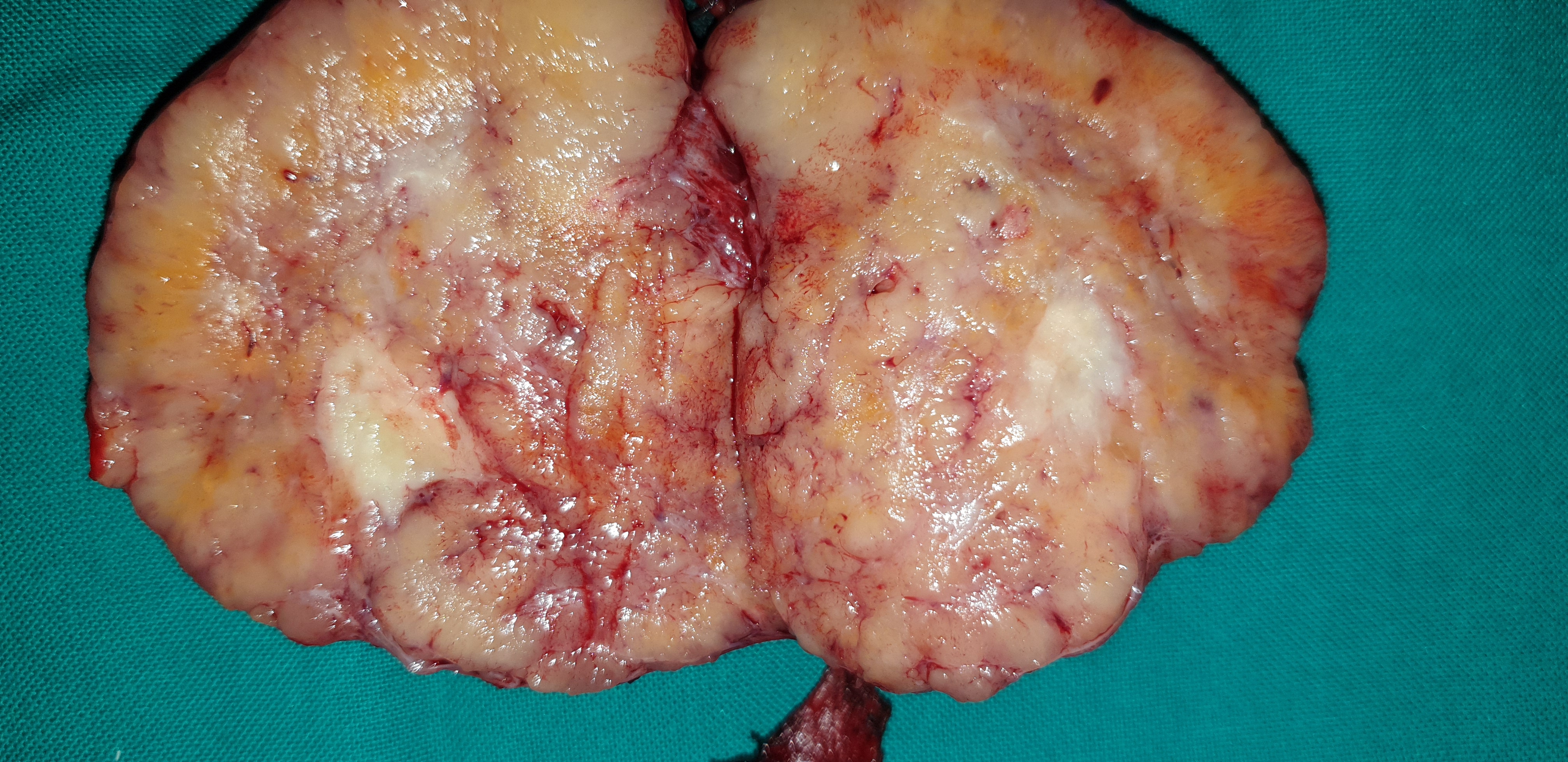
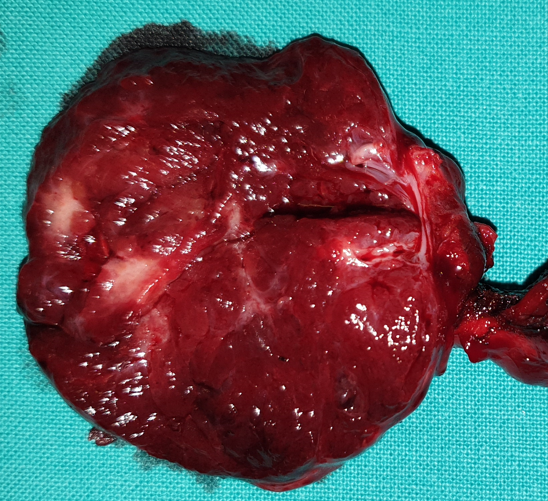
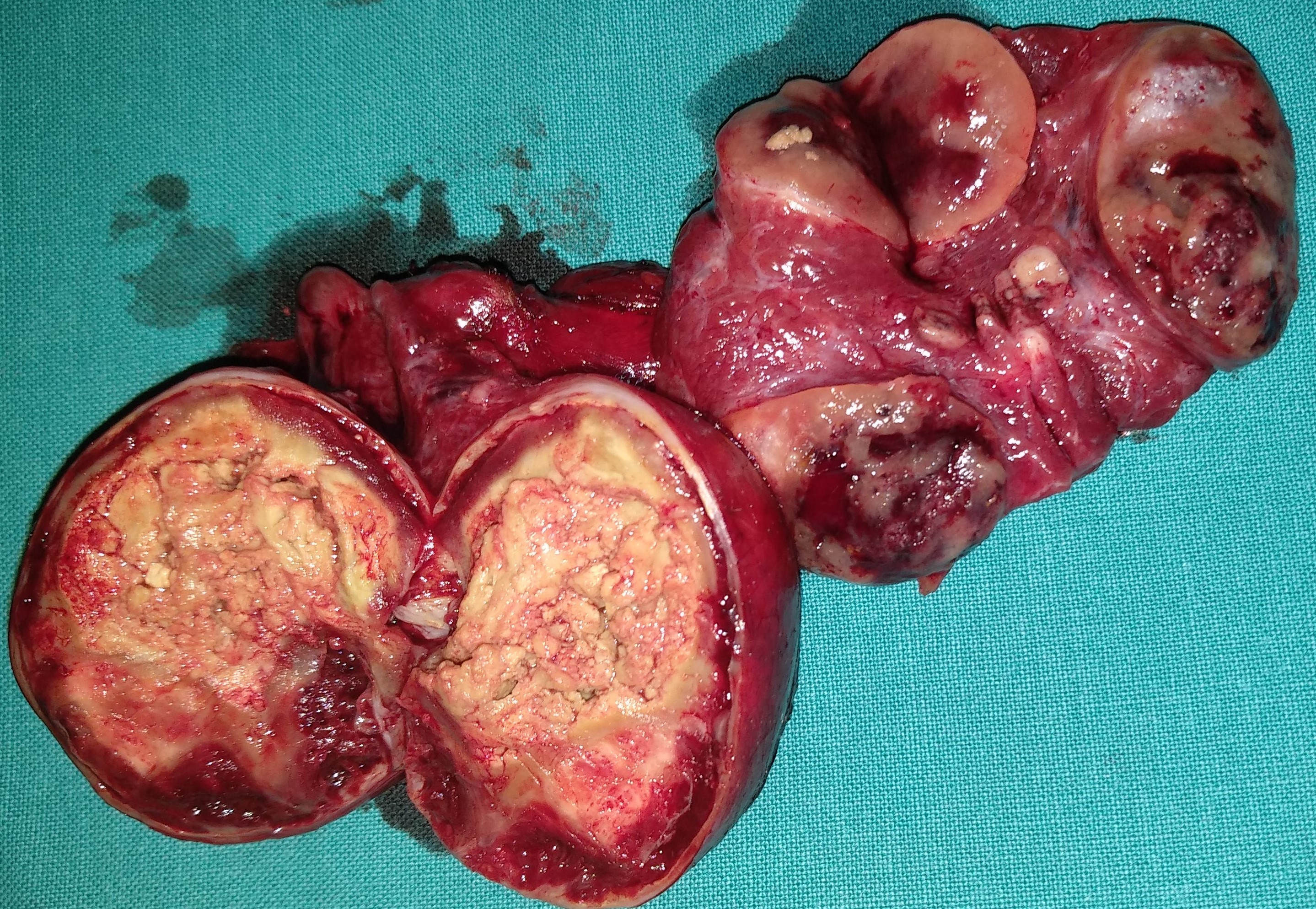
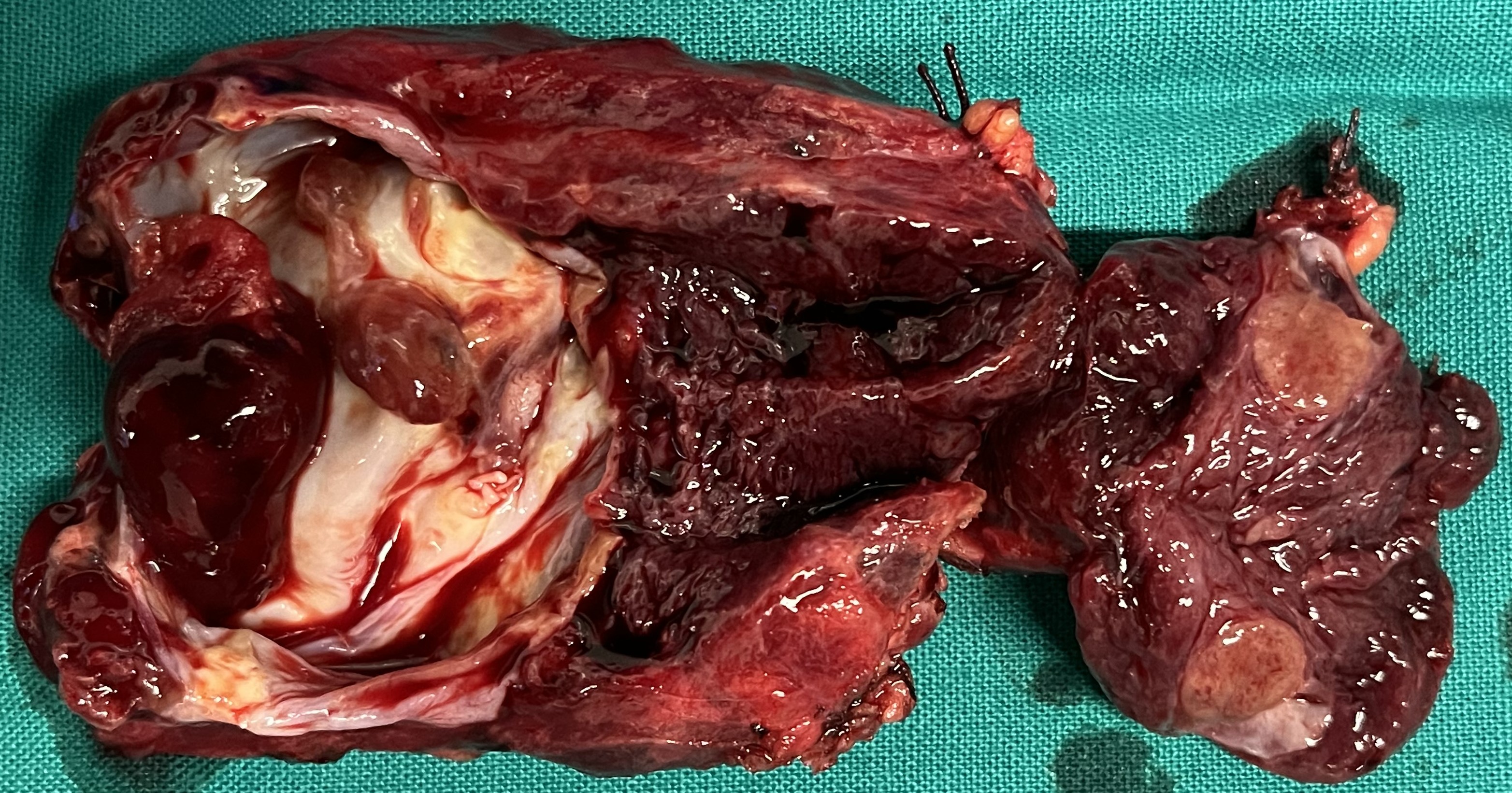
