Περιτόναιο
30 images
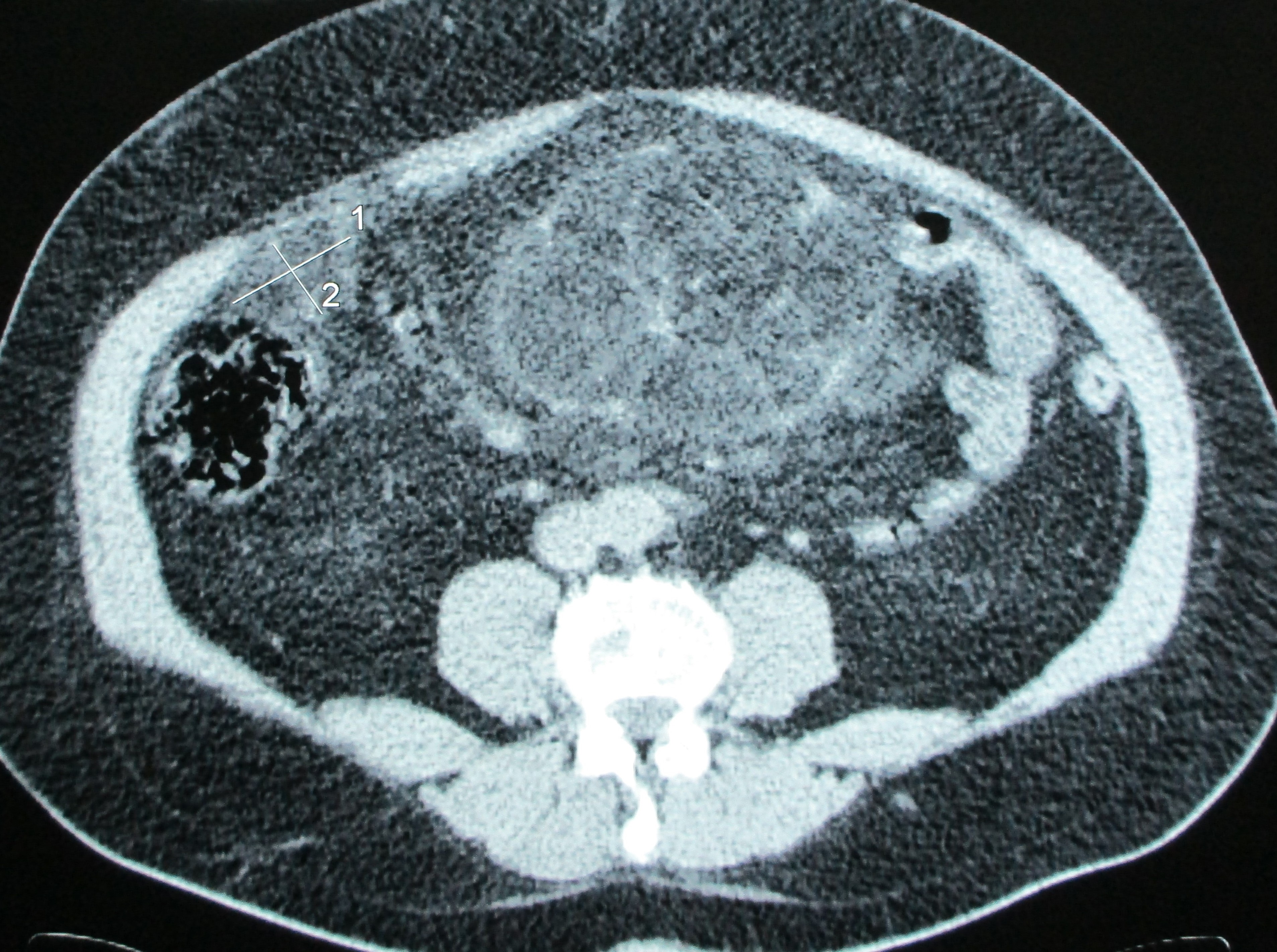
CYSTIC LYMPHANGIOMA
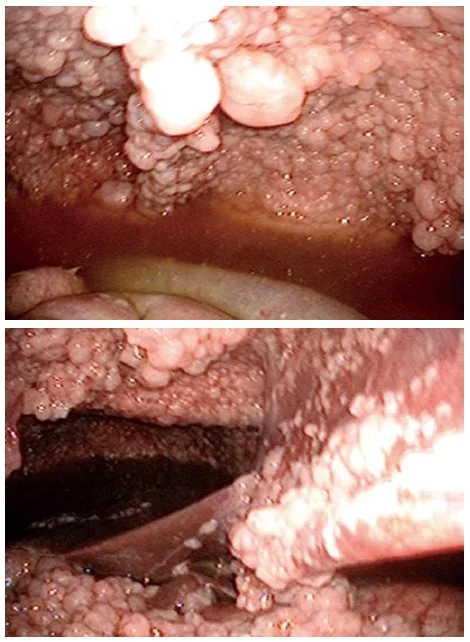
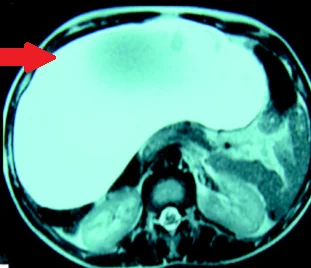
MALIGNANT MESOTHELIOMA
GIANT MESOTHELIAL CYST
CYSTIC PERITONEAL LYMPHANGIOMA
CHEMICAL PERITONITIS
SOLITARY PERITONEAL CYST
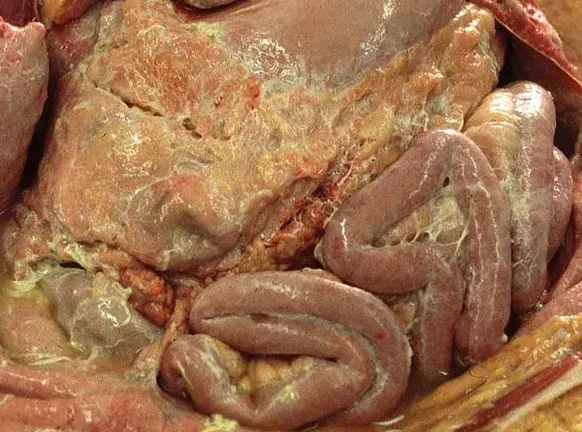
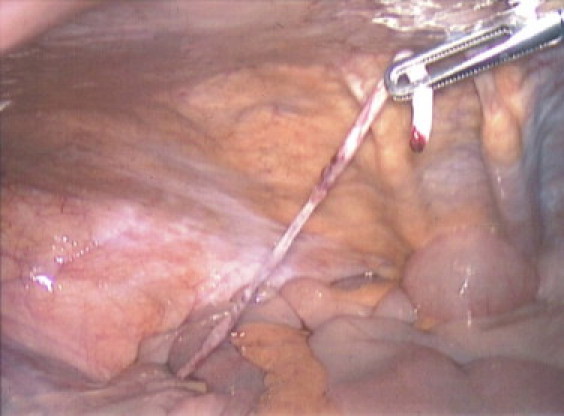
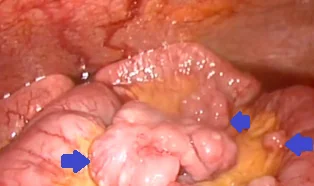
