Large Intestine
Παχύ Έντερο
634 images · 4 sub-chapters





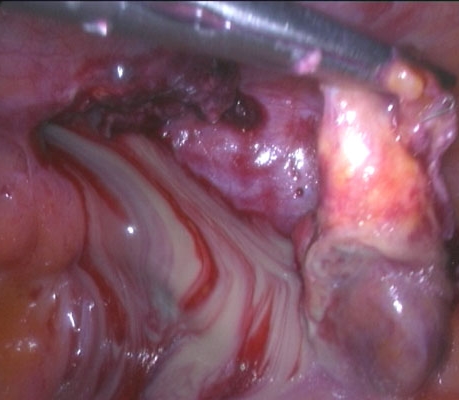
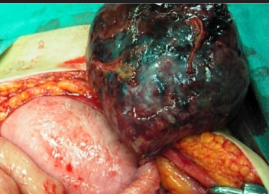
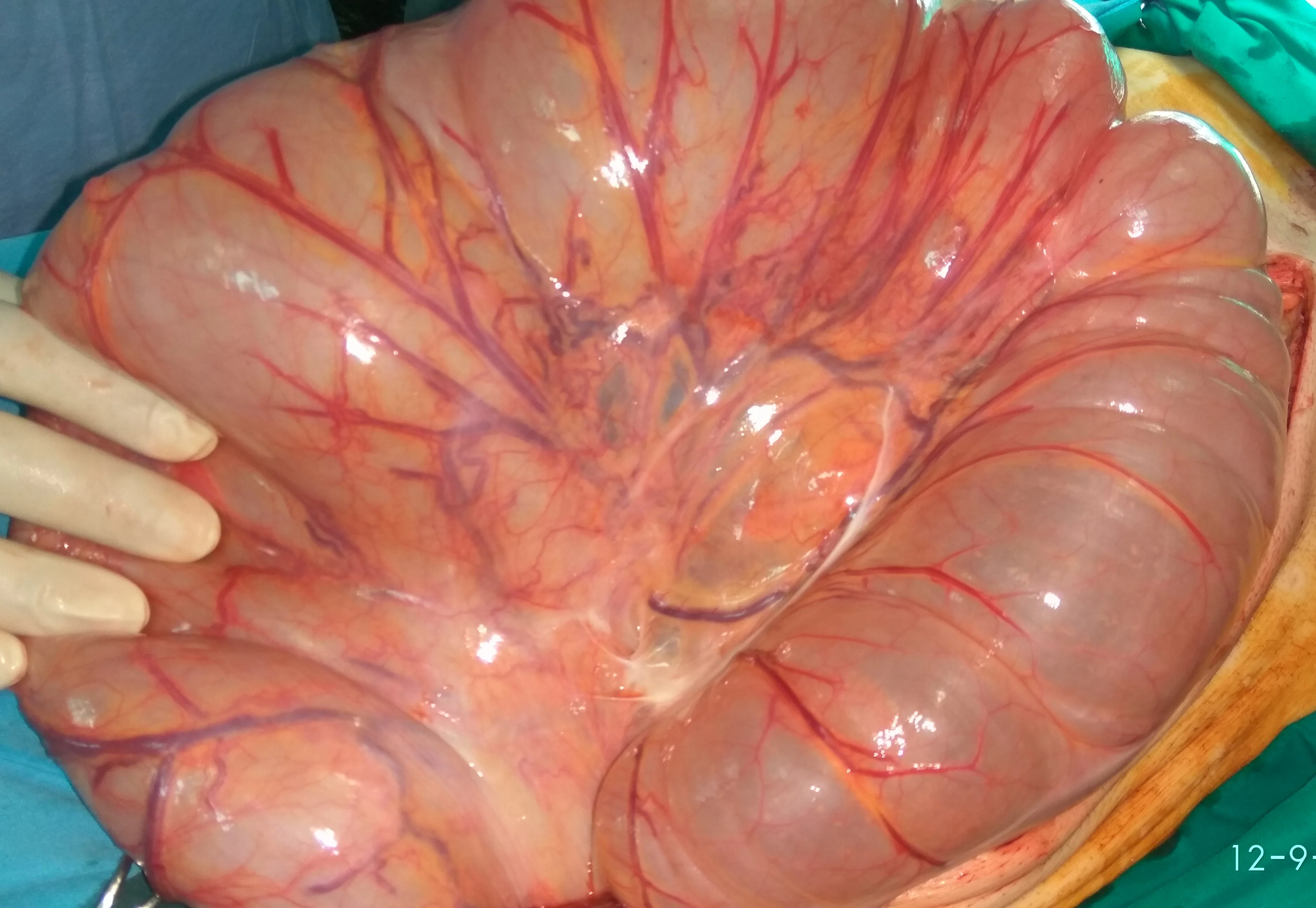
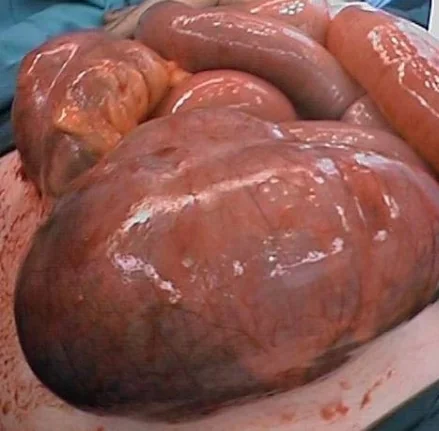
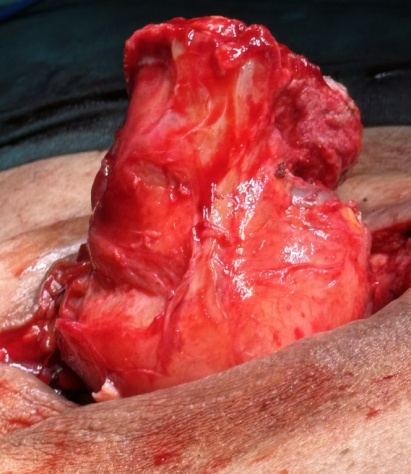
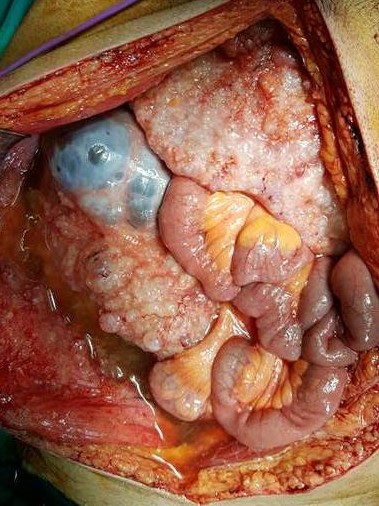
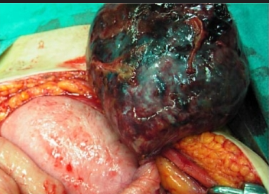
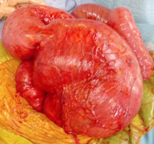
The patient on the operating table.Massive abdominal distension.(Courtesy Dr.V.Penopoulos).
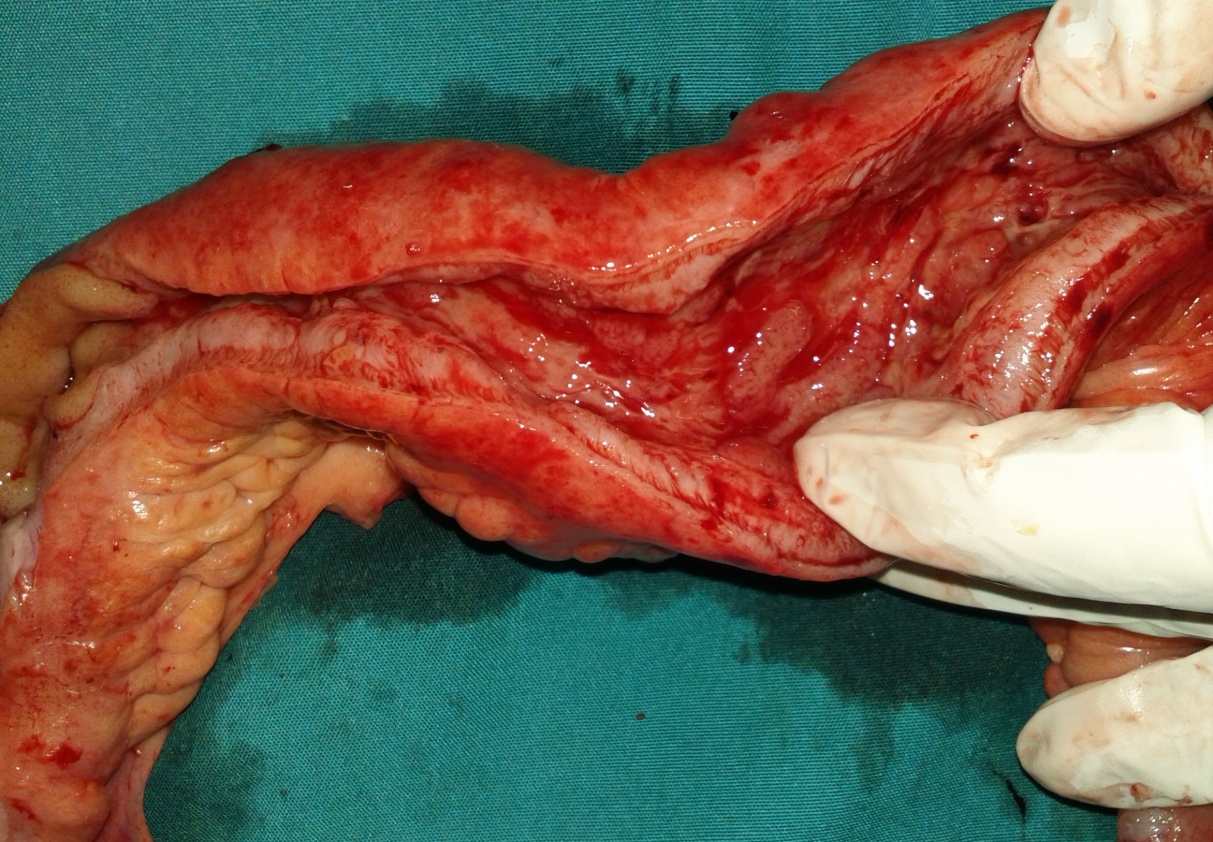
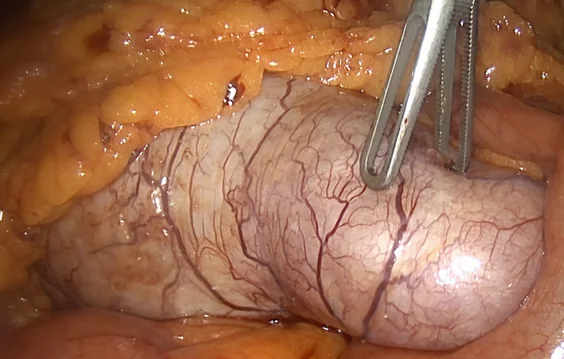
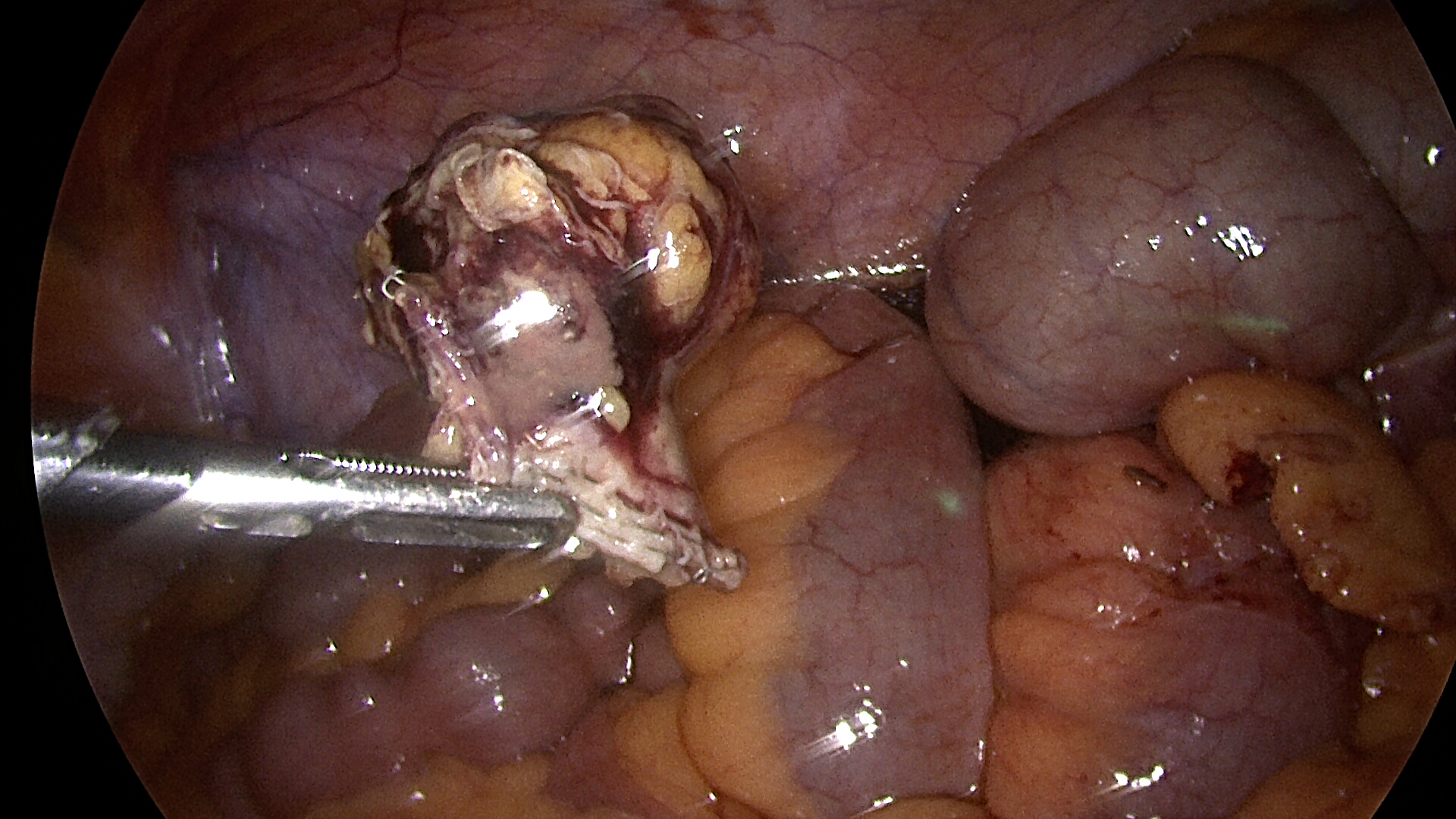
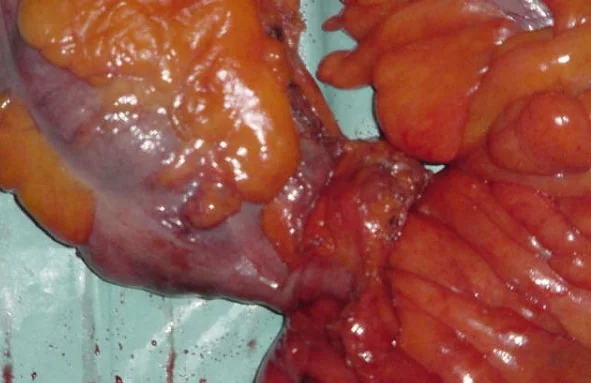
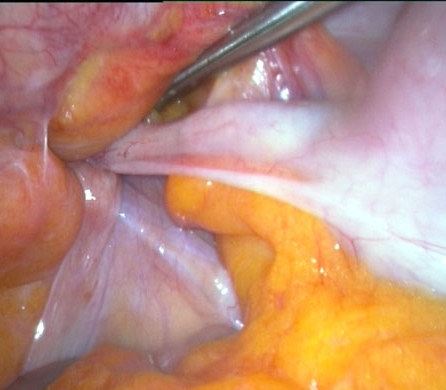
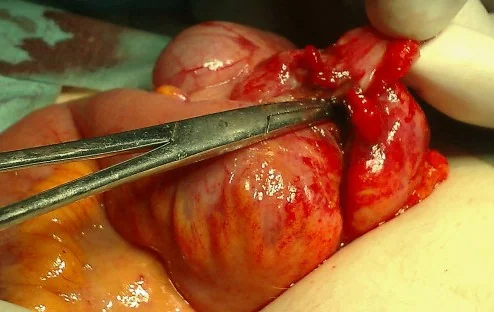
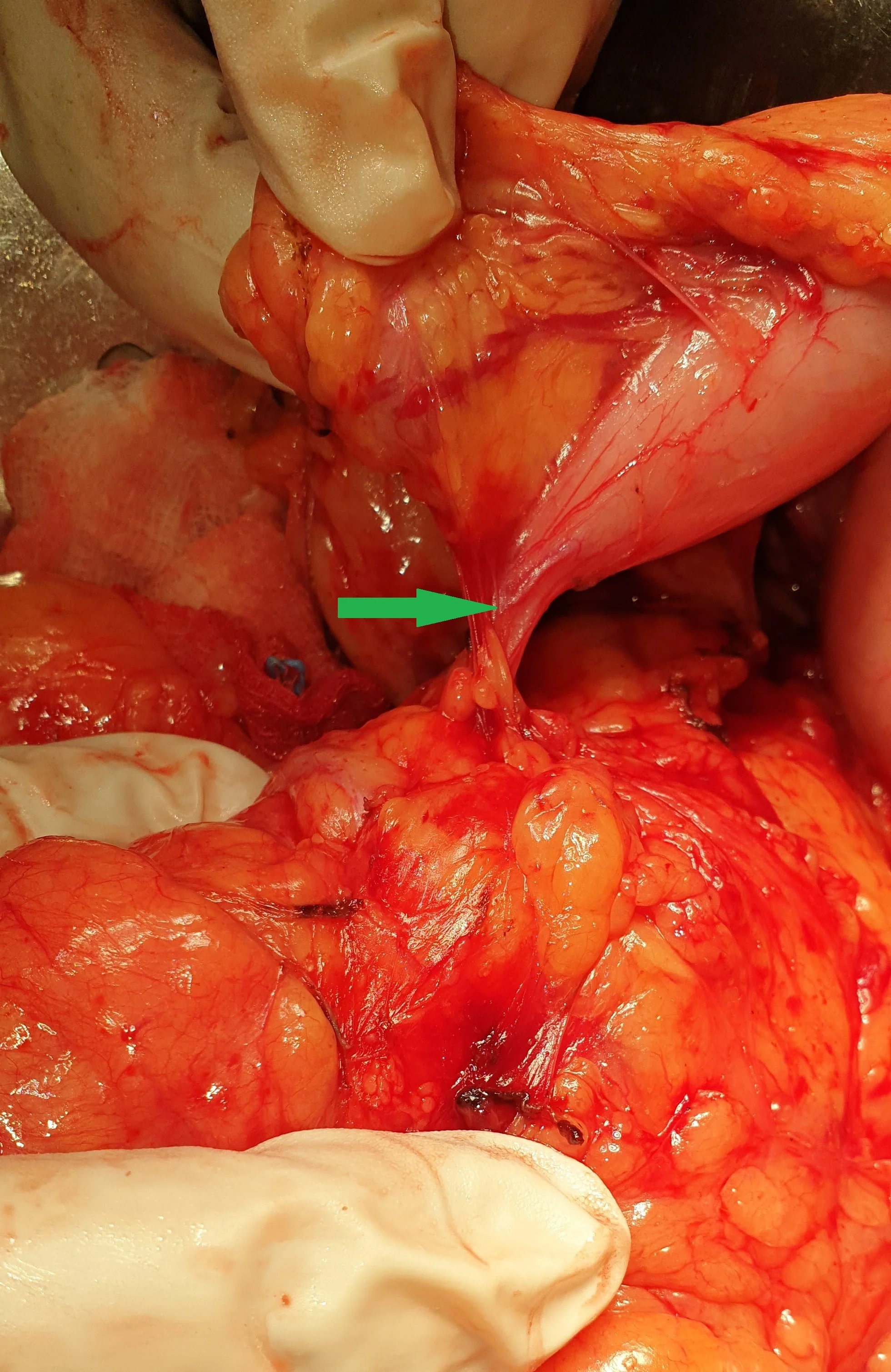
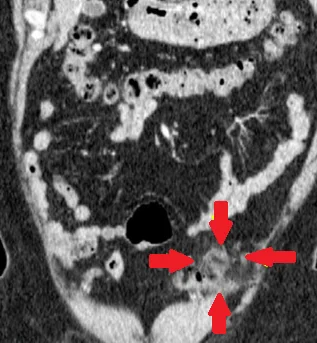
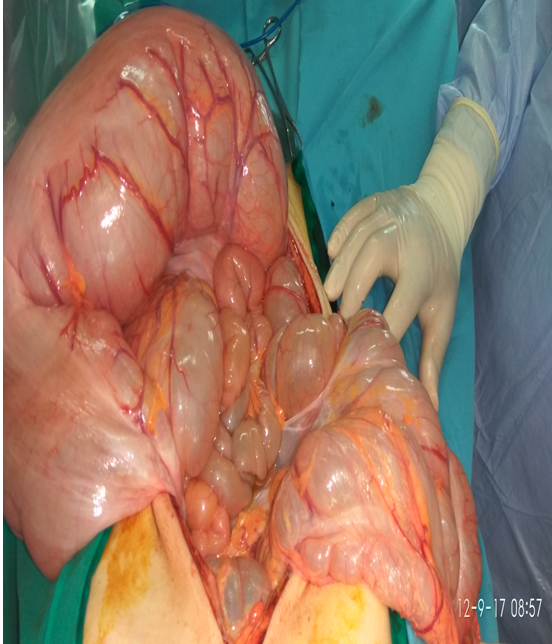
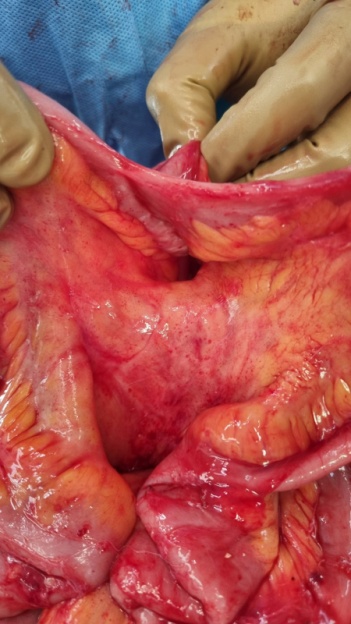
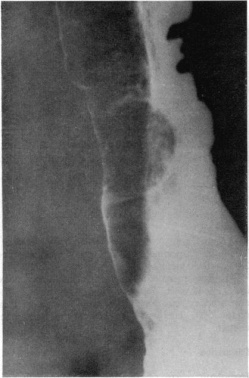
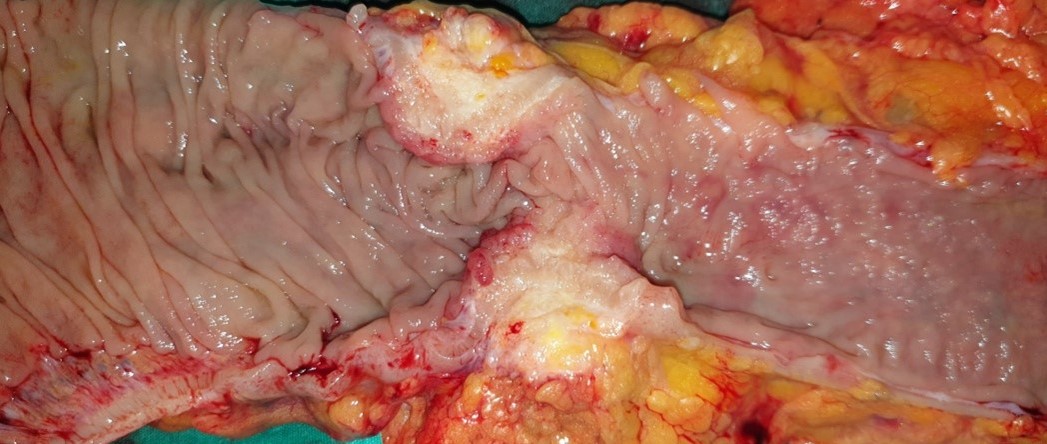
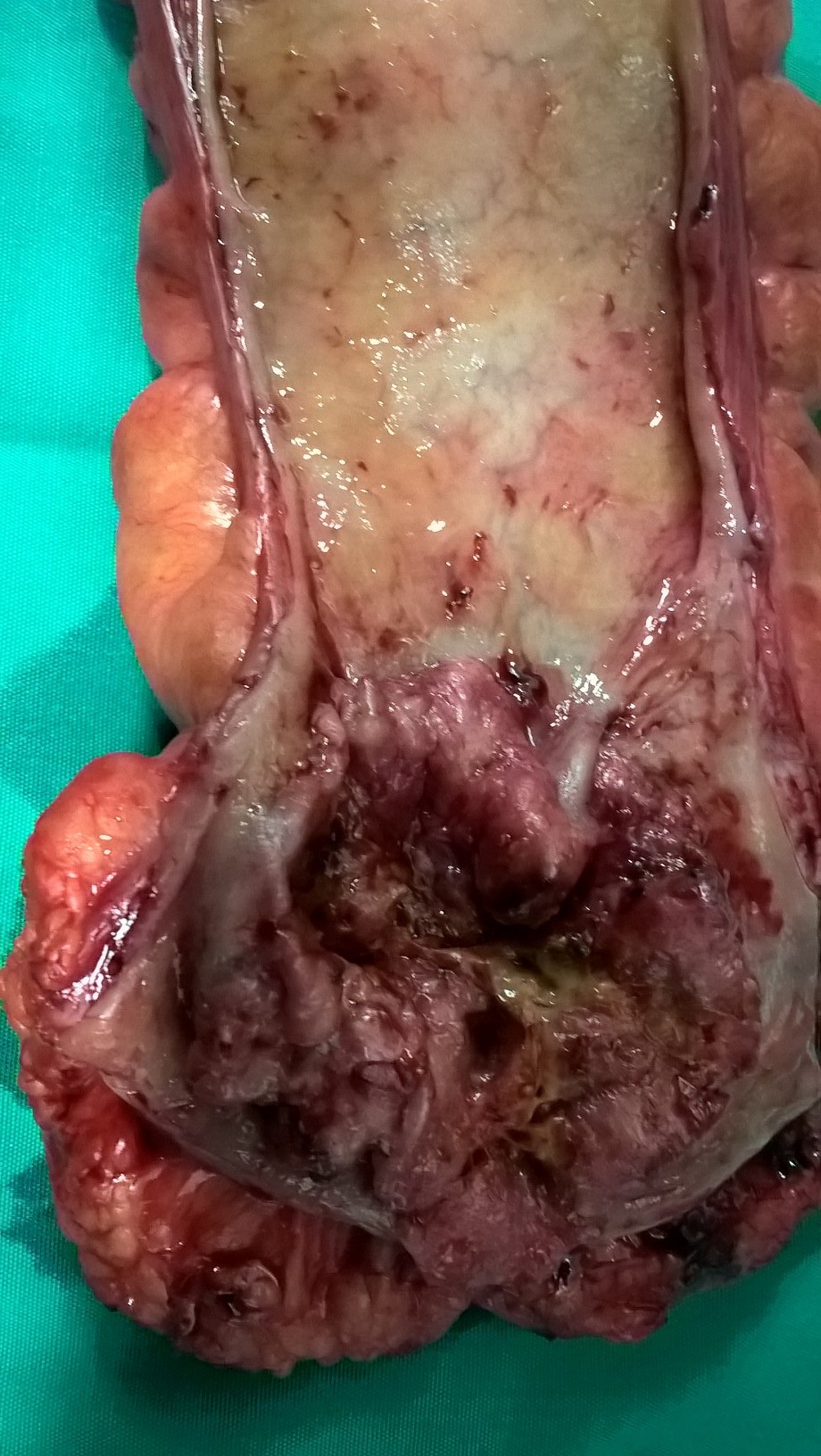
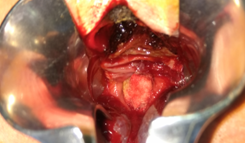
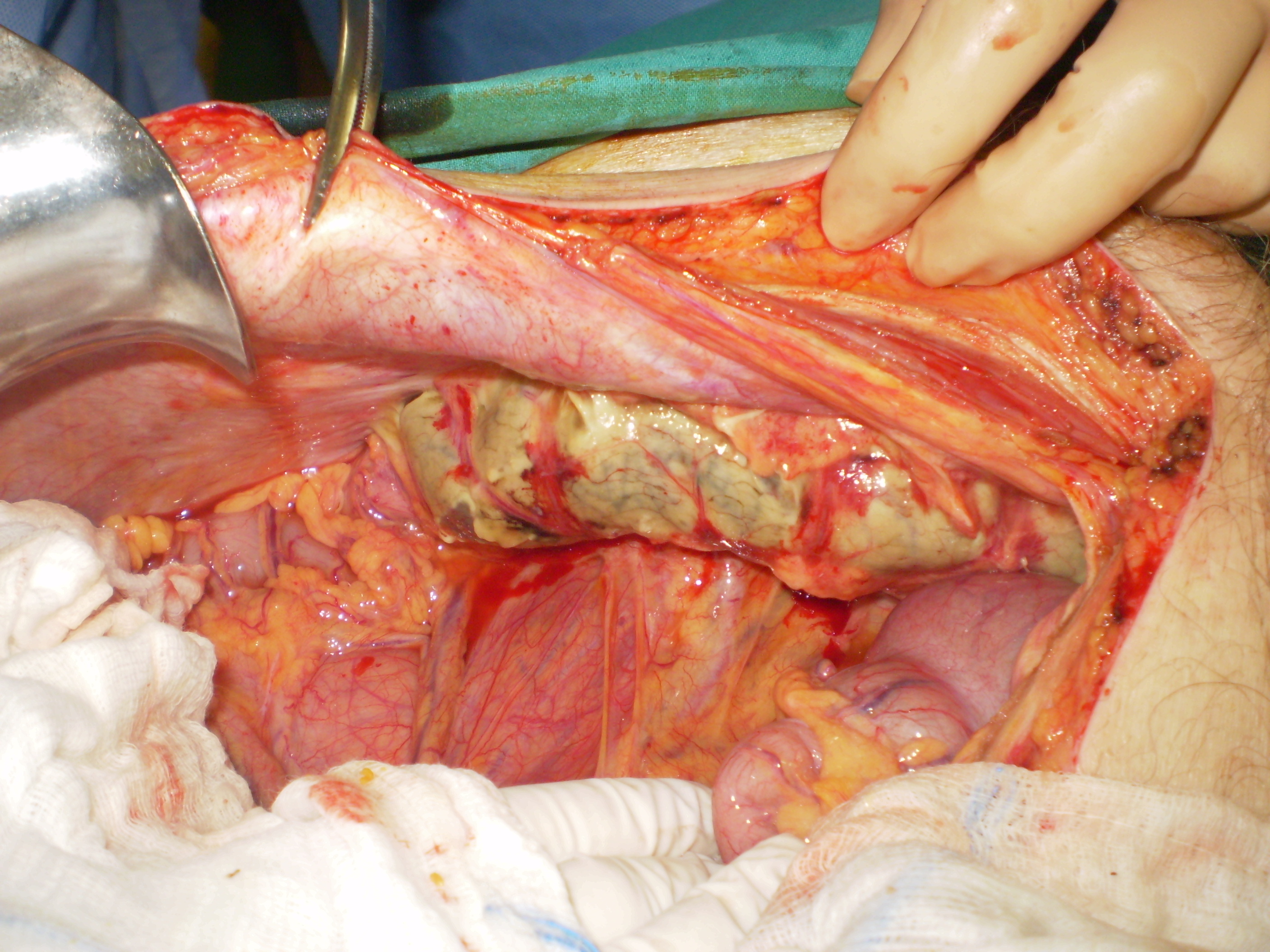
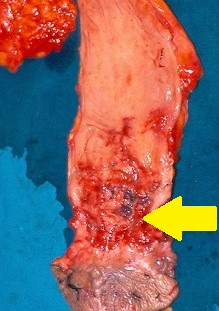
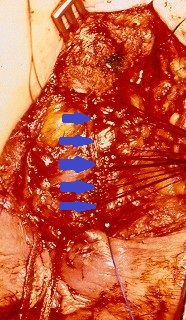
The terminal ileal stricture is evident between the surgeon's fingers (Courtesy Dr. V. Penopoulos)
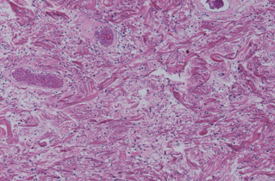
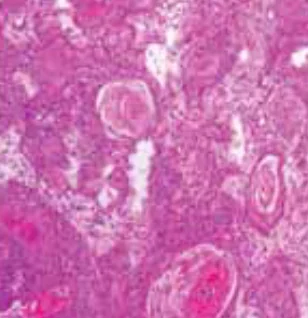
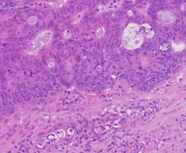
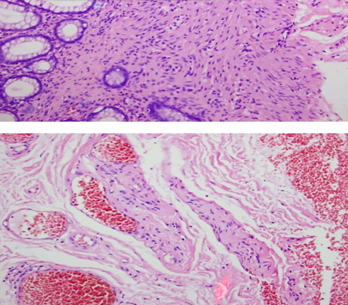
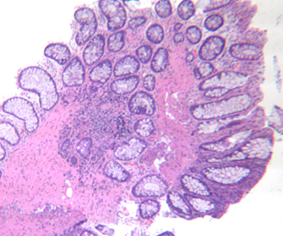
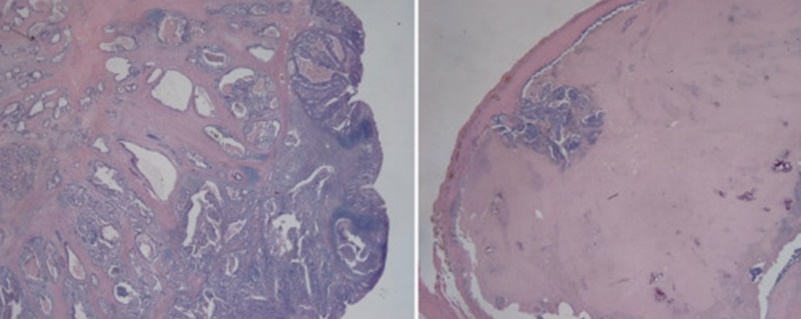
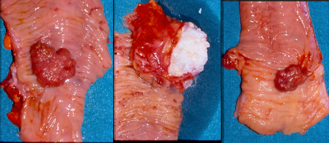
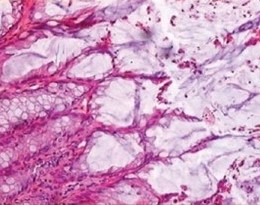
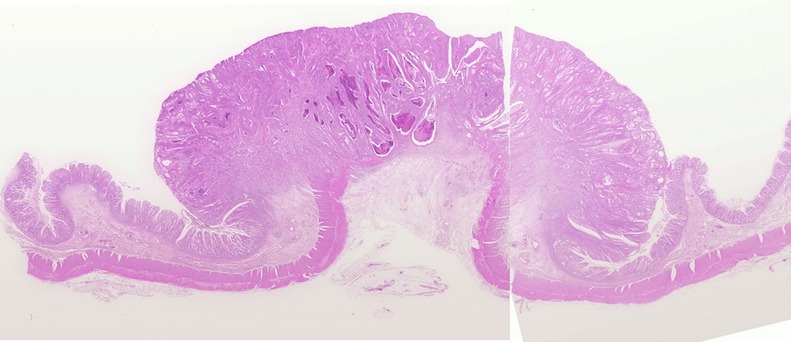
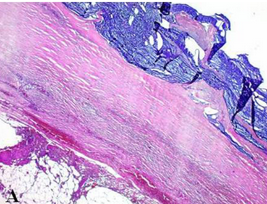
Microscopic image after Hematoxylin and Eosin staining, showing fibrous connective tissue without atypia, resembling skin fibroma (Courtesy Dr. V. Penopoulos)