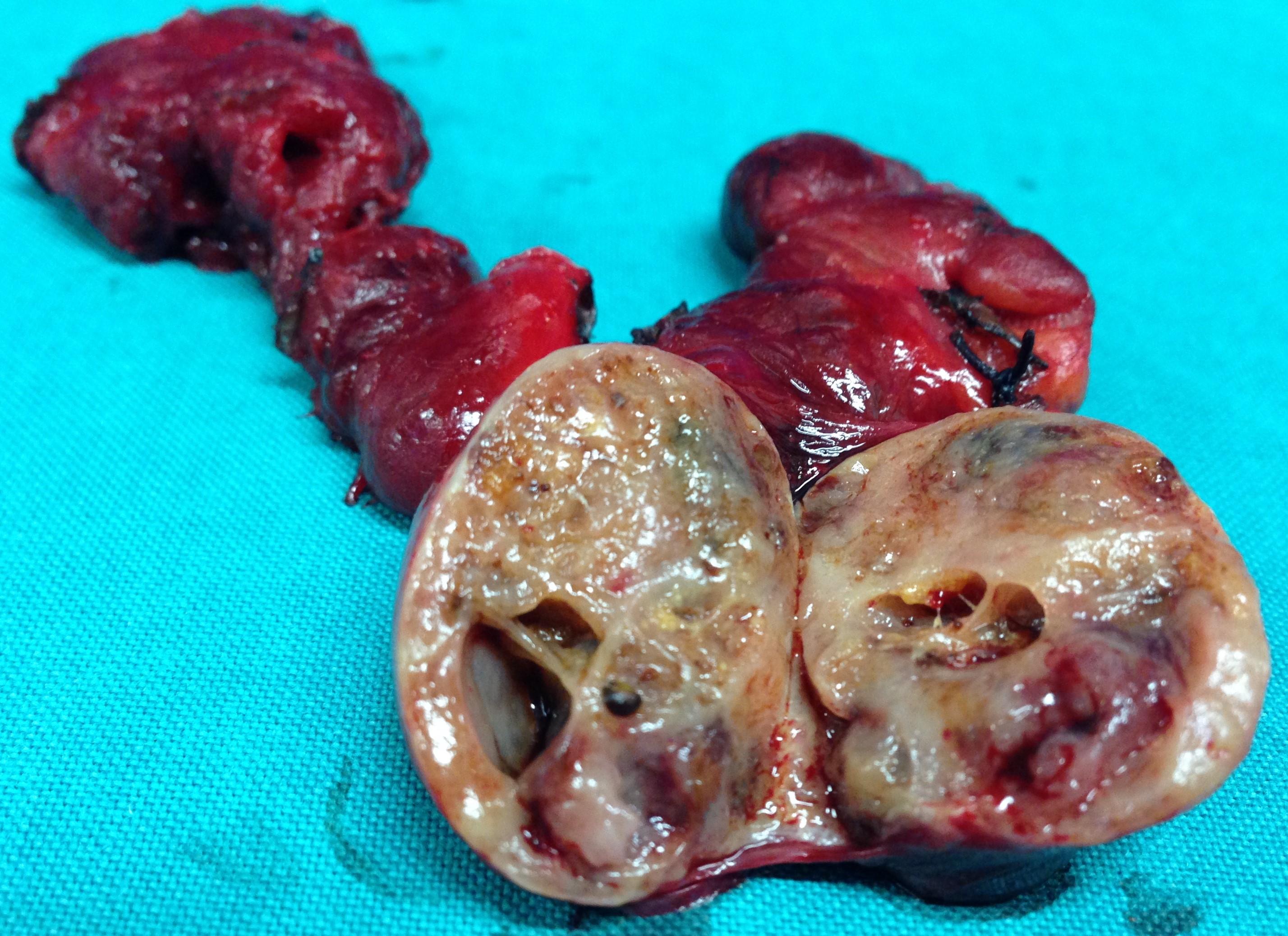
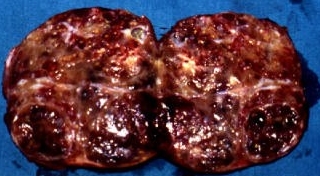
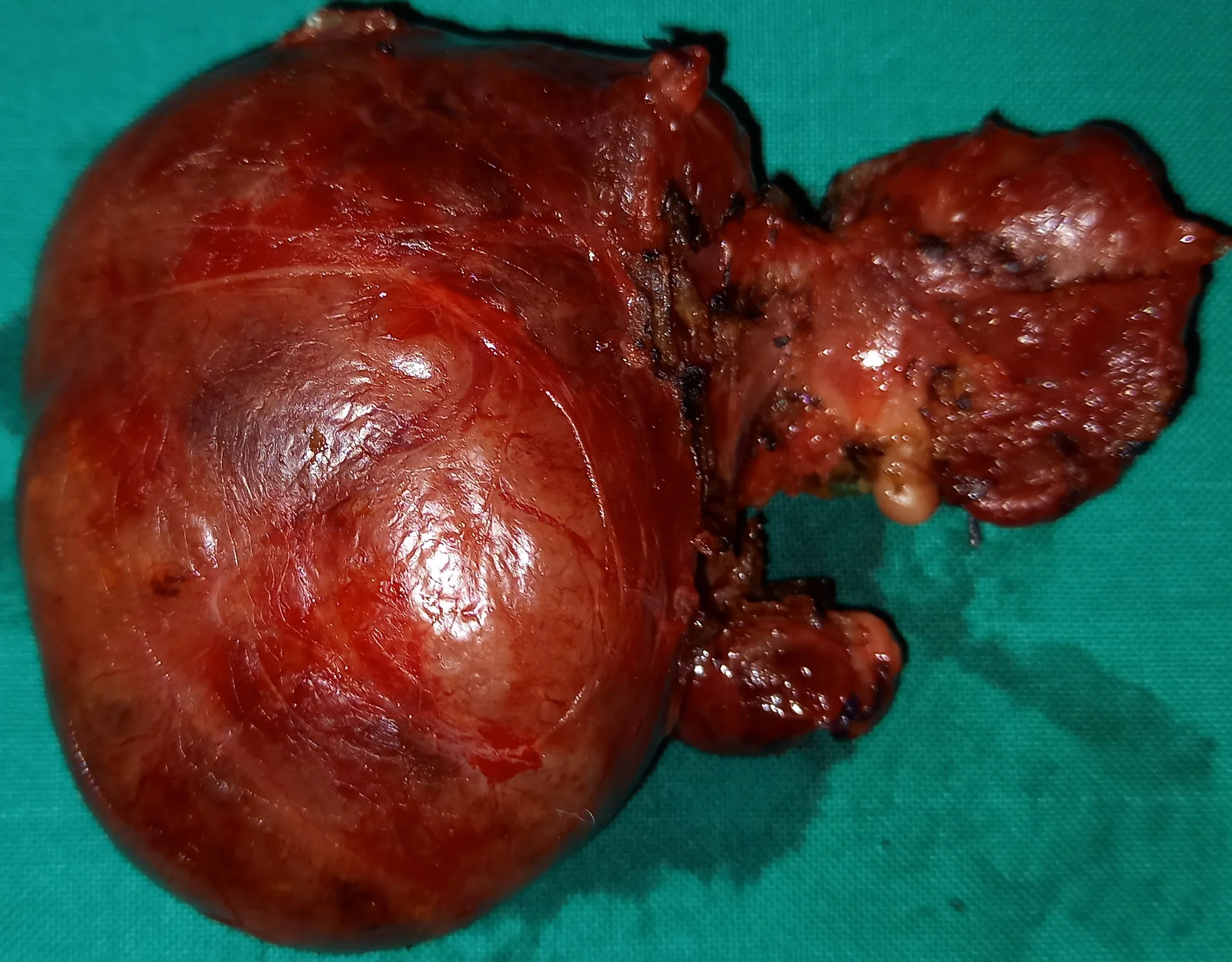
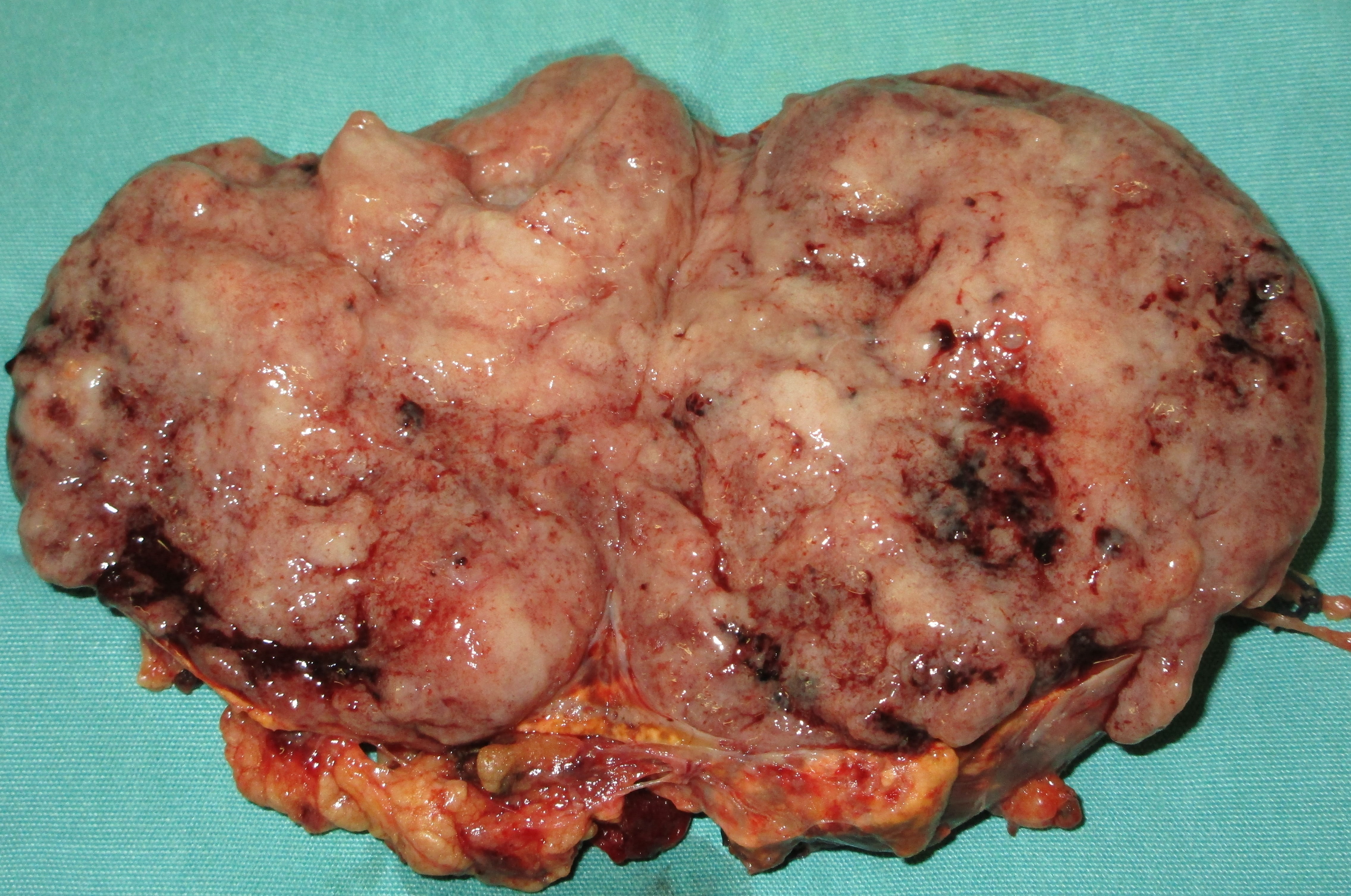