CONGENITAL BAND VITELLINE ARTERY
MALIGNANT PERITONEAL MESOTHELIOMA
PERITONITIS
ILEAL NET - PERITONEAL DISSEMINATION
KRUKENBERG TUMOR
PSEUDOMYXOMA PERITONEI-APPENDICEAL MUCINOUS NEOPLASM
WELL DIFFERENTIATED PAPILLARY MESOTHELIOMA
PSEUDOMYXOMA PERITONEI
PRIMARY PERITONEAL SEROUS CARCINOMA
BENIGN MULTICYSTIC PERITONEAL MESOTHELIOMA
MALIGNANT SARCOMATOID PERITONEAL MESOTHELIOMA
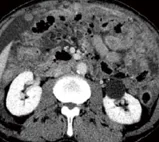
PERITONEAL CARCINOMATOSIS
PERITONEAL STROMAL TUMOR
DISSEMINATED PERITONEAL LEIOMYOMATOSIS
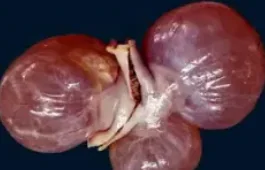
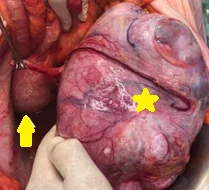
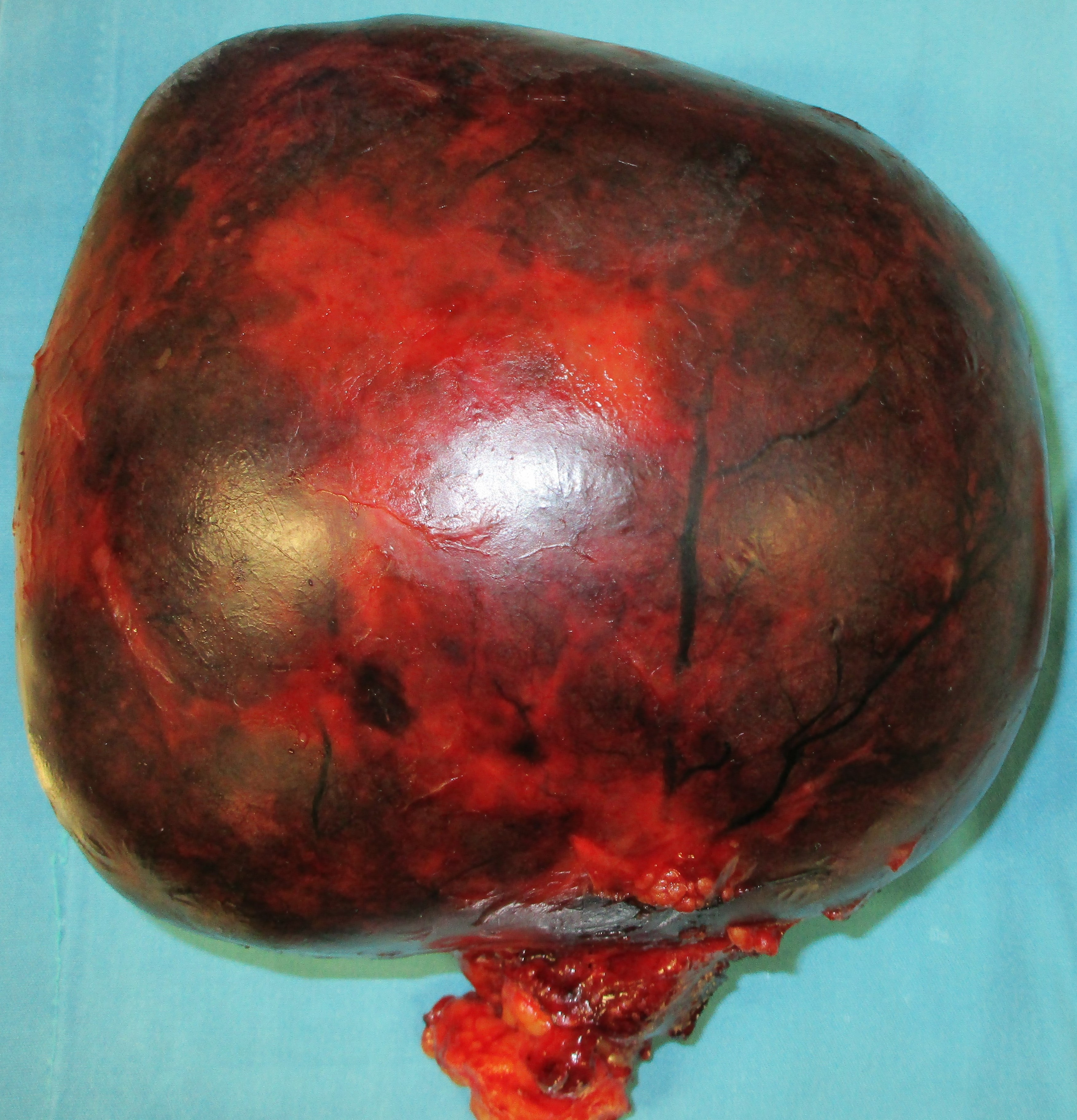
PRIMARY PERITONEAL TUMOR - SPECIMEN
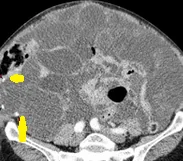
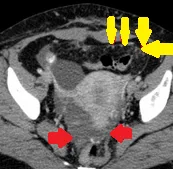
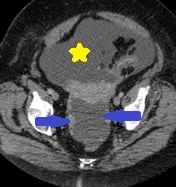
PRIMARY PERITONEAL TUMOR