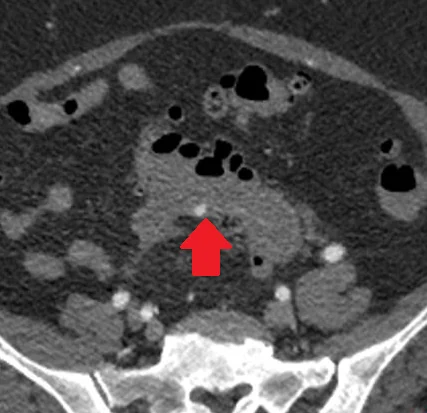
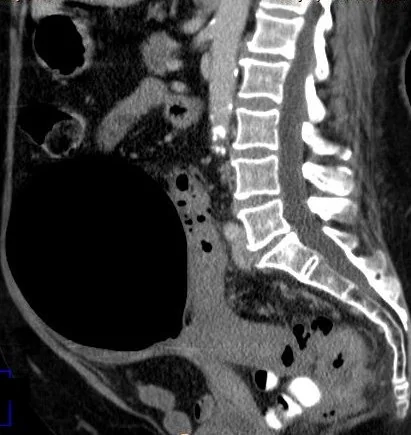
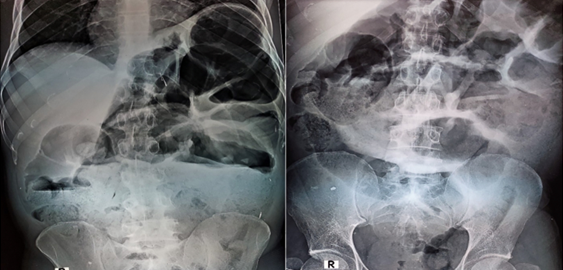
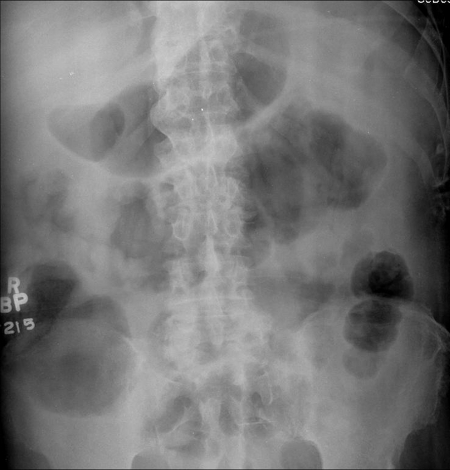
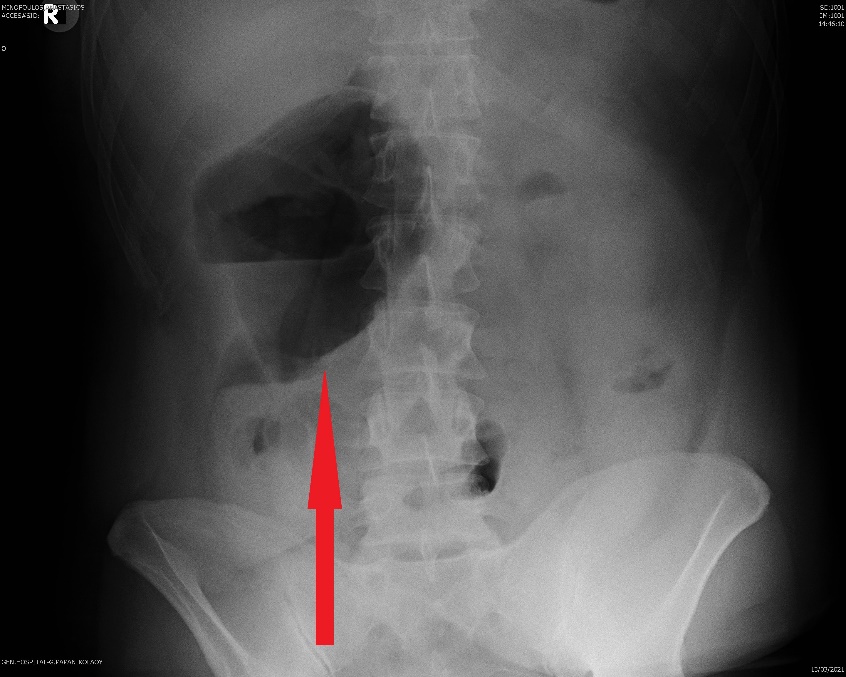
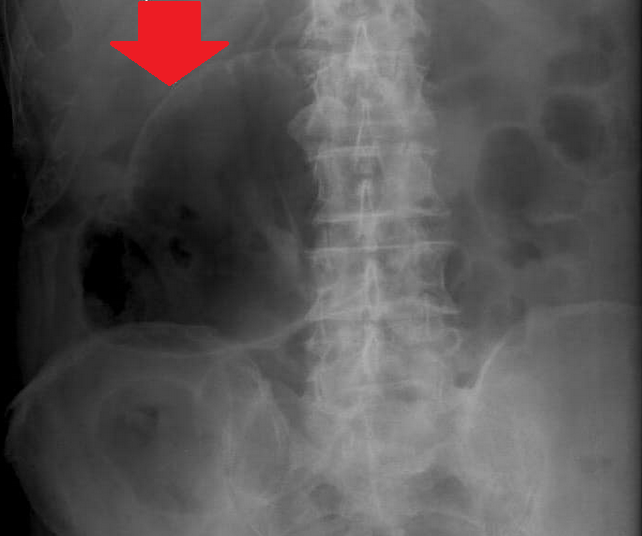
Plain abdominal X-Rays.Pseudo-obstruction of large bowel.(Courtesy Dr. V. Penopoulos)
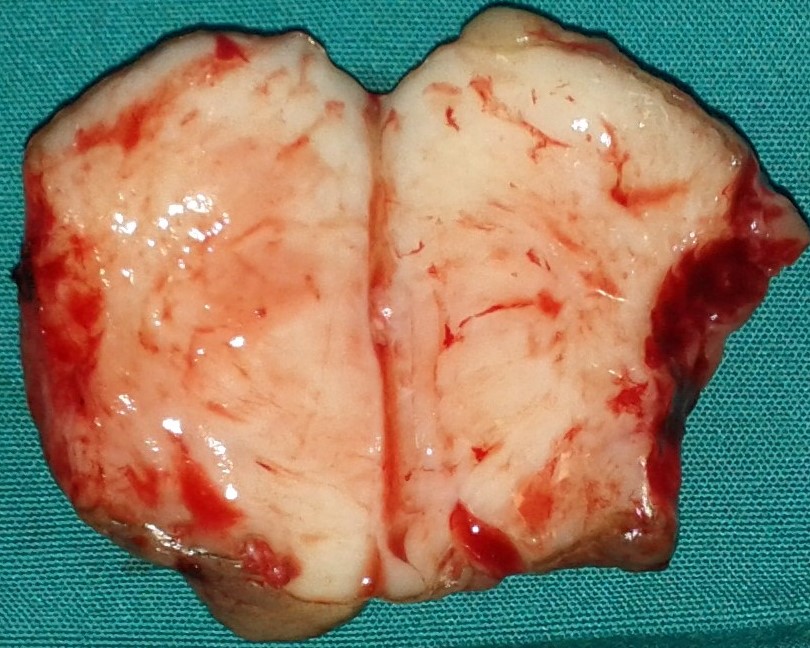
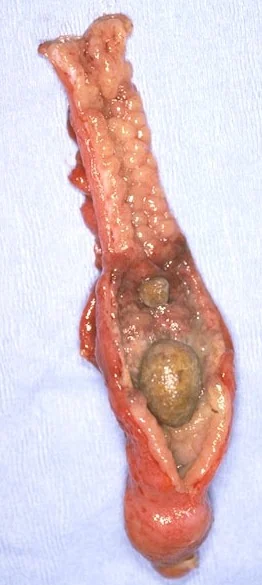
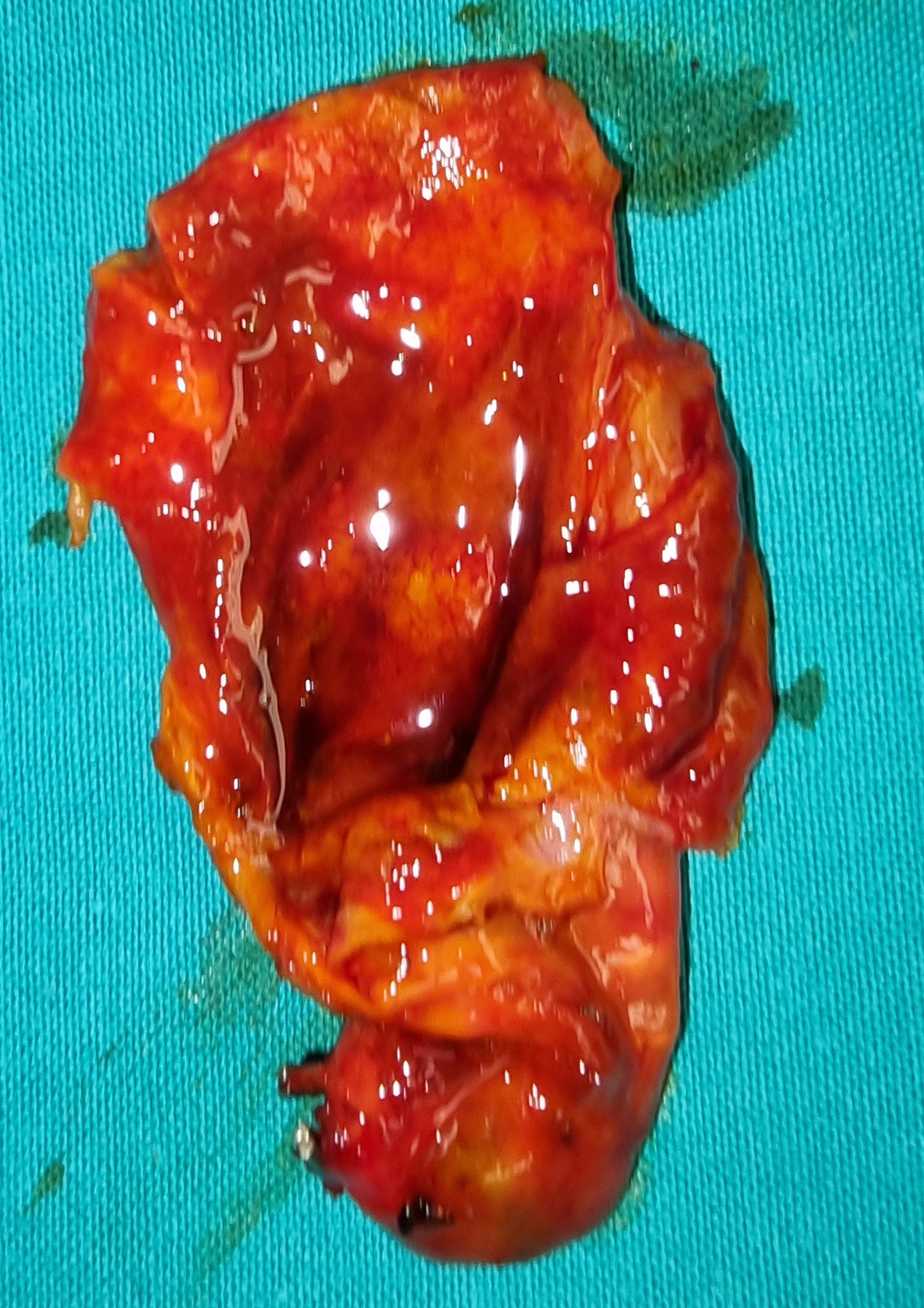
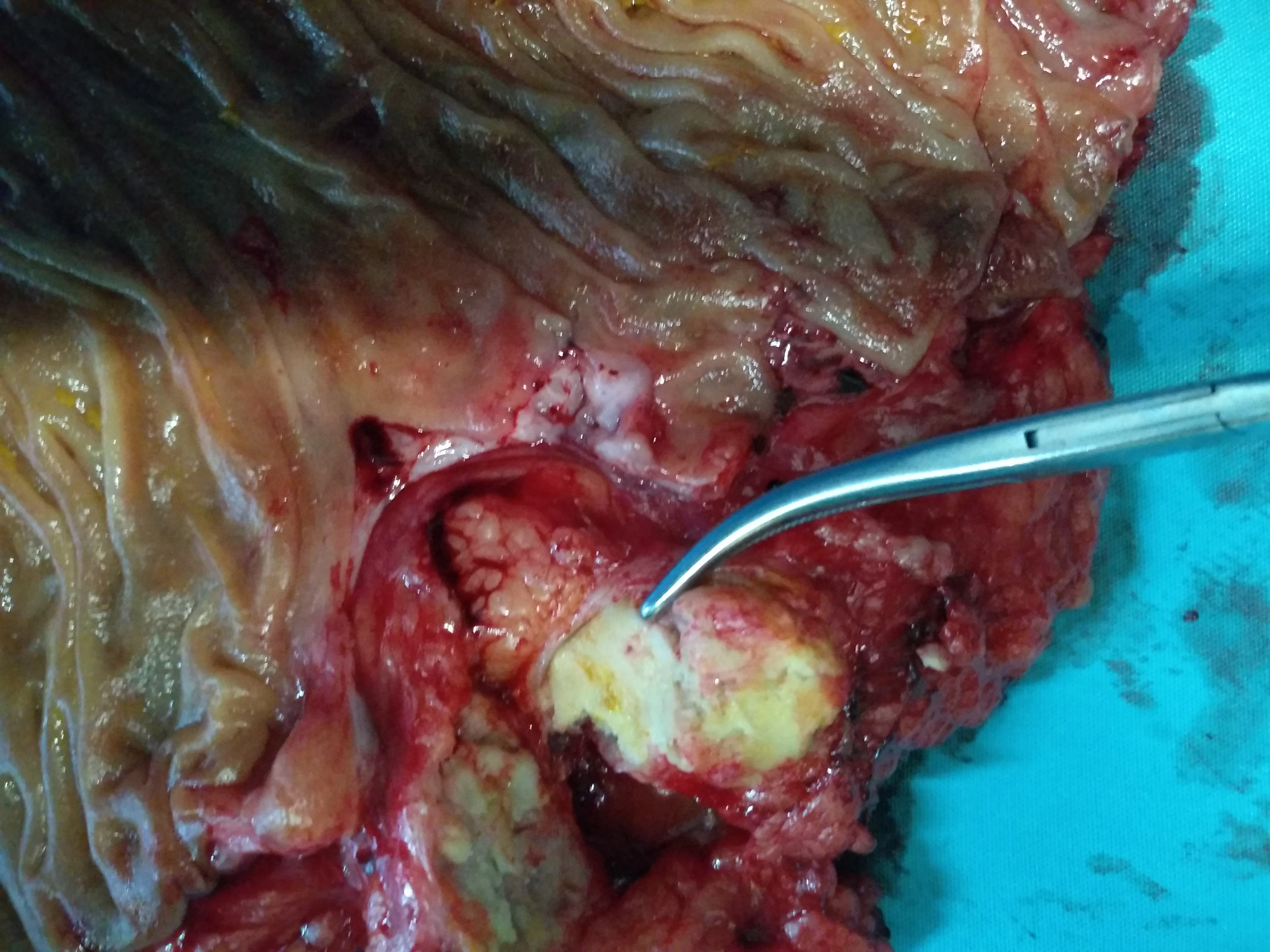
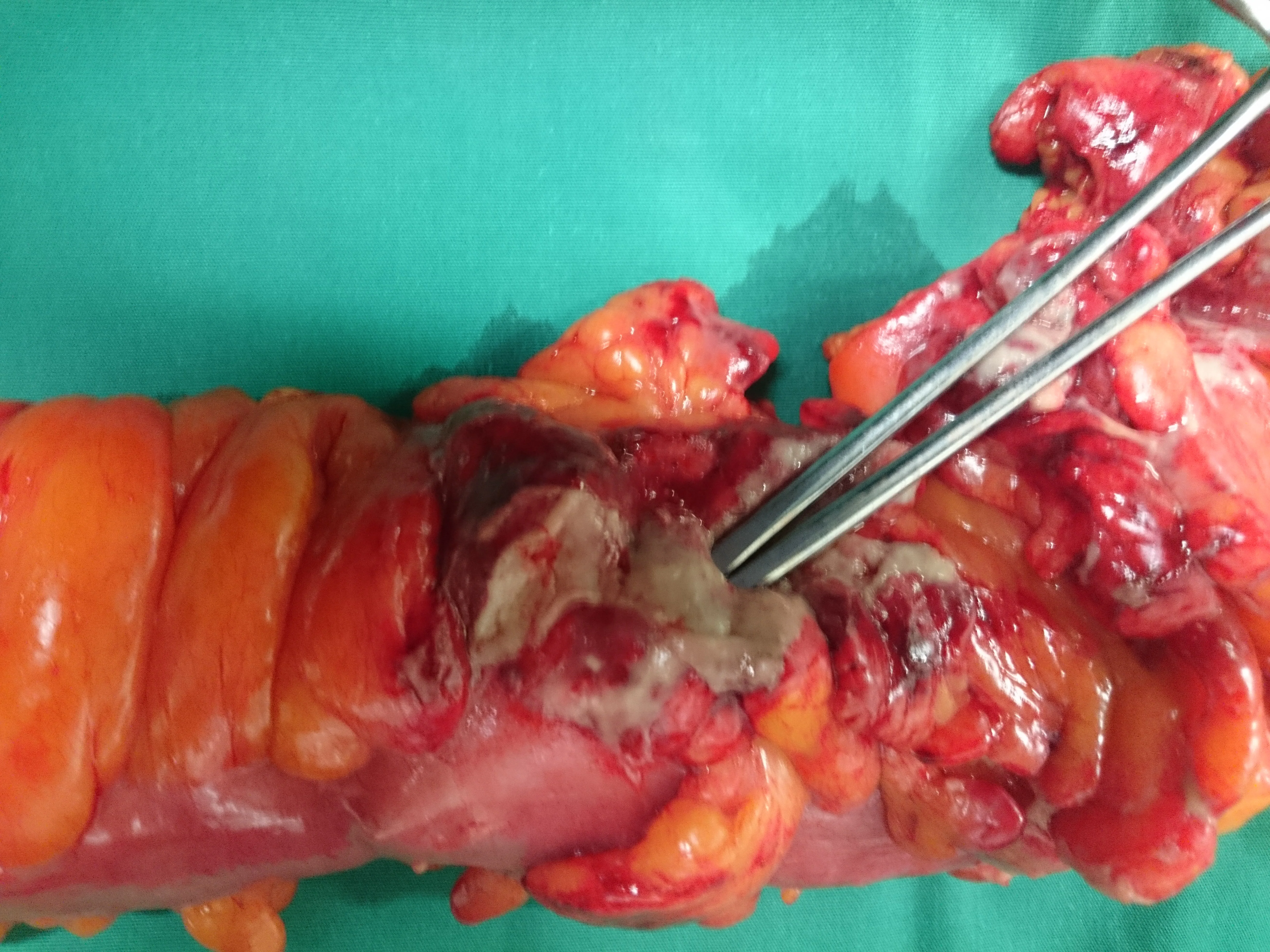
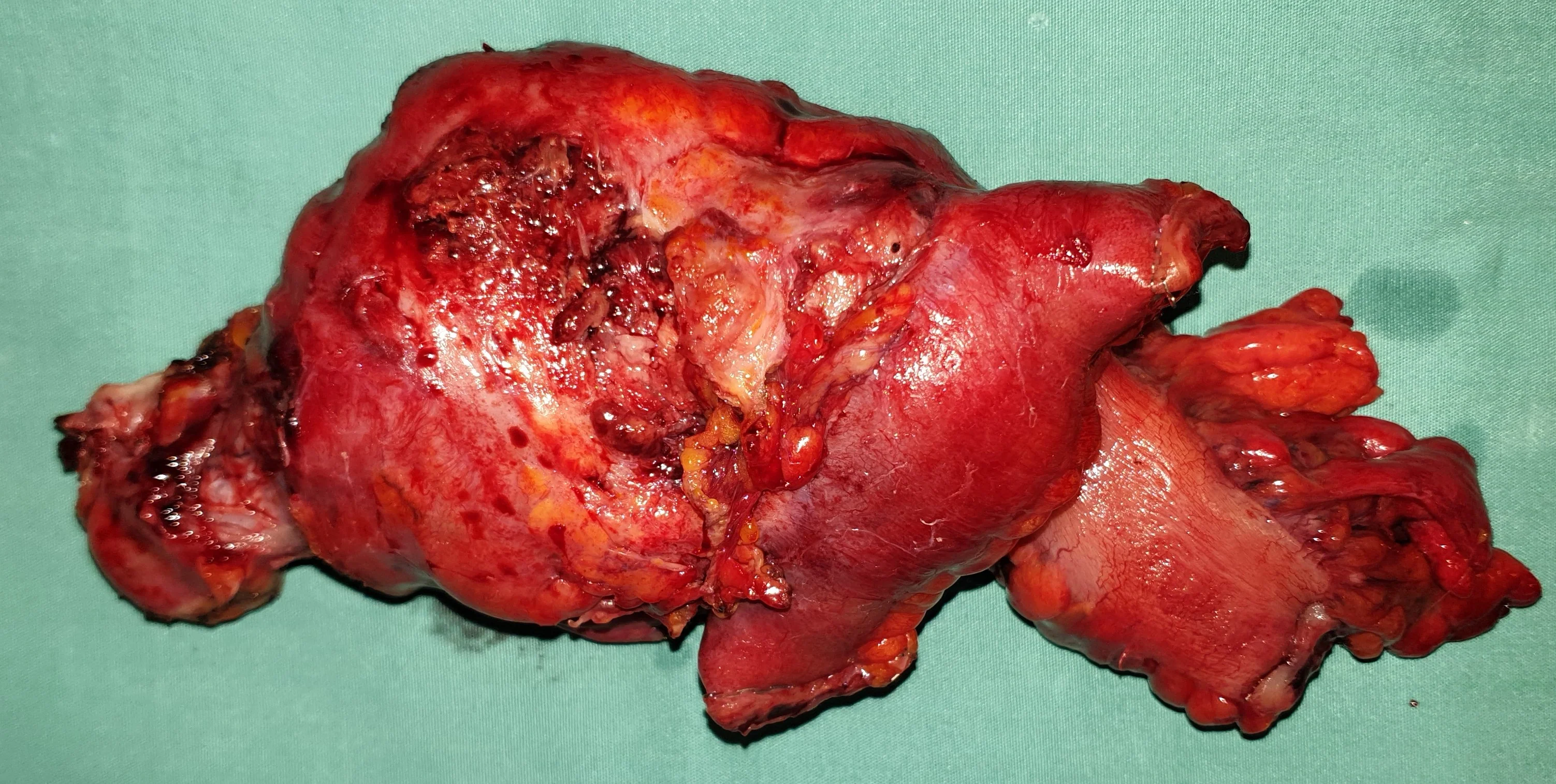
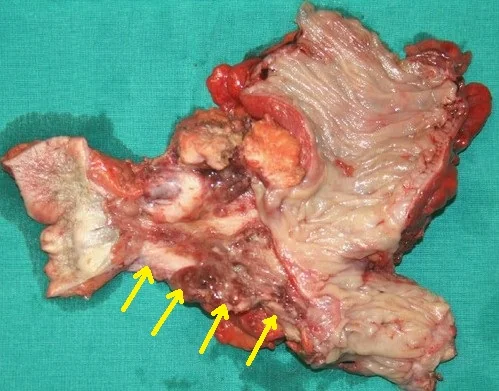
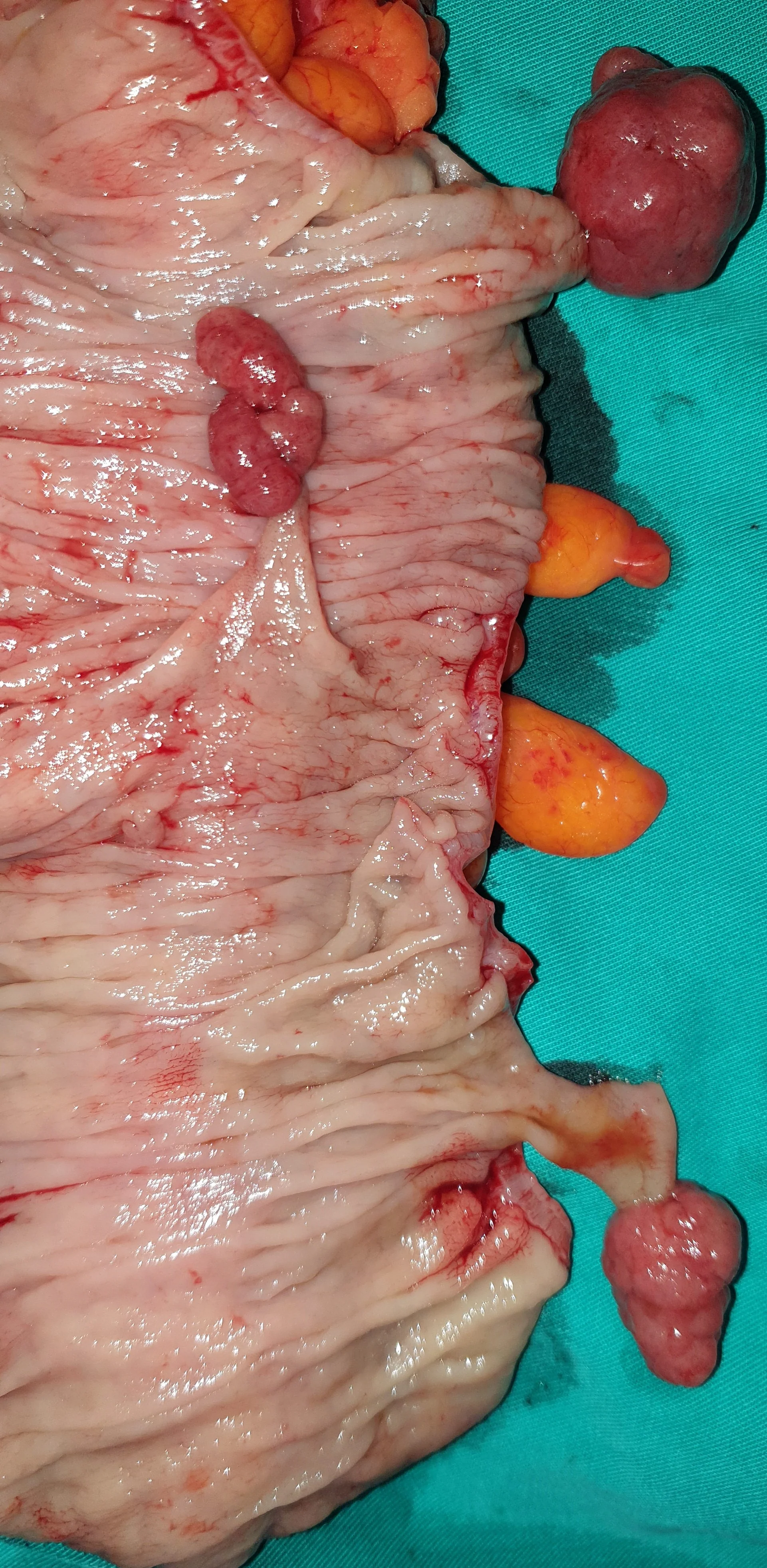
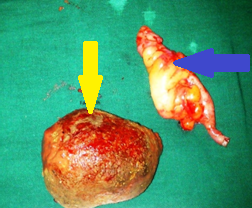
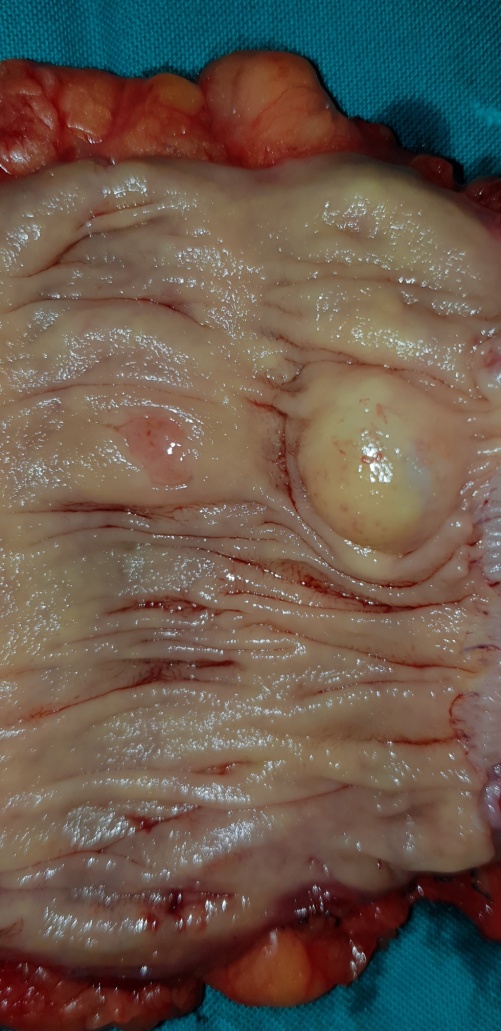
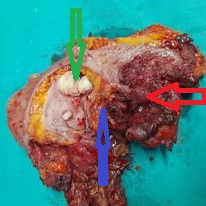
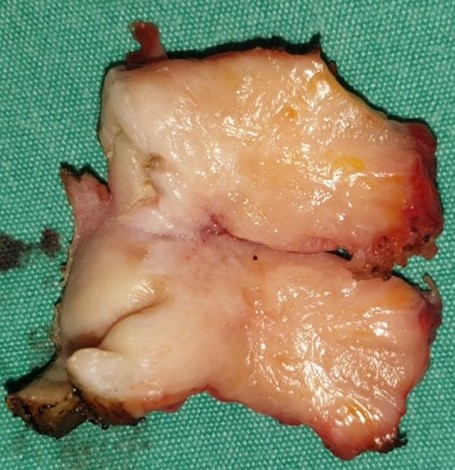
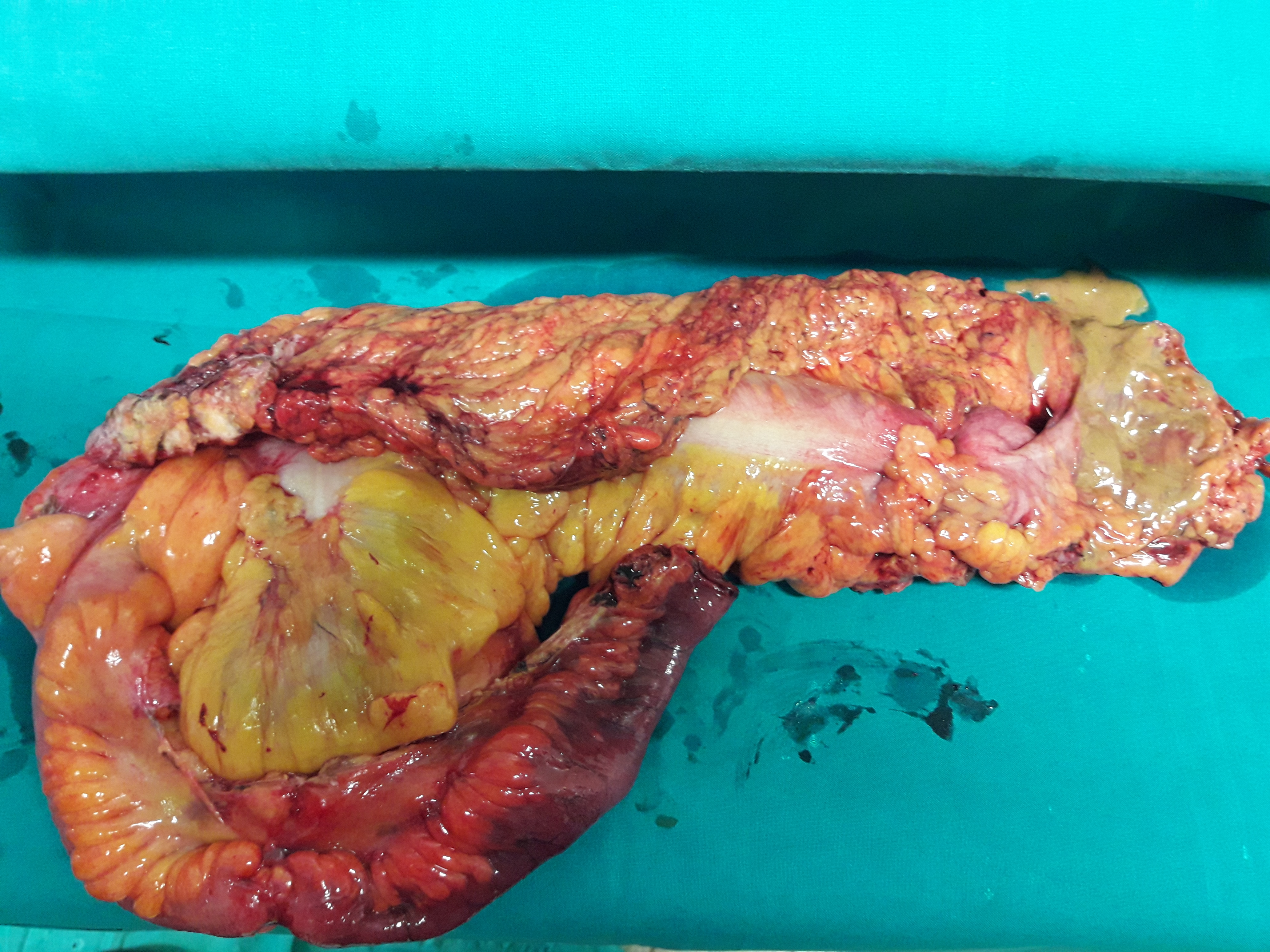
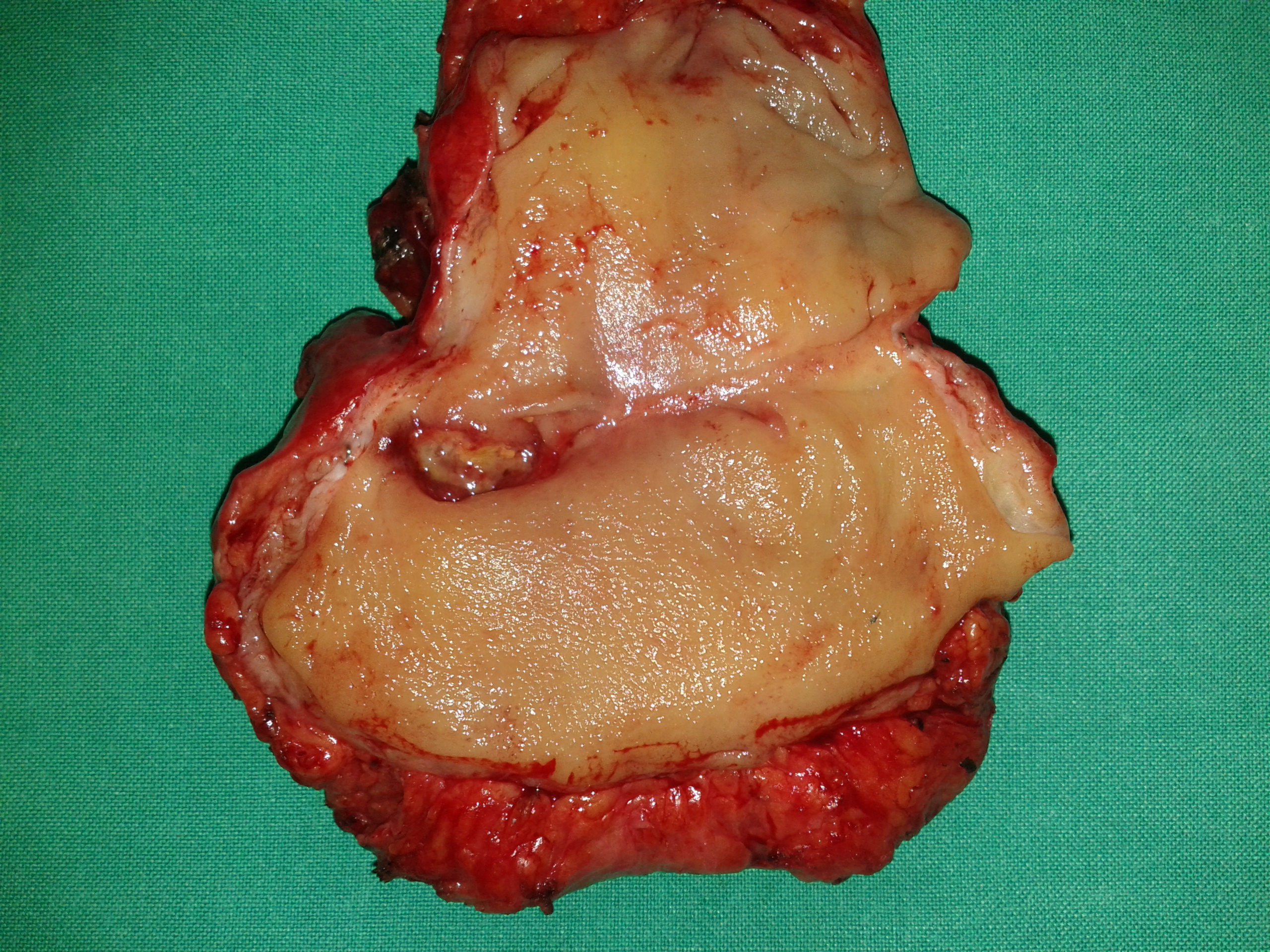
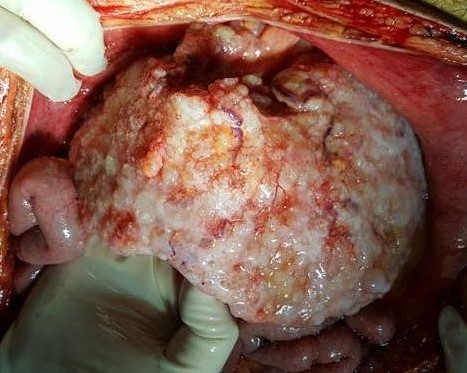
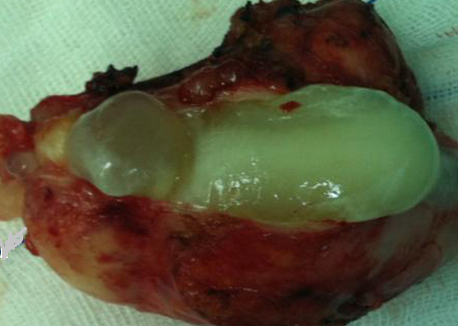
The excised fibroma. A white, homogeneous, fibrous mass is observed (Courtesy Dr. V. Penopoulos)

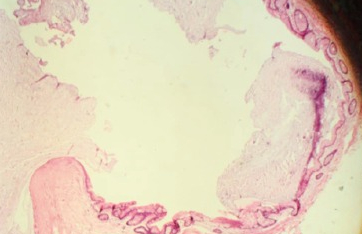
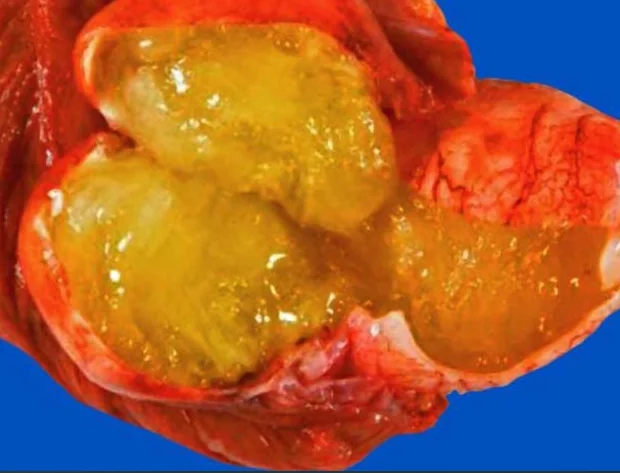
Cyst containing condensed mucus, lined with benign colonic epithelium, surrounded by fibrosis (Courtesy Dr. V. Penopoulos)