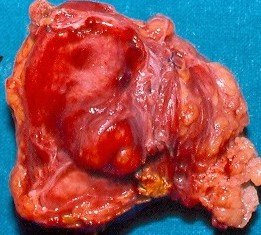
Cross section of the surgical specimen. Areas of necrosis are evident (Courtesy Dr. V. Penopoulos)

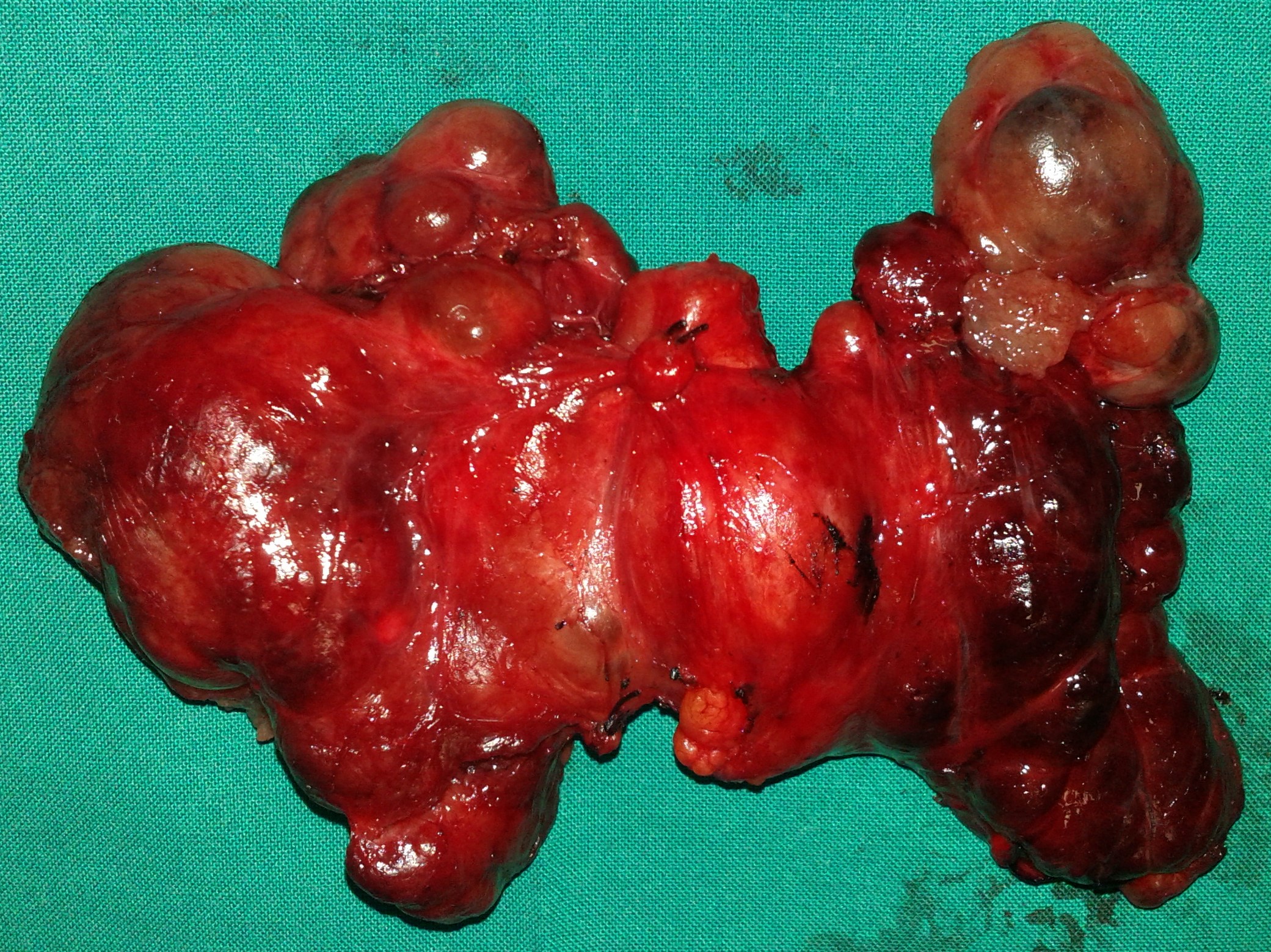
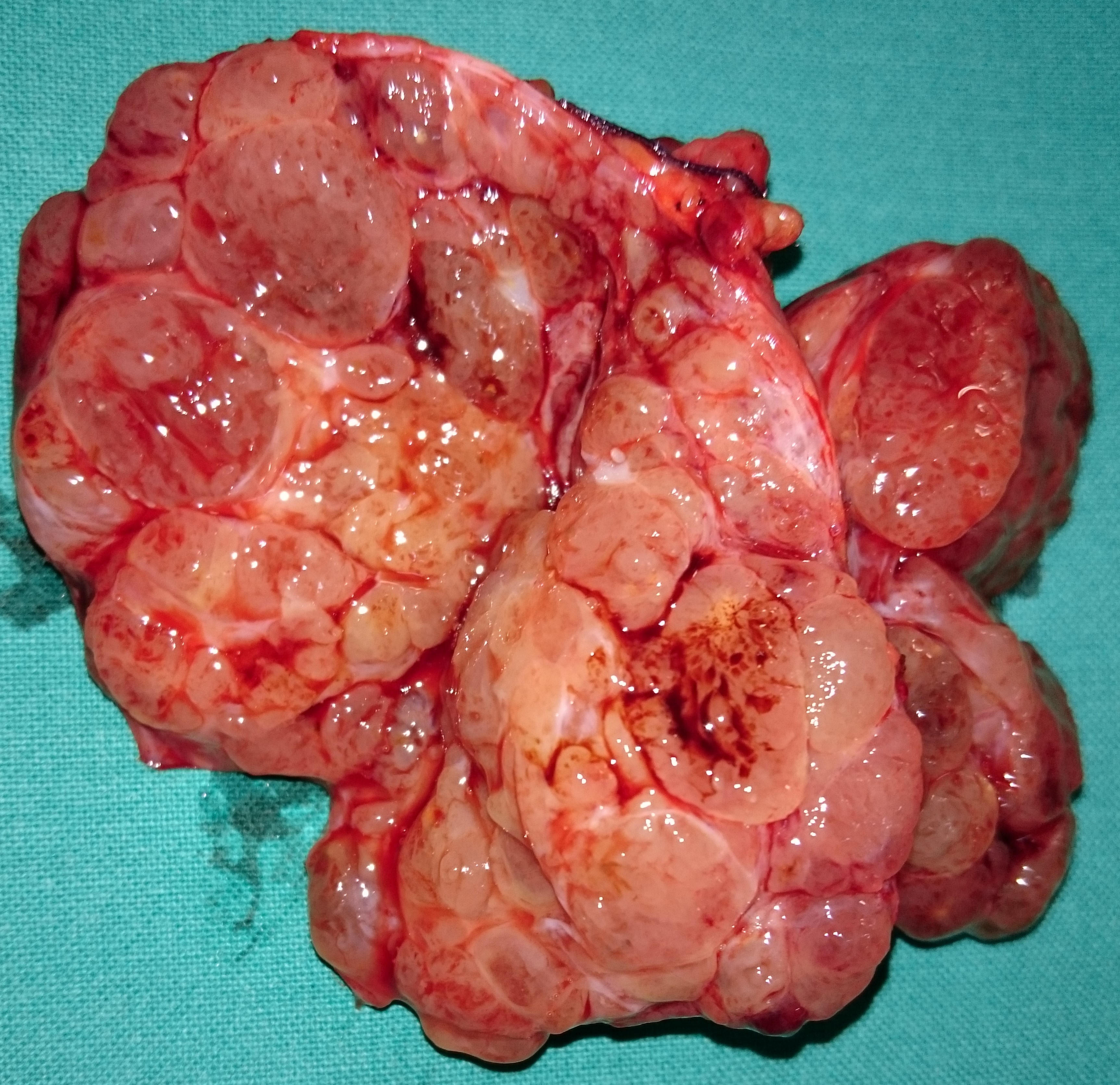
Multifocal papillary carcinomas,distributed in both thyroid lobes.(Courtesy Dr.V.Penopoulos).