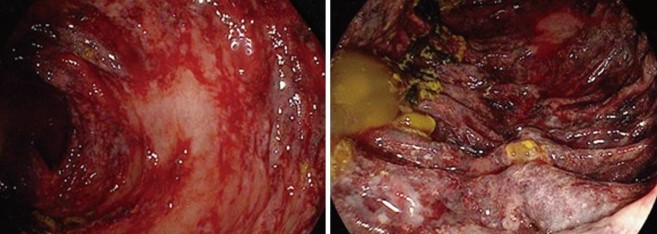
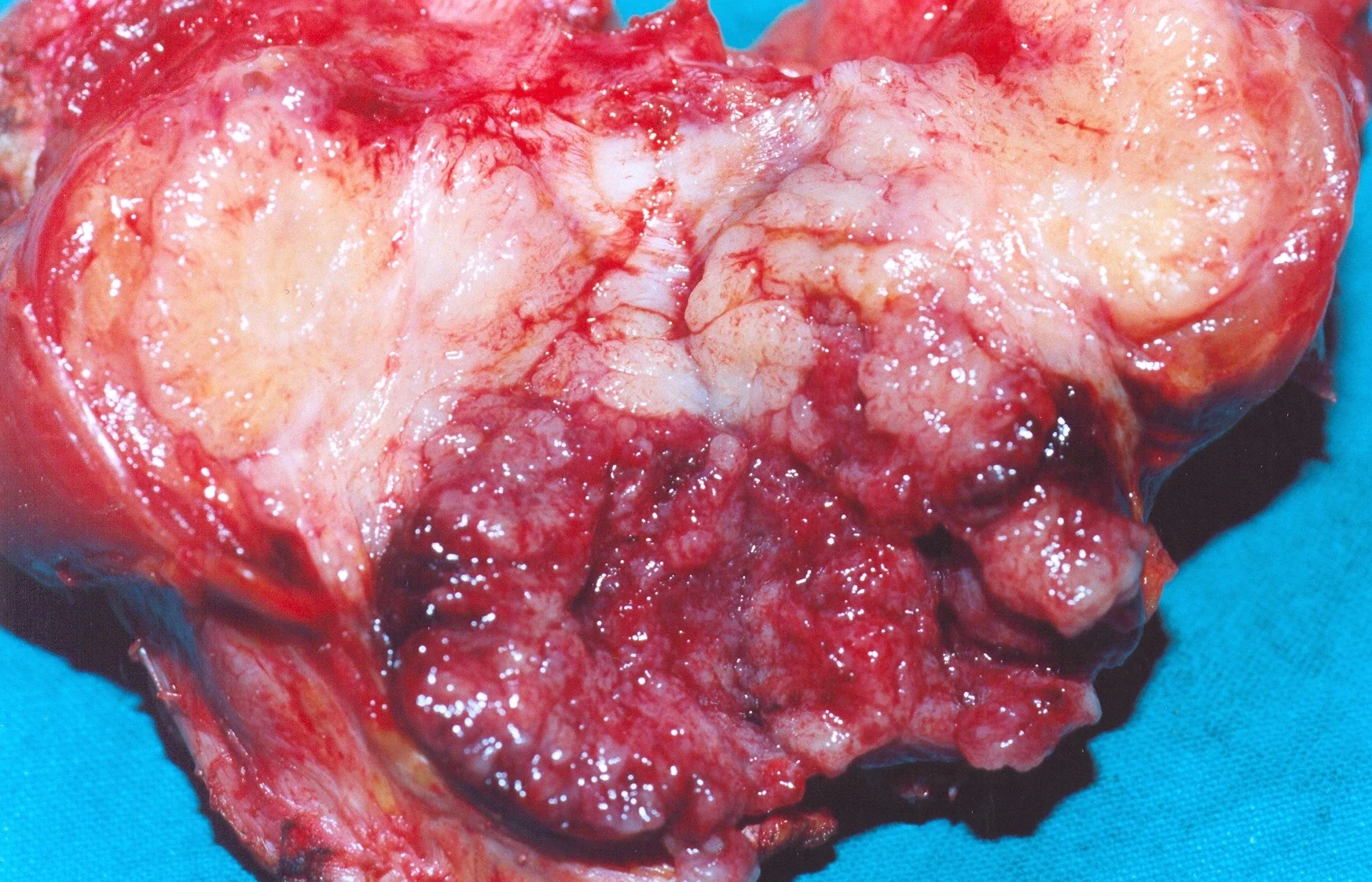
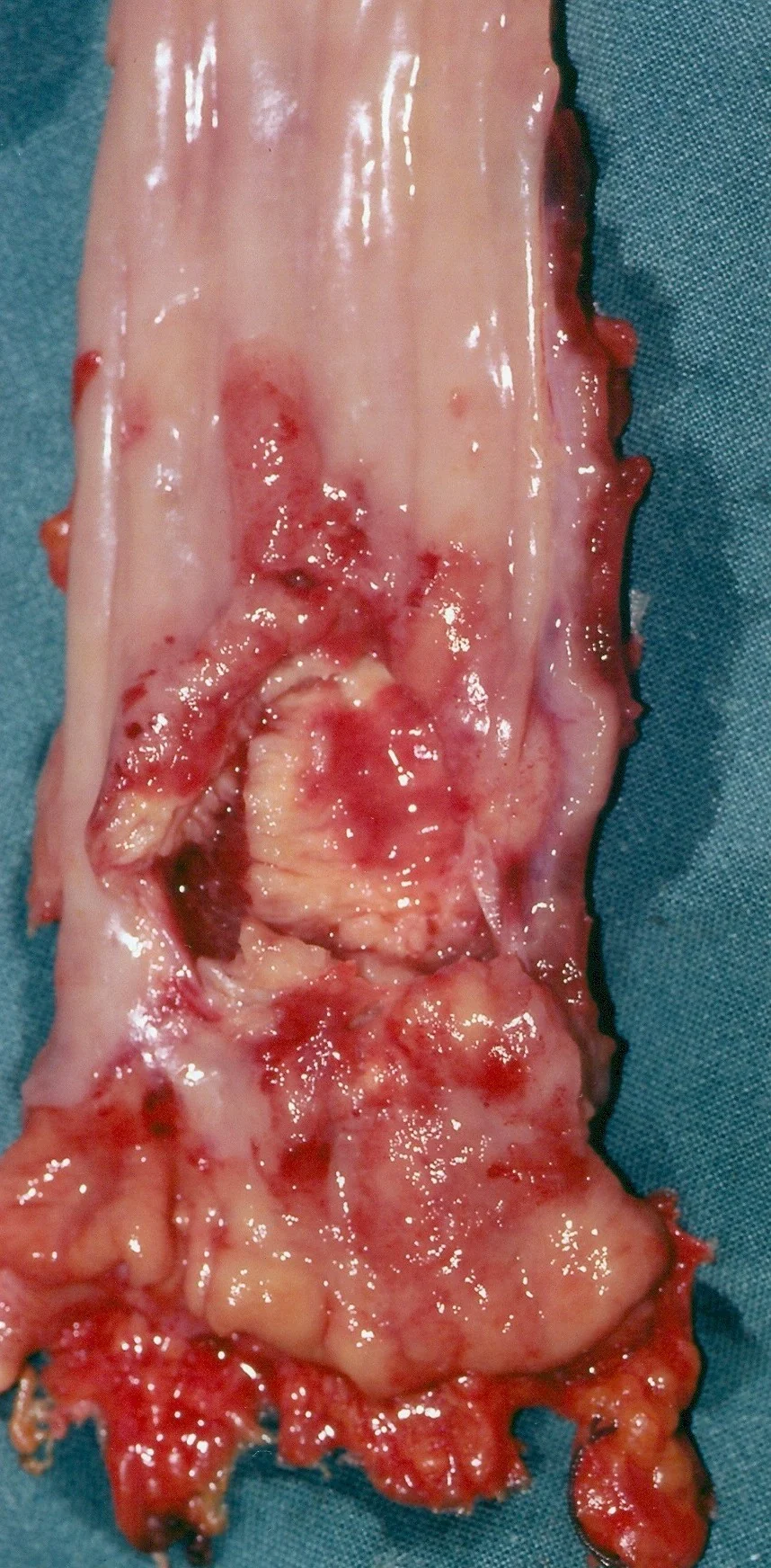
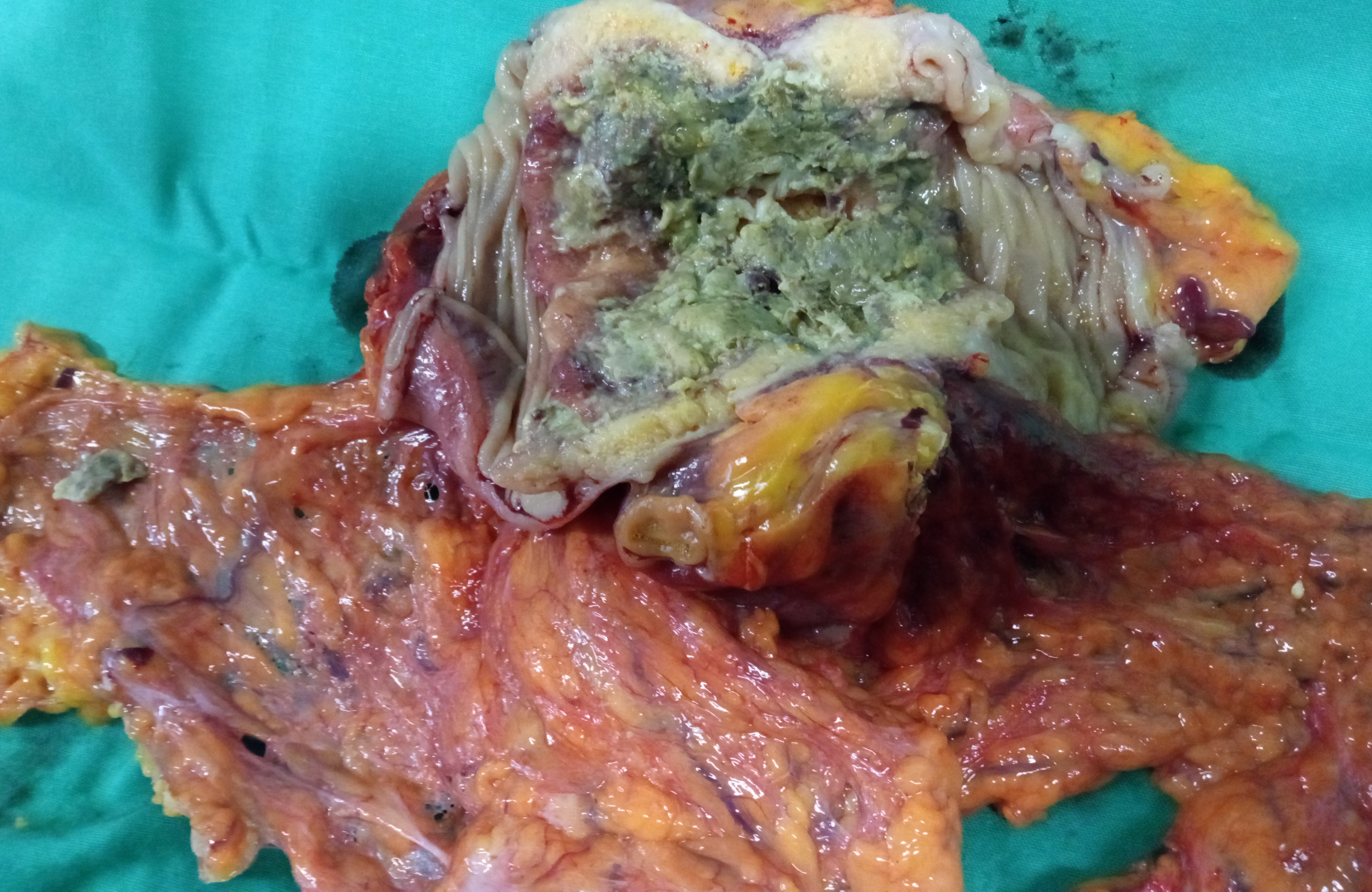
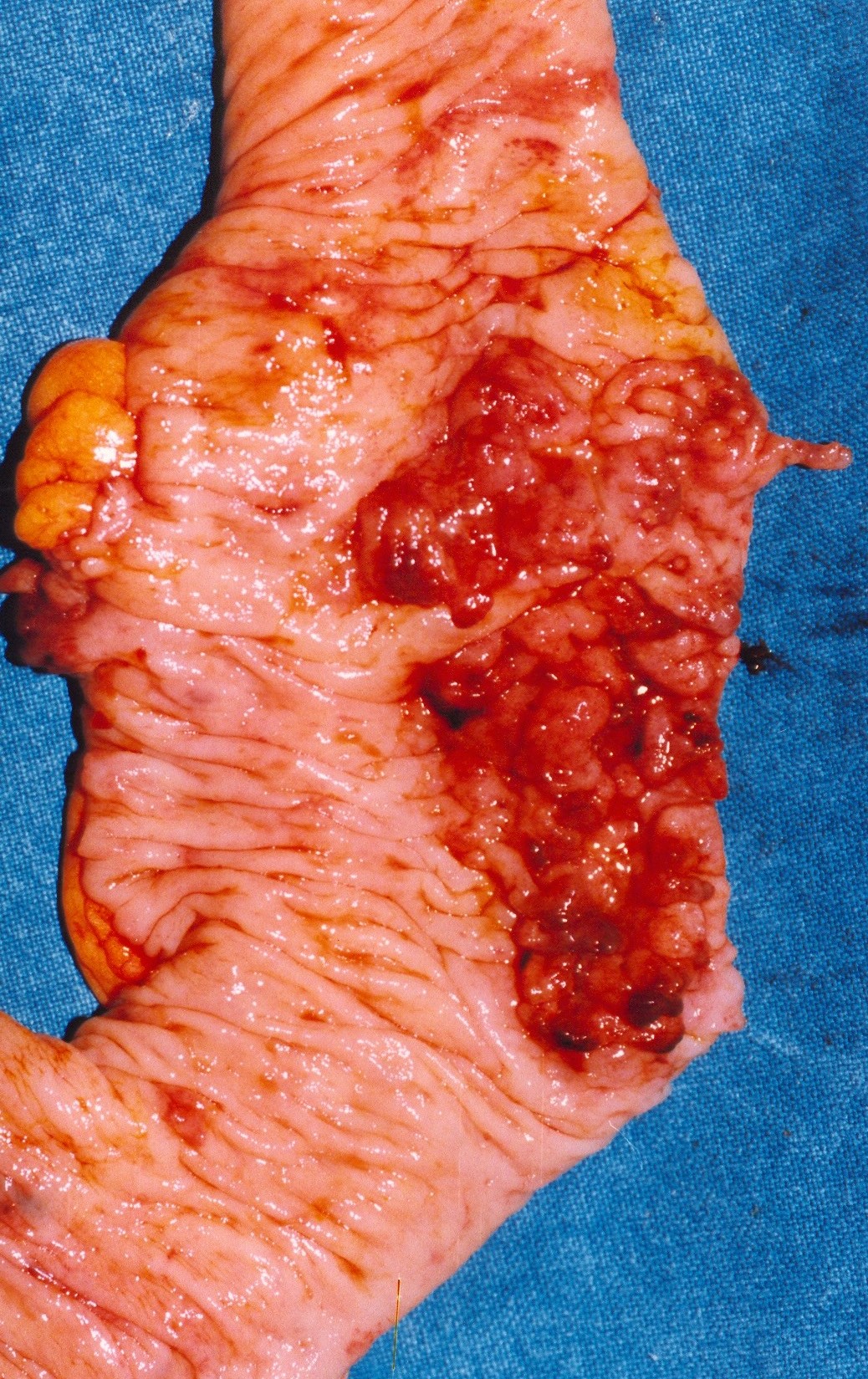
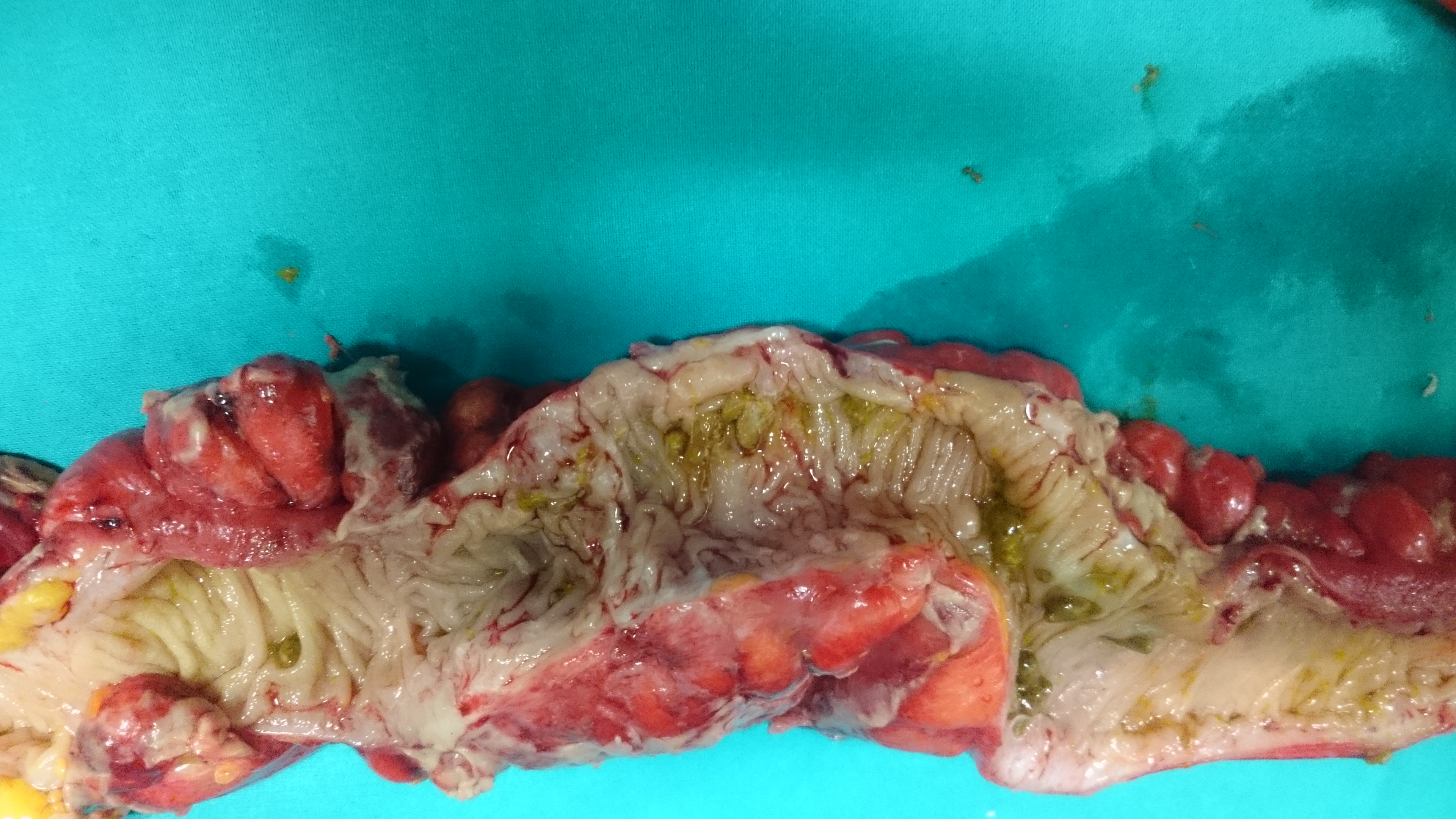
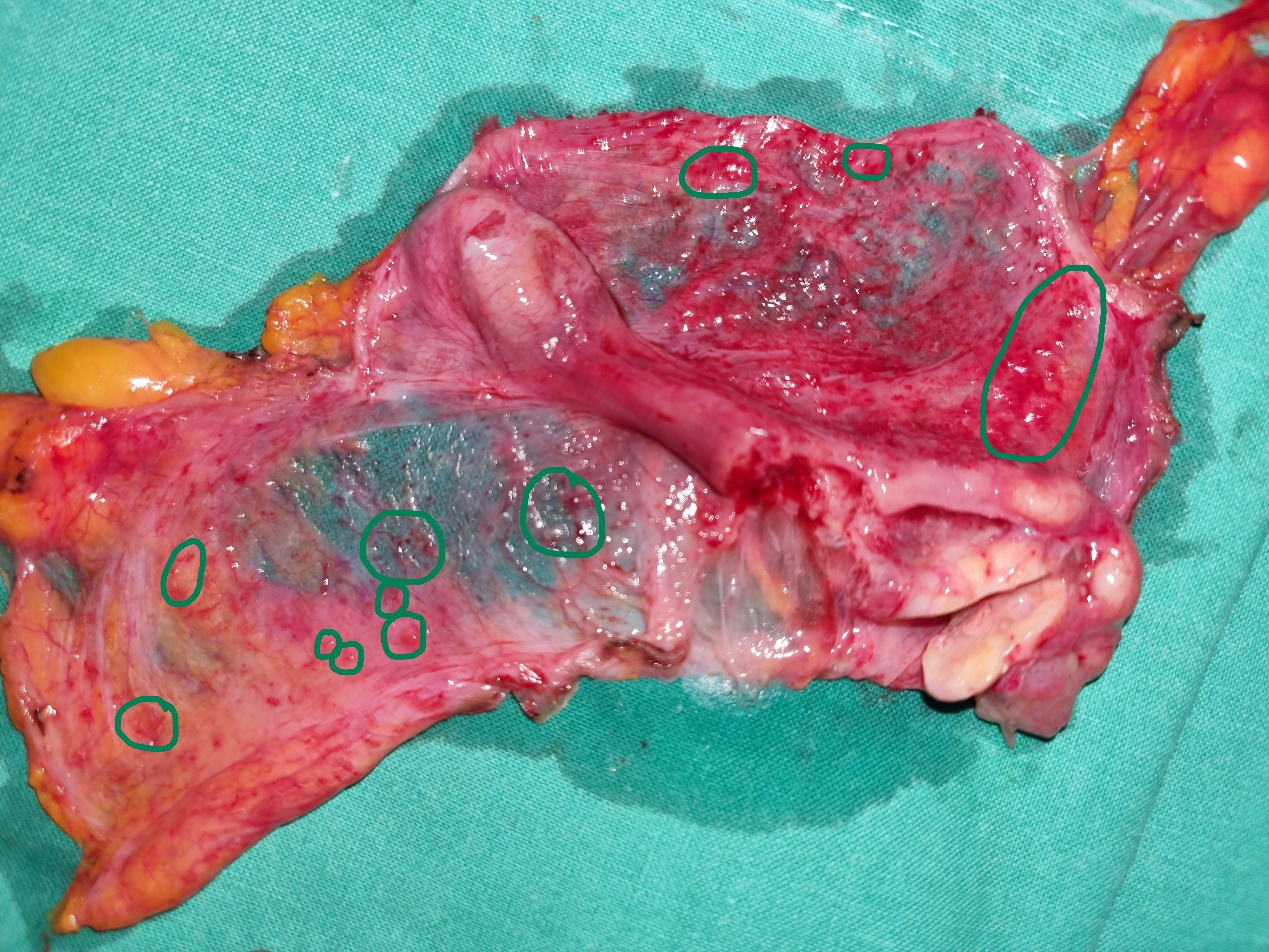
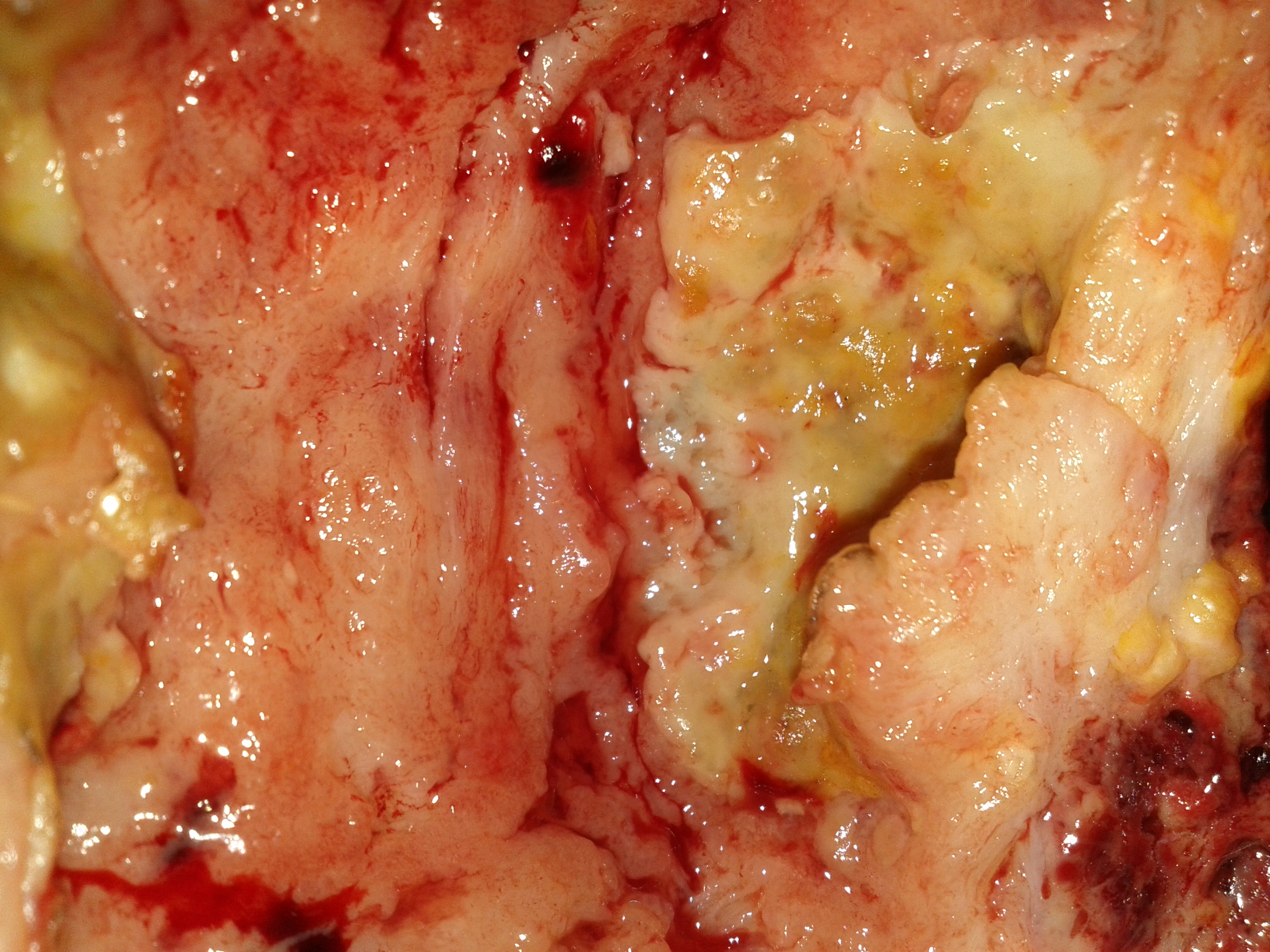
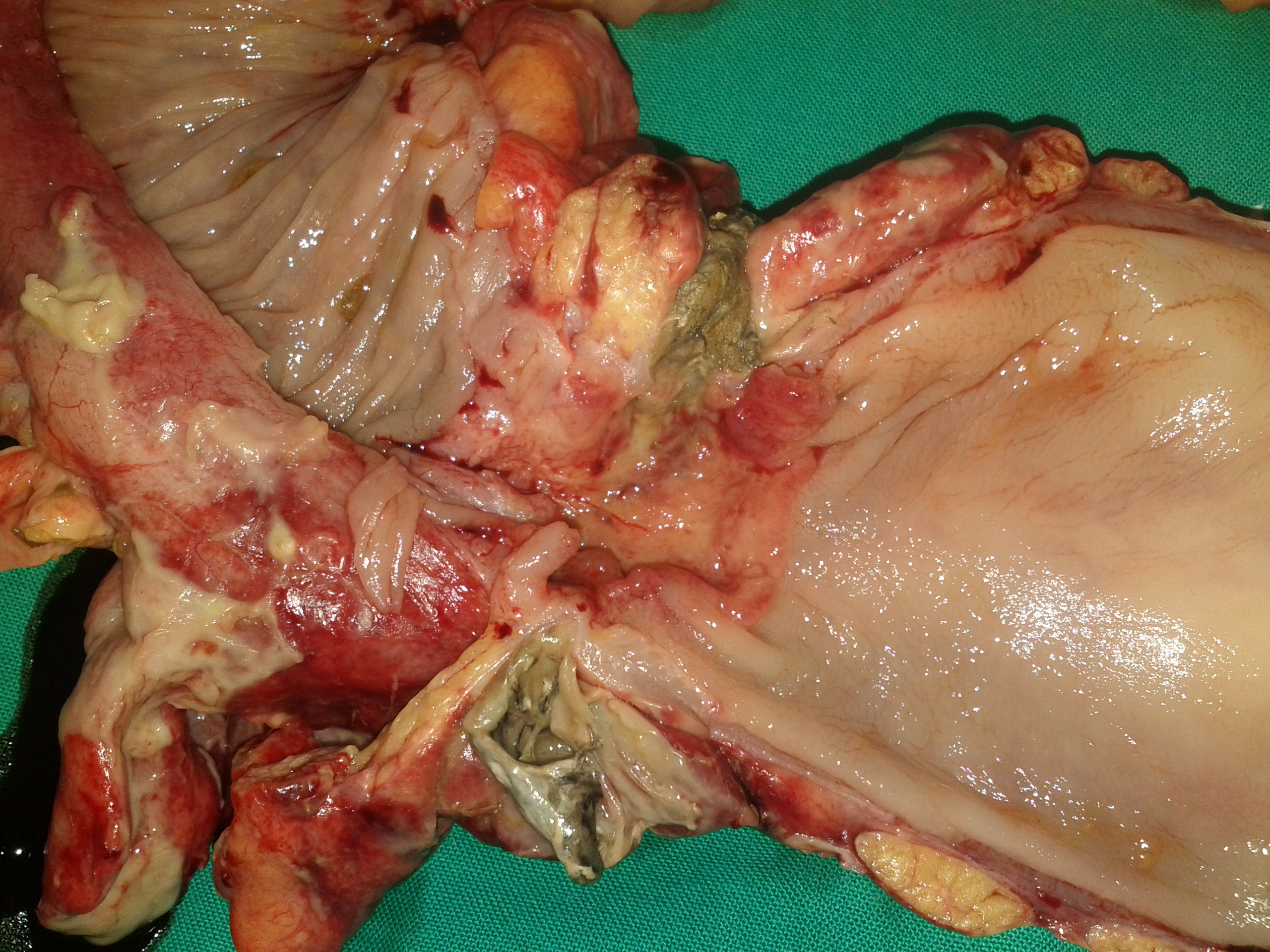
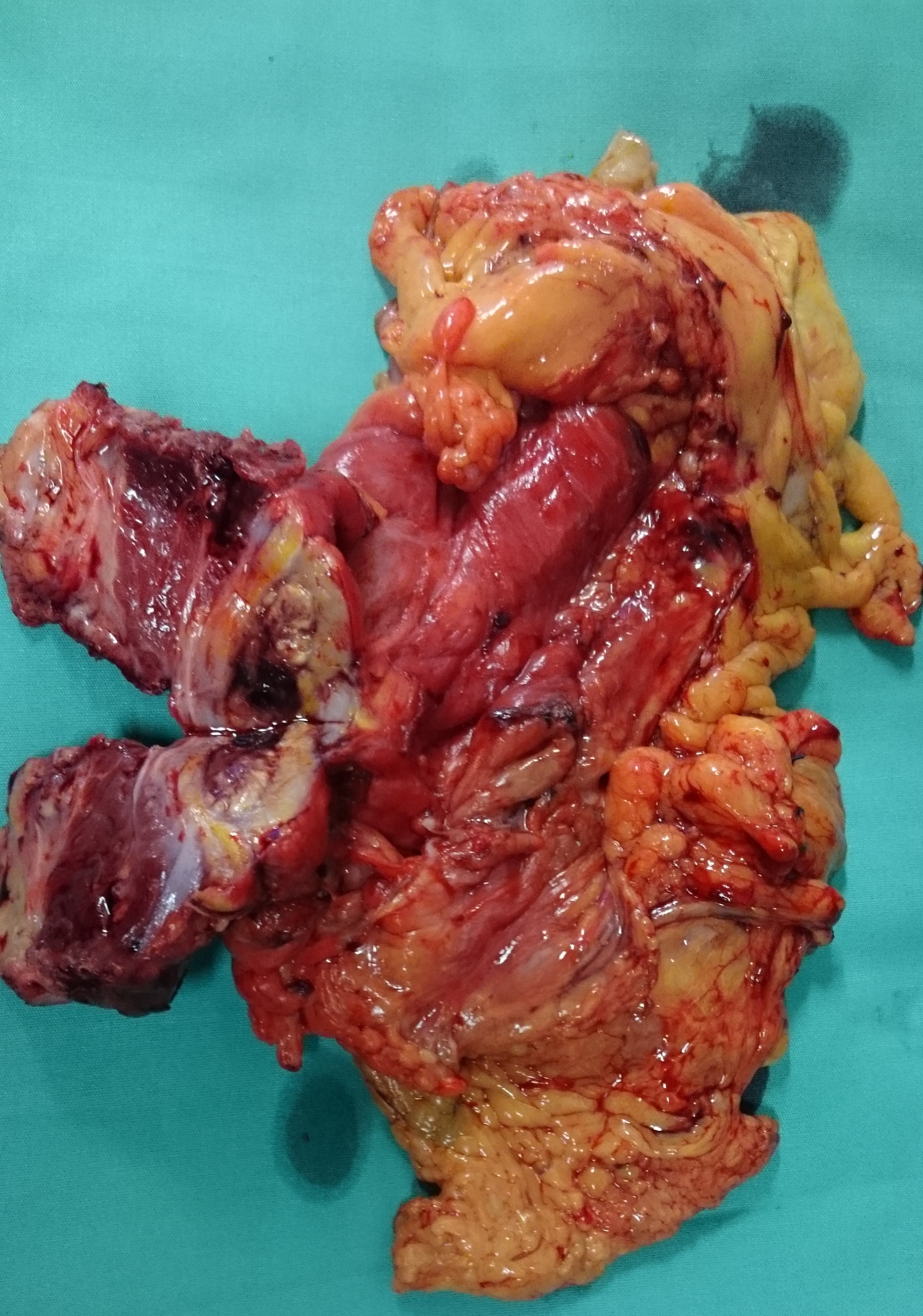
Non Obstructive Ischaemic Colitis .Macroscopic view part of the specimen.(Courtesy Dr. V. Penopoulos)
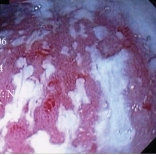
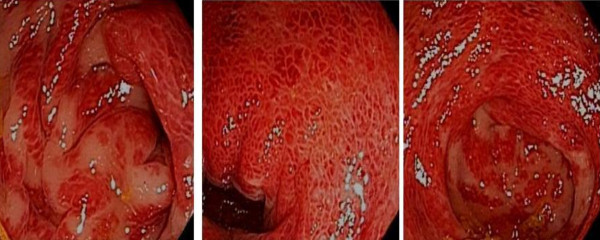
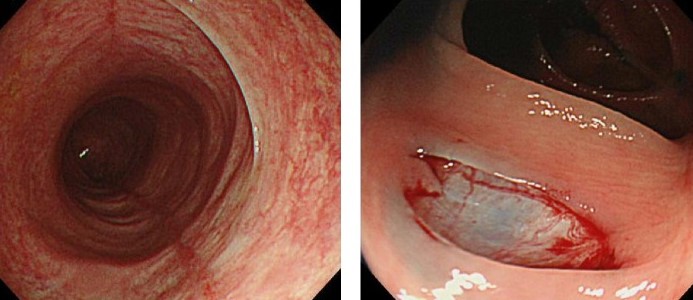
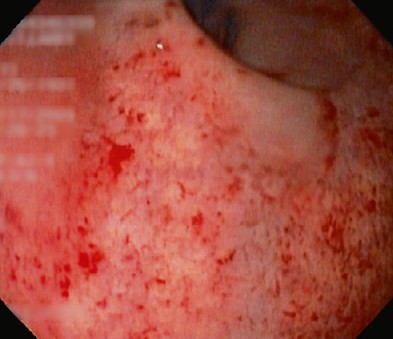
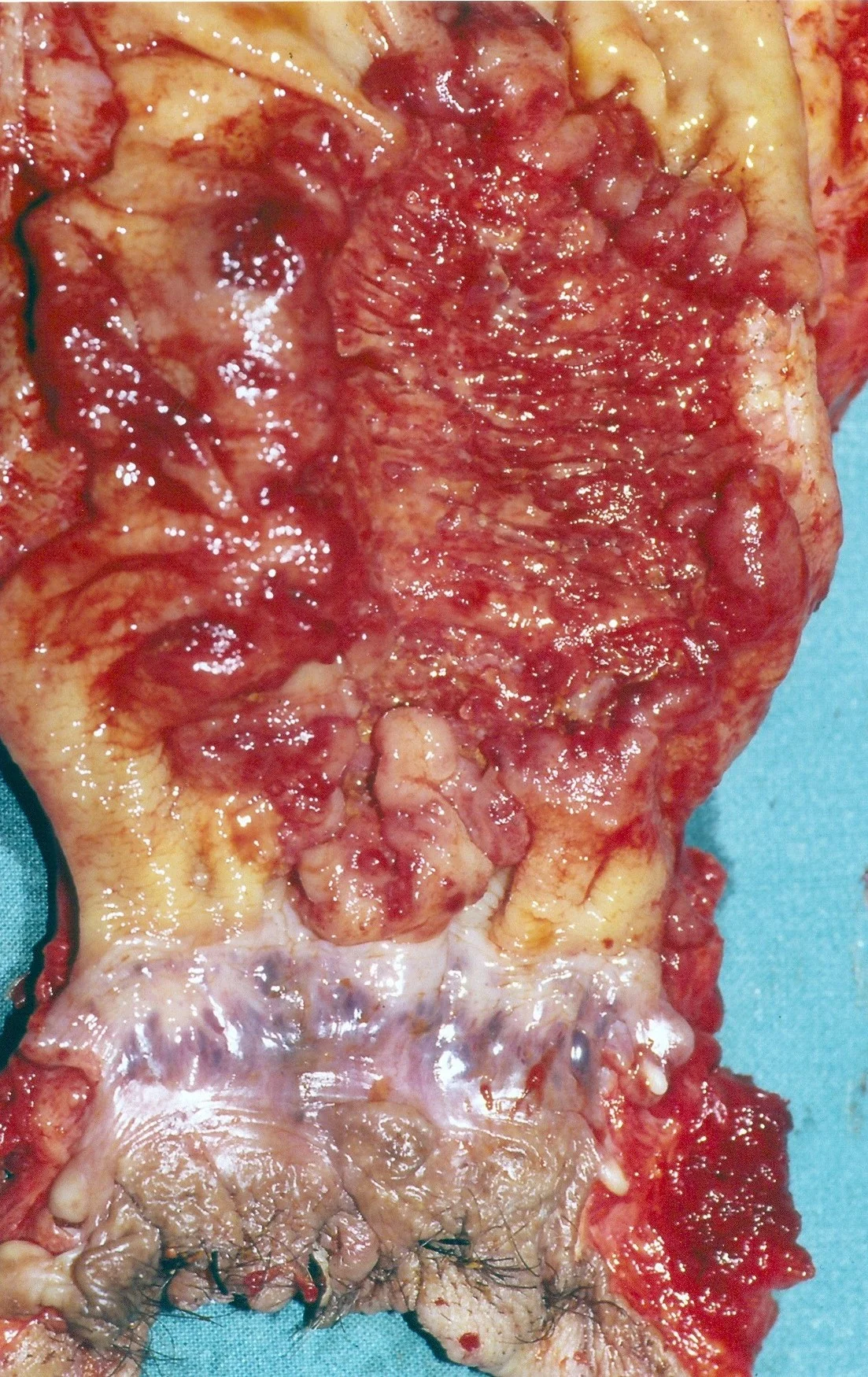
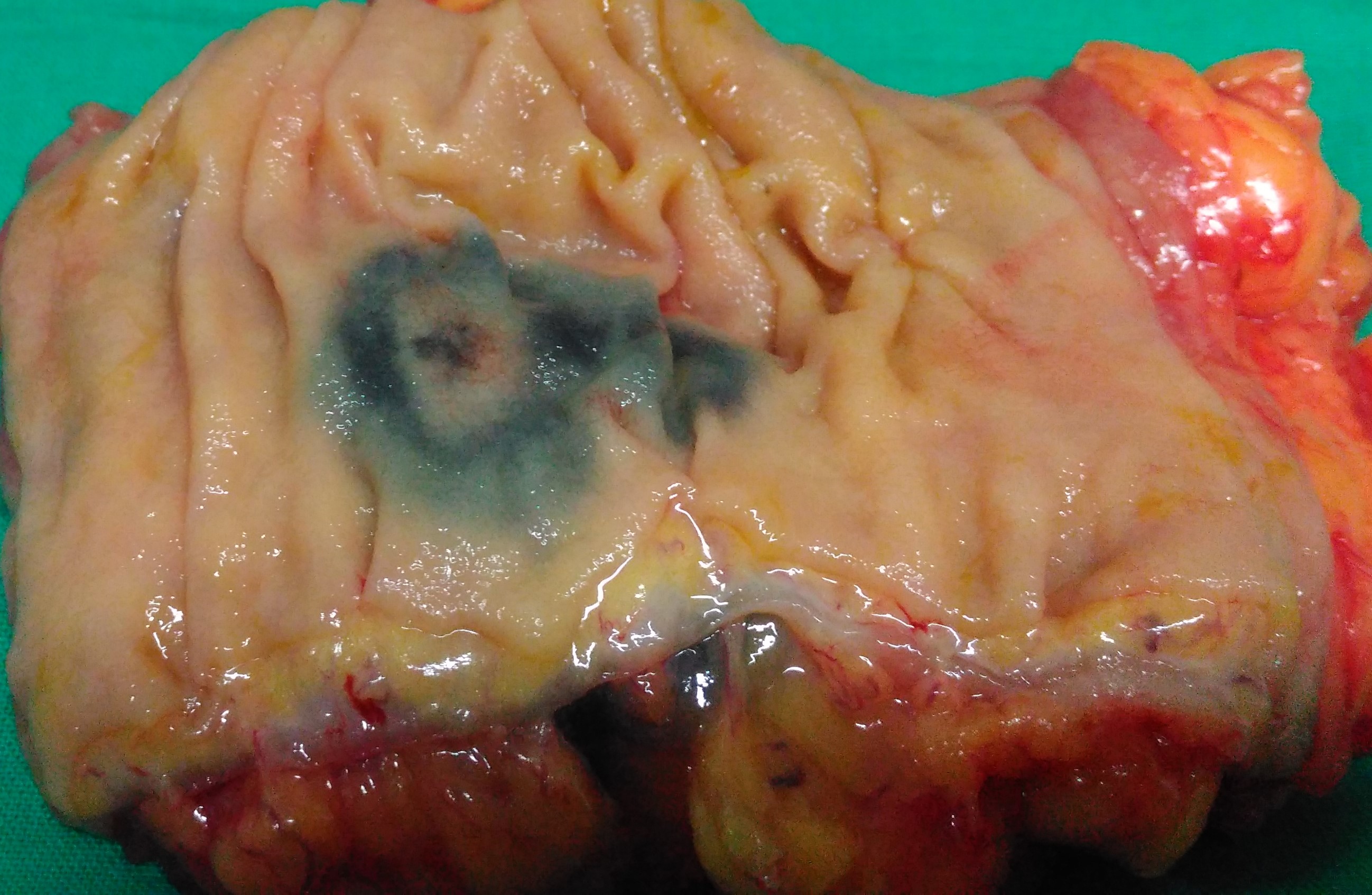
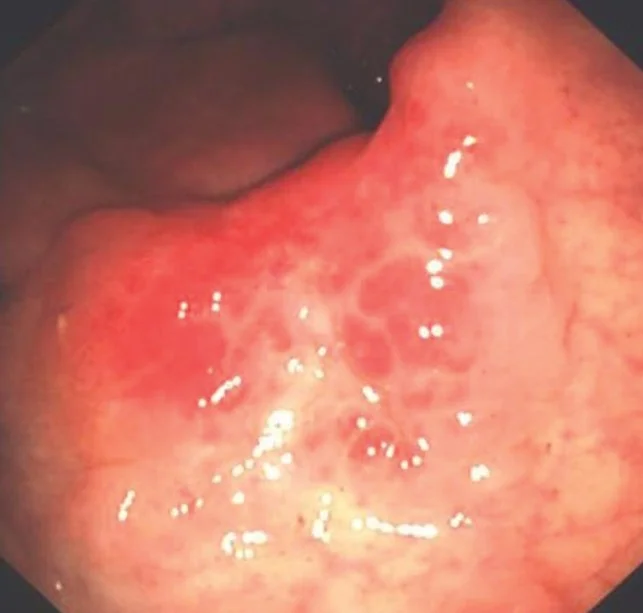
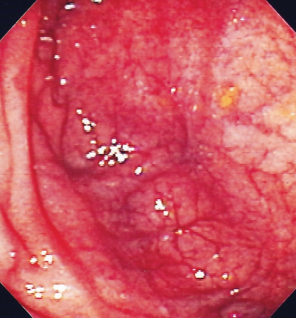
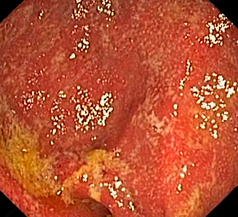
Indeterminate Colitis - Characteristic lesions of the descending colon (Courtesy Dr. V. Penopoulos)
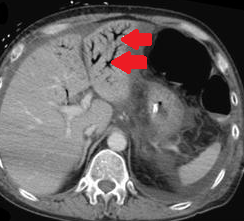
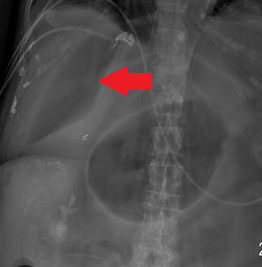
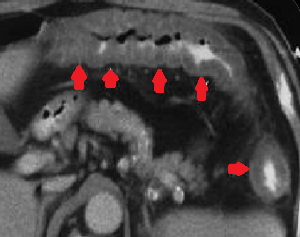
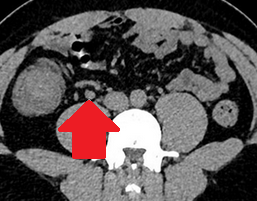
Presence of air in the portal venous system, secondary to ischemic colitis.(Courtesy Dr. V. Penopoulos).


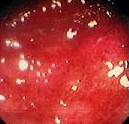
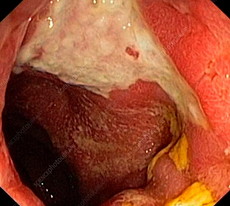
Details of the extensive lesions in the transverse colon.(Courtesy Dr. V. Penopoulos).
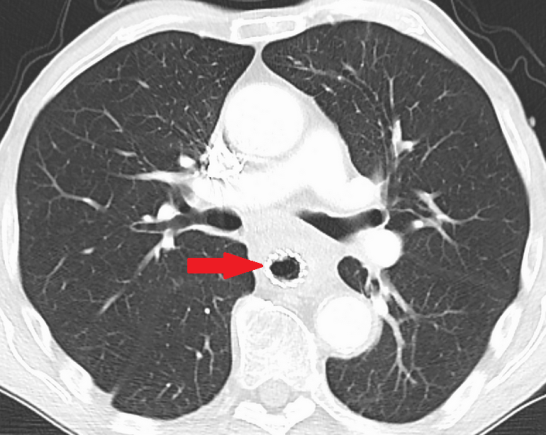
Chest CT Scan-Thirty days following esophageal stent placement-Stent in the right place.(Courtesy Dr. V. Penopoulos).
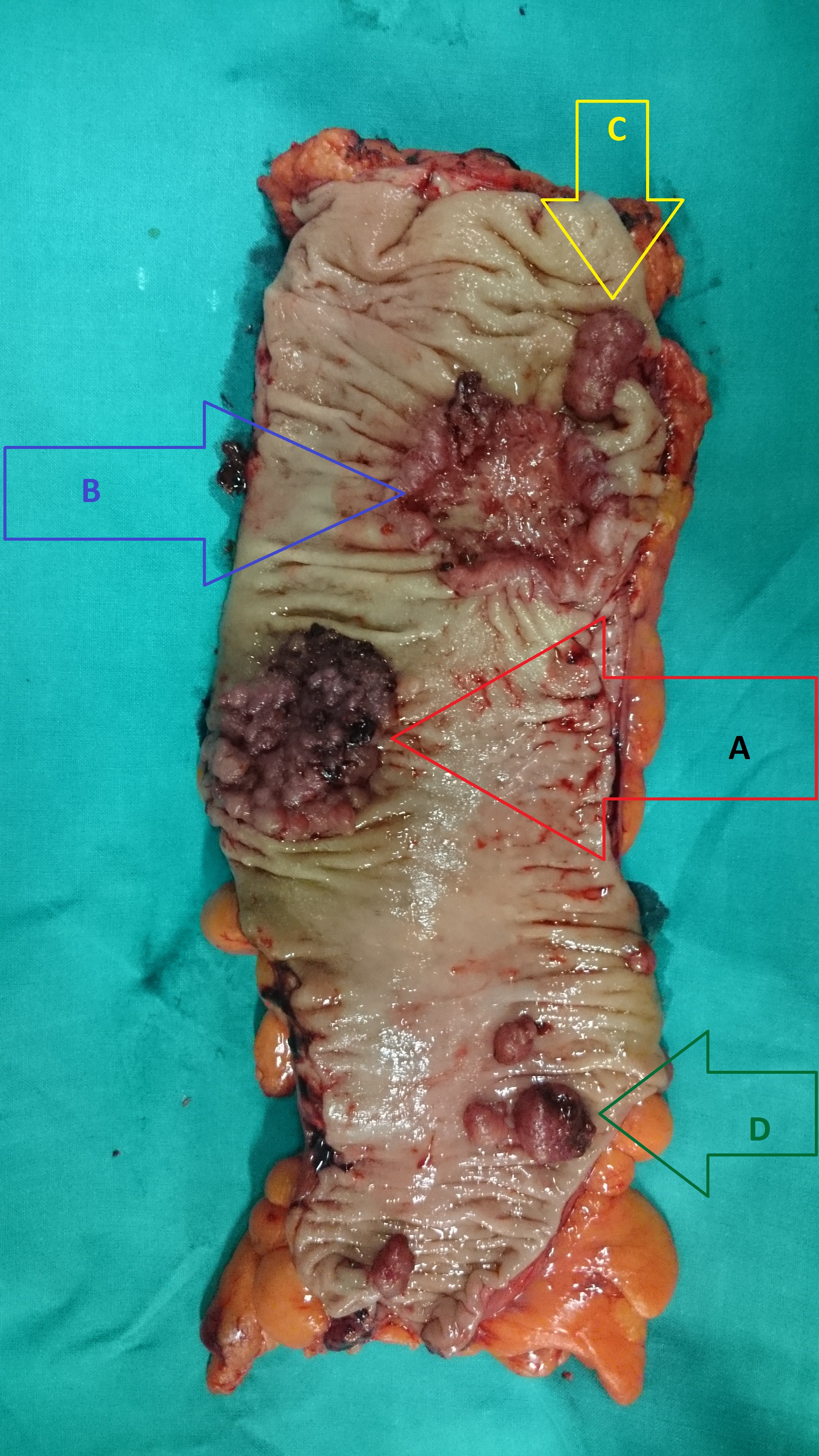
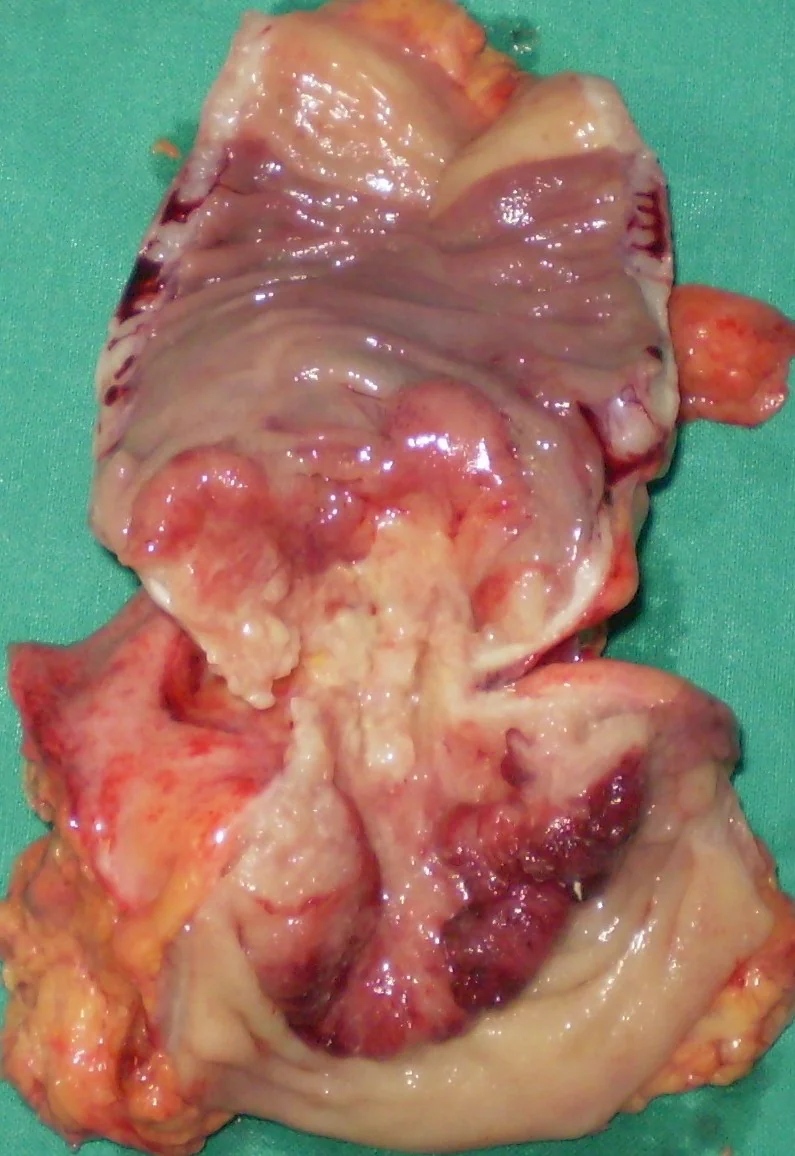
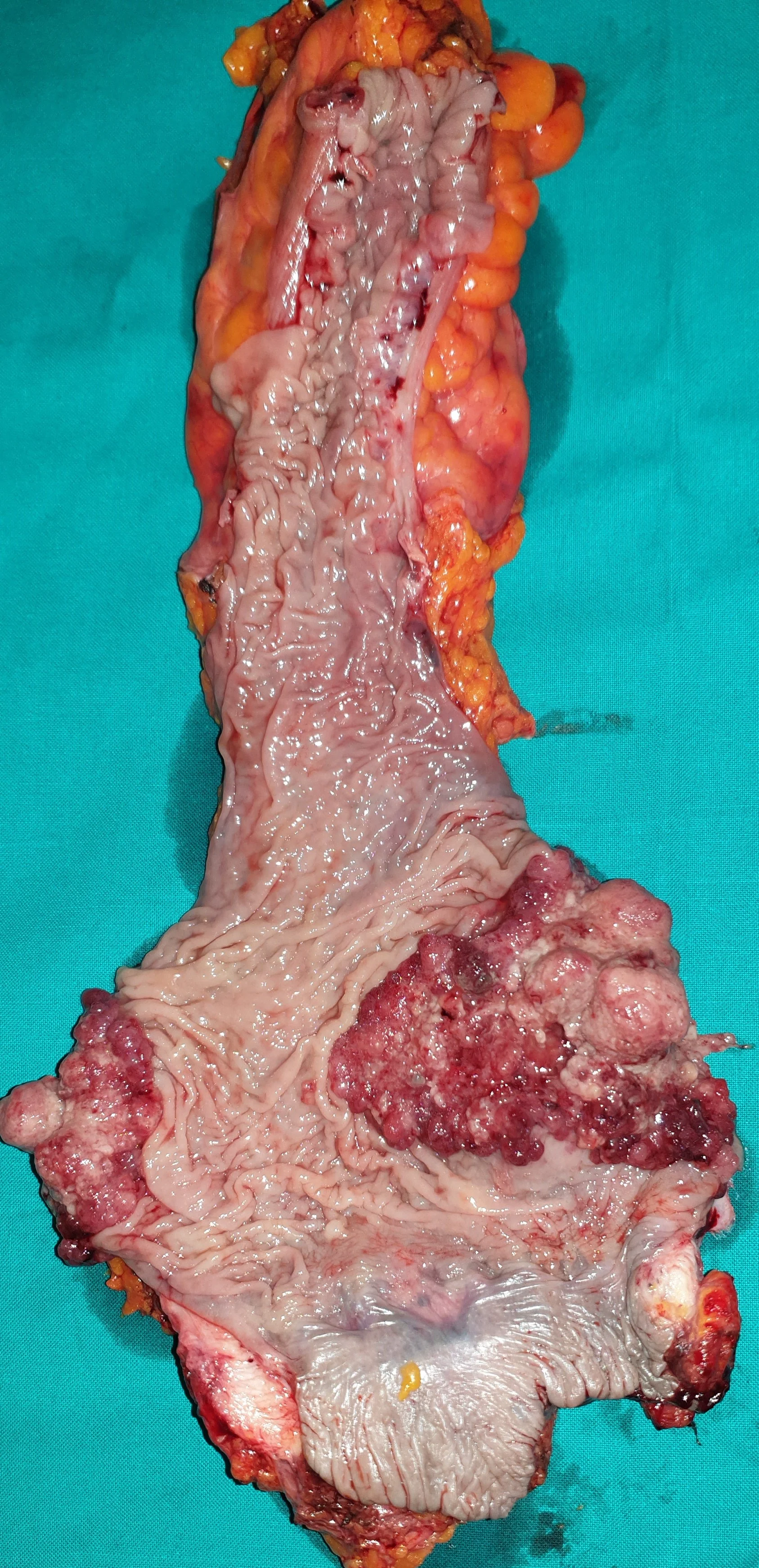
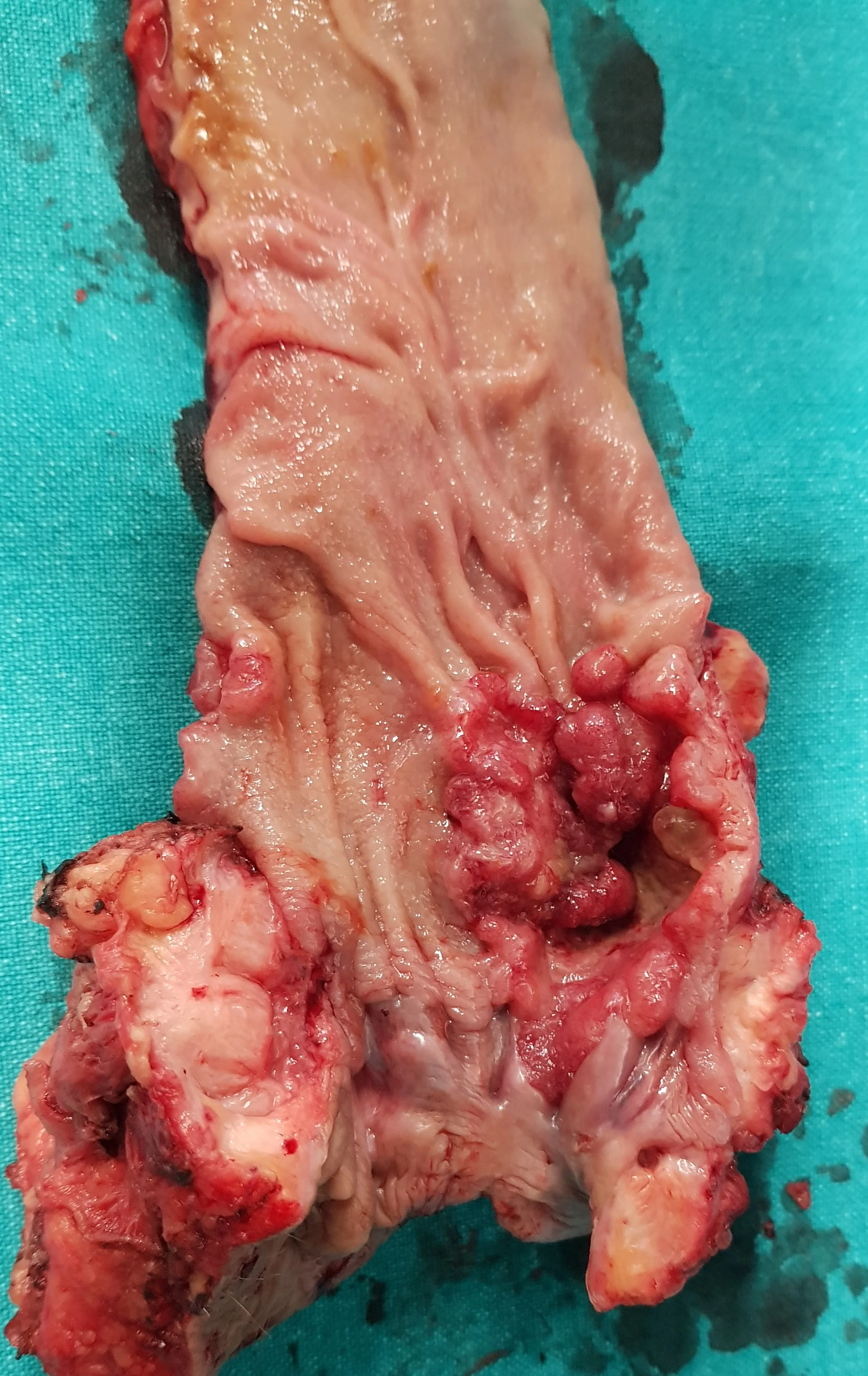
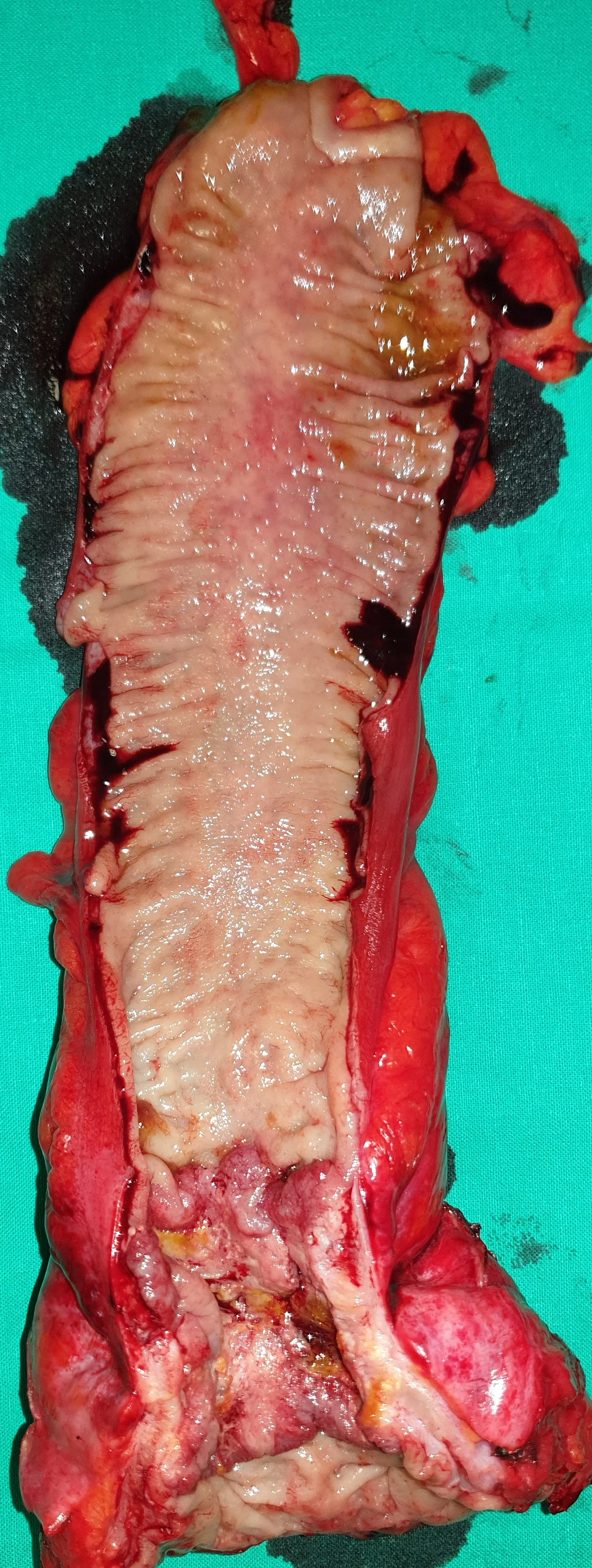
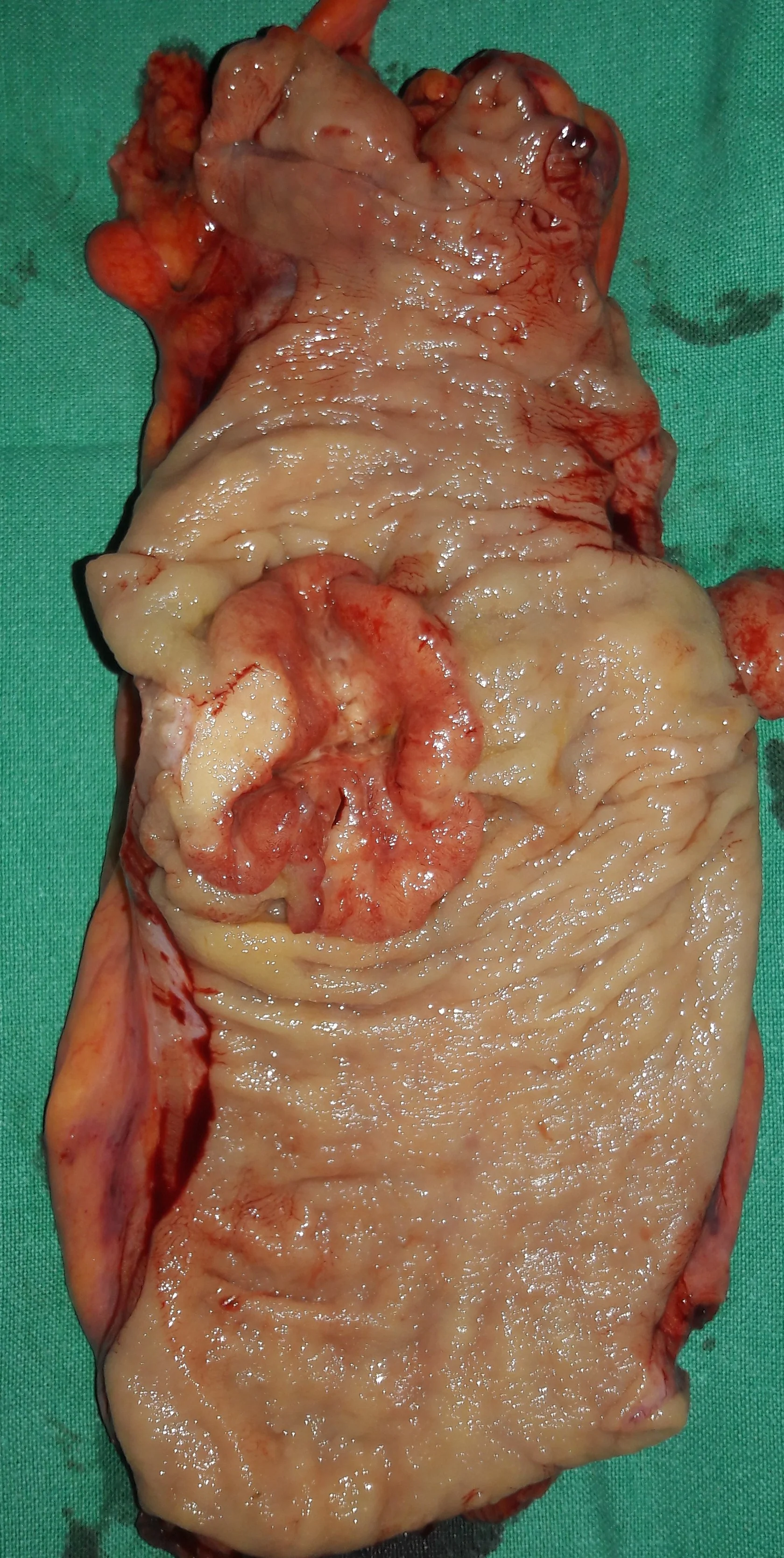
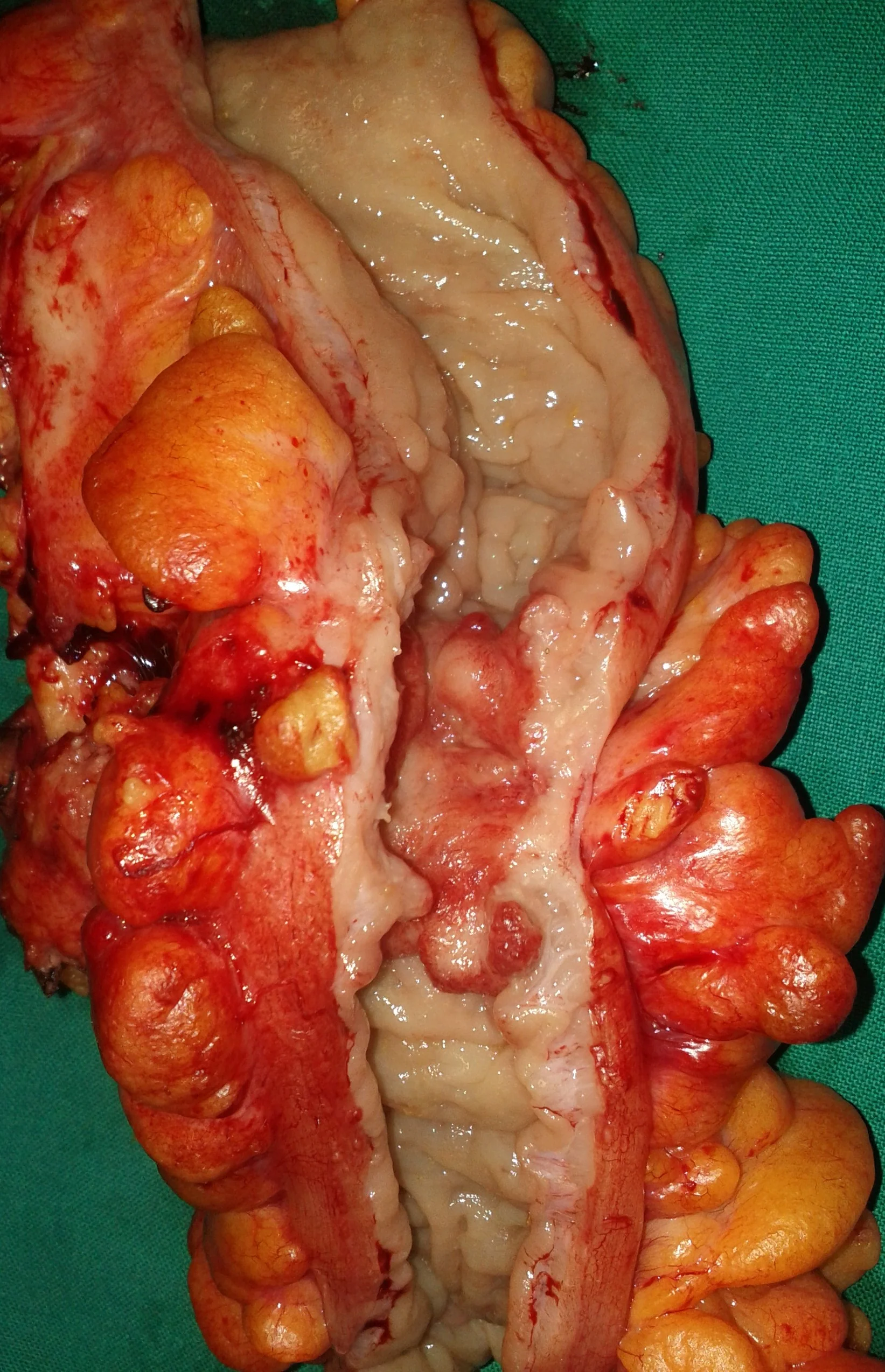
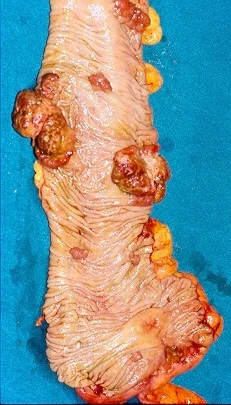
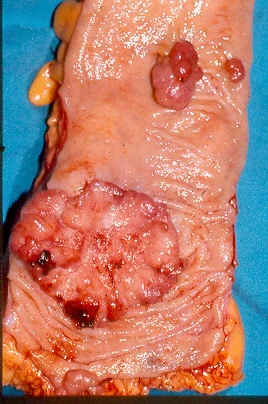
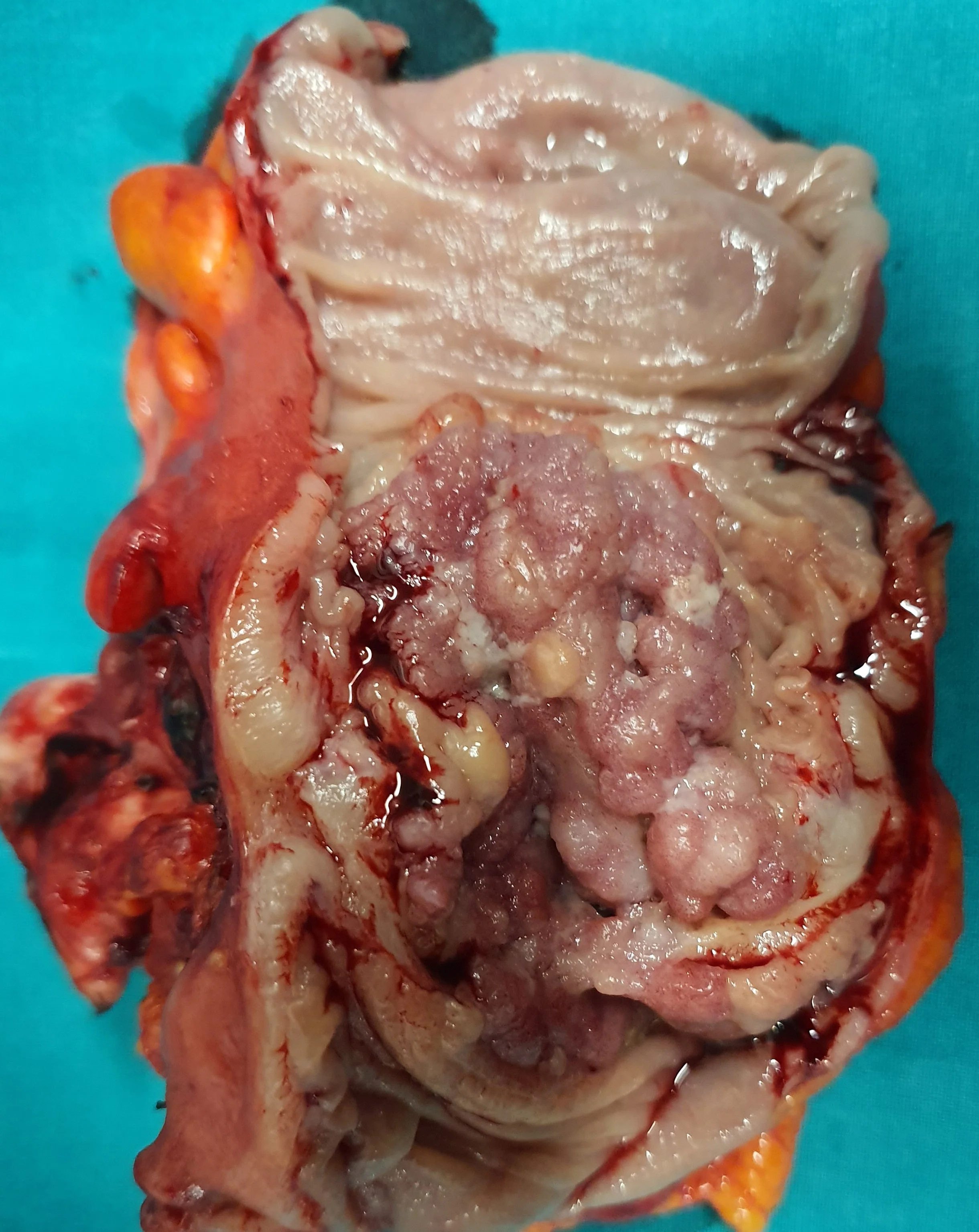
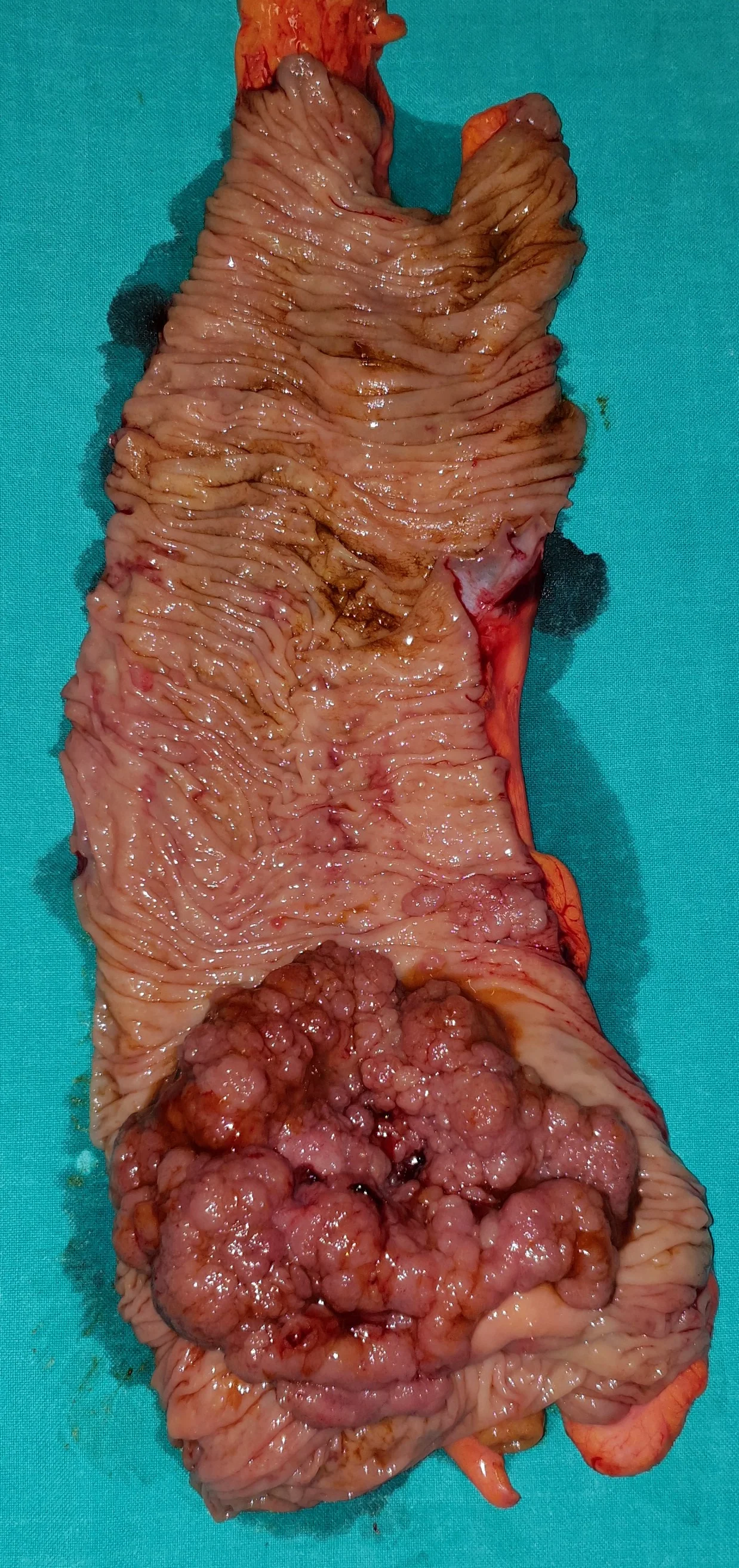
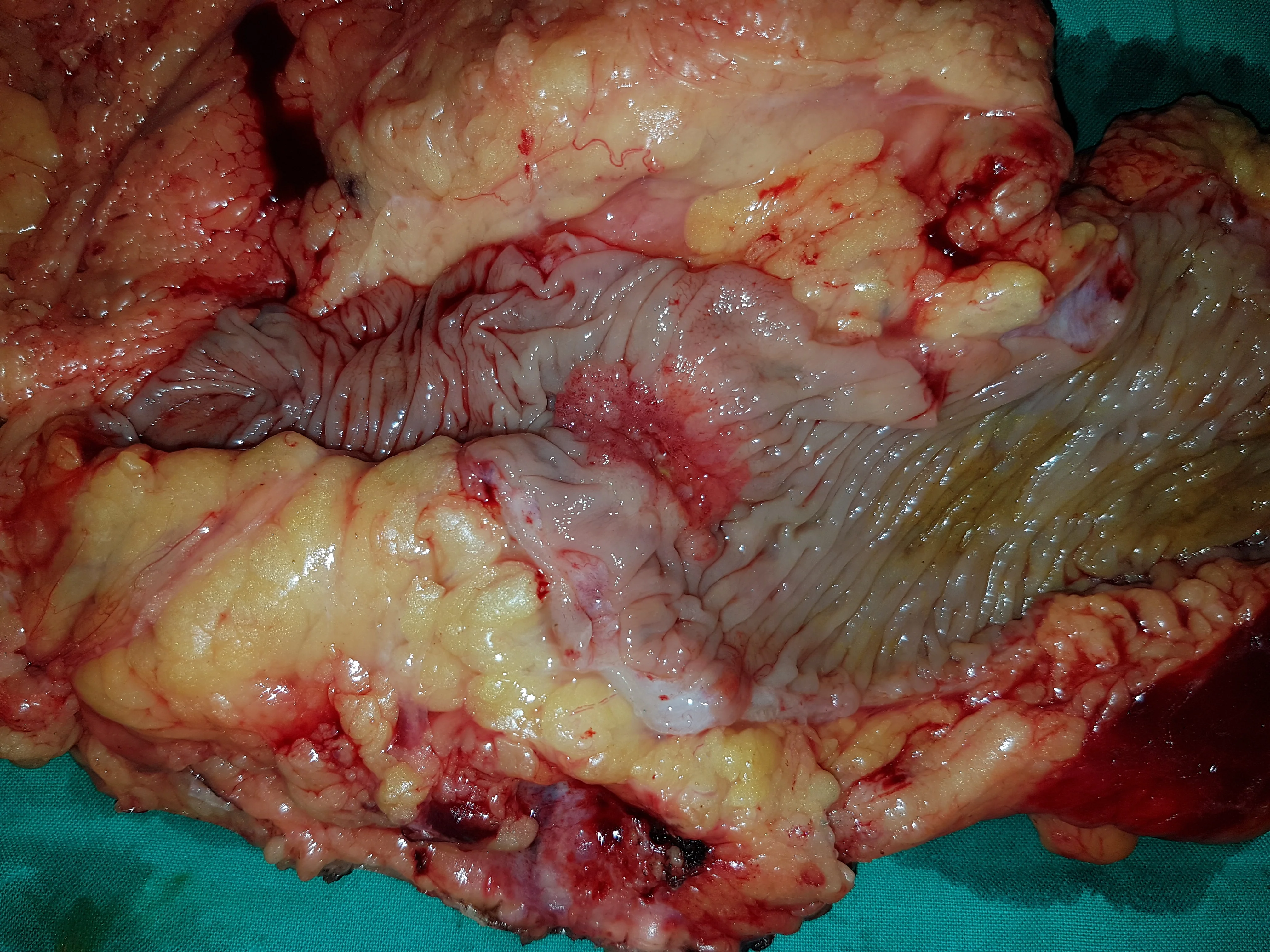
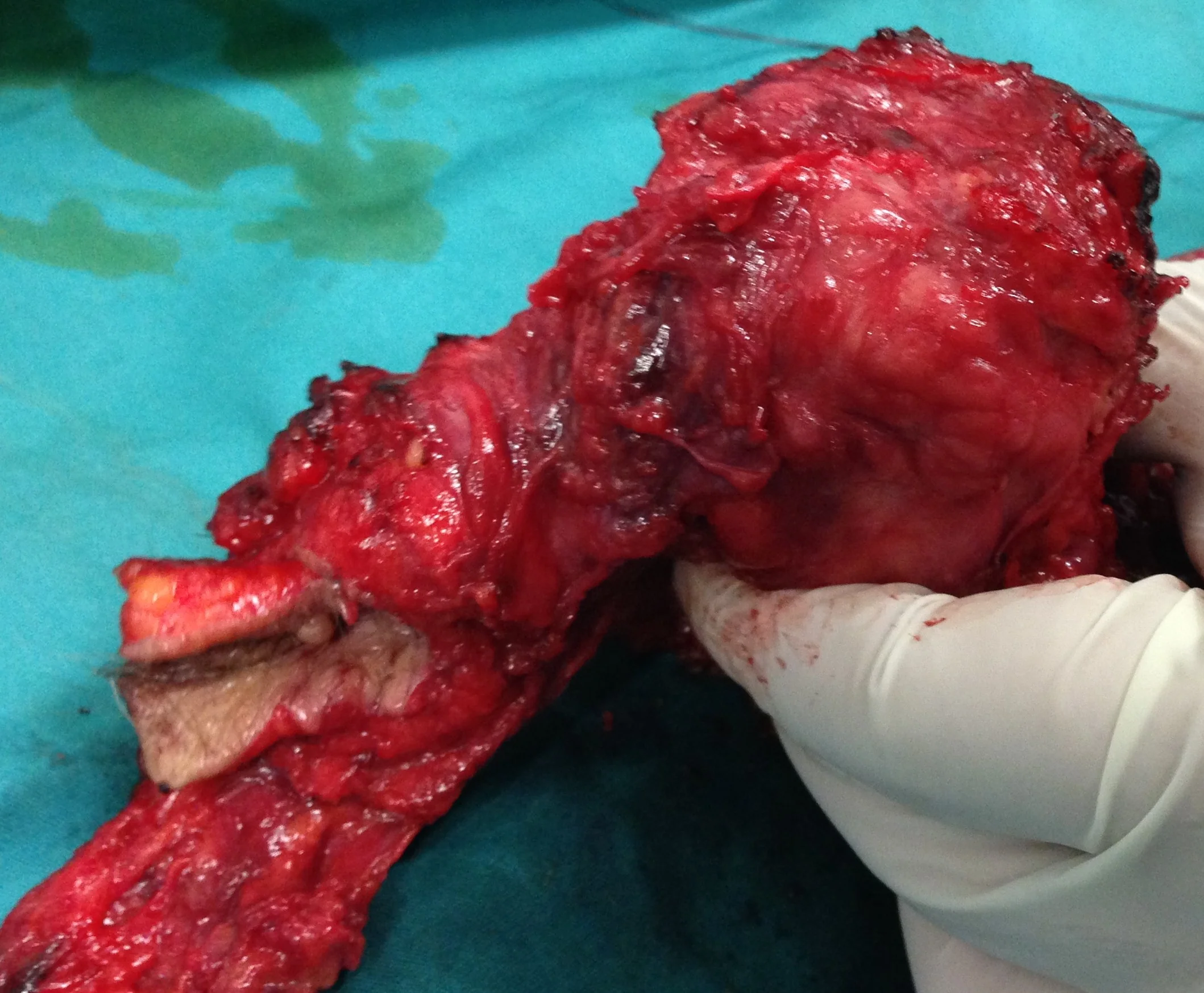
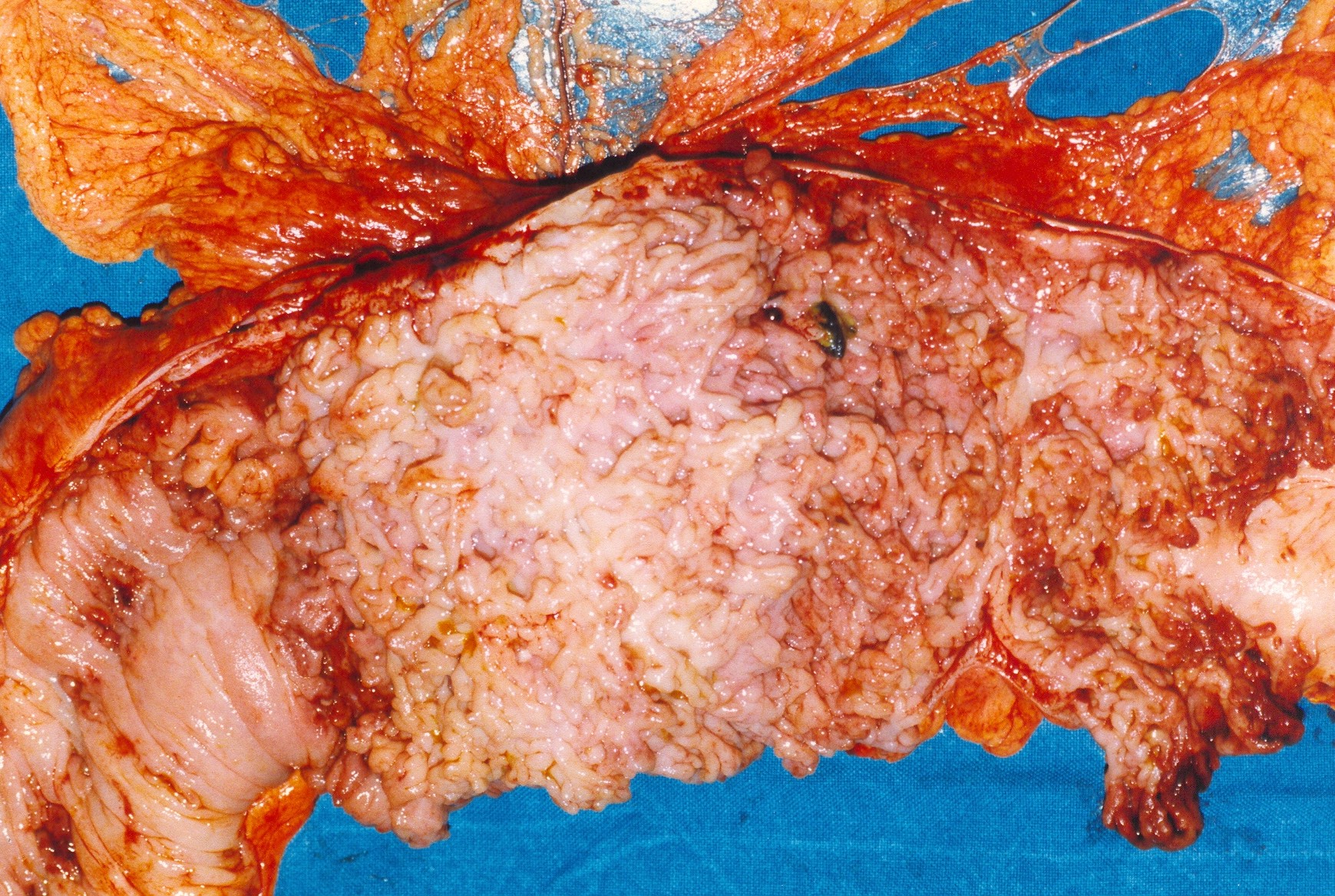
Resected specimen showing quintuple synchronous rectal adenocarcinomas (A, B, C, D)
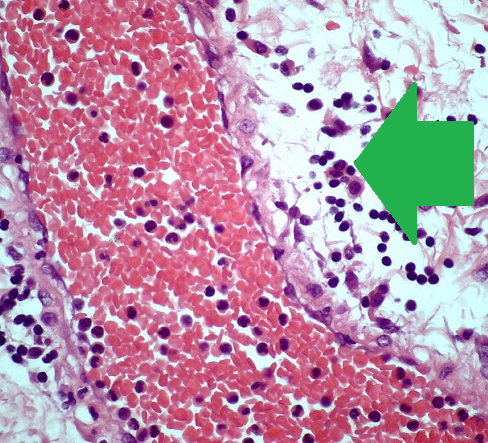
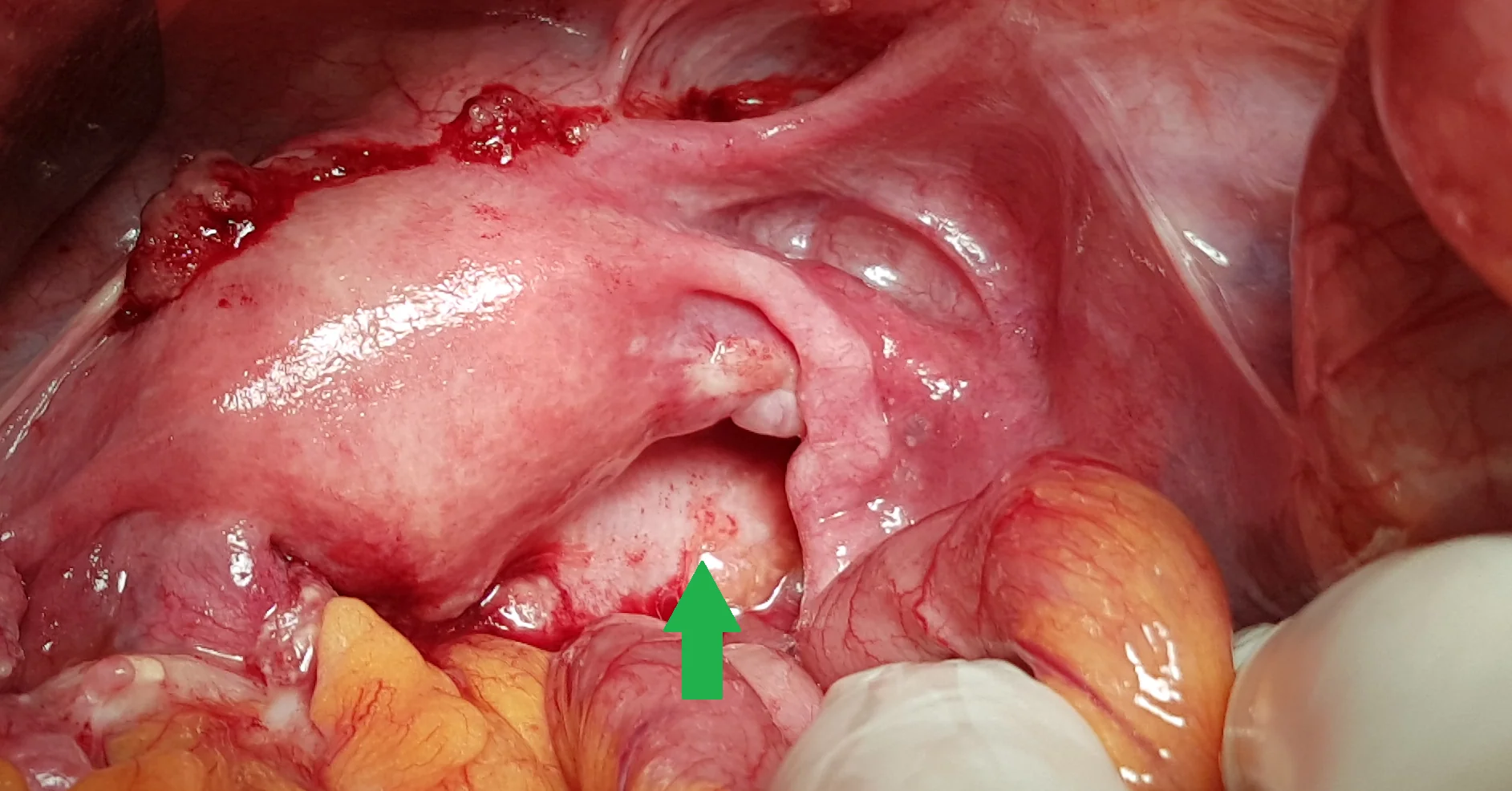
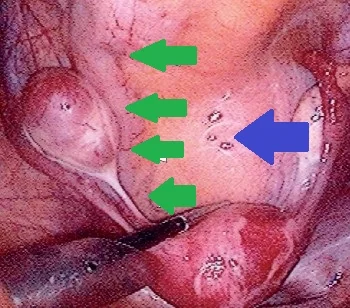
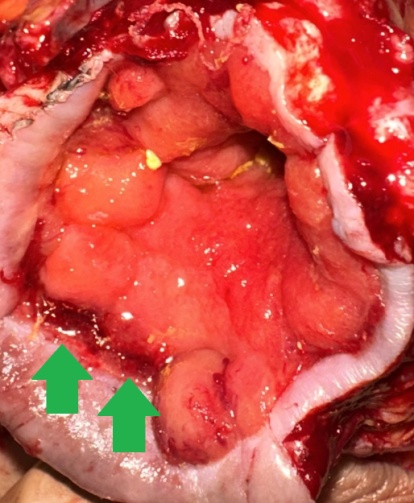
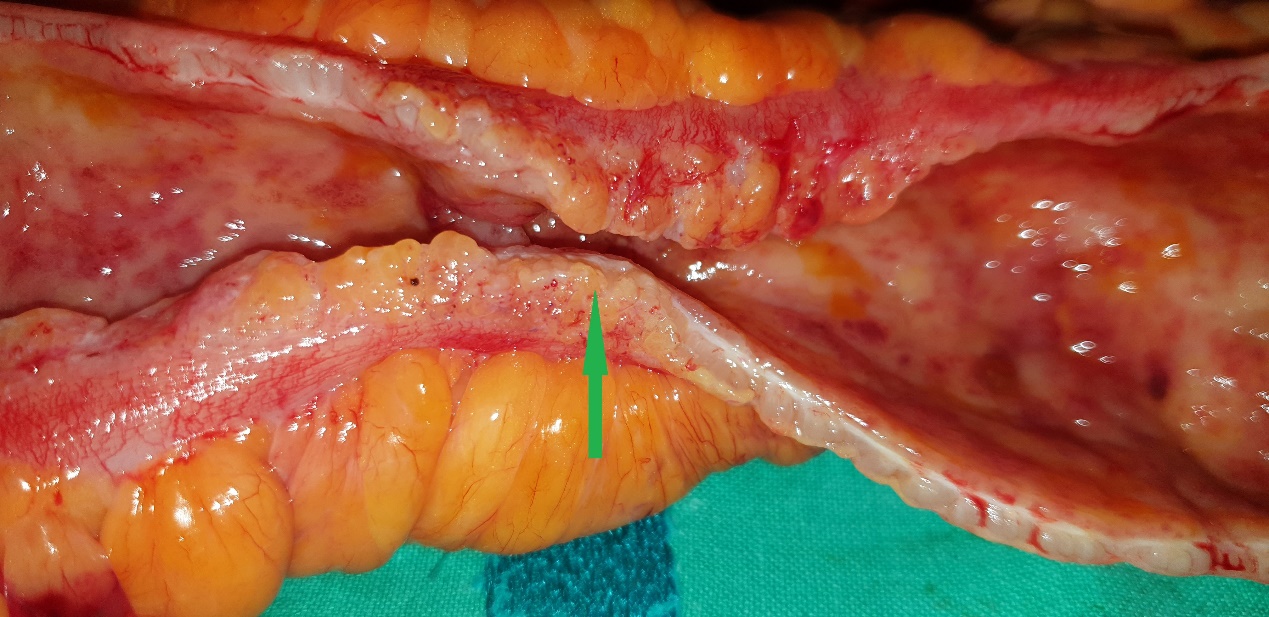
Green arrow – perivenular lymphocytic infiltration in a submucosal location (Courtesy Dr. V. Penopoulos)

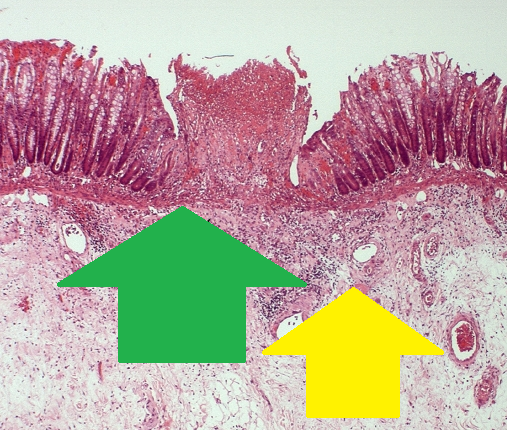
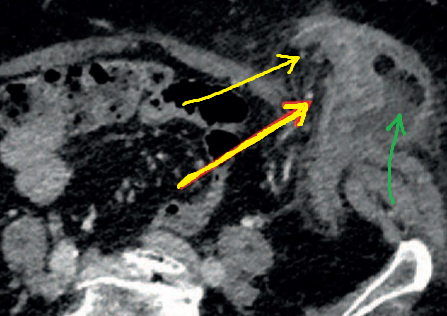
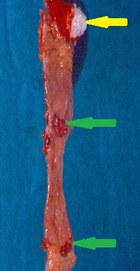
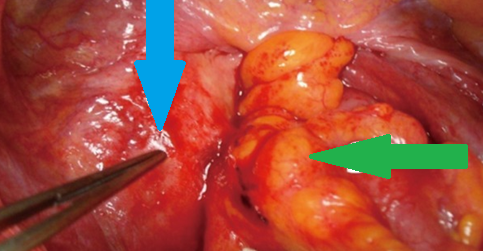
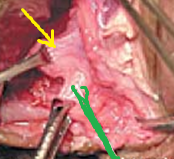
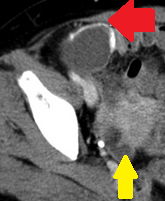
Green arrow - Focal mucosal ulceration.Yellow arrow - Submucosal lymphocytic infiltration.(Courtesy Dr. V. Penopoulos).
Postoperative hernia at the site of ileostomy closure.(Courtesy Dr.V.Penopoulos).(Courtesy Dr. V. Penopoulos)
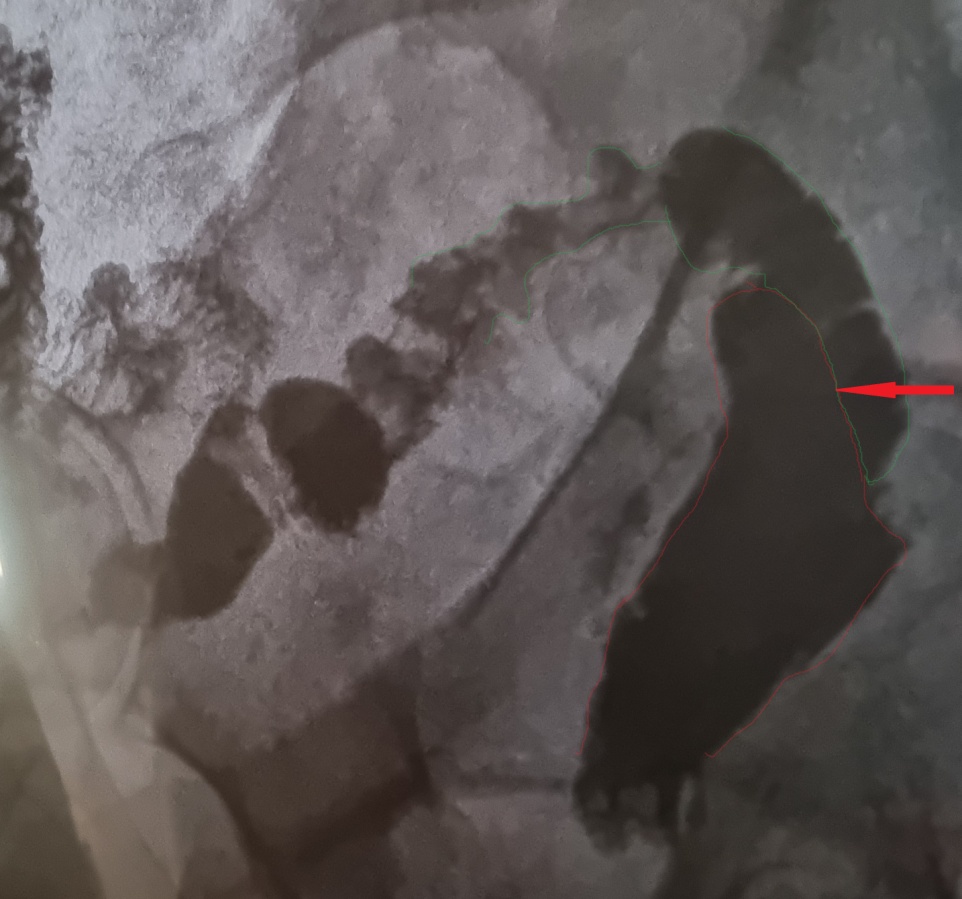
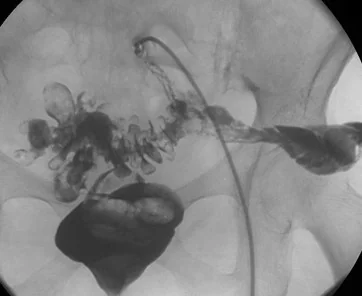
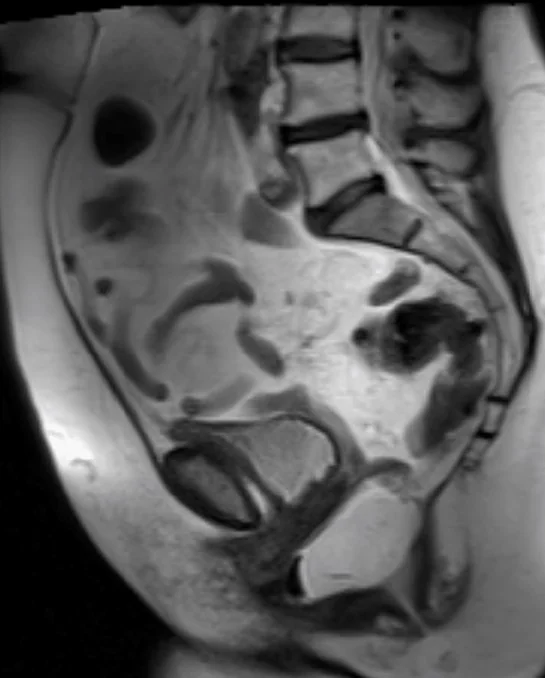
Postoperative imaging of ileorectal anastomosis (modified Duhamel). The anastomosis of the terminal ileum to the anterior wall of the remaining rectal stump is evident (Courtesy Dr. V. Penopoulos)