Neck U/S.Hypoechoic nodule with microcalcifications in the thyroid isthmus.(Courtesy Dr.V.Penopoulos).
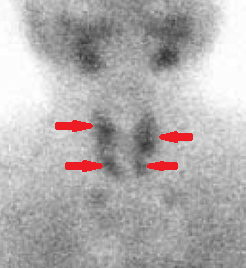
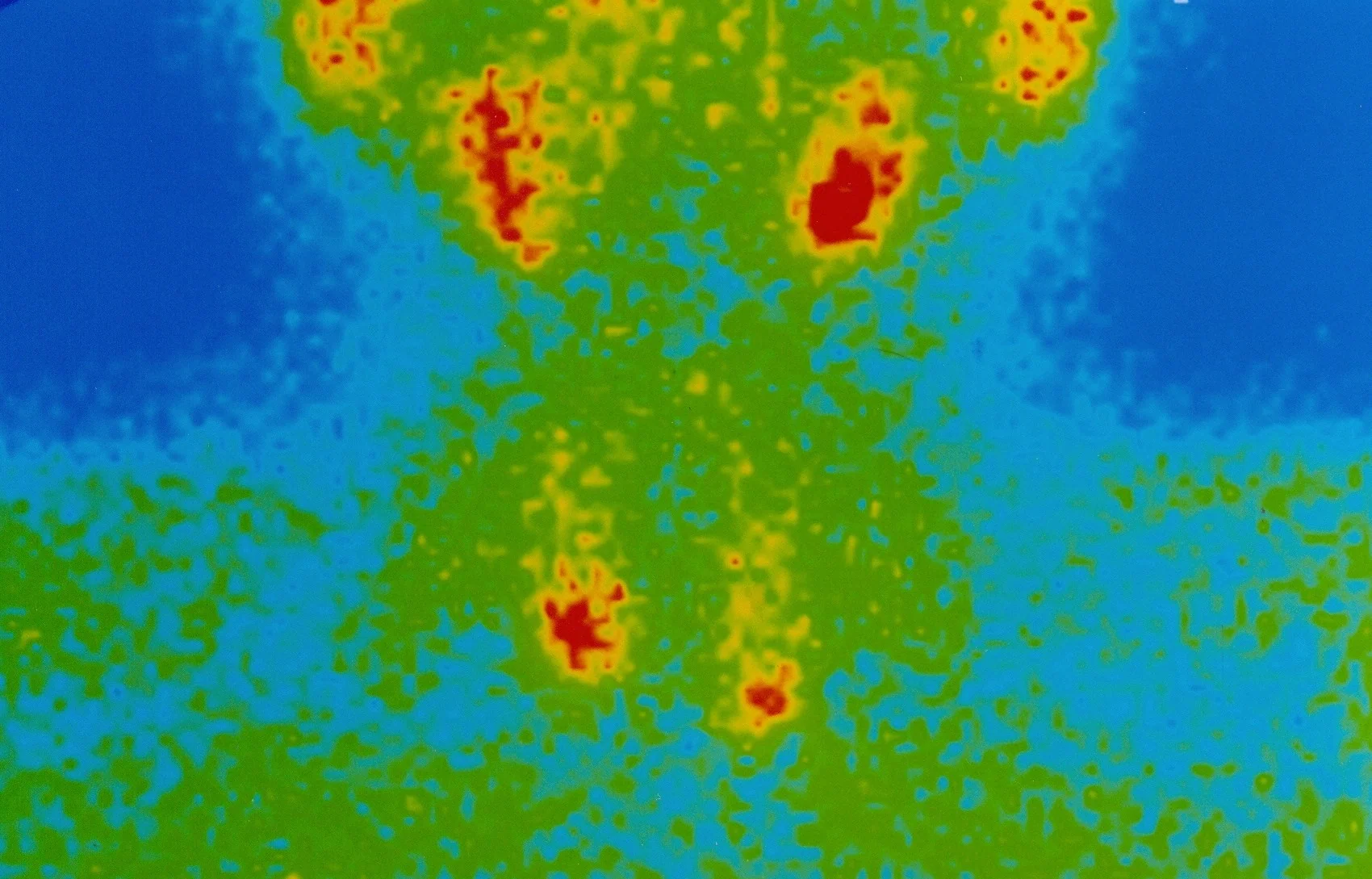
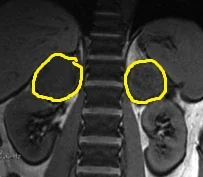
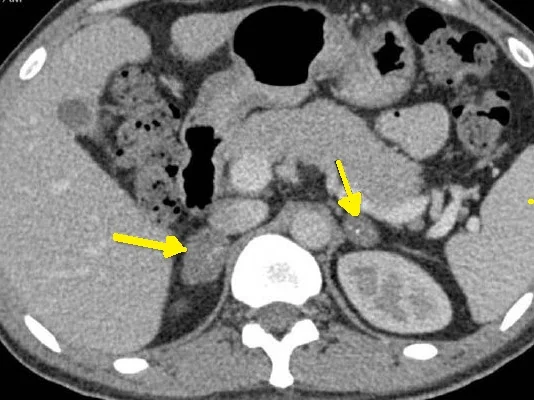
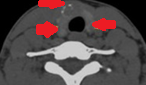
99mTc-MIBI SPECT scan.Red arrows-Hyperplasia of parathyroid glands.(Courtesy Dr.V.Penopoulos).