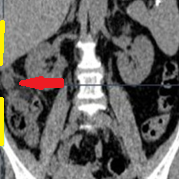
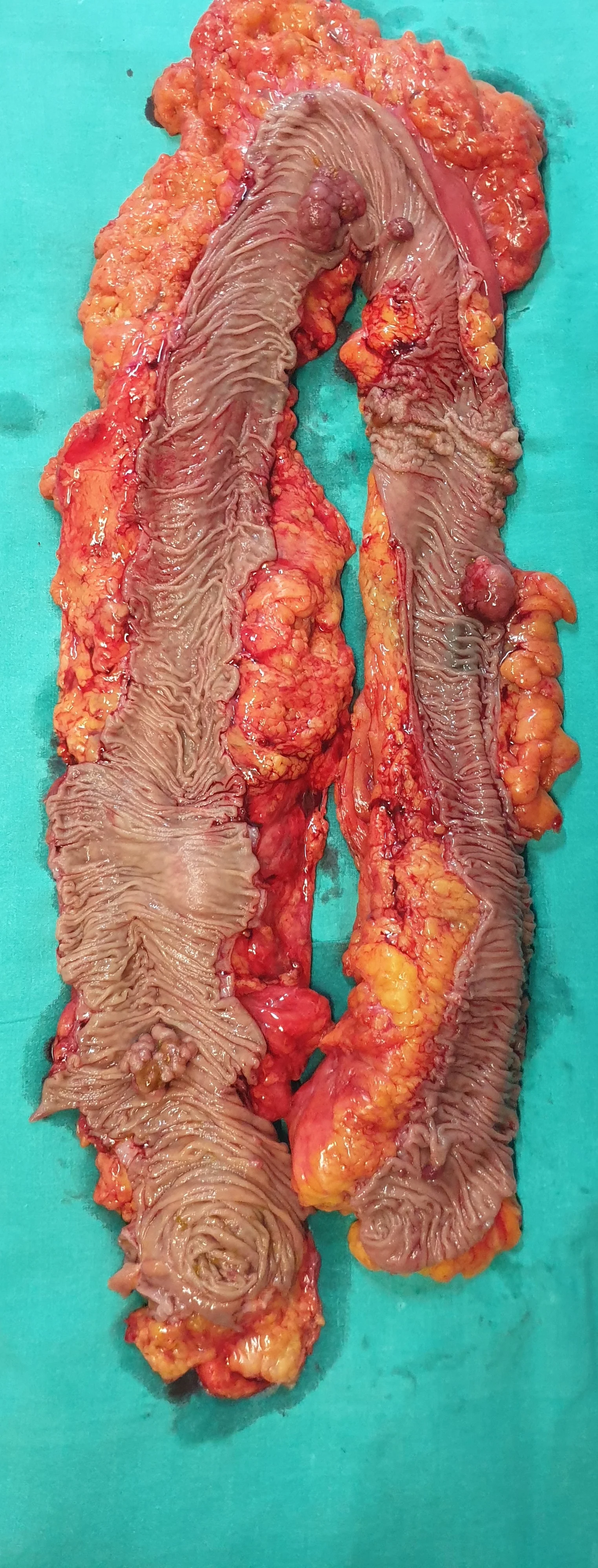
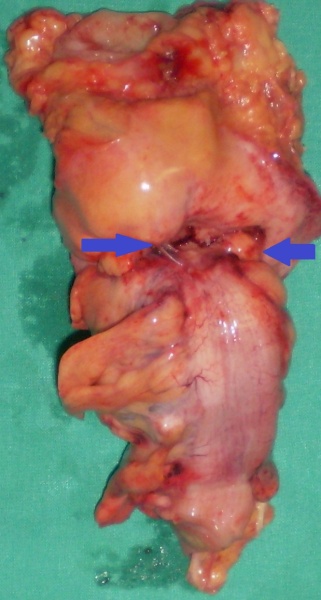
Total colectomy specimen. Red arrow: previous colocolonic anastomosis (Courtesy Dr. V. Penopoulos)



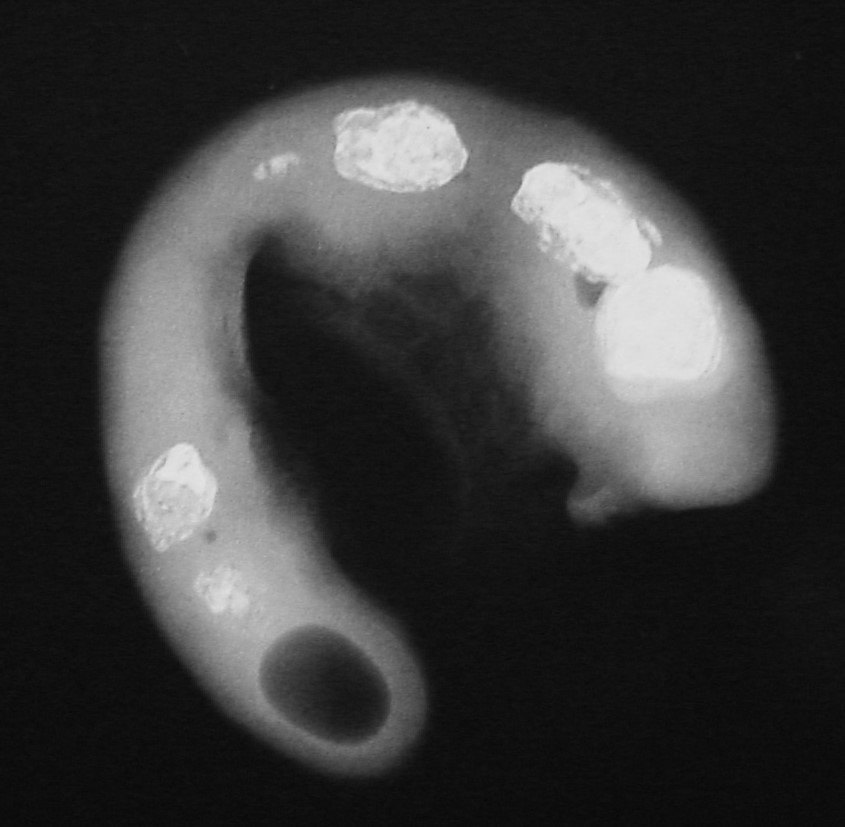
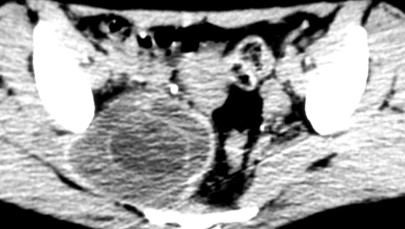
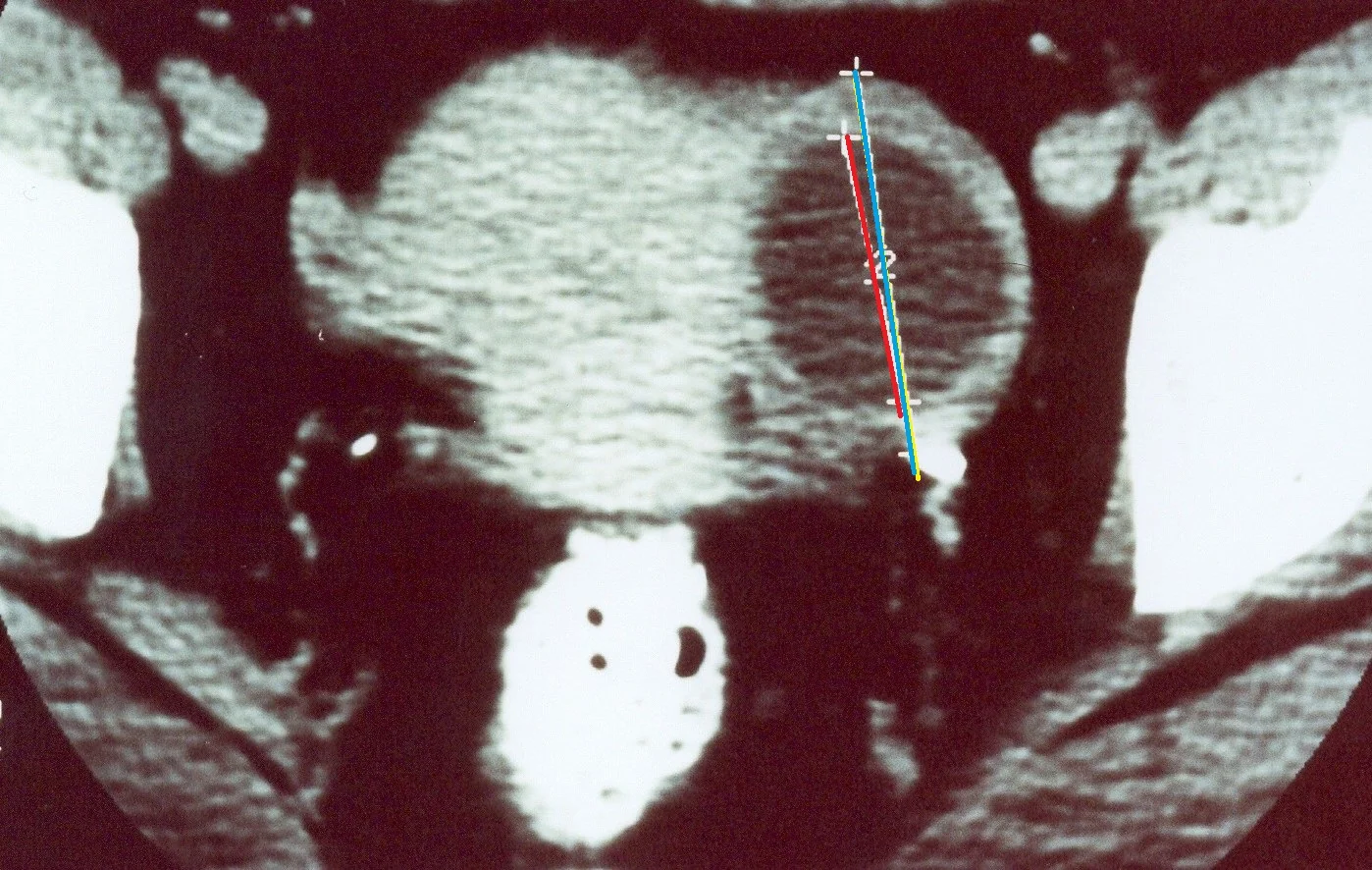
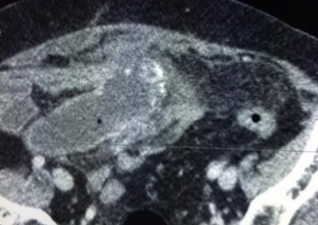
Abdominal CT scan. Presence of calcifications, cystic-solid areas, and adipose tissue, suggestive of a right-sided teratoma (Courtesy Dr. V. Penopoulos)


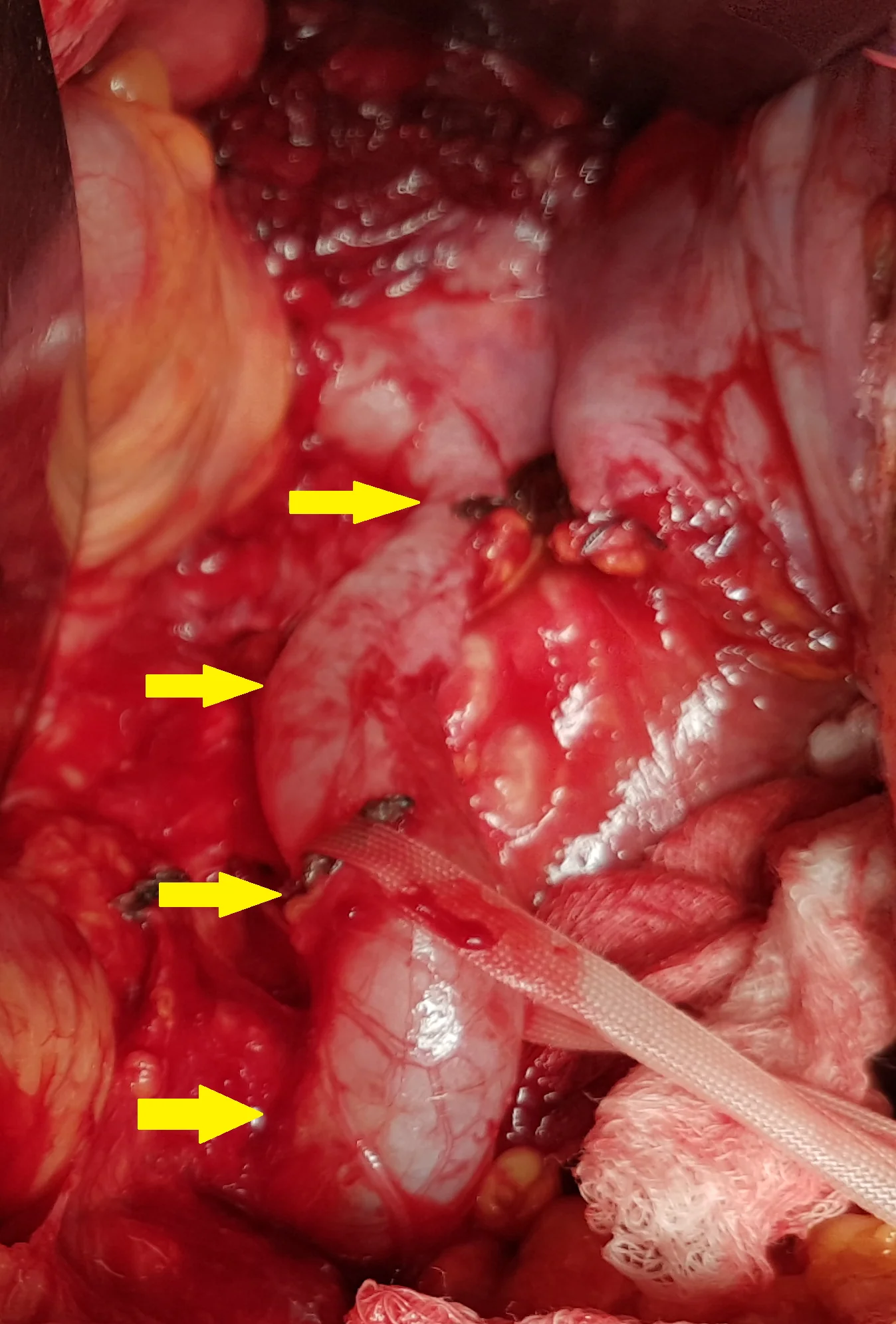
Yellow arrows — Inflamed diverticula in the extra-abdominal bowel segment. Green arrow — Fluid collection (Courtesy Dr. V. Penopoulos)

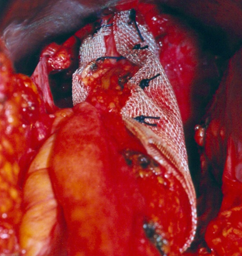
Abdominal CT scan. Erosion/migration of the mesh within the rectum (Courtesy Dr. V. Penopoulos)

Non-inflamed diverticula in the colon segment immediately beneath the exteriorized end colostomy (Courtesy Dr. V. Penopoulos)
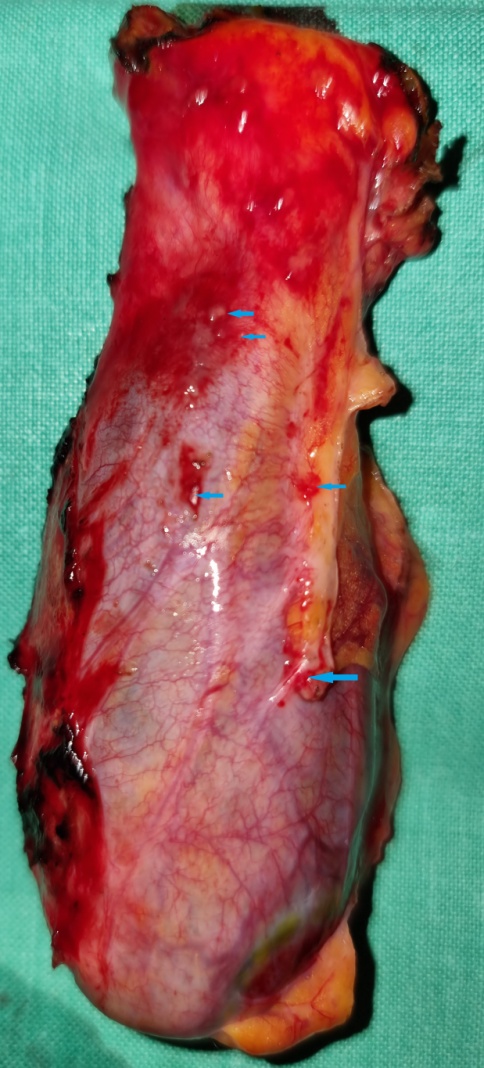
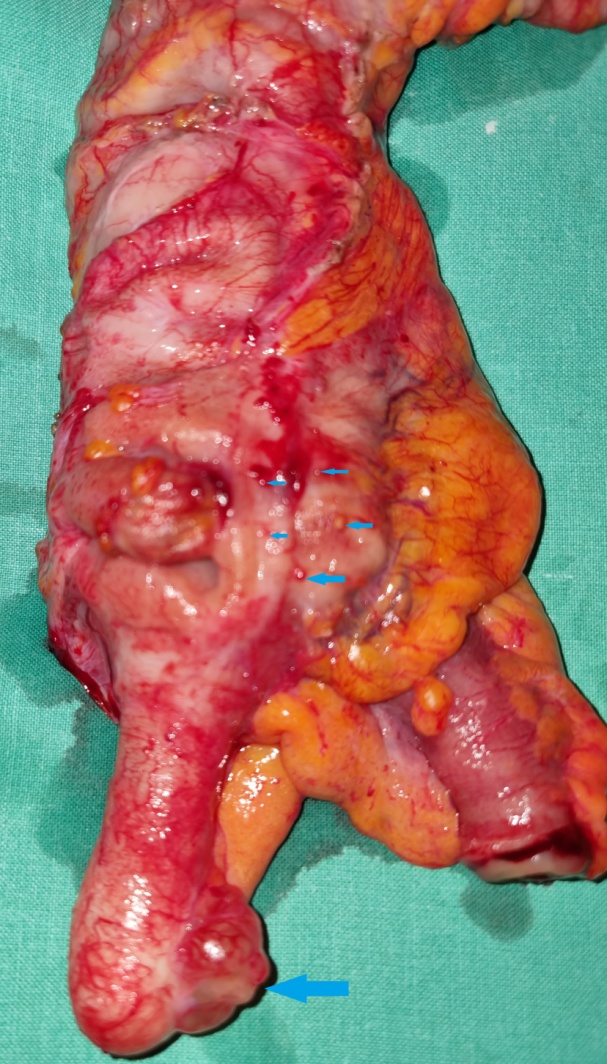
Excised end colostomy segment. Blue arrows — Diverticular sites (Courtesy Dr. V. Penopoulos)

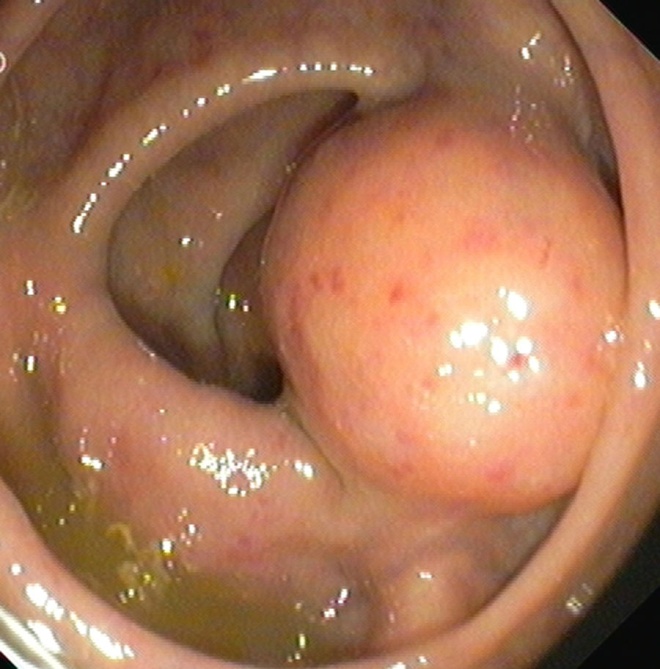
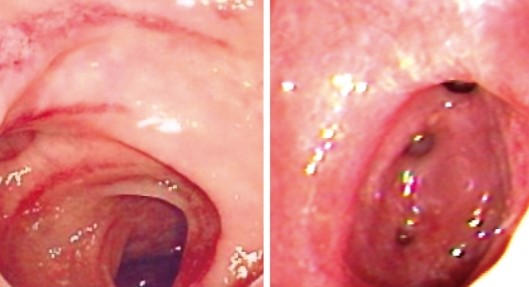
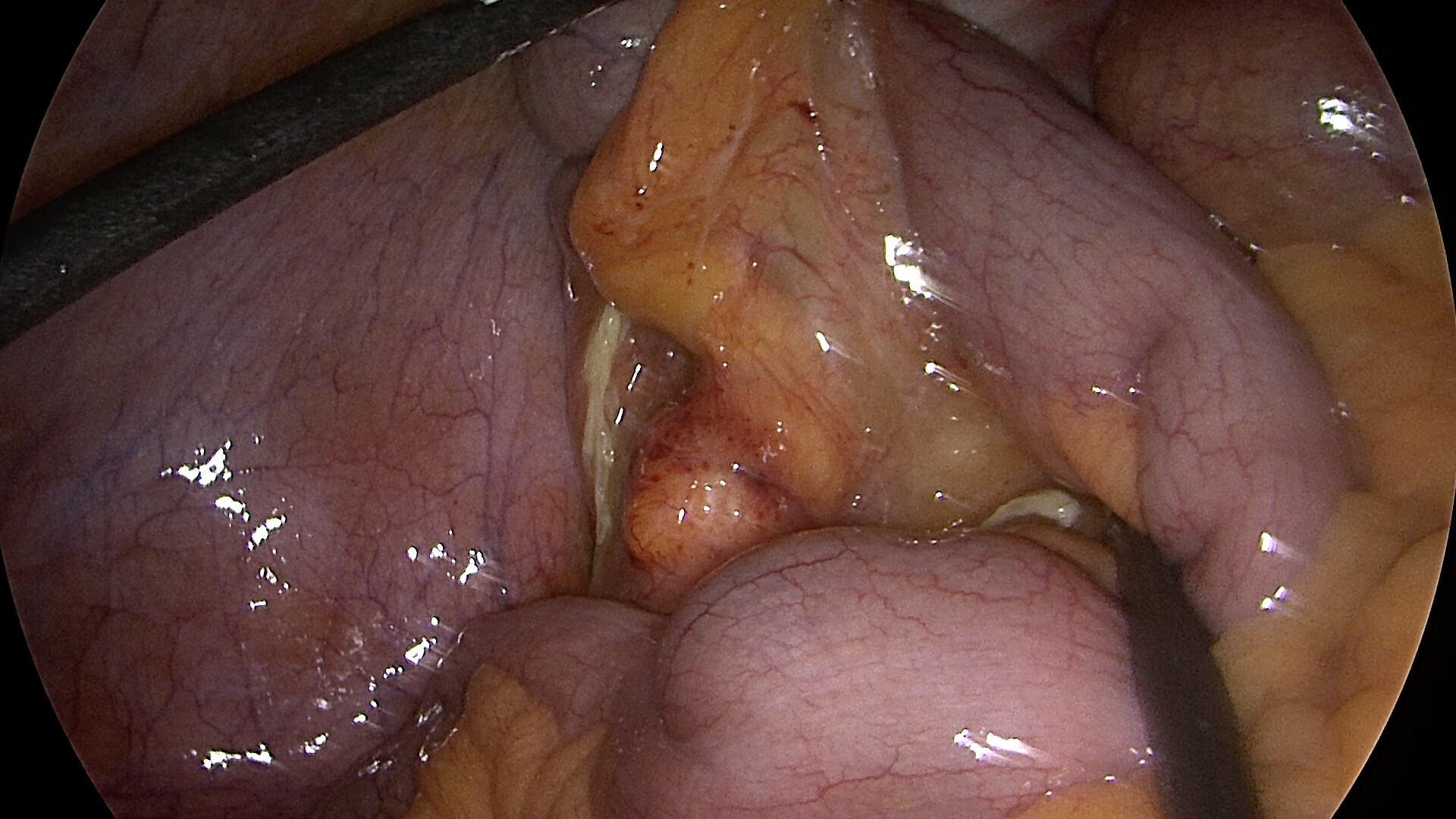
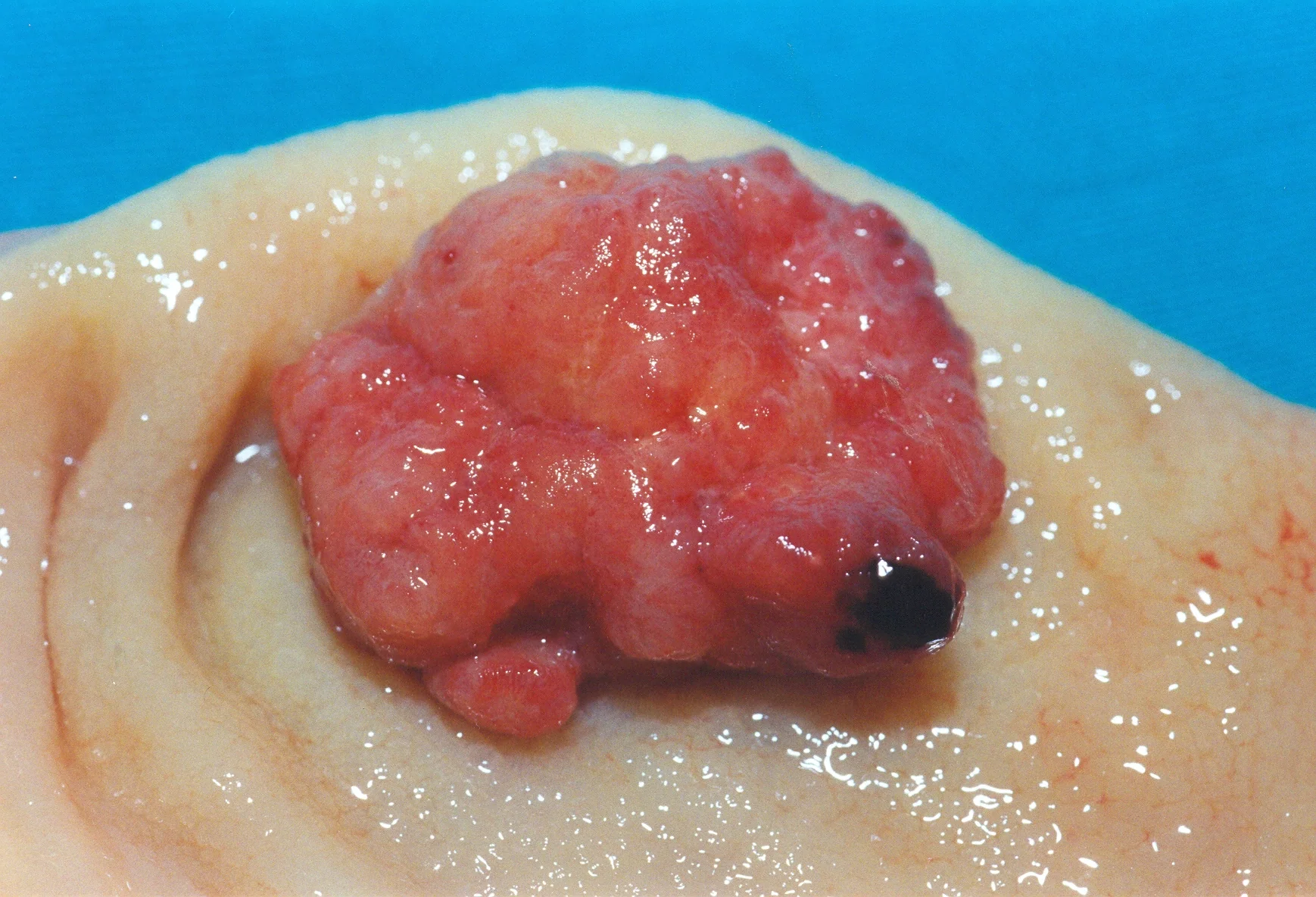
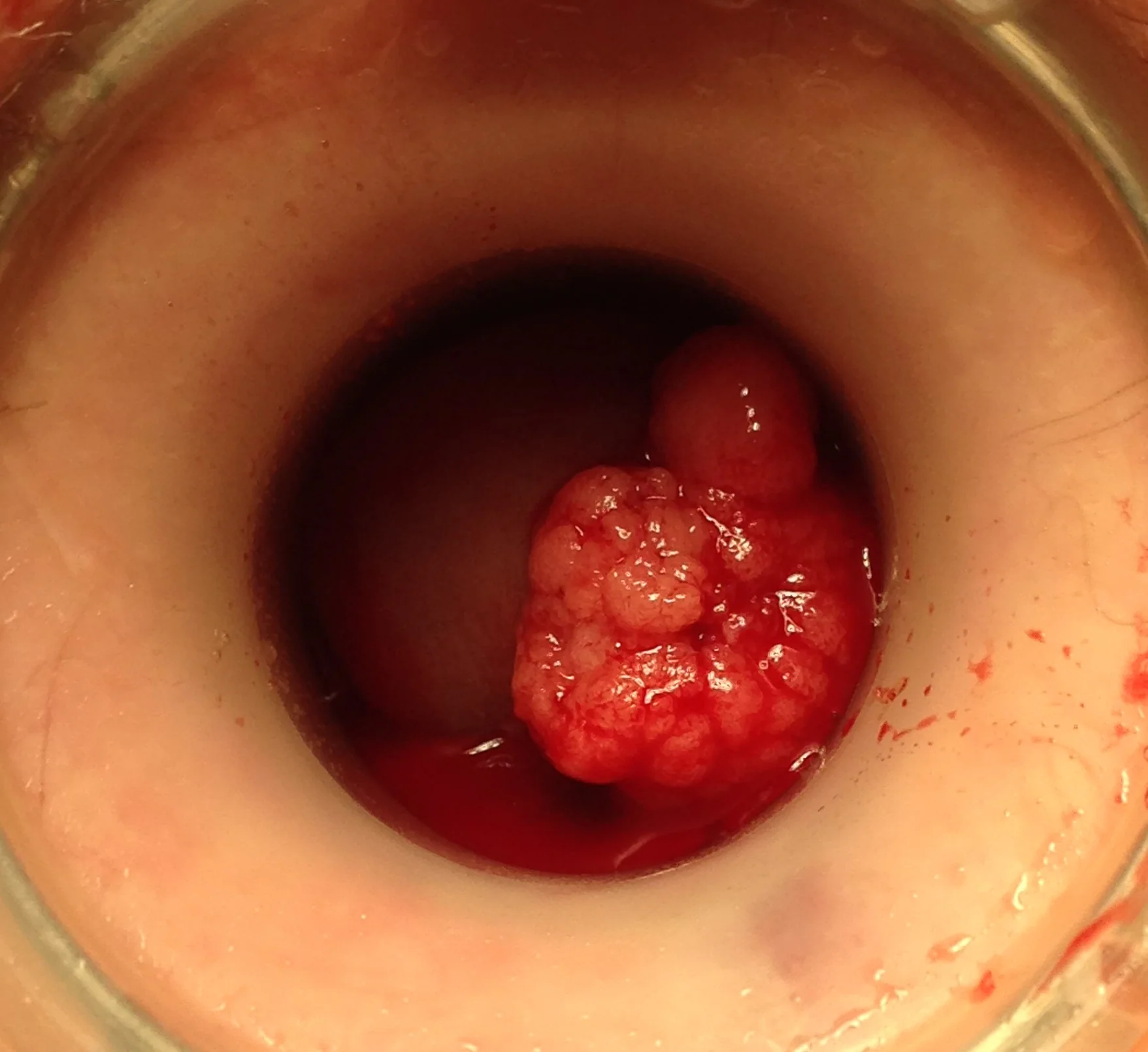
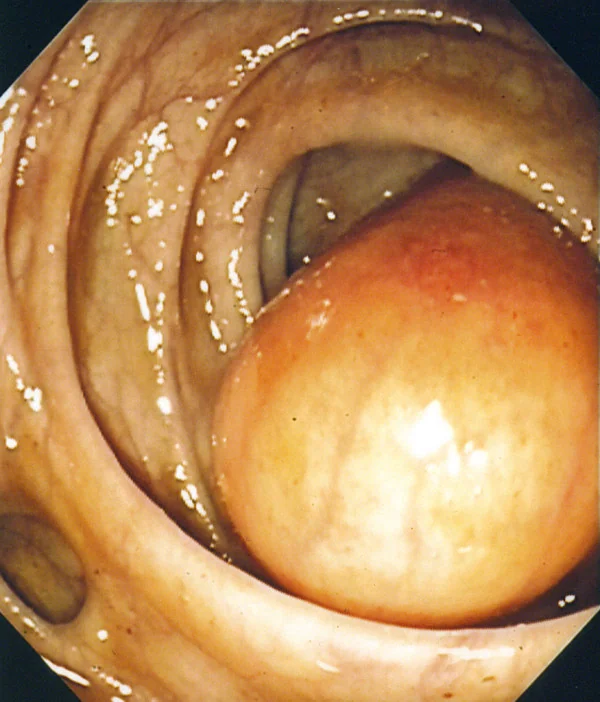
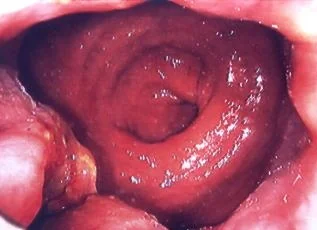
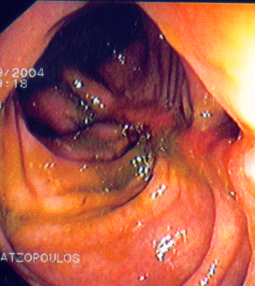
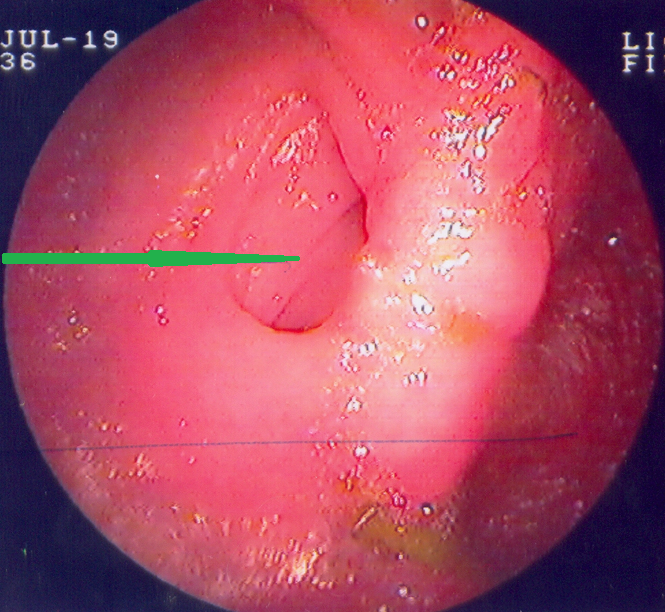
Lymphatic cyst .Colonoscopy revealed a polypoid mass protruding in the medial aspect of the left colonic flexure

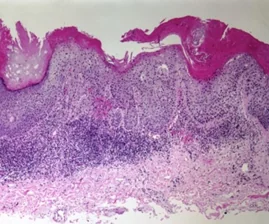
Inflammatory cloacogenic polyp with inflammatory fibromuscular stroma and hyperplastic epithelium (Courtesy Dr. V. Penopoulos)
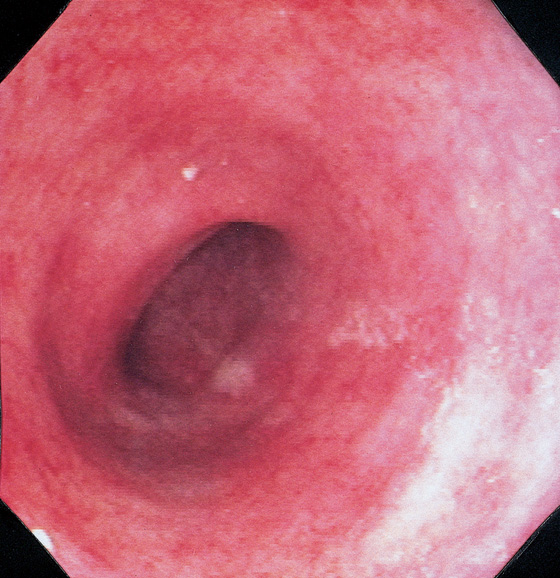
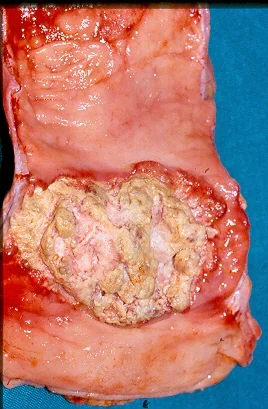
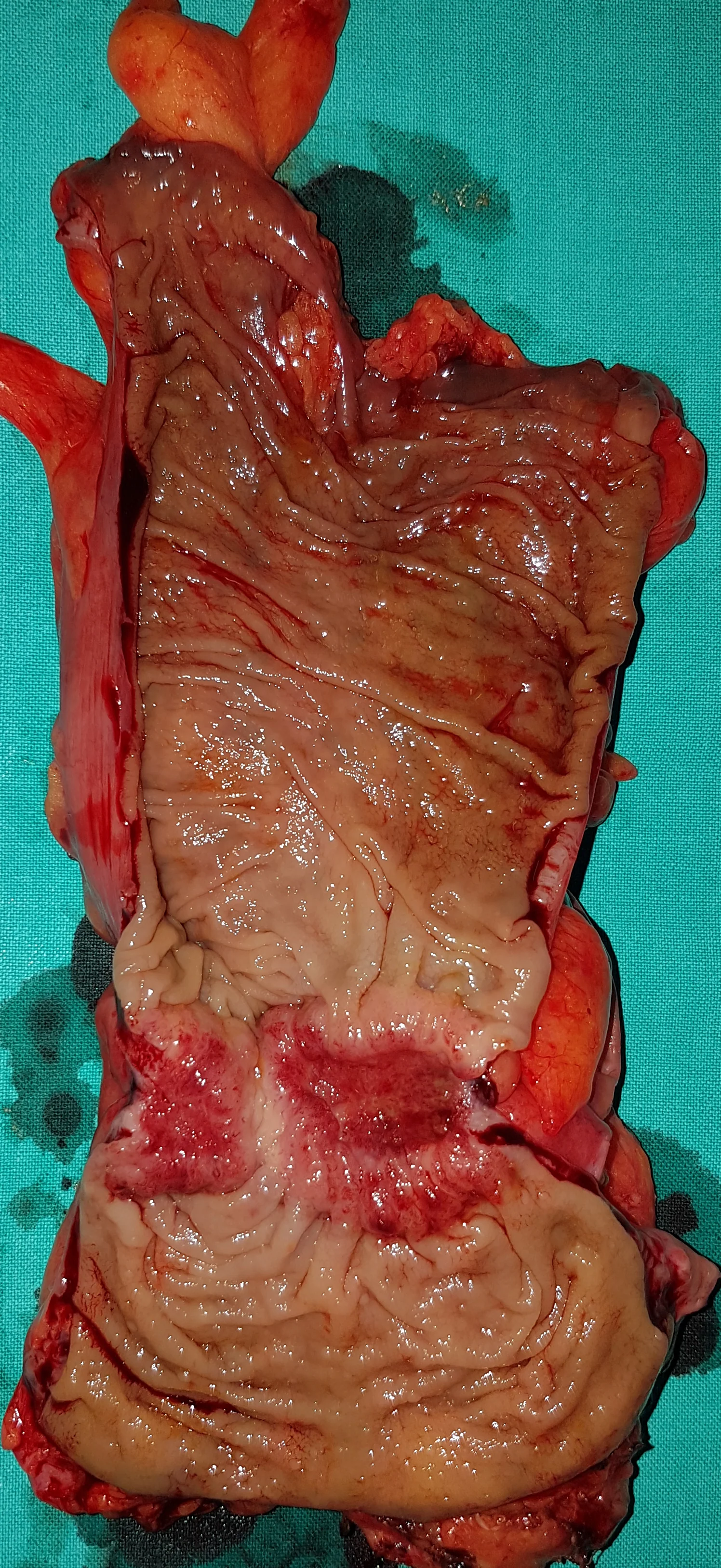
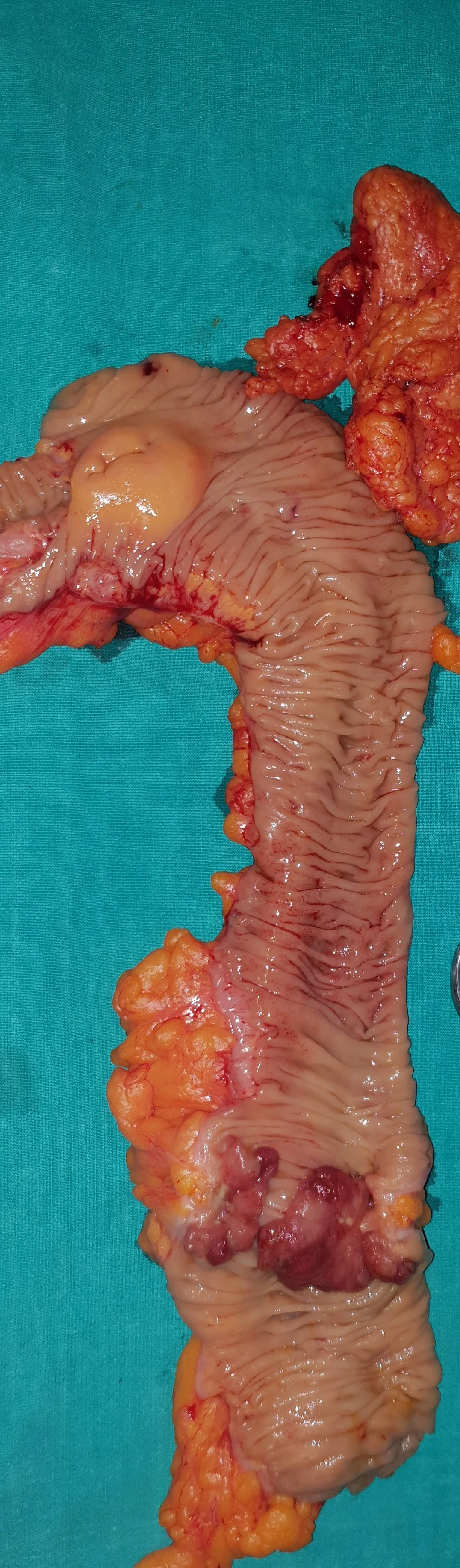
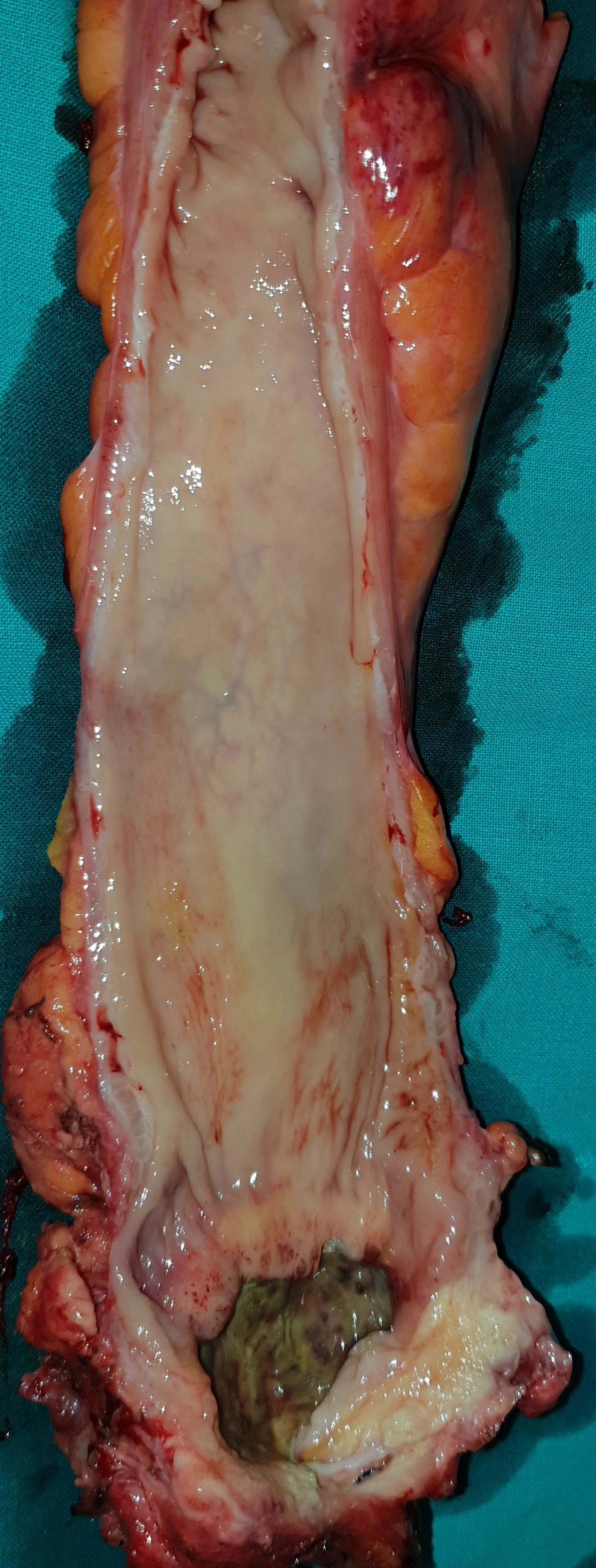
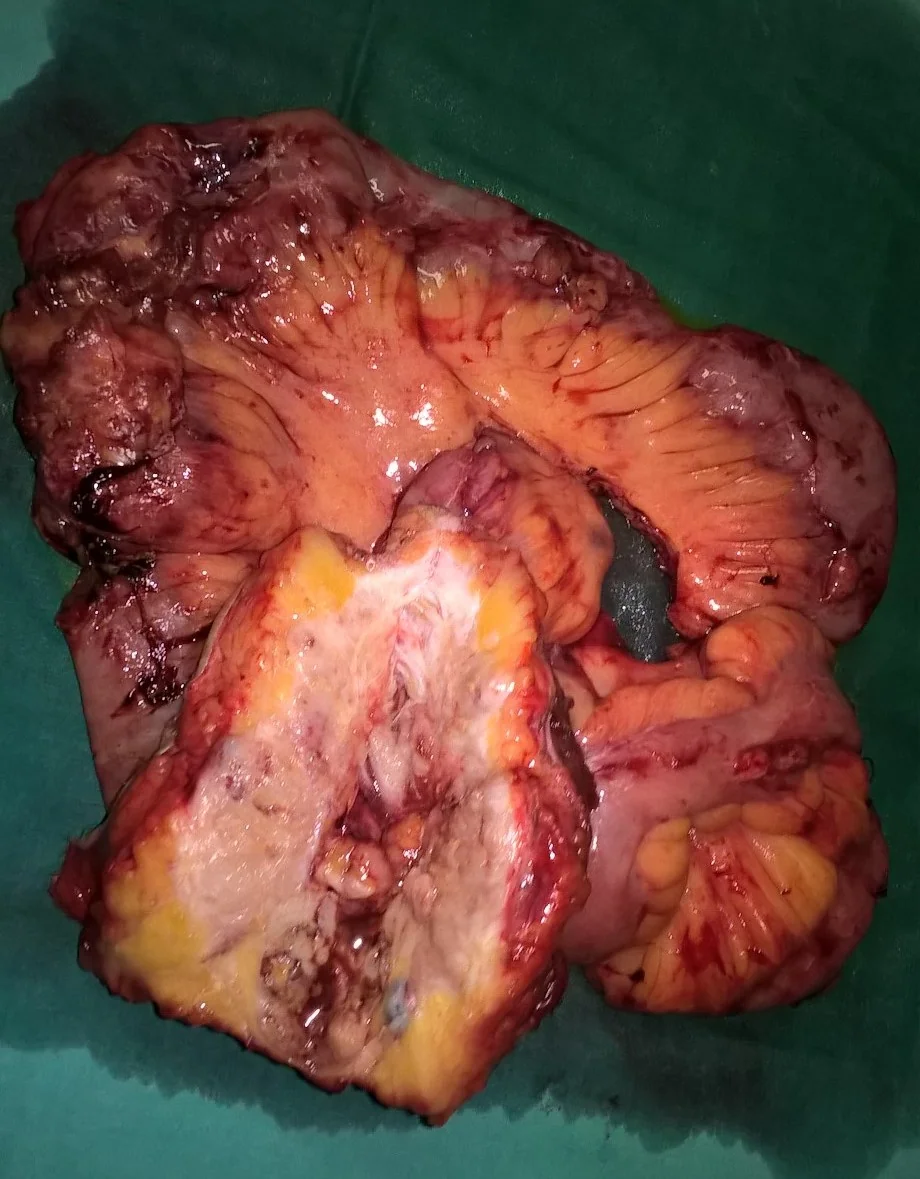
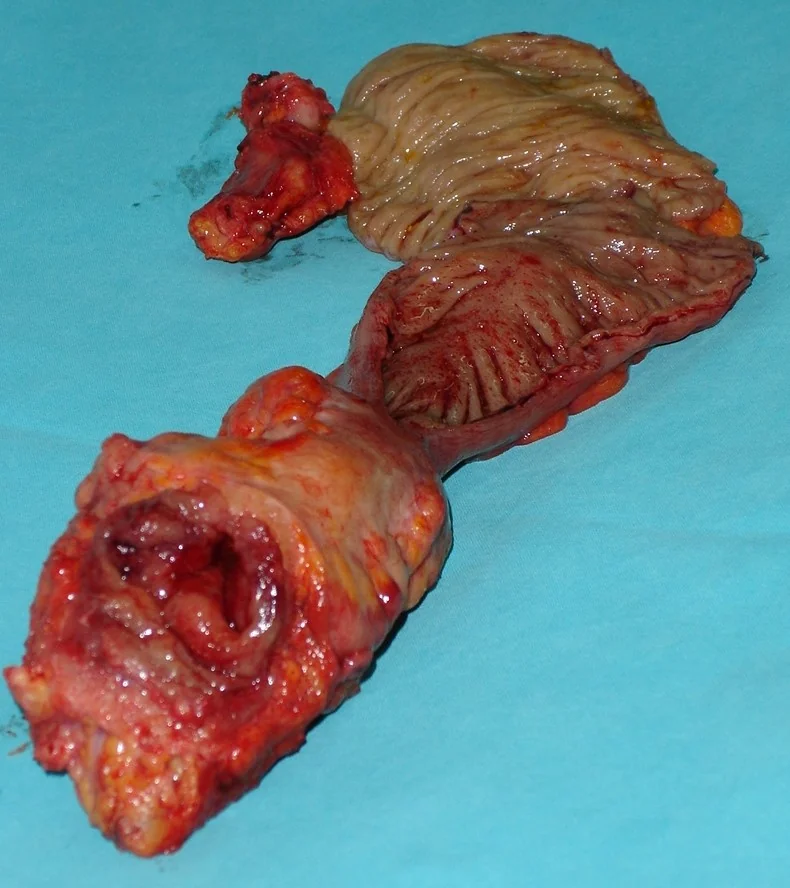
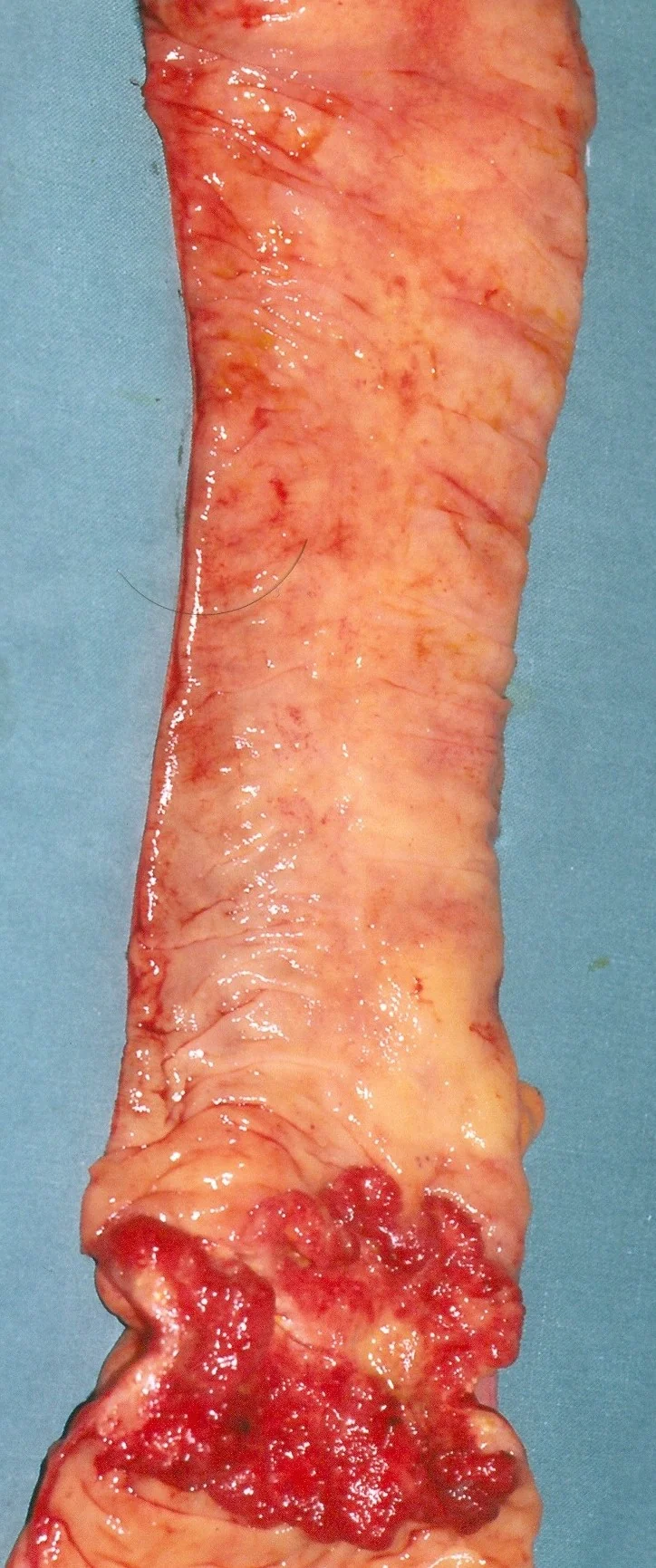
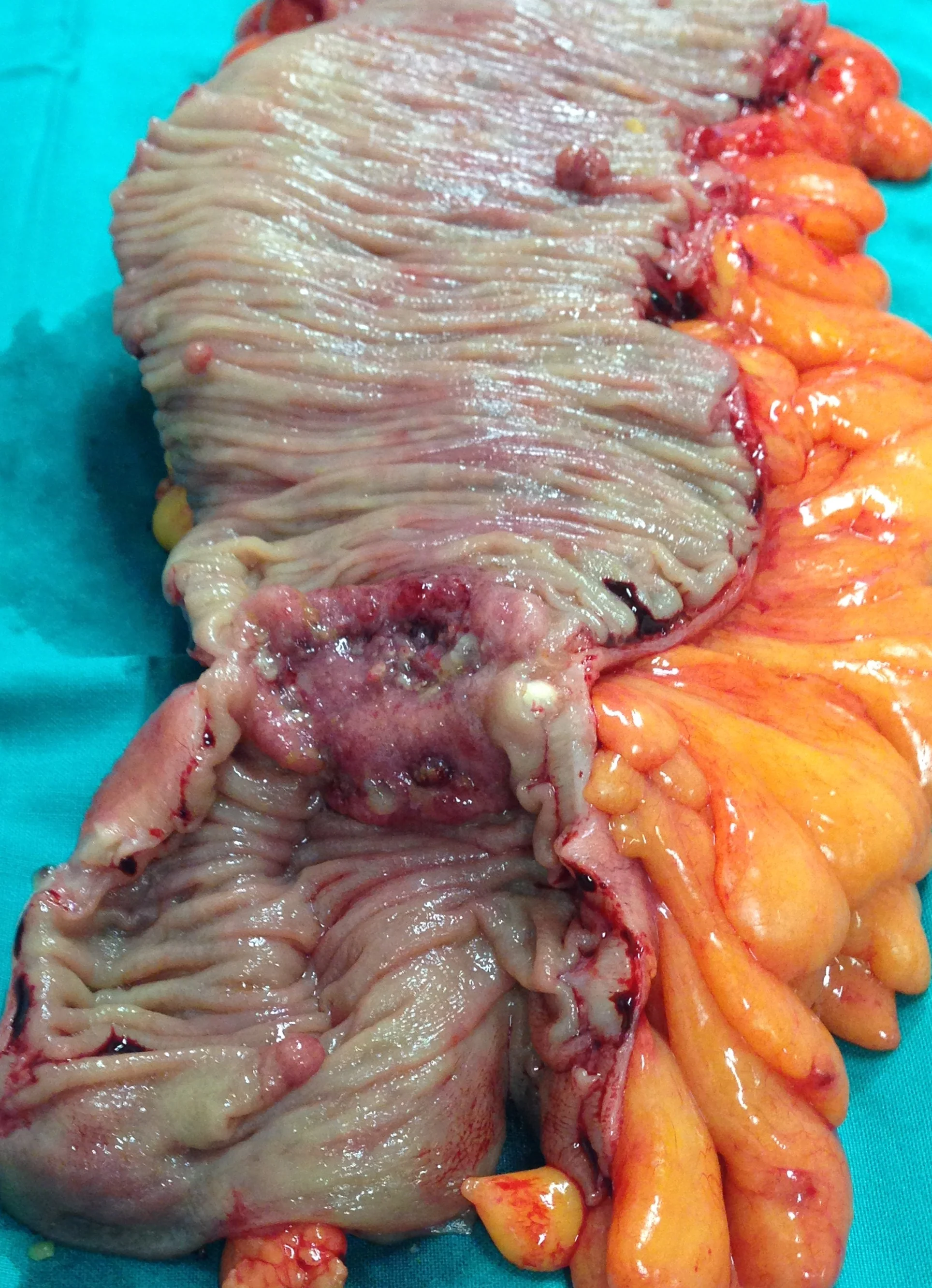
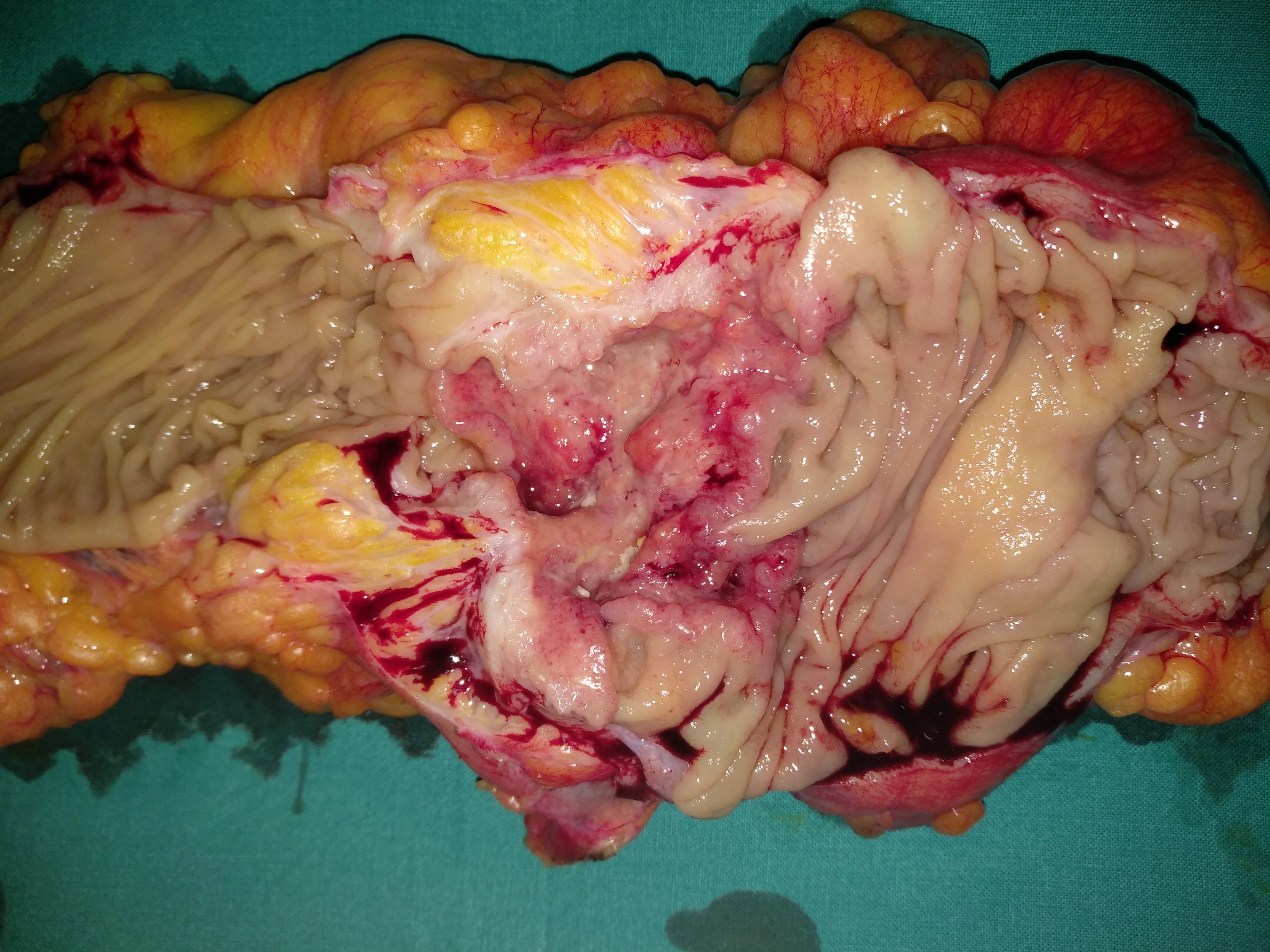
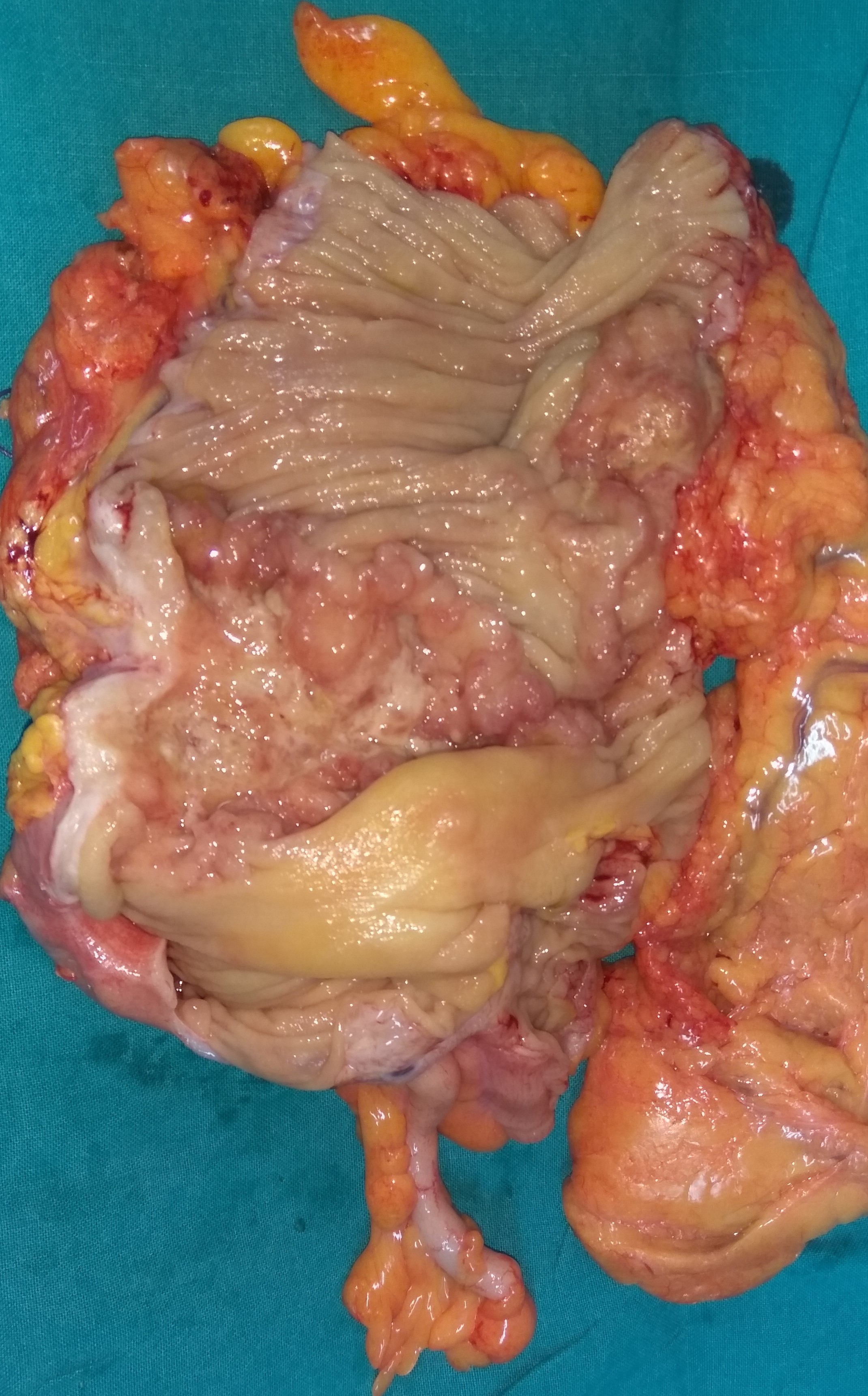
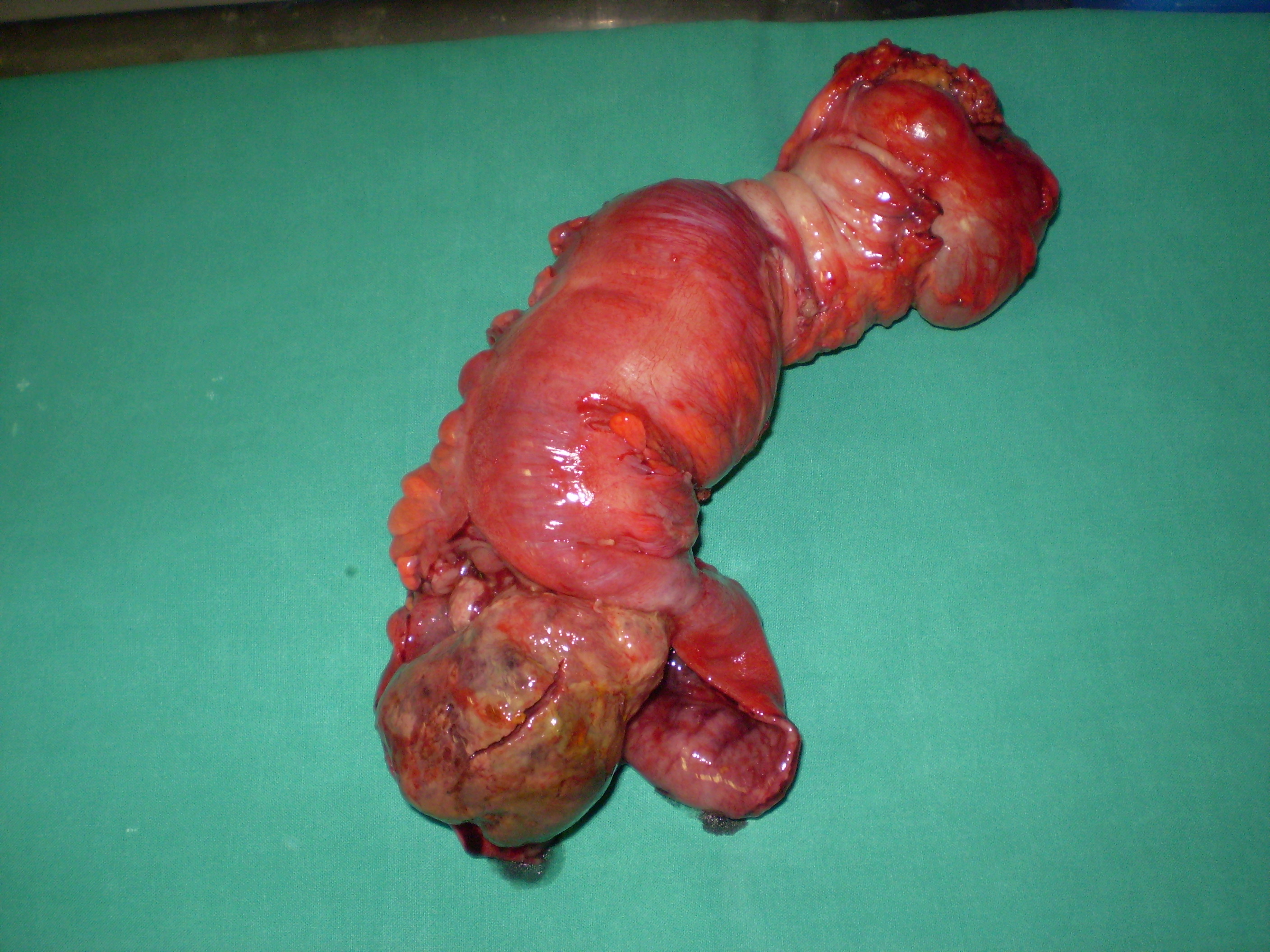
Ulcerative colitis . Stenosis of excised sigmoid colon causing complete bowel obstruction.(Courtesy Dr . V . Penopoulos).

Inflammatory cloacogenic polyp with inflammatory fibromuscular stroma and hyperplastic epithelium.(Courtesy Dr. V. Penopoulos)
Inflammatory cloacogenic polyp with inflammatory fibromuscular stroma and hyperplastic epithelium (Courtesy Dr. V. Penopoulos)
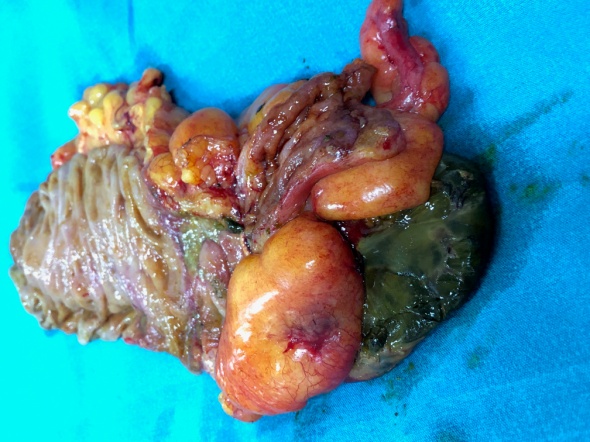
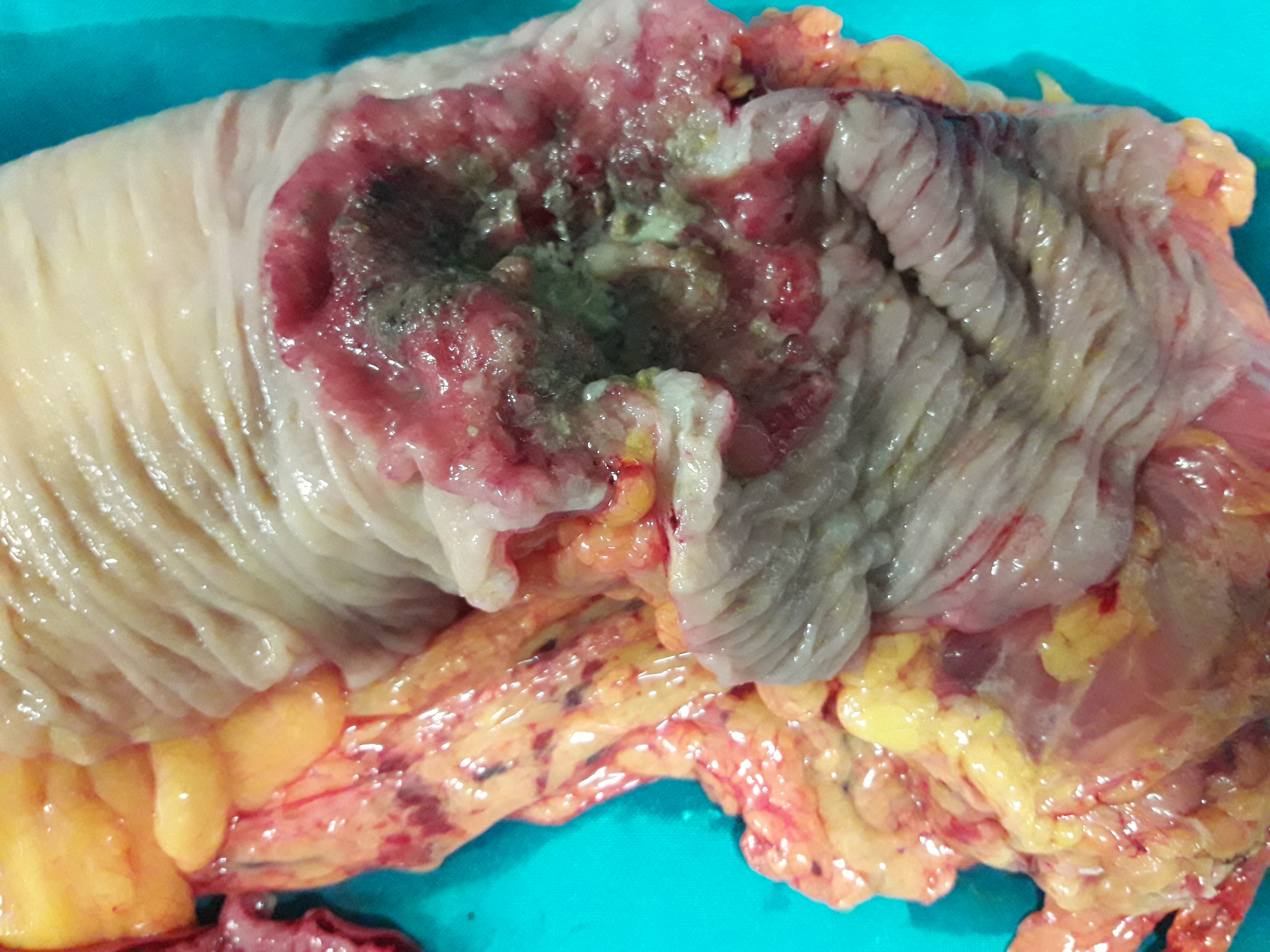
Surgical specimen. Necrosis of a portion of the cecum is evident (Courtesy Dr. V. Penopoulos)
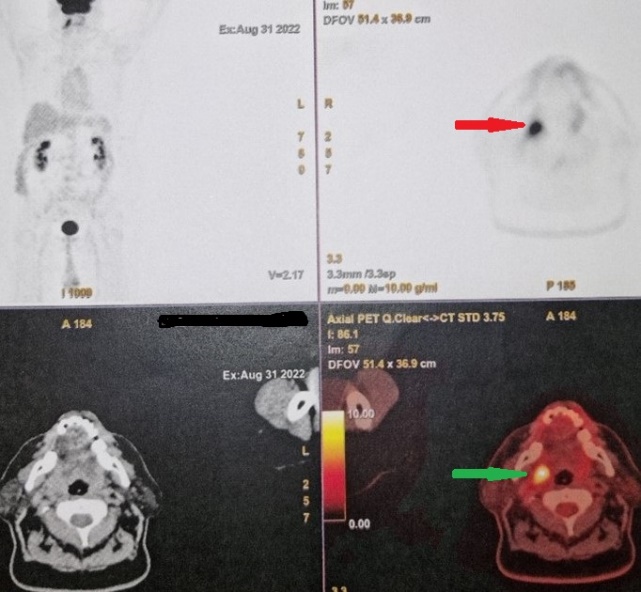
PET Scan . Metastatic carcinoma in the right palatine tonsil (Courtesy Dr. V. Penopoulos).


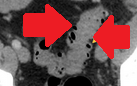
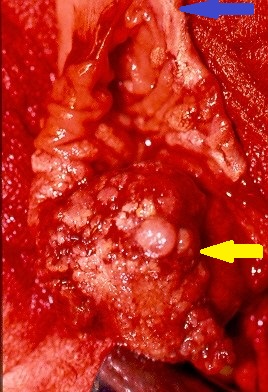
Green arrow: necrosis of the cecum. Blue arrow: normal appendix (Courtesy Dr. V. Penopoulos)

Surgical specimen. Necrosis of a portion of the cecum is evident (Courtesy Dr. V. Penopoulos)
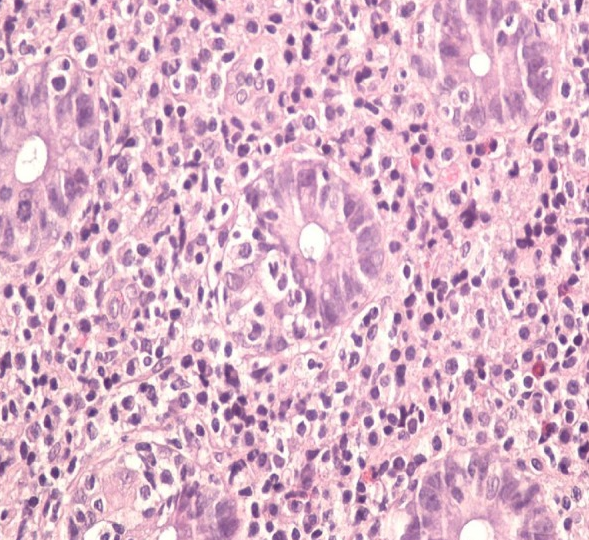
Microscopic picture showing extensive psammoma body formation (Courtesy Dr. V. Penopoulos)

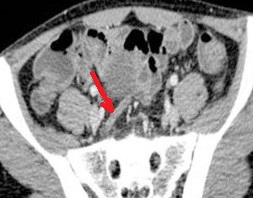
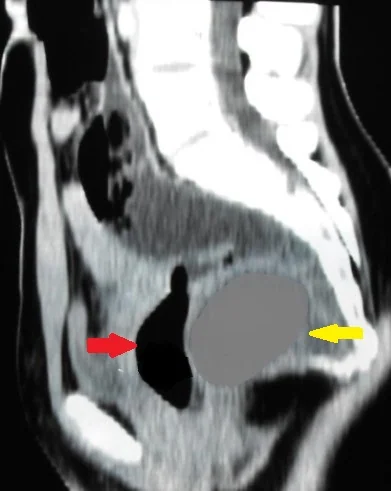
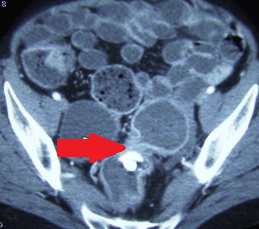
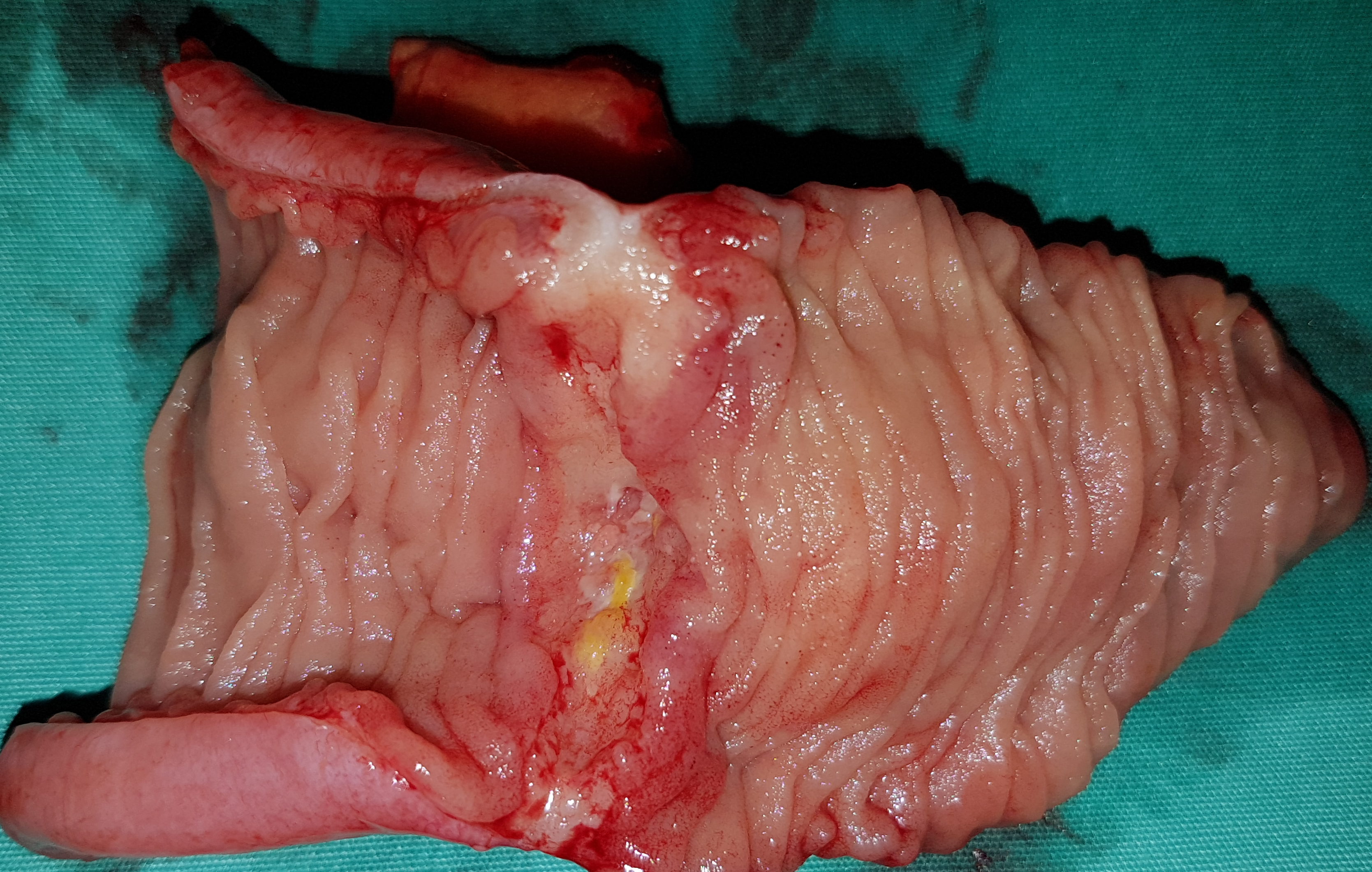
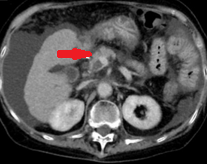
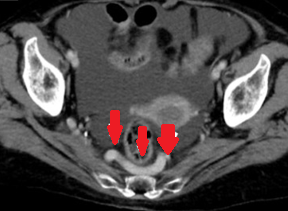
Abdominal CT Scan with contrast, showing the rectosigmoid mass with the leakage of contrast into the mesorectum at the site suspected of perforation .( Courtesy Dr . V . Penopoulos ) .
Cystography.The site of urinary leak in the dome of the bladder is obvious.( Courtesy Dr . V . Penopoulos).
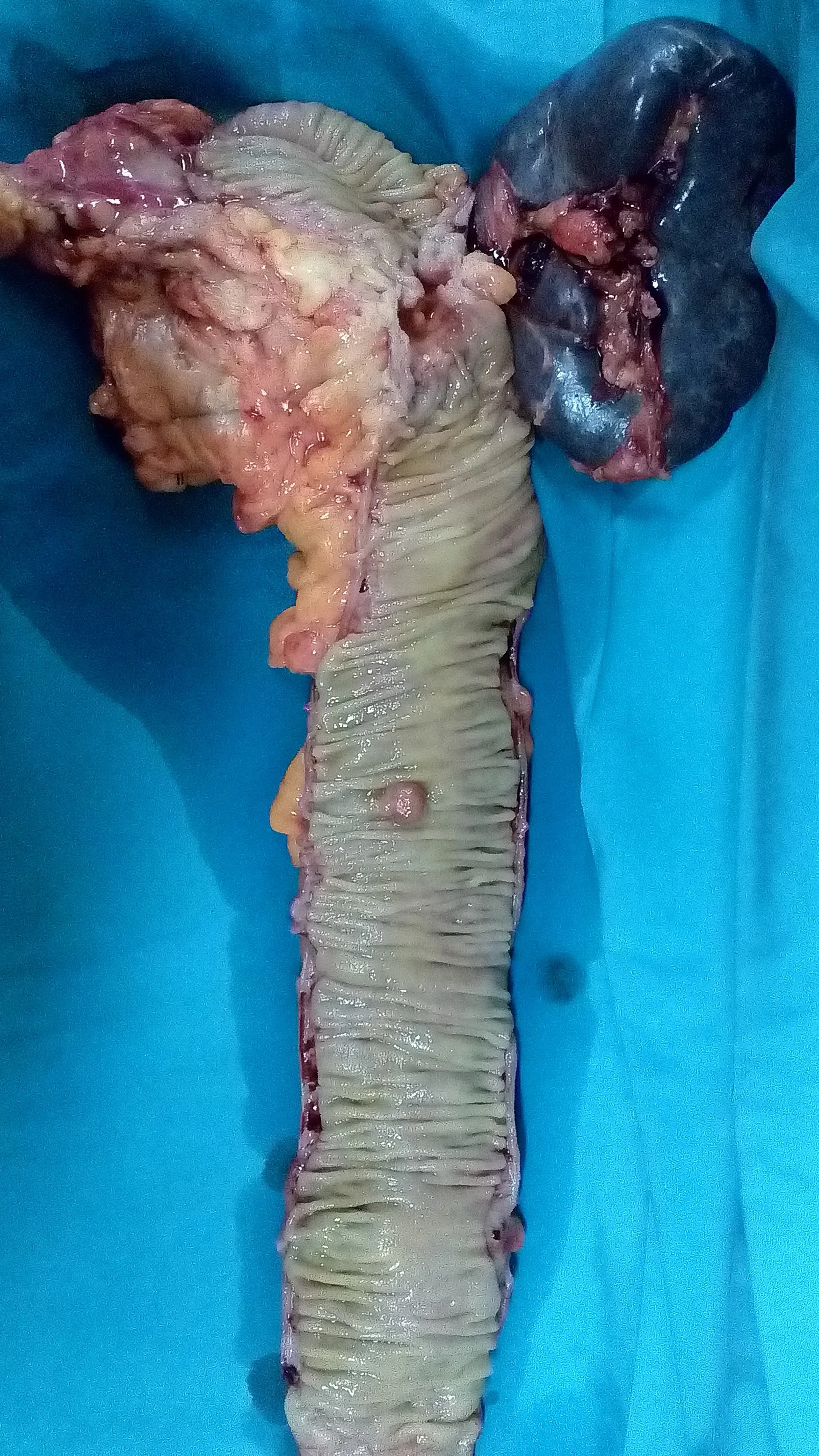
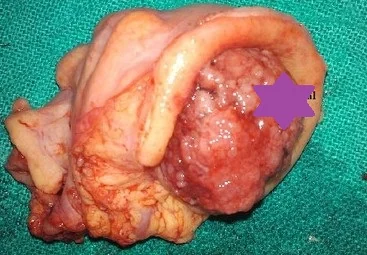
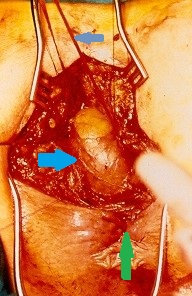
Excised specimen en bloc . Red arrow rectosigmoid adenocarcinoma . Green arrow uterus – uterine fibroids . Purple arrow , hidden left ovarian psammocarcinoma (Courtesy Dr. V. Penopoulos)
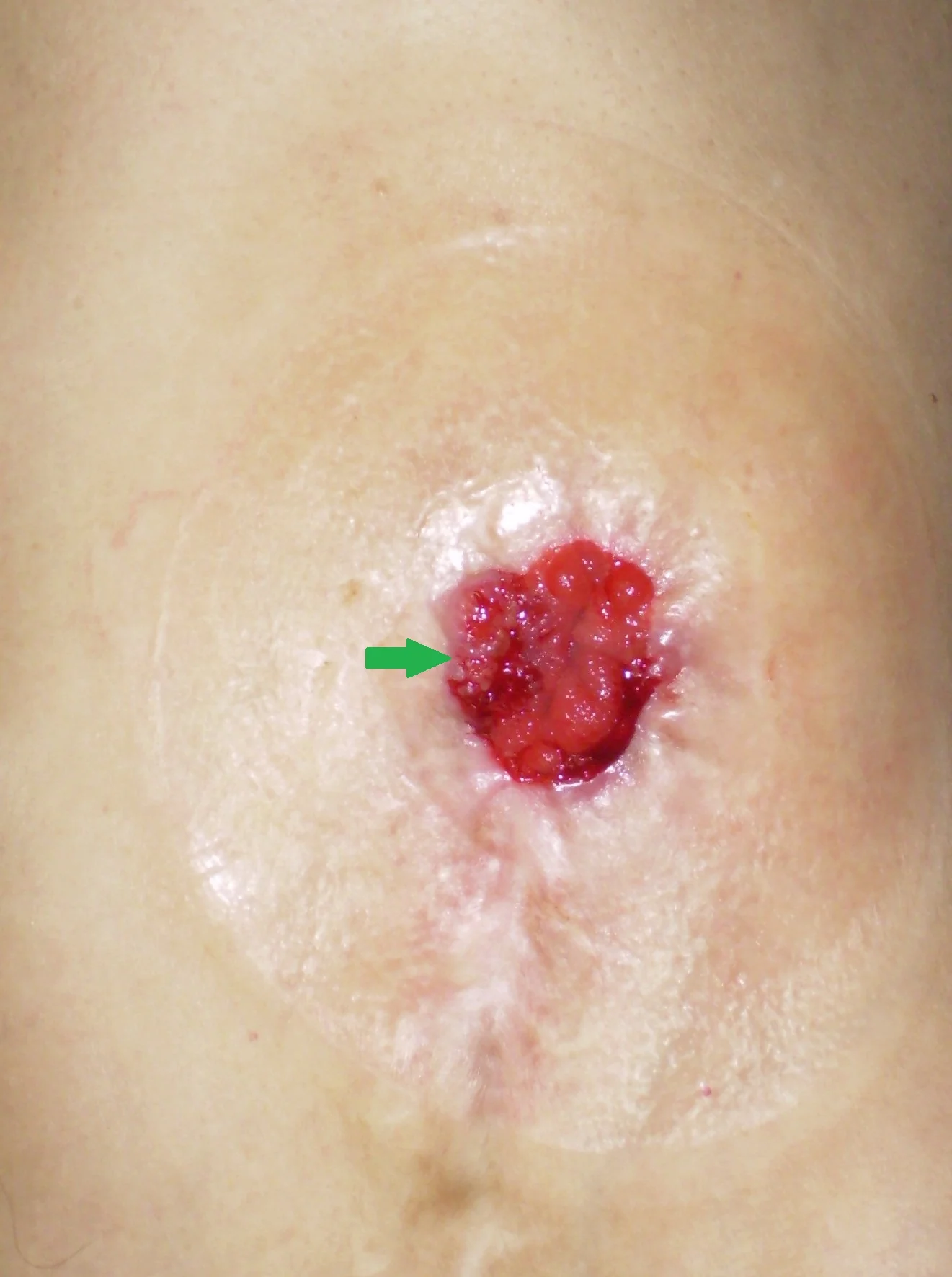
Histopathological examination showed moderate adenocarcinoma in the ascending colon and umbilical tumor .
A contrast-enhanced CT Scan showed an umbilical tumor lesion and an intraperitoneal nodule.( Courtesy Dr . V . Penopoulos ).

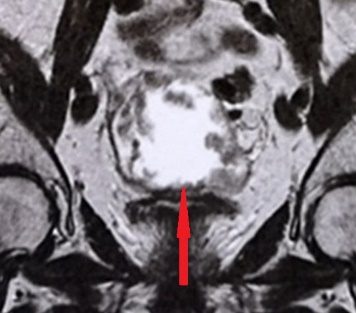
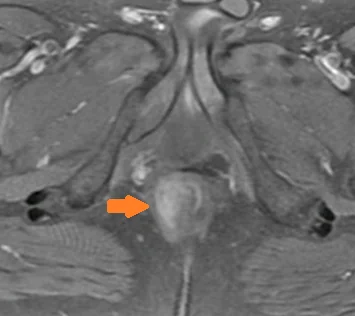
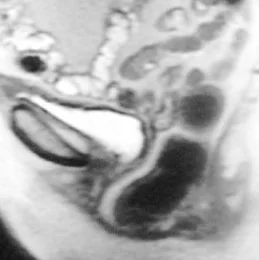
Pelvic MRI . A cystic mass is shown in the right ovary.(Courtesy Dr . V . Penopoulos).
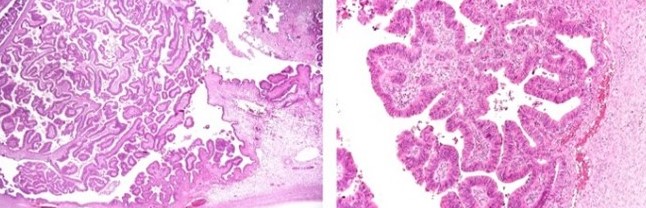
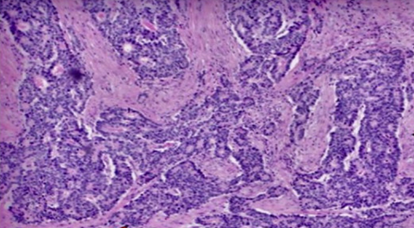
Histopathology of the ovarian tumor tissue shows solid areas consisting mainly of papillary structures and few glands that are covered by a layer of malignant epithelial cells.
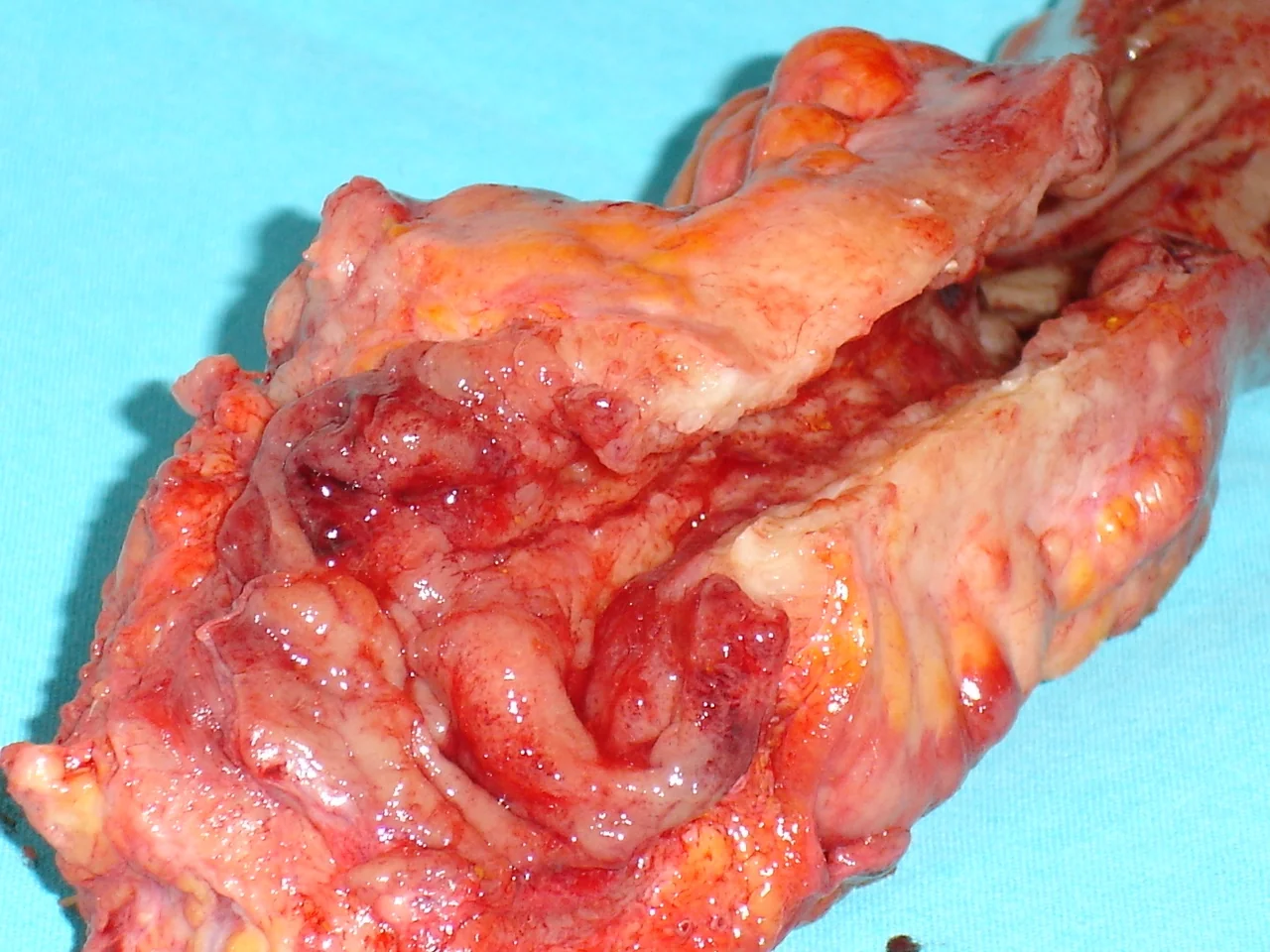
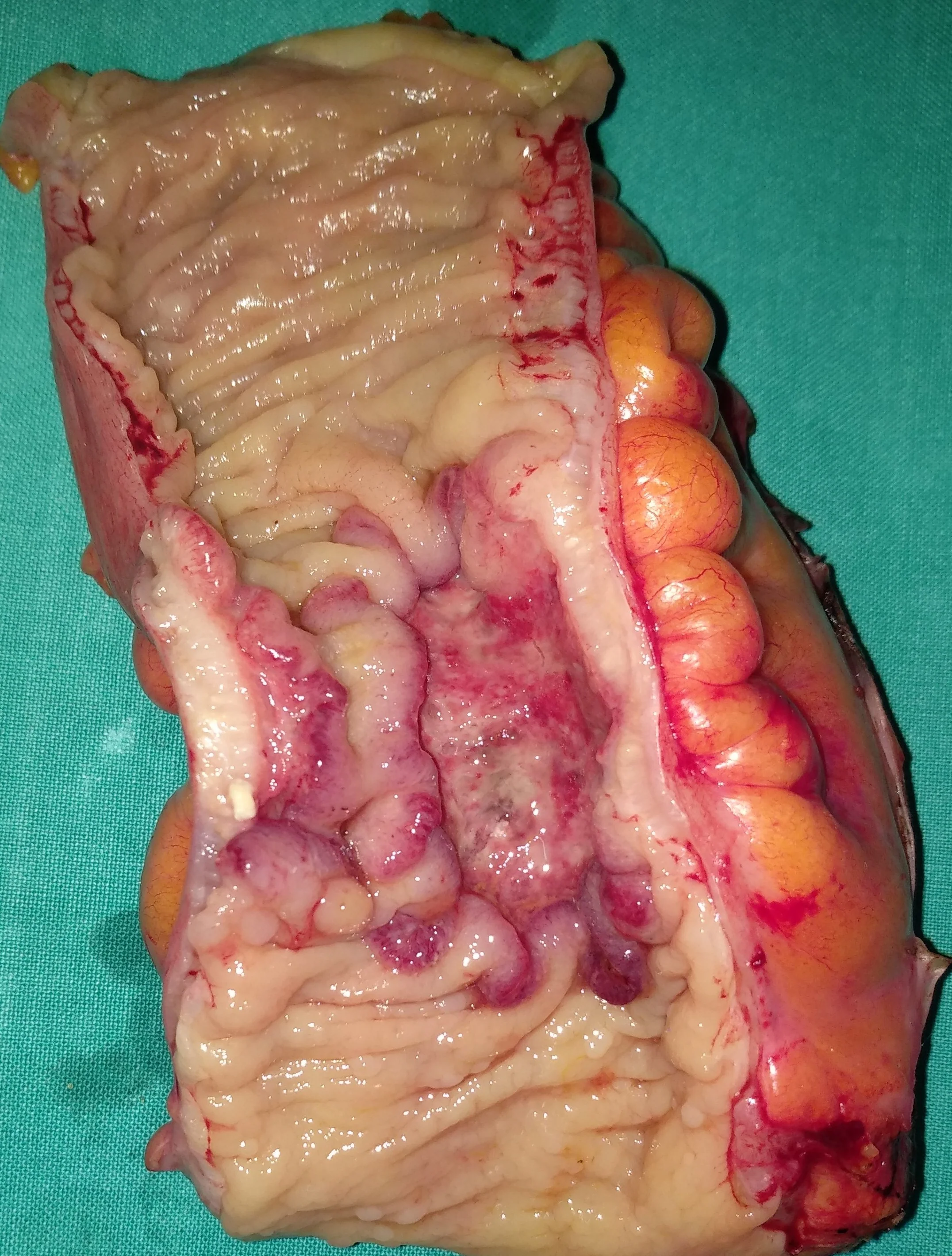
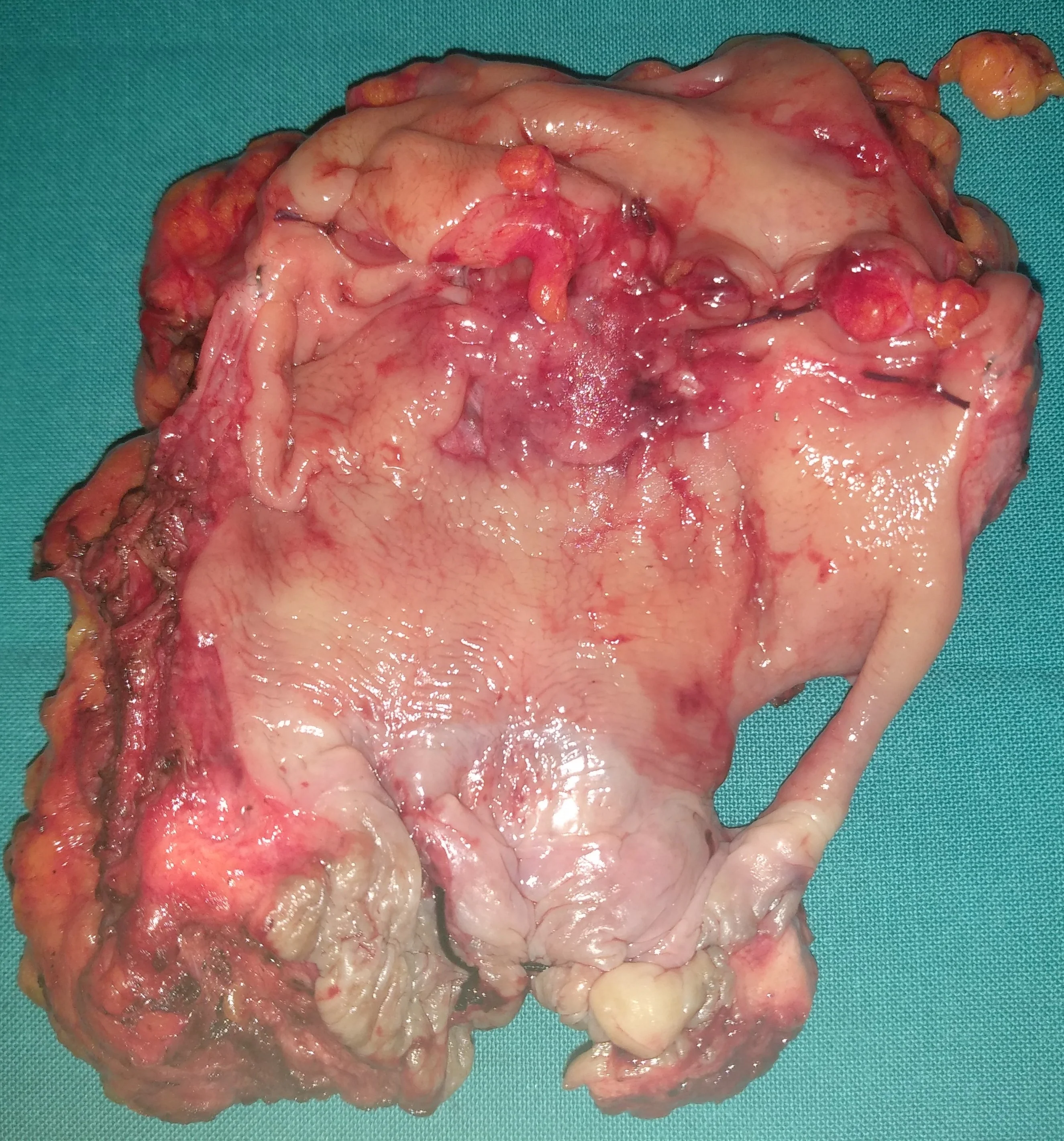
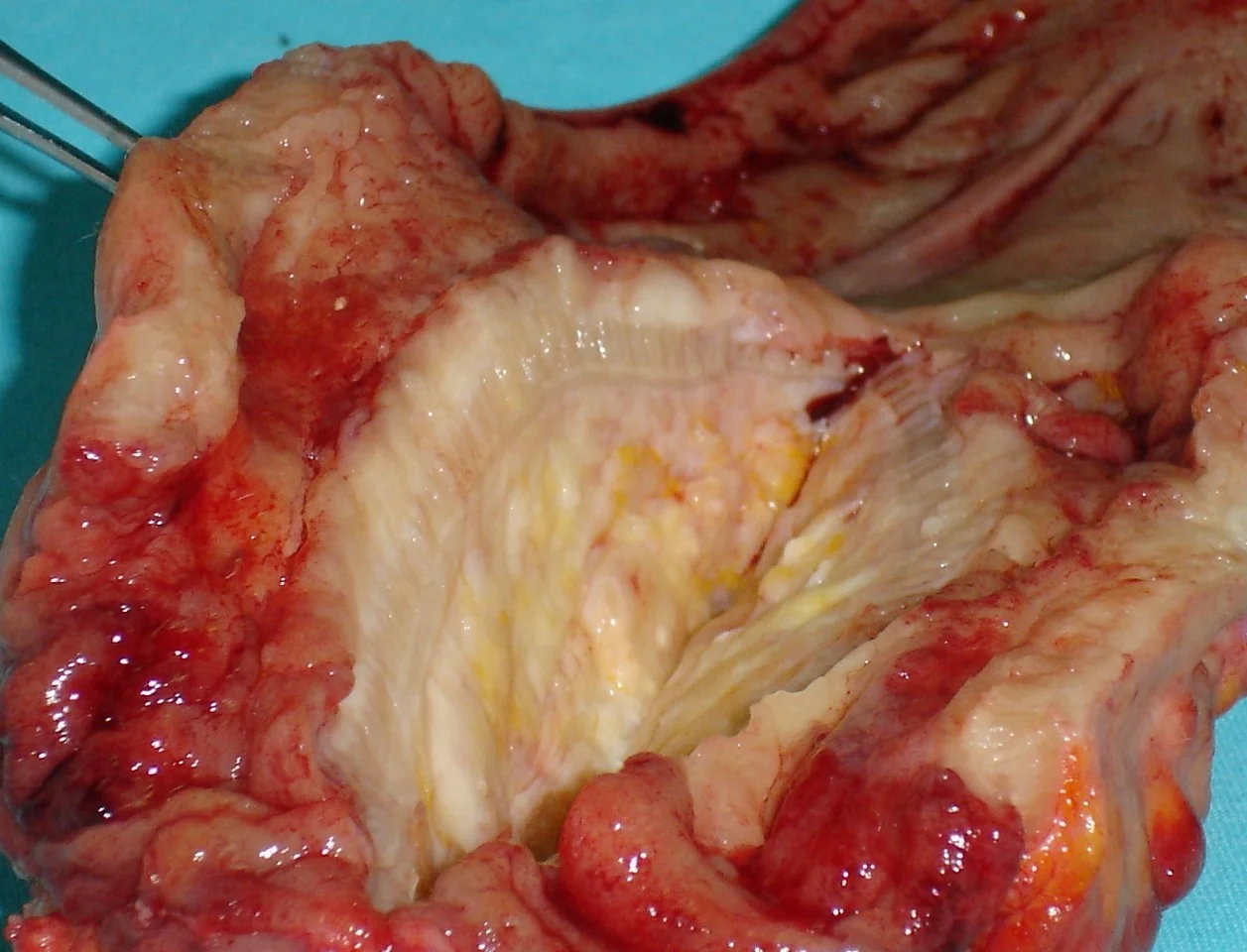
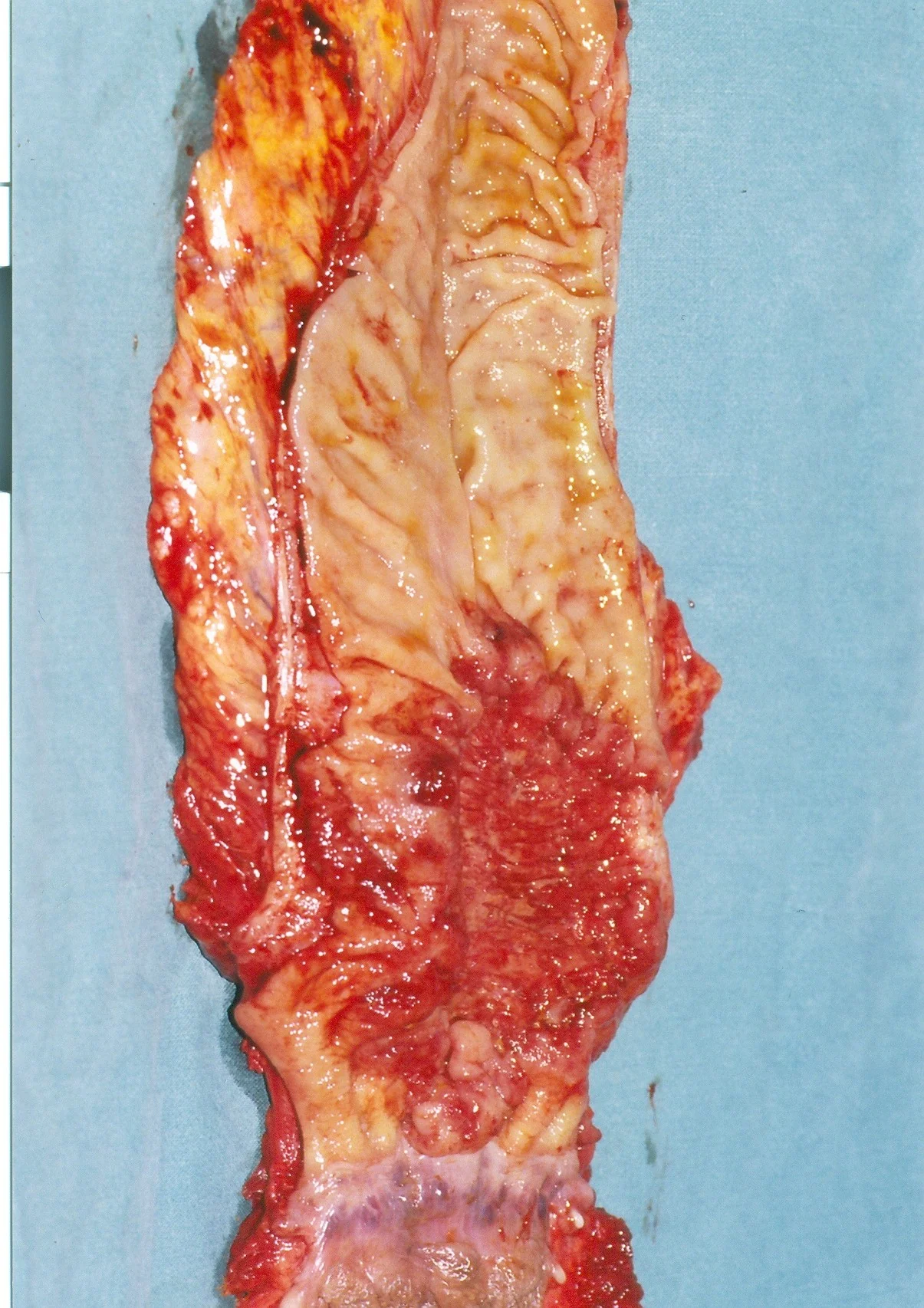
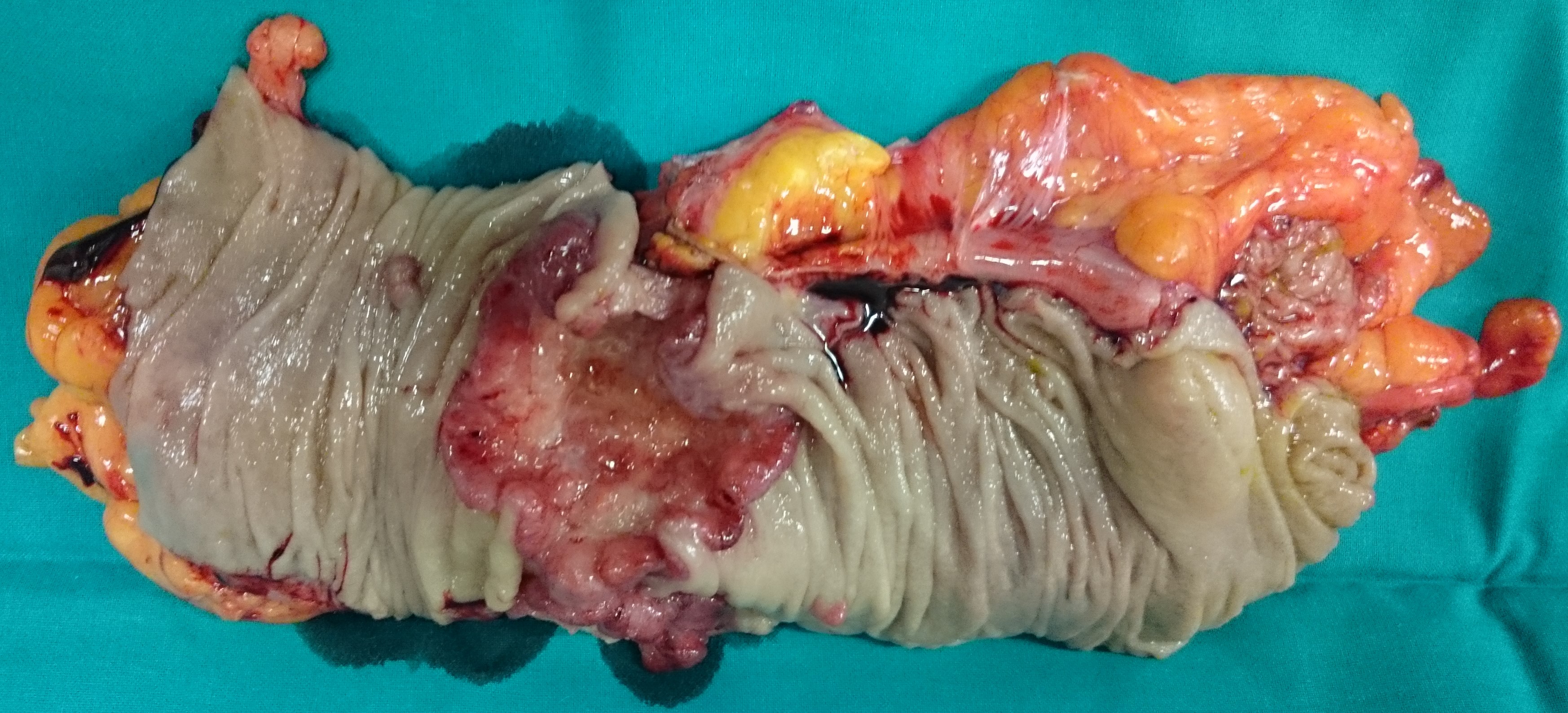
Extreme inflammation of left hemicolon secondary to diverticulitis and covered perforations (Courtesy Dr. V. Penopoulos)
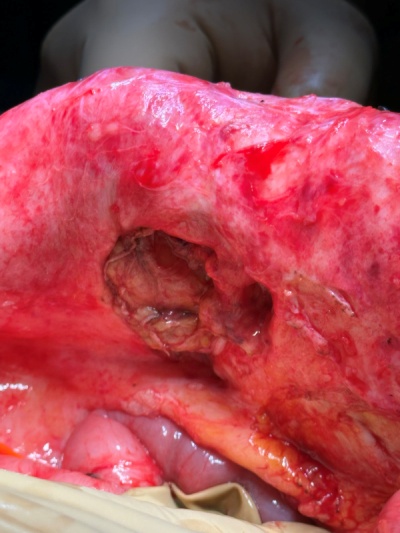
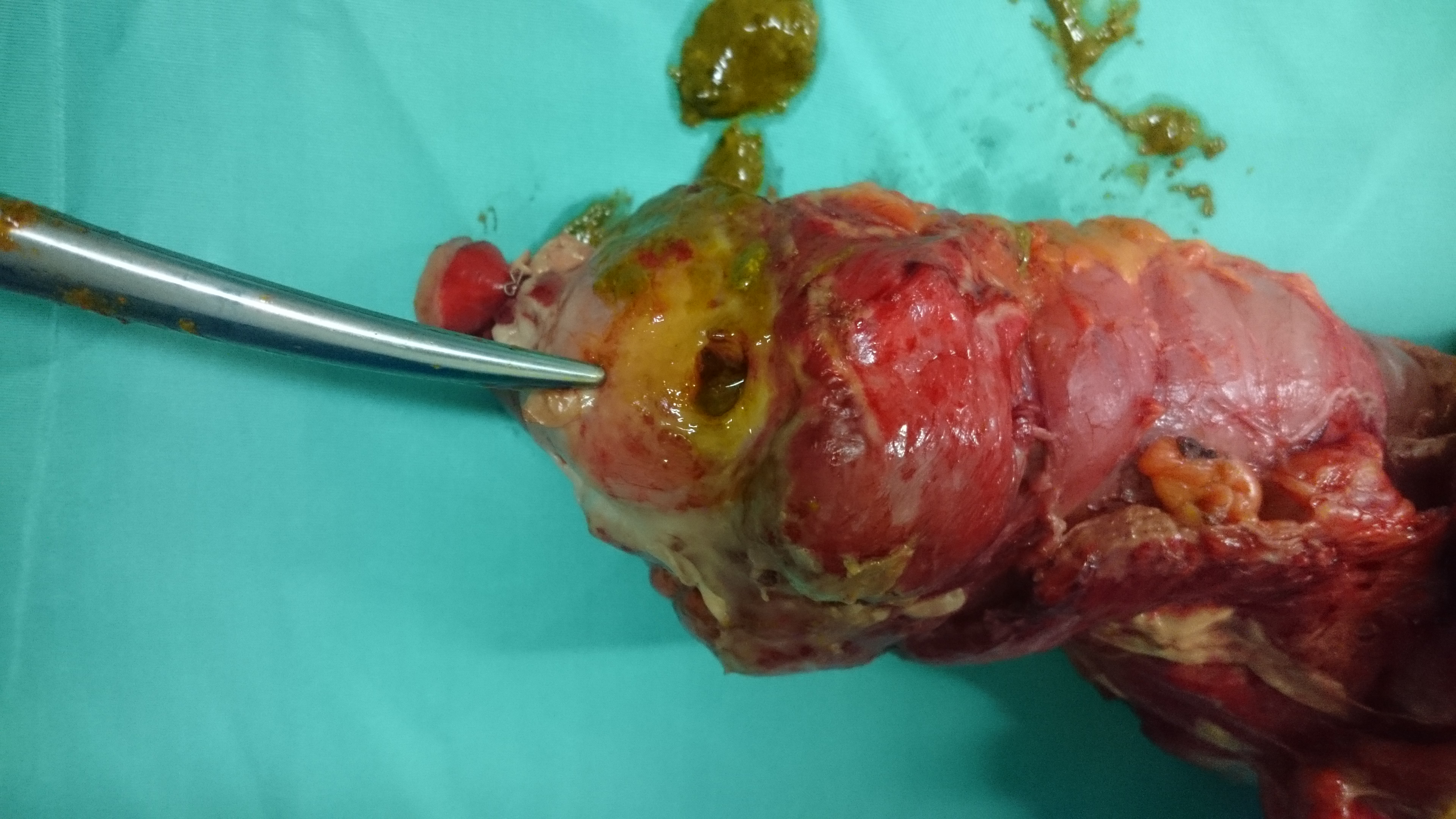
Perforation of caecum secondary to coexisting descending sigmoid colon stenosis obstruction (Courtesy Dr. V. Penopoulos)

Extreme inflammation of left hemicolon secondary to diverticulitis and covered perforations (Courtesy Dr. V. Penopoulos)

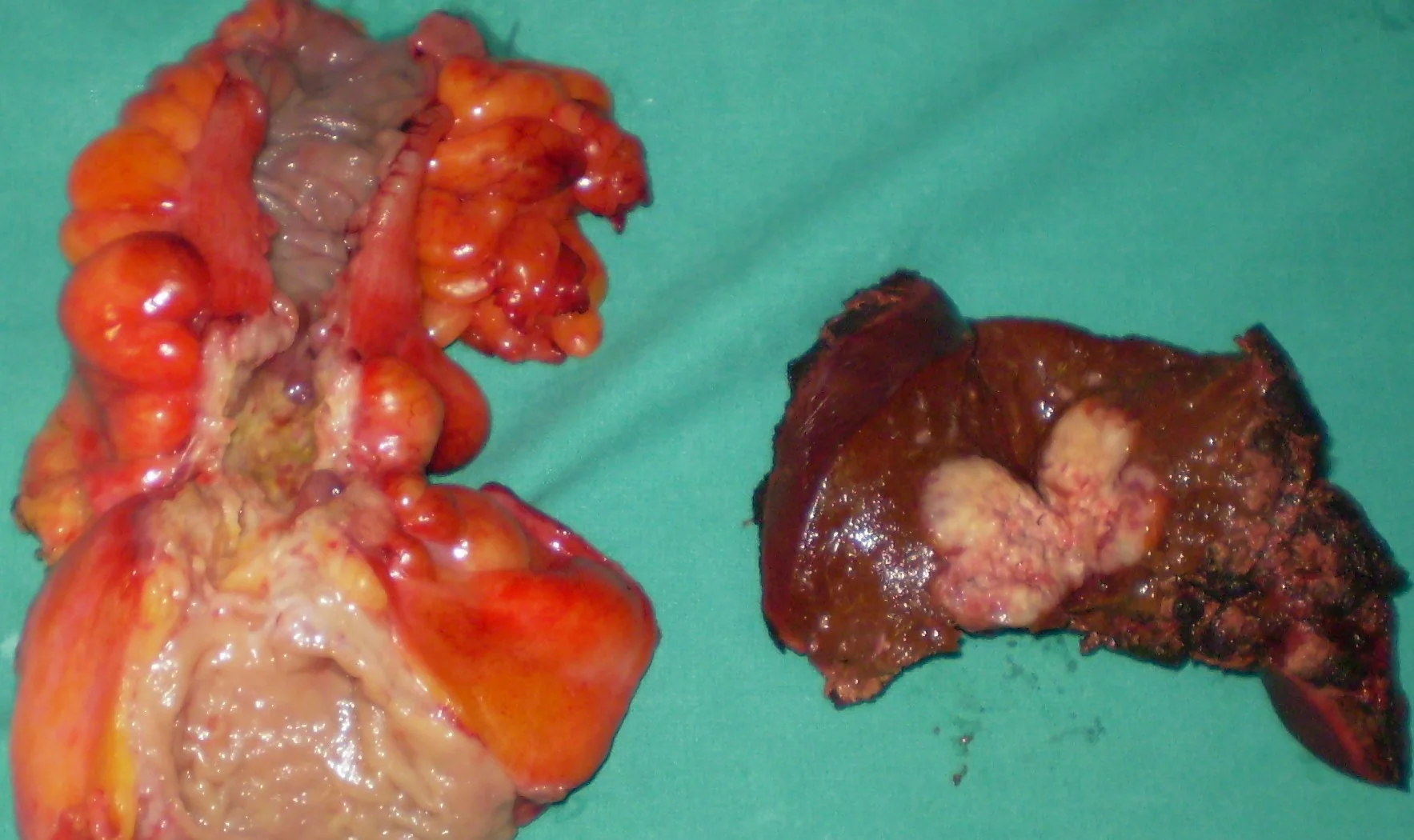
Green arrows-Synchronous colonic adenocarcinomas.Yellow arrow-Hydatid cyst.(Courtesy Dr.V.Penopoulos).

Mini right hemicolectomy specimen.Cecal necrosis-perforation.(Courtesy Dr.V.Penopoulos).

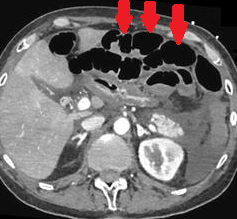
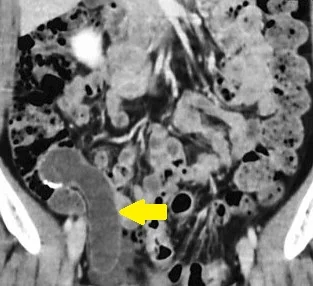
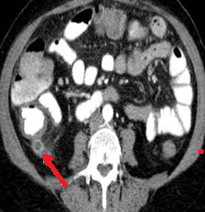
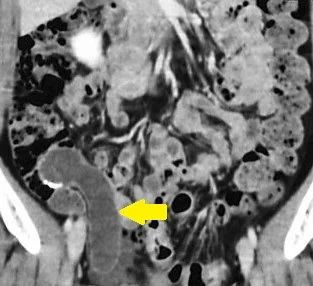
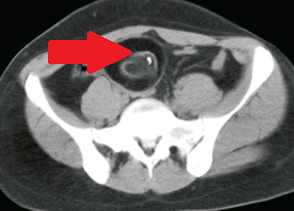
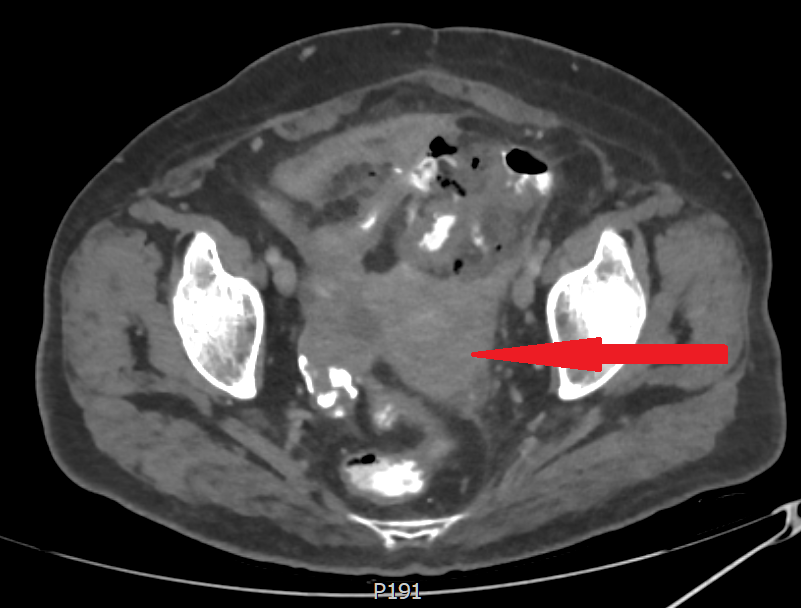
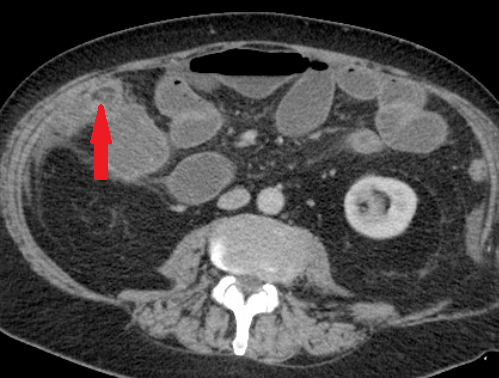
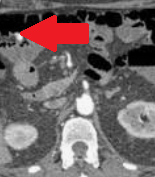
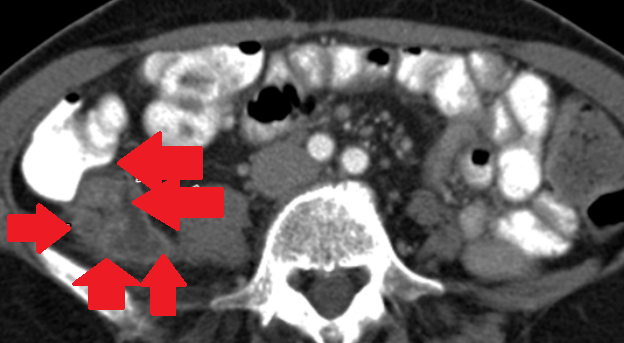
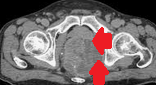
Abdominal CT. Red arrow — Typhlitis. Significant cecal wall thickening (Courtesy Dr. V. Penopoulos)

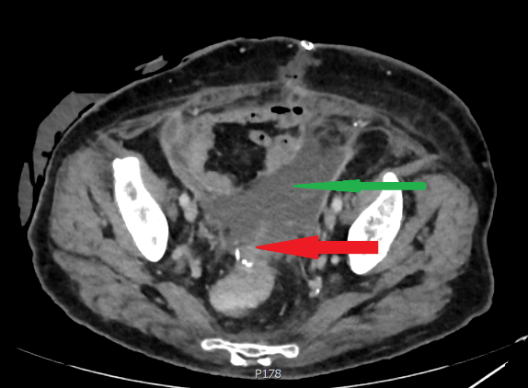
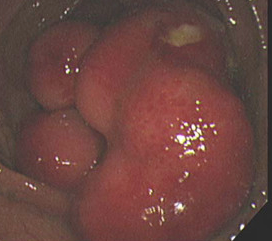
Blue arrow - Uterus. Green arrow - Sigmoid colon.Uterocolic fistula.(Courtesy Dr. V. Penopoulos).

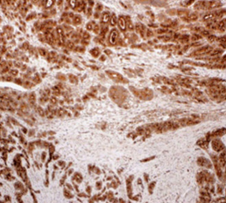
Immunohistochemical examination. Positivity for Chromogranin B (Courtesy Dr. V. Penopoulos).



Histological findings of mucinous cystadenoma of the appendix. Cylindrical epithelium and mucin production. Note the absence of atypia and mitotic figures
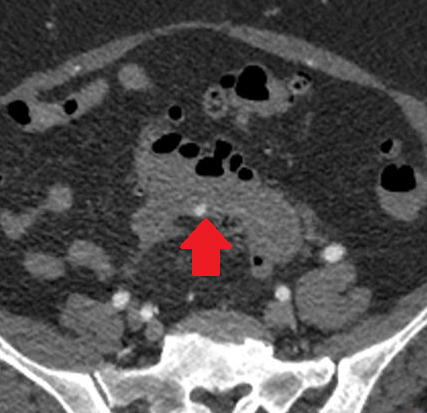




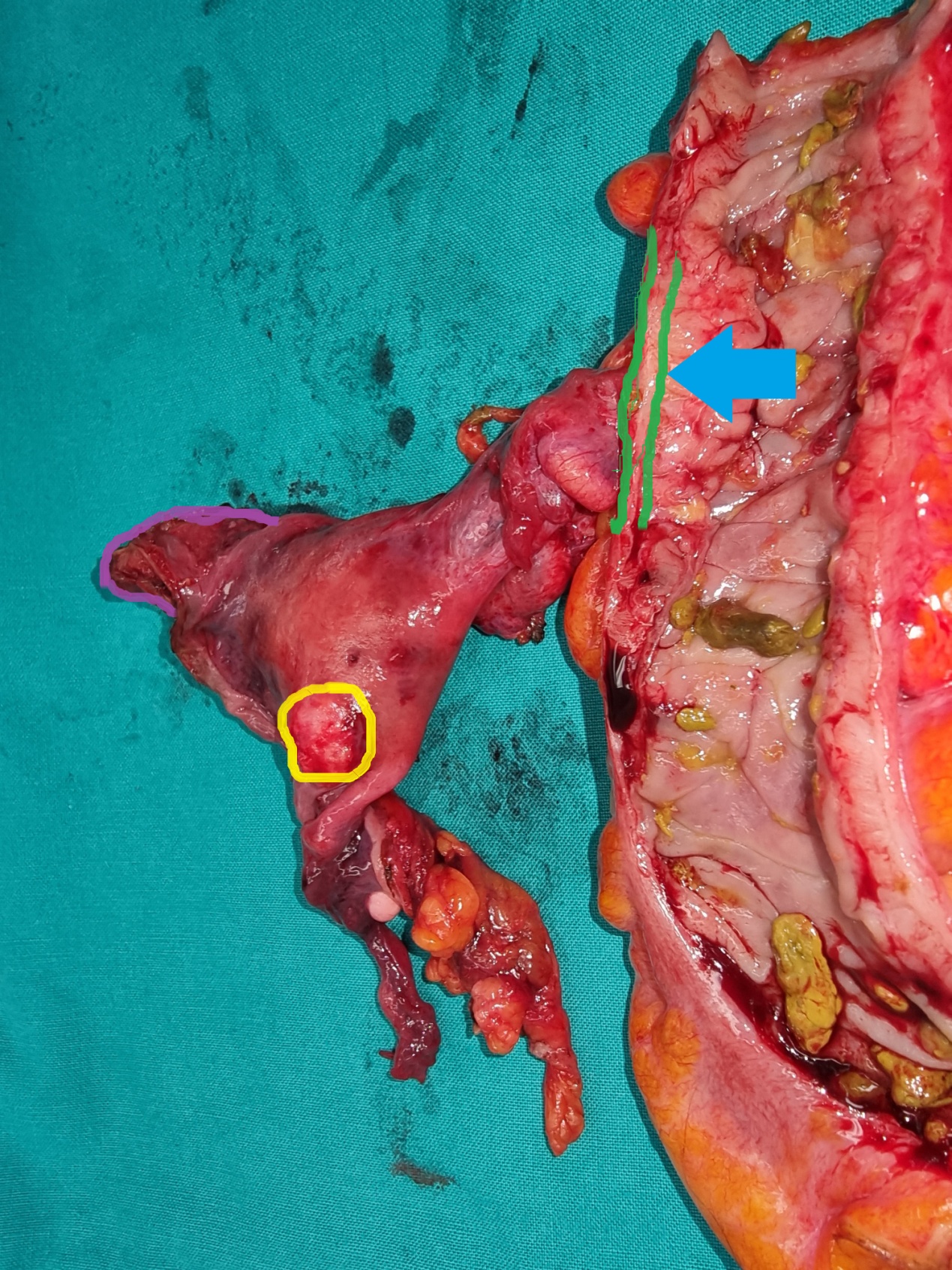
En bloc rectosigmoidectomy plus total hysterectomy. Blue arrow: Utero-colic fistula. Yellow circle: Uterine leiomyoma (Courtesy Dr. V. Penopoulos).


Right hemicolectomy specimen. The cecal neoplasm is clearly visible (Courtesy Dr. V. Penopoulos).
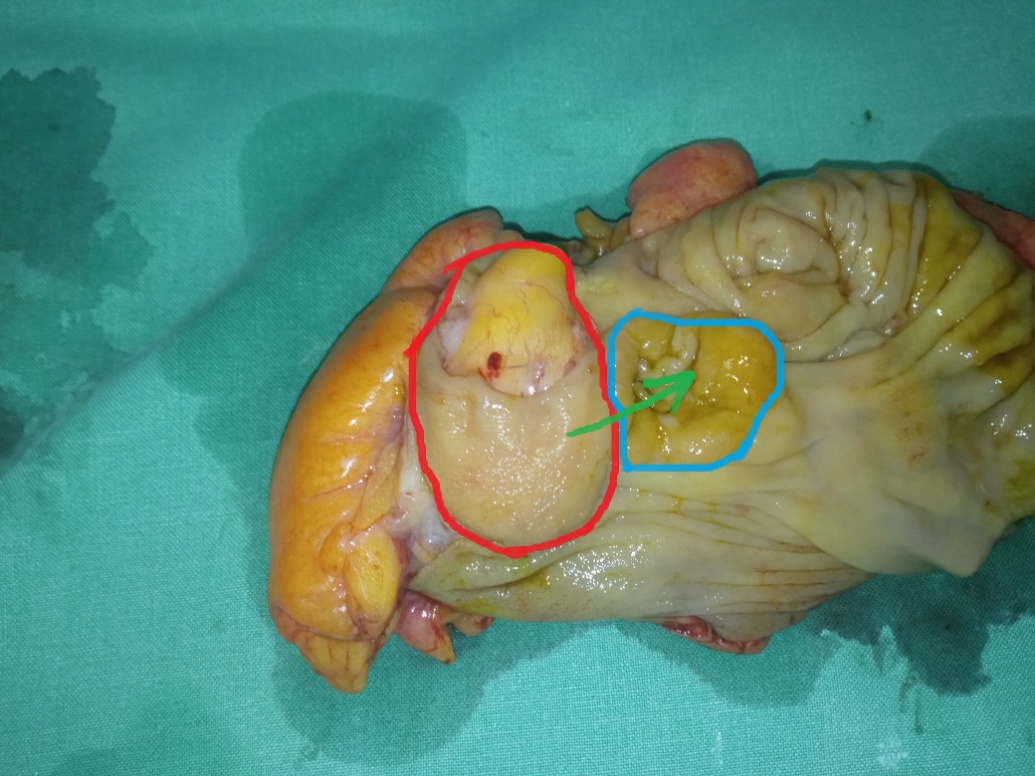
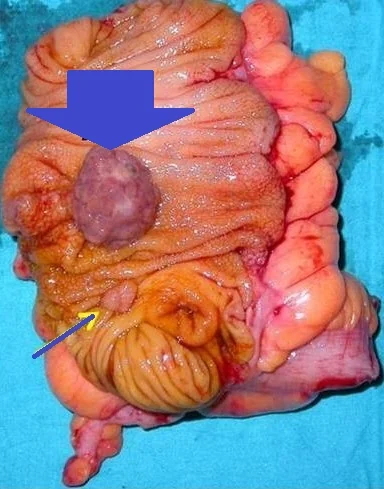
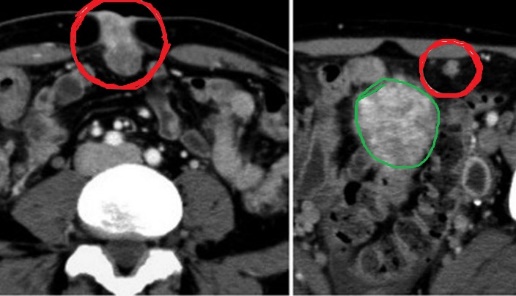
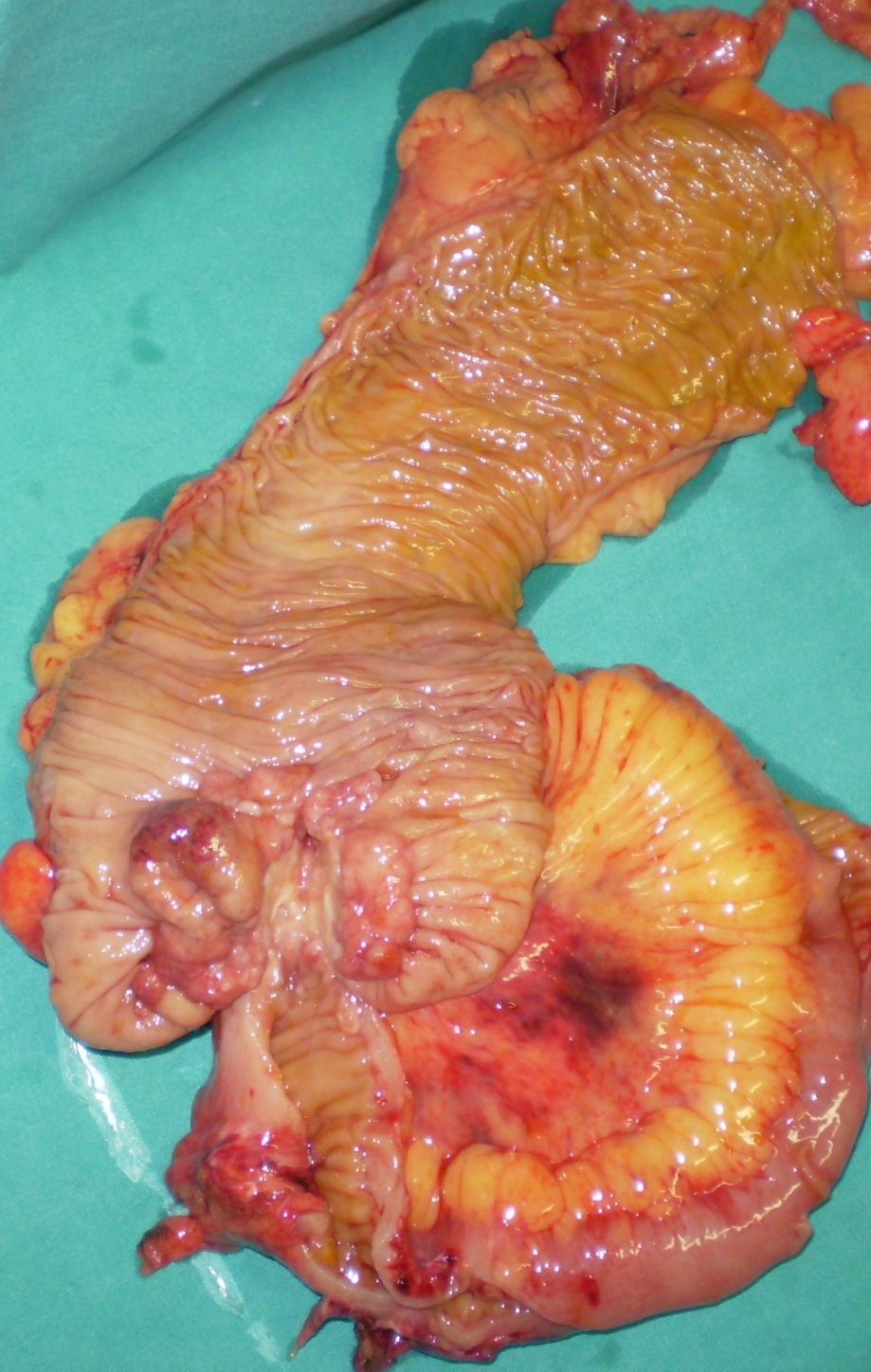
Mini right hemicolectomy specimen. Red outline: lipoma. Blue outline: ileocecal valve. Green arrow: shows the course of the lipoma, resulting in complete obstruction of the ileocecal valve (Courtesy Dr. V. Penopoulos)
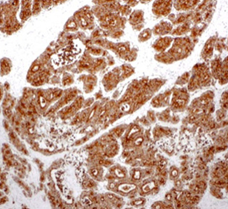
Immunohistochemical examination. Positivity for Synaptophysin (Courtesy Dr. V. Penopoulos).

Red arrow - Bleeding diverticulum of the transverse colon (Courtesy Dr. V. Penopoulos)
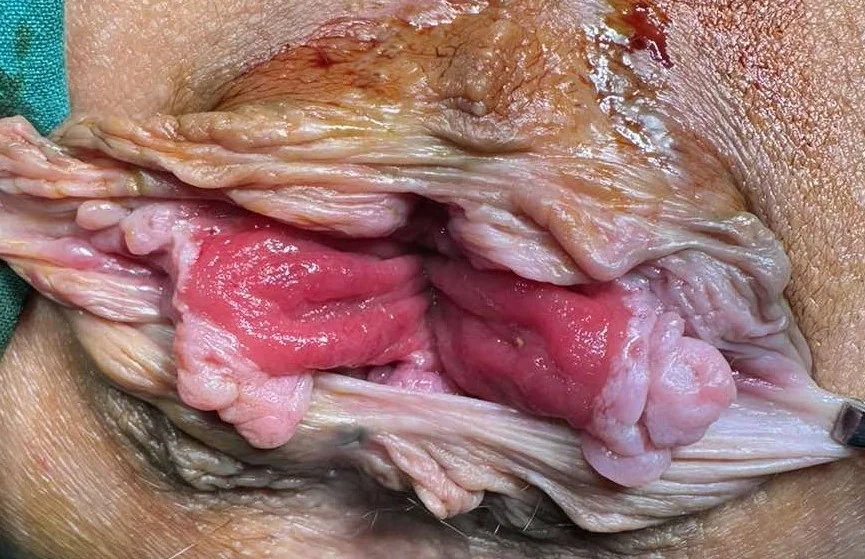
Green arrow - Internal and Yellow arrow external sphincters following meticulous dissection (Courtesy Dr. V. Penopoulos)

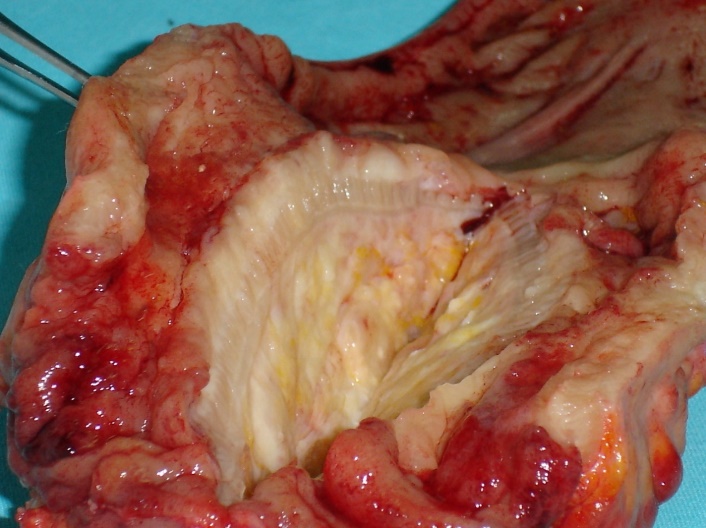
Figure 4 . Large Cell Neuroendocrine-Adenocarcinoma Mixed Tumour of Colon. . ( Courtesy Dr . V . Penopoulos ) .
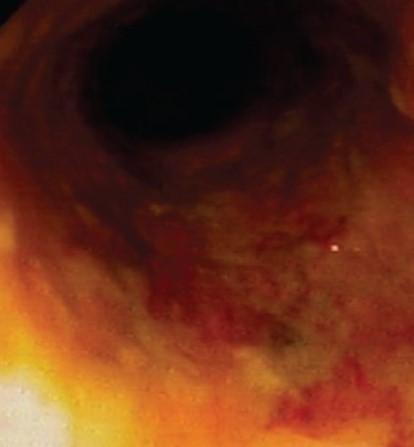



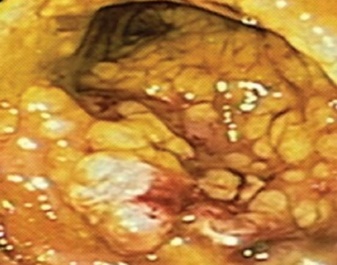


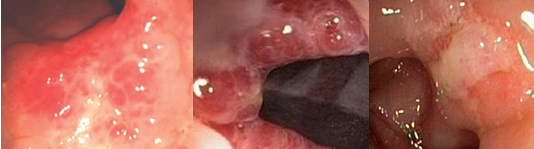
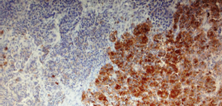
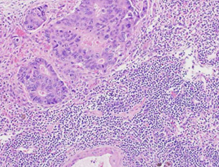
Figure 2 . Large cell neuroendocrine carcinoma, positive for Chromogranin A, and moderately differentiated adenocarcinoma in a collision pattern.
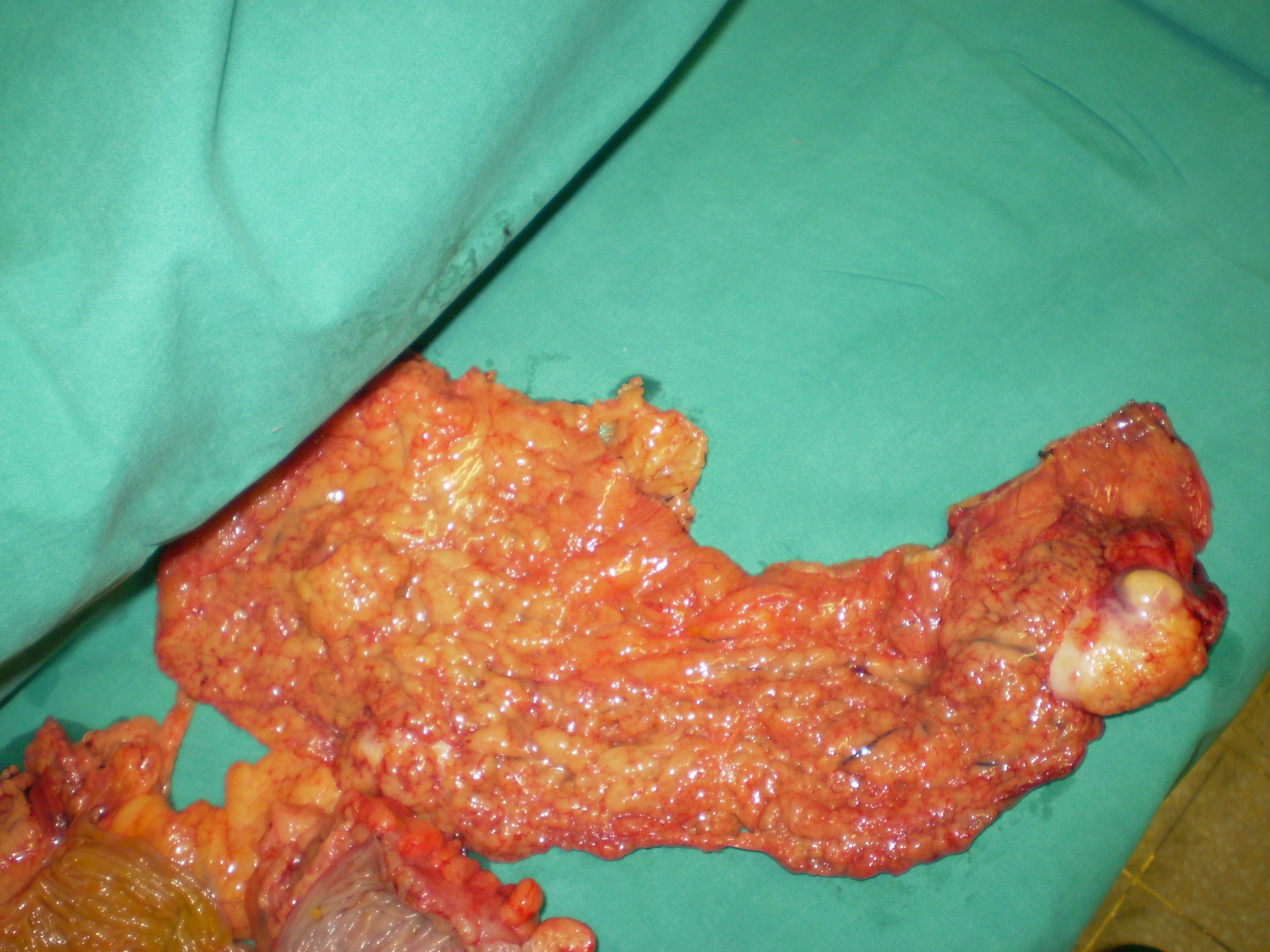
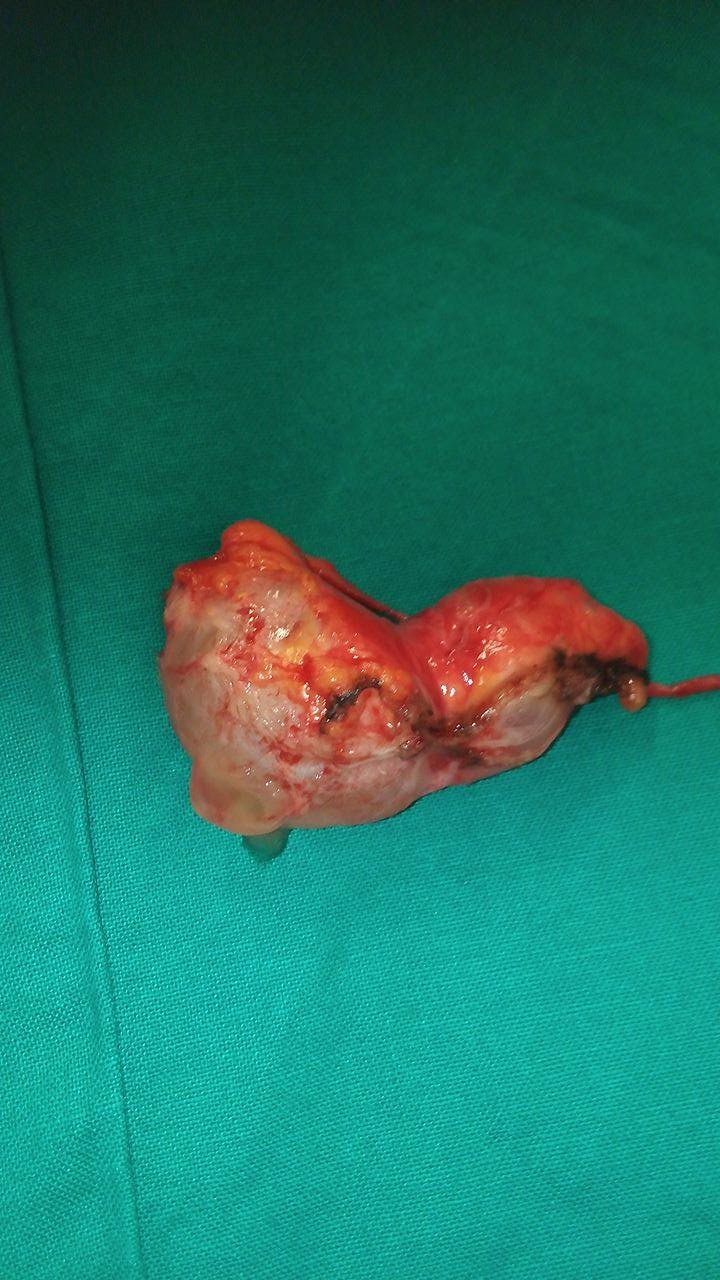
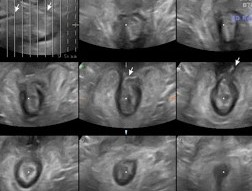
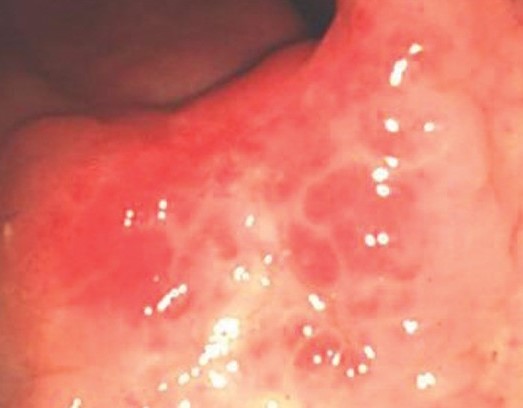
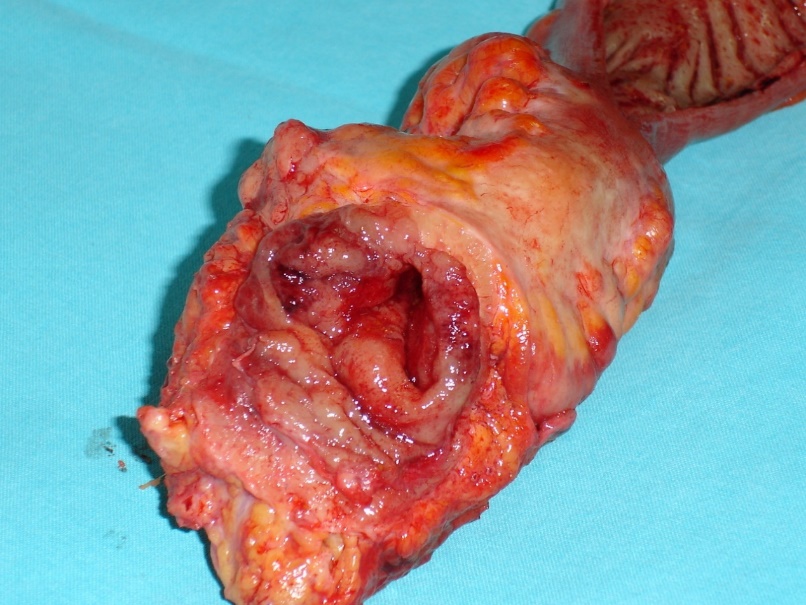
Figure 3 . Large Cell Neuroendocrine-Adenocarcinoma Mixed Tumour of Colon. . ( Courtesy Dr . V . Penopoulos ) . - Colectomy specimen . ( Courtesy Dr . V . Penopoulos ) .
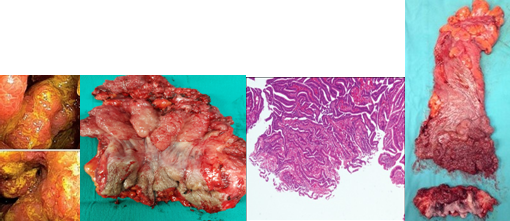
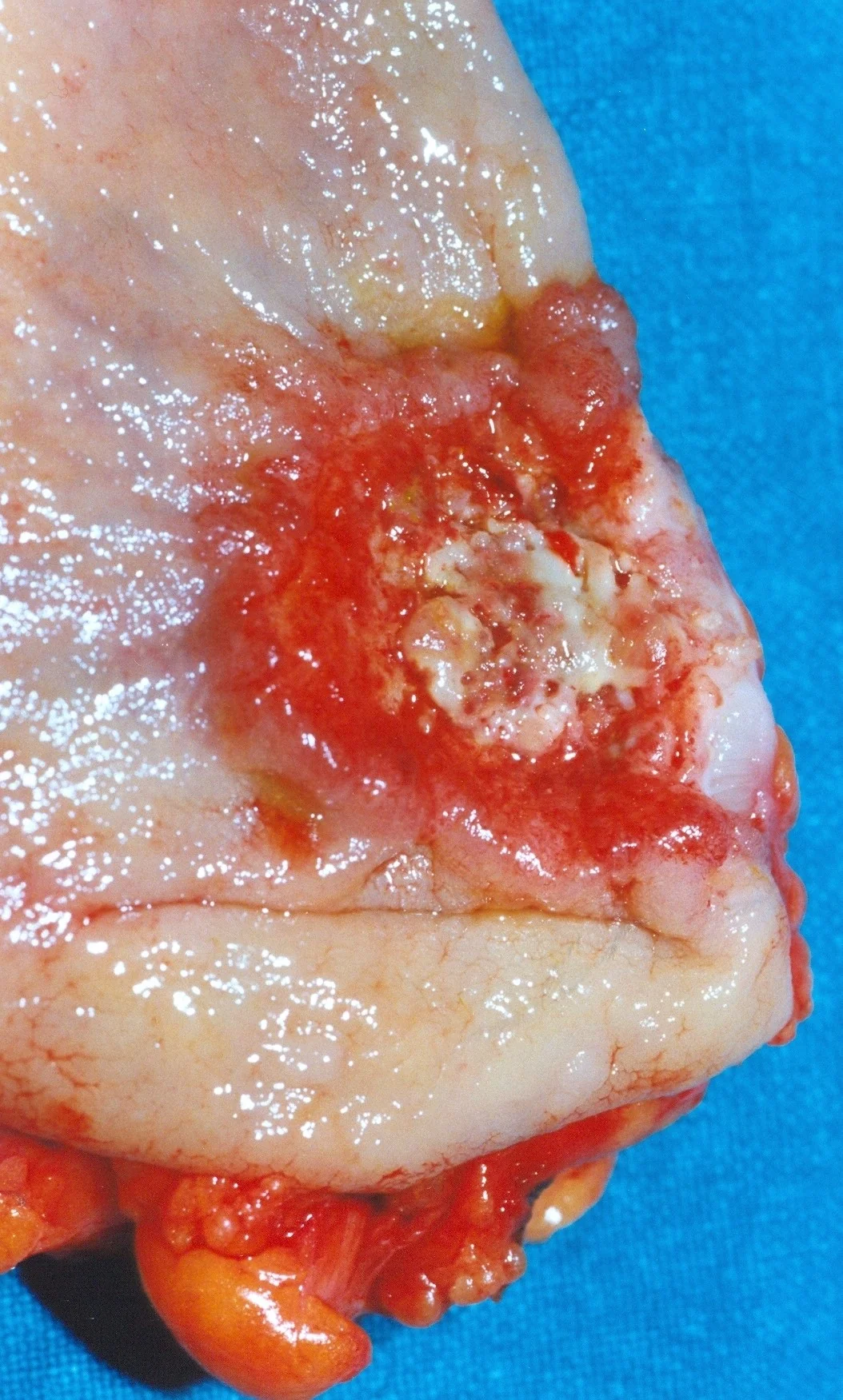
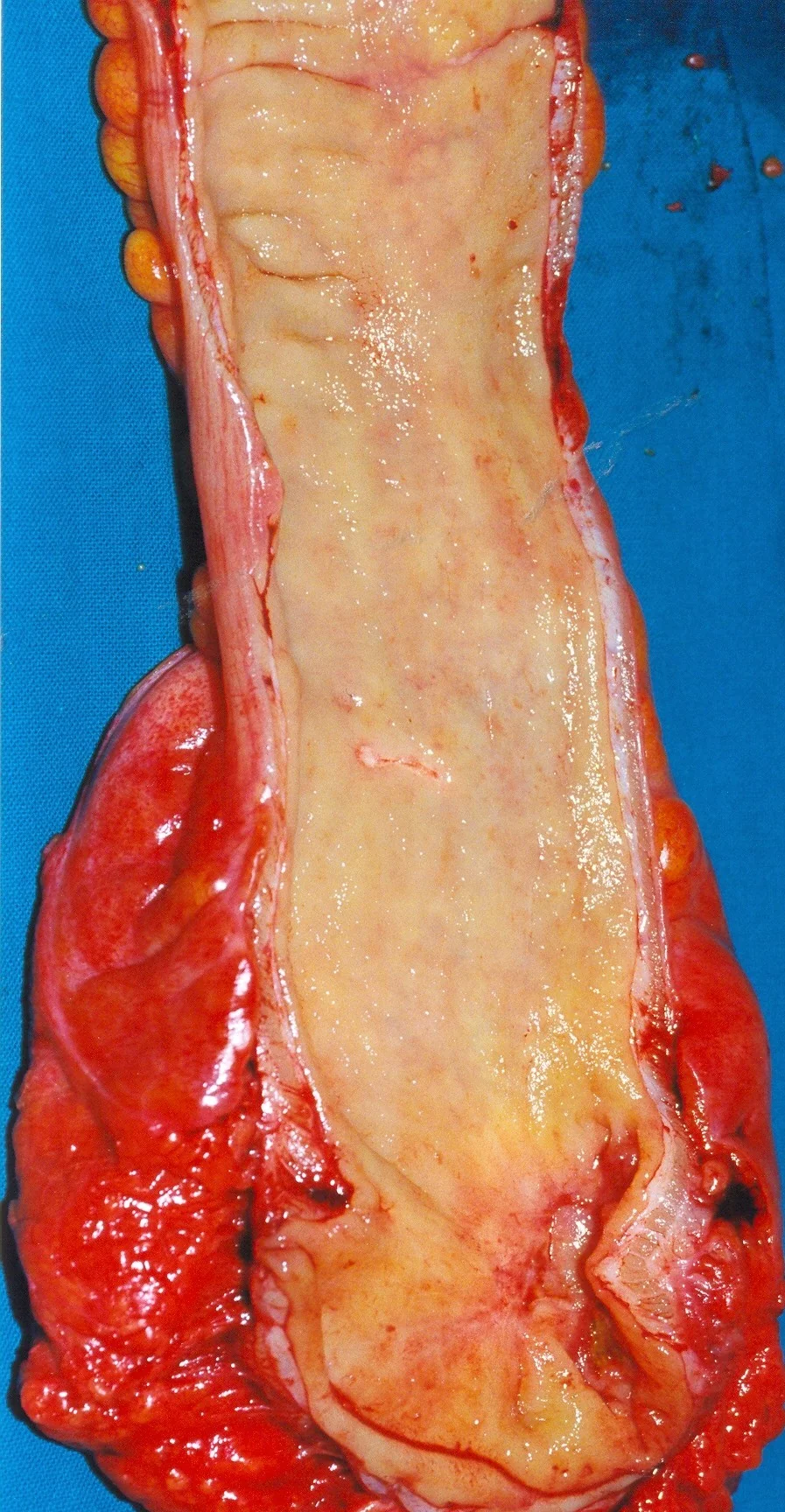
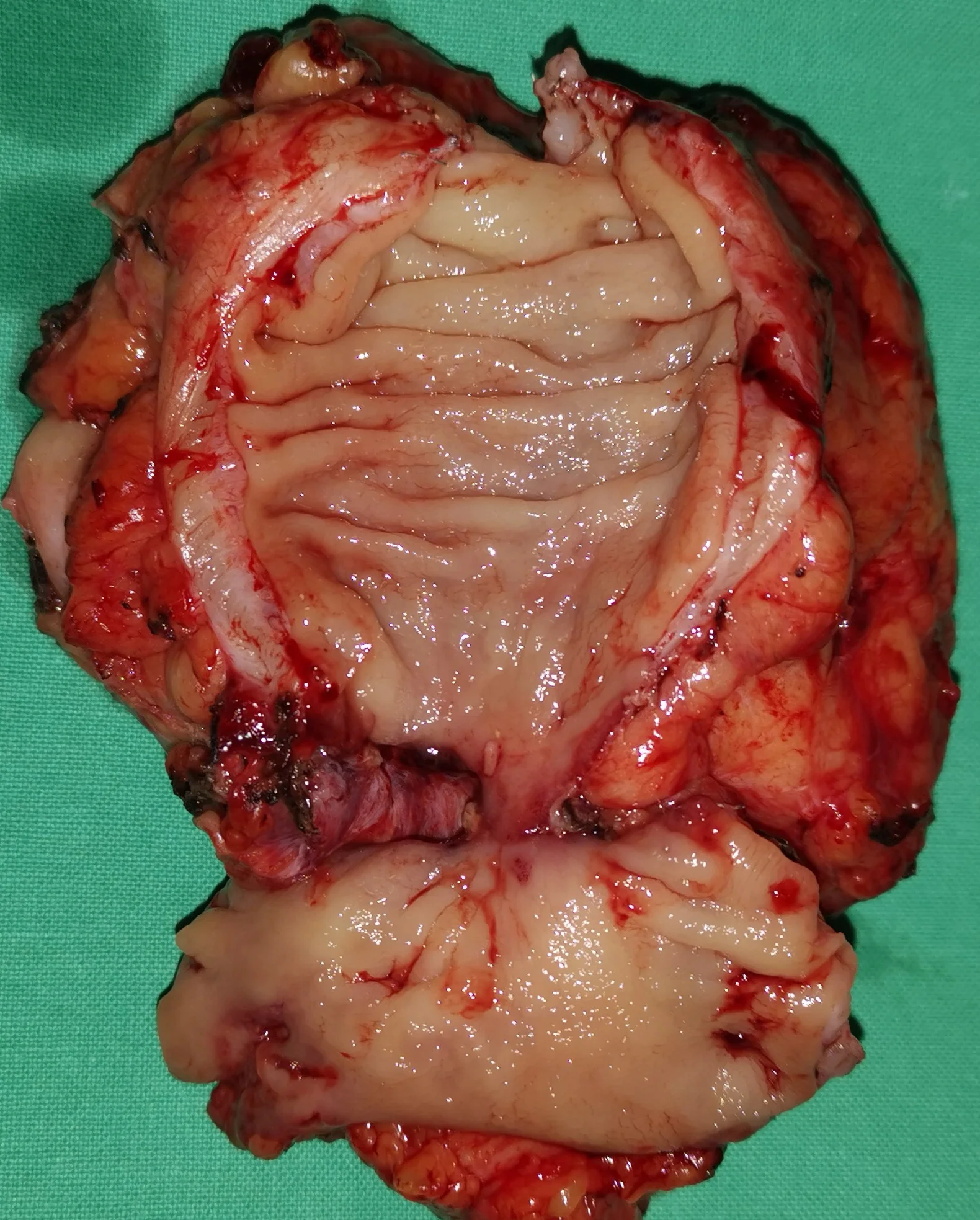
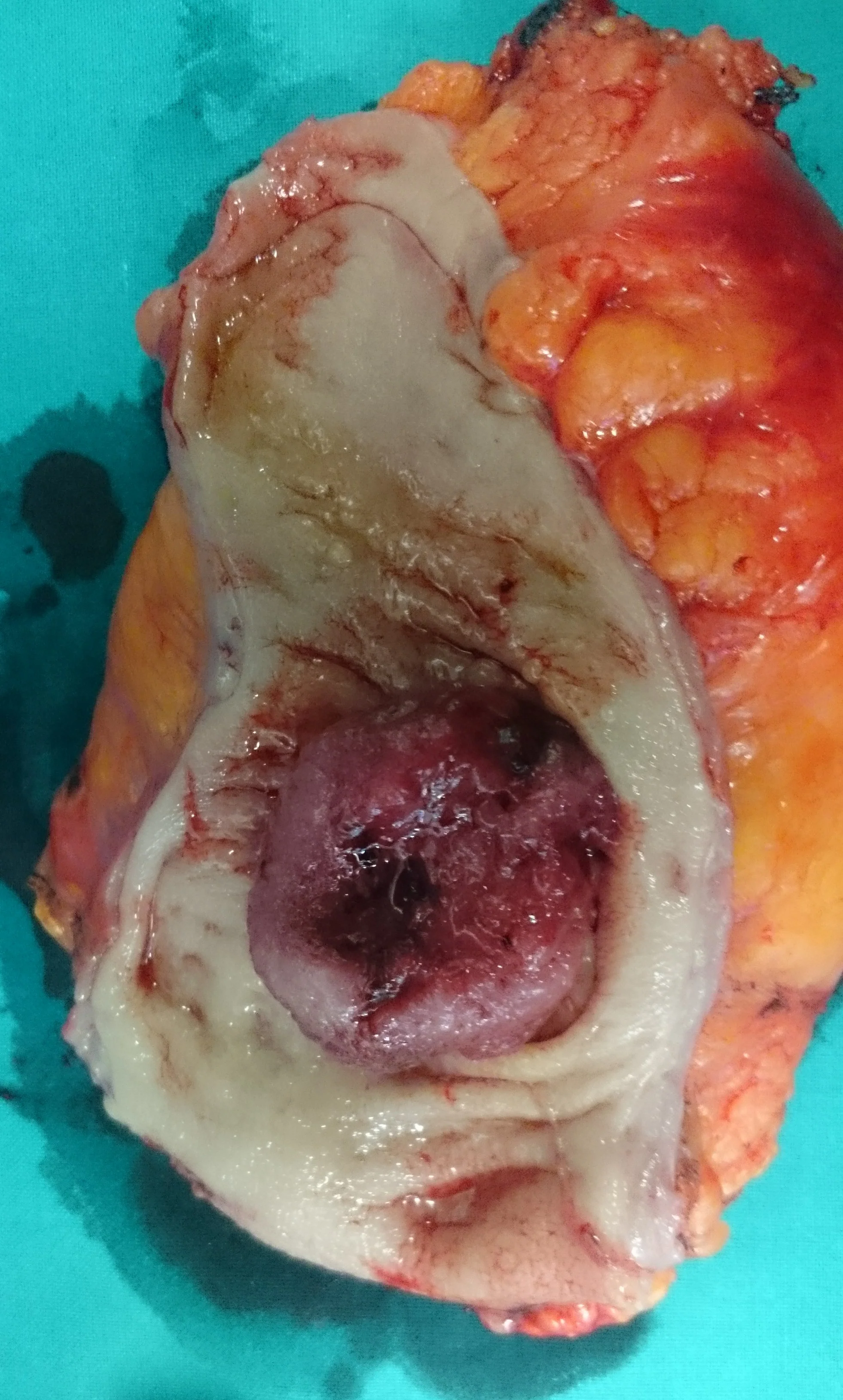
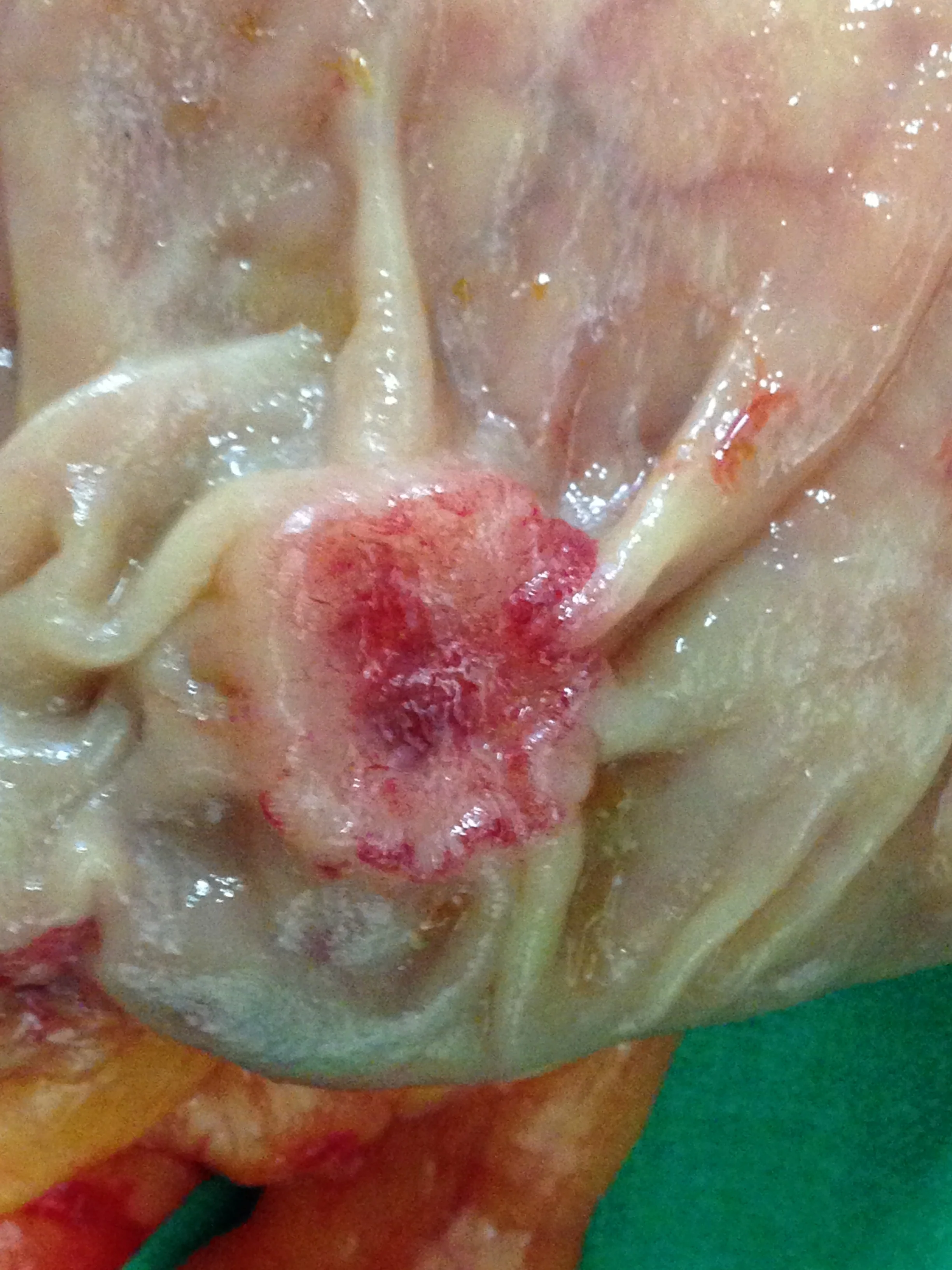
Figure 1 . Giant villous adenoma fully excised with AP resection . ( Courtesy Dr . V . Penopoulos ) .





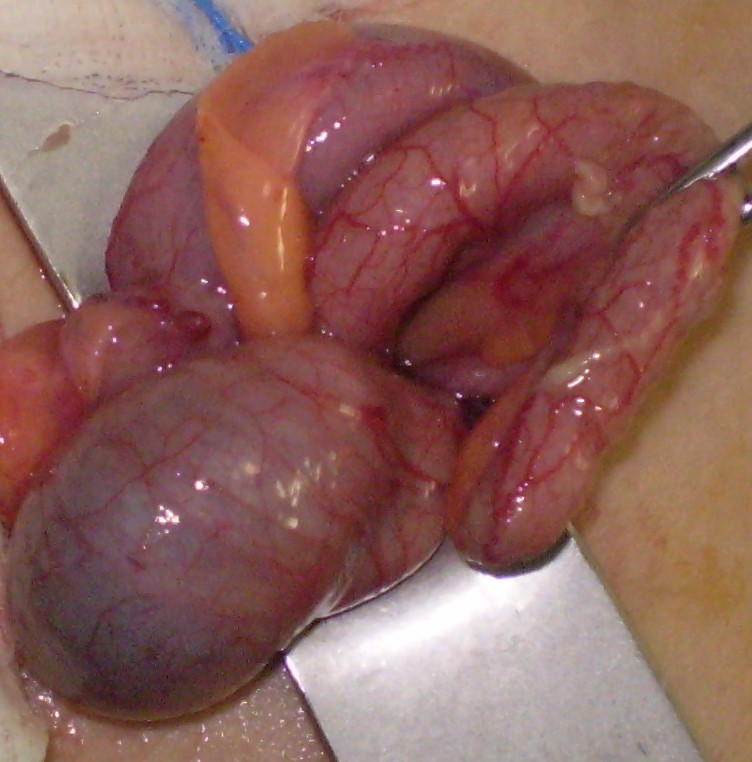
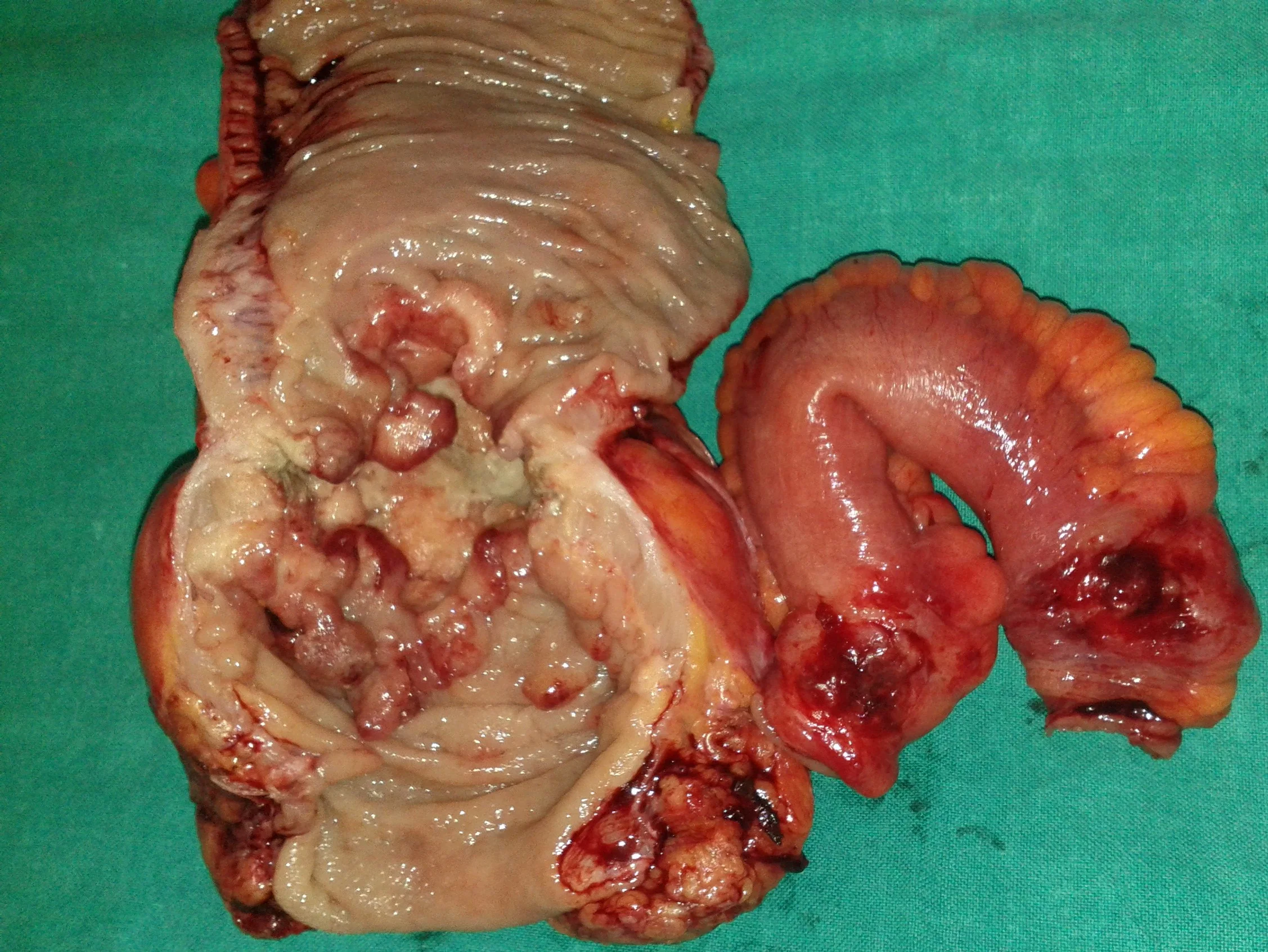
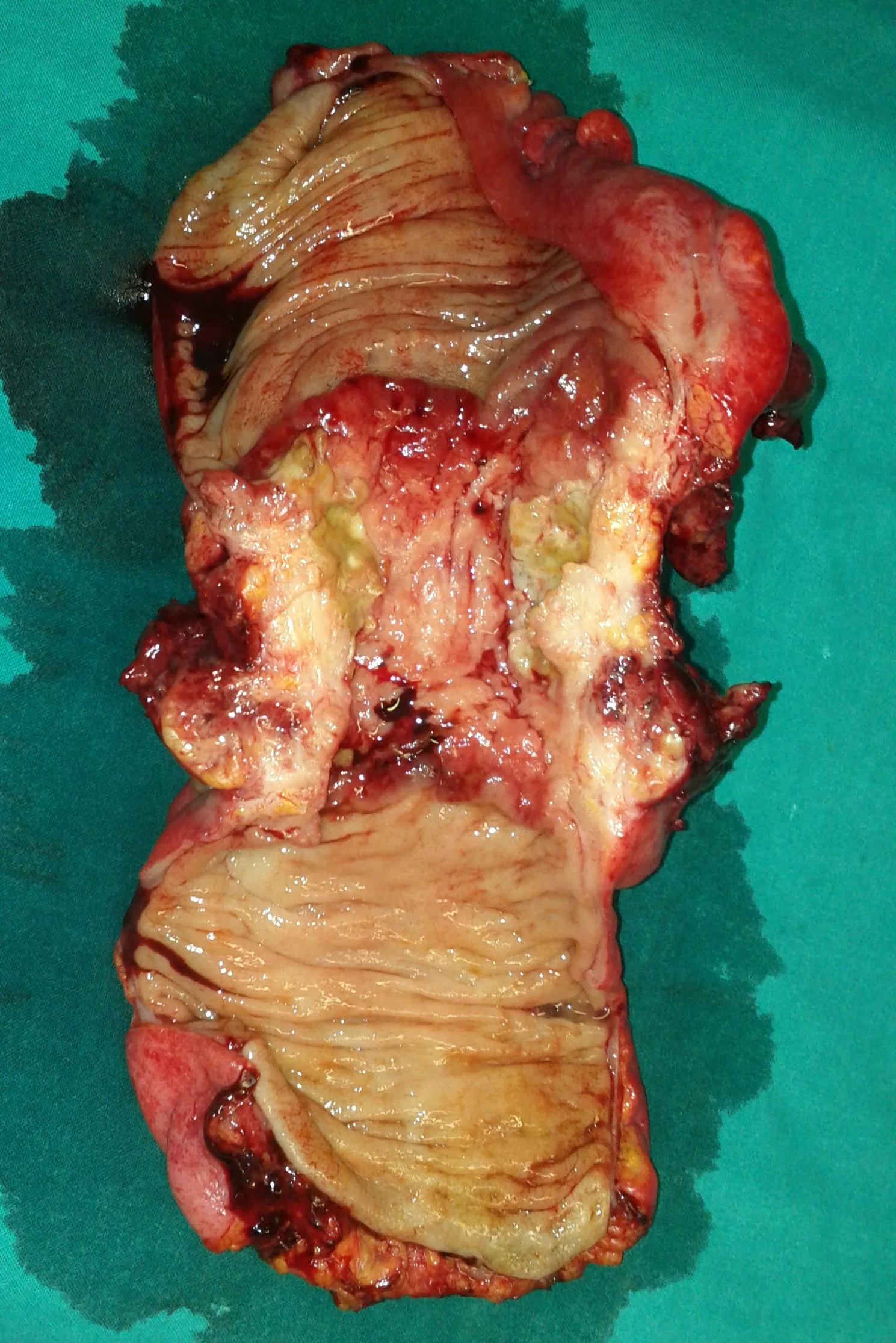