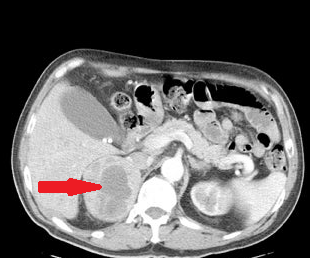
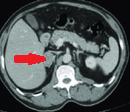
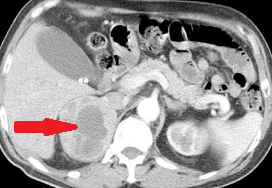
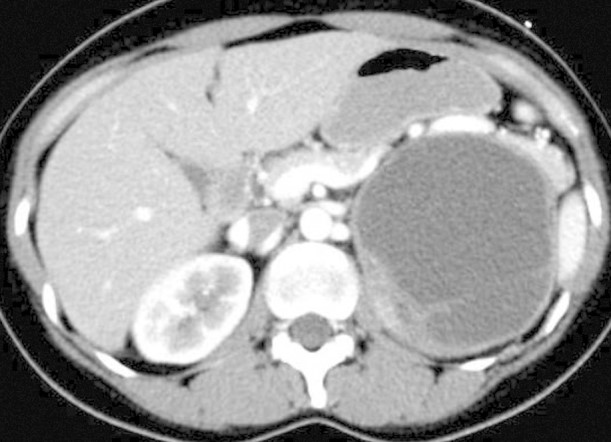
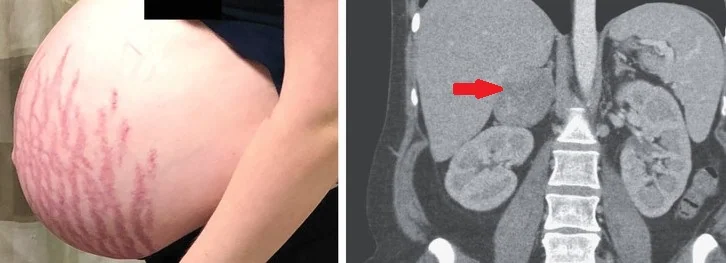
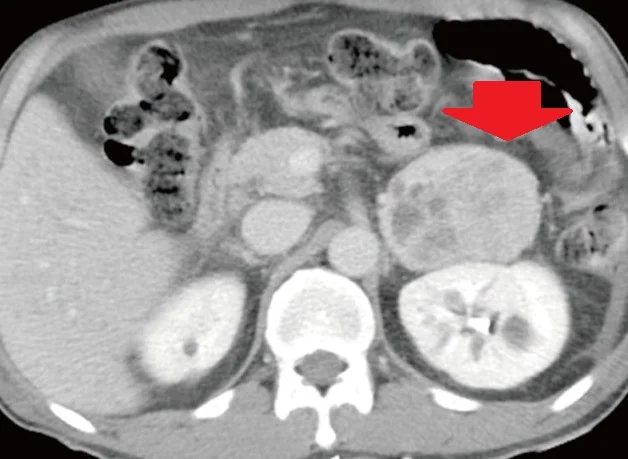
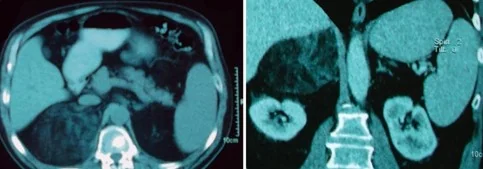
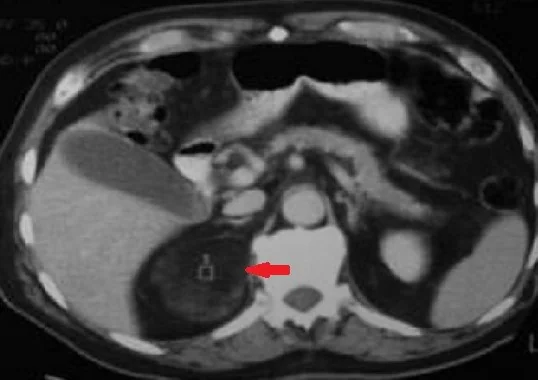
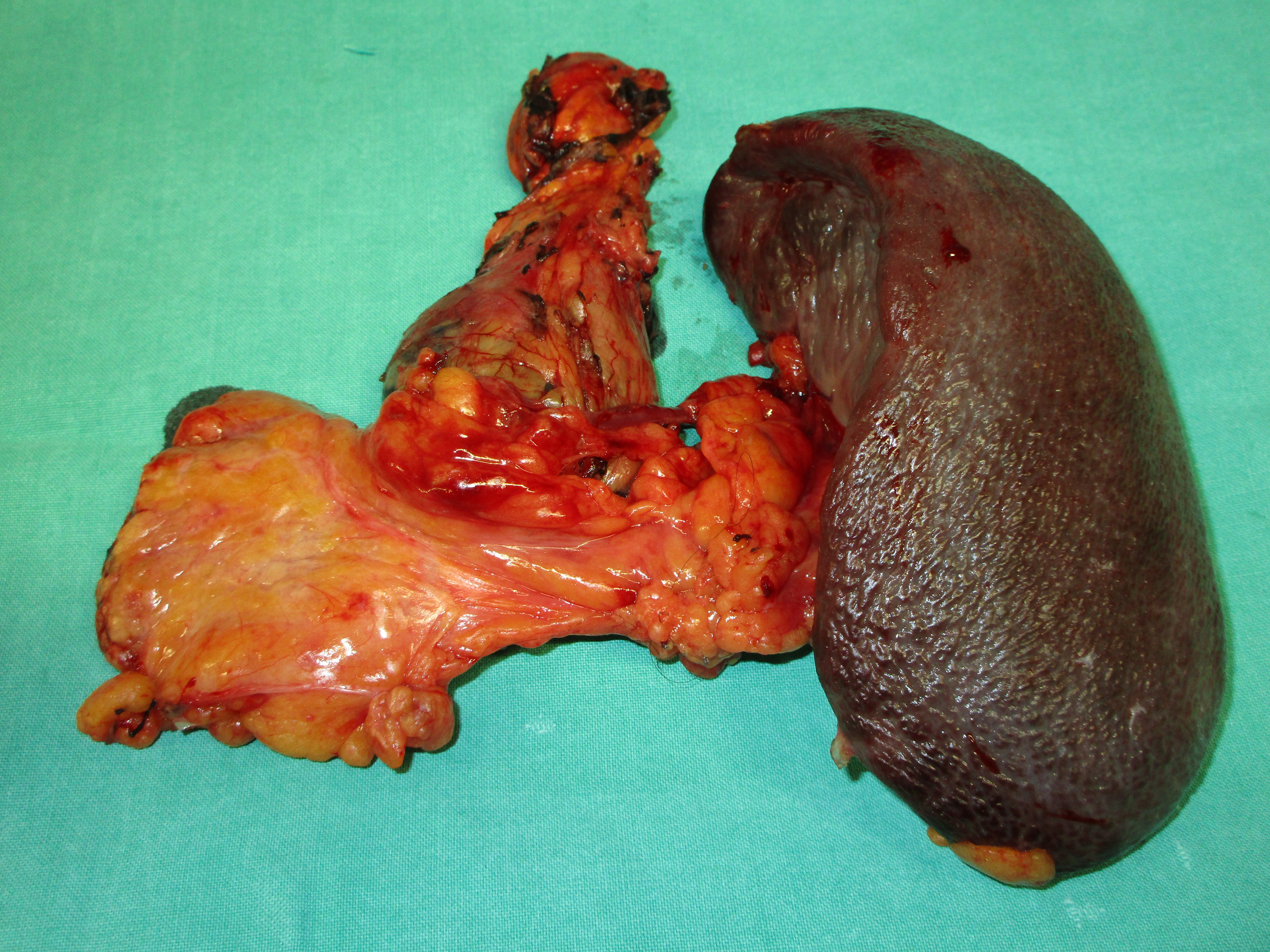
Abdominal CT Scan.Space occupying lesion, at the upper pole of the right kidney.(Courtesy Dr.V.Penopoulos).
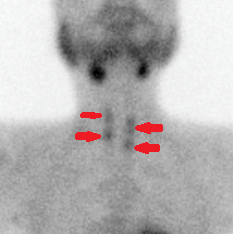
99mTc-MIBI SPECT scan.Red arrows-Hyperplasia of parathyroid glands.(Courtesy Dr.V.Penopoulos).

99mTc-MIBI SPECT scan.Red arrows-Hyperplasia of parathyroid glands.(Courtesy Dr.V.Penopoulos).


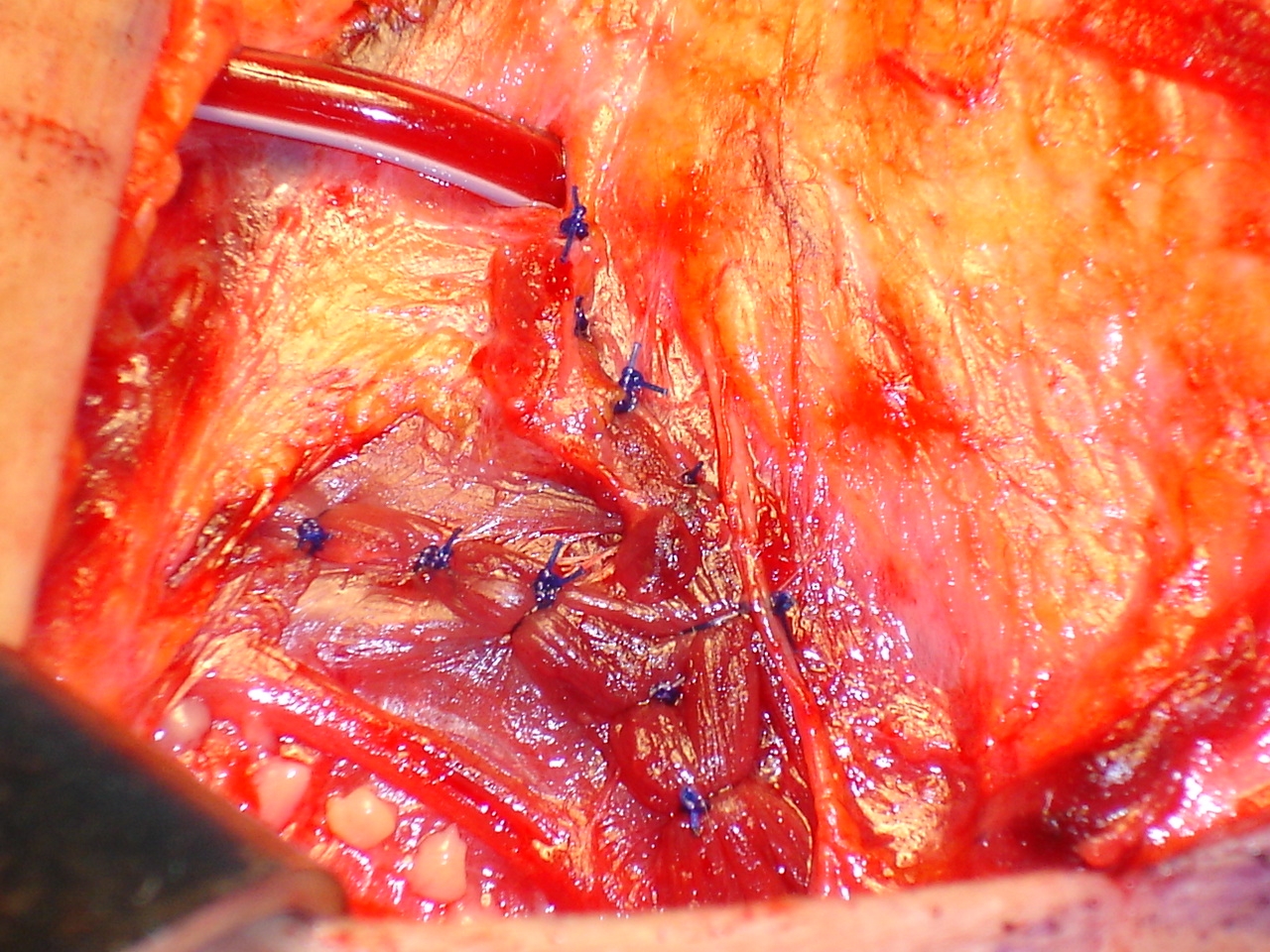
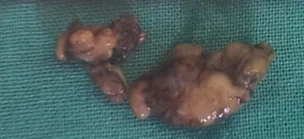
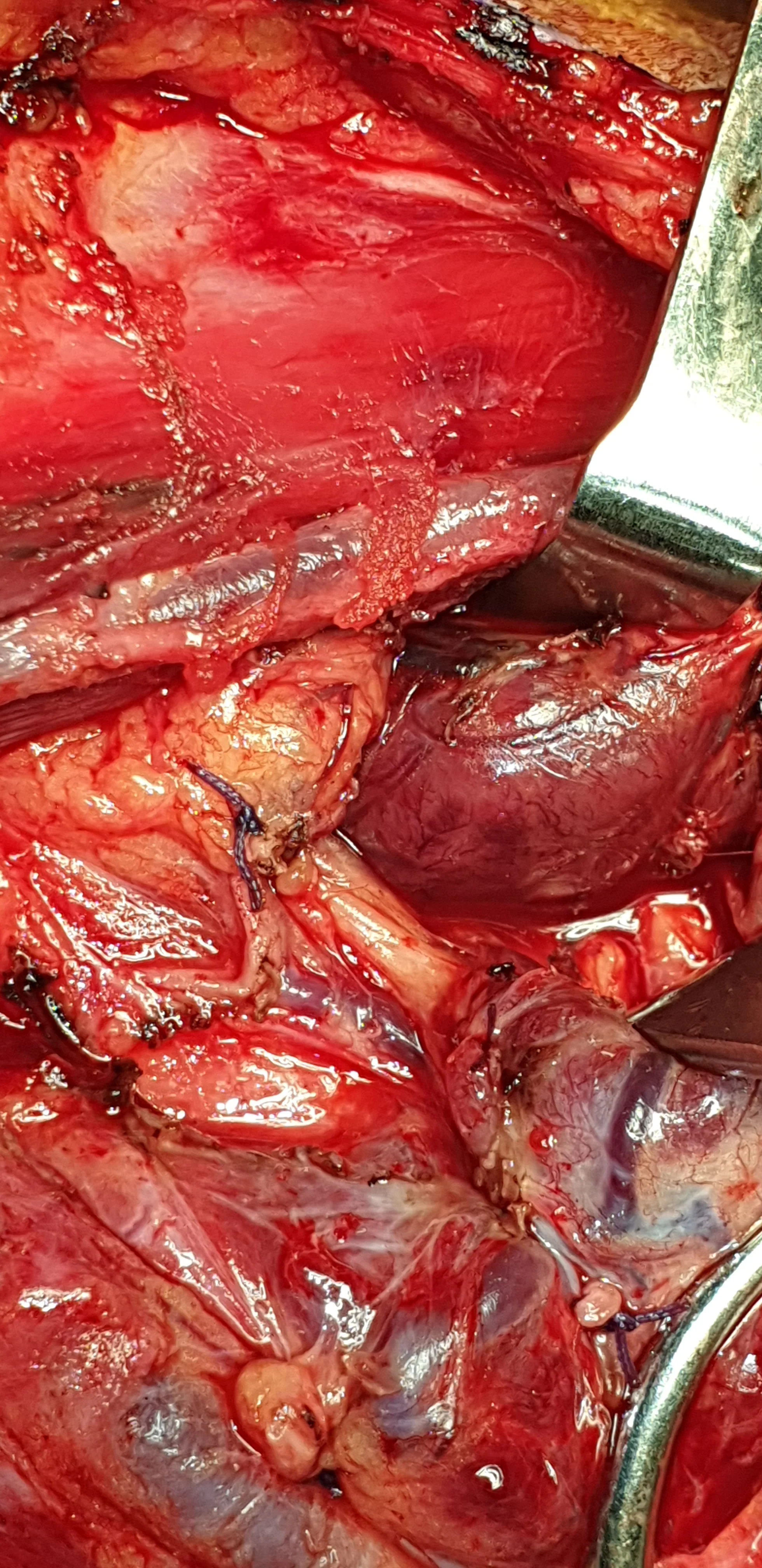
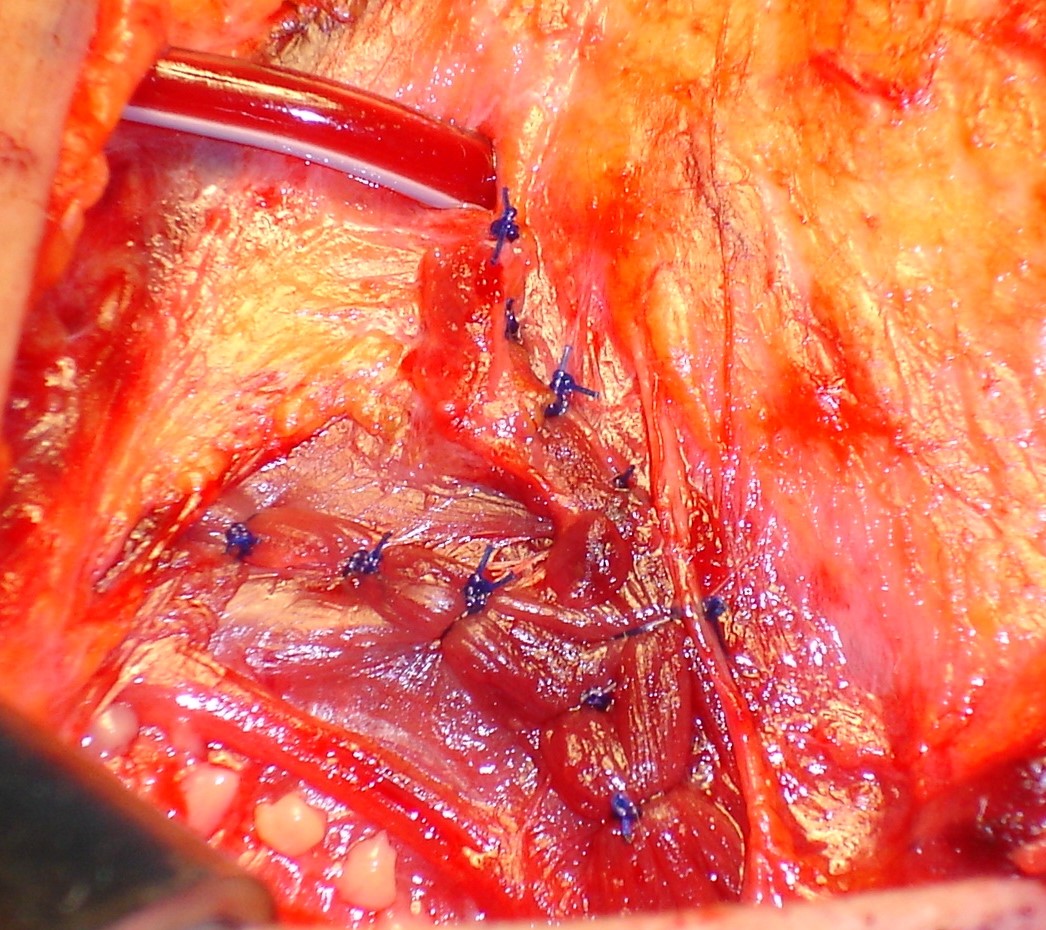
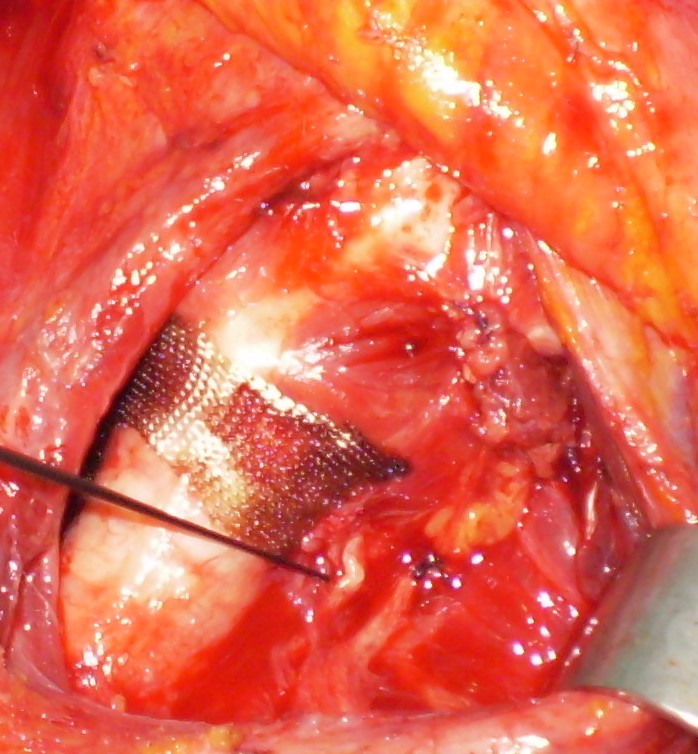
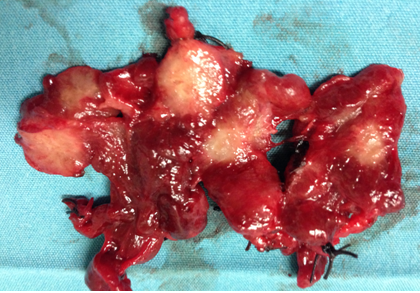
Autotransplantation of diffusely hyperplastic parathyroid tissue fragments into the right sternocleidomastoid muscle in two separately marked pockets (Courtesy Dr. V. Penopoulos)

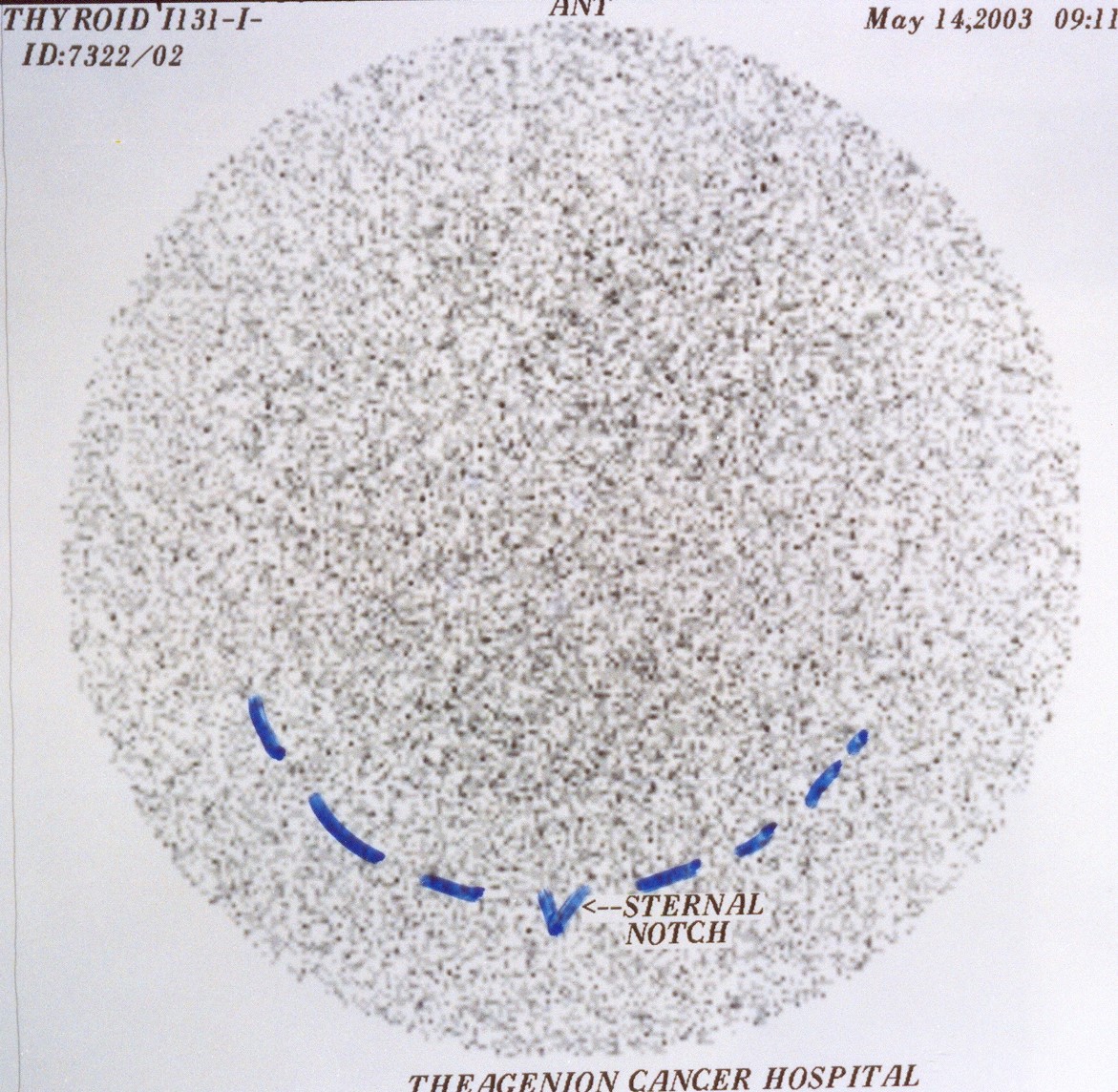
Scintigraphy with technetium 99m or iodine 131.Ectopic thyroid.(Courtesy Dr.V.Penopoulos).
Neck ultrasound. Well-circumscribed nodule corresponding to ectopic thyroid (Courtesy Dr. V. Penopoulos)

Neck U/S.Presence of a solid nodule in the left thyroid lobe.(Courtesy Dr.V.Penopoulos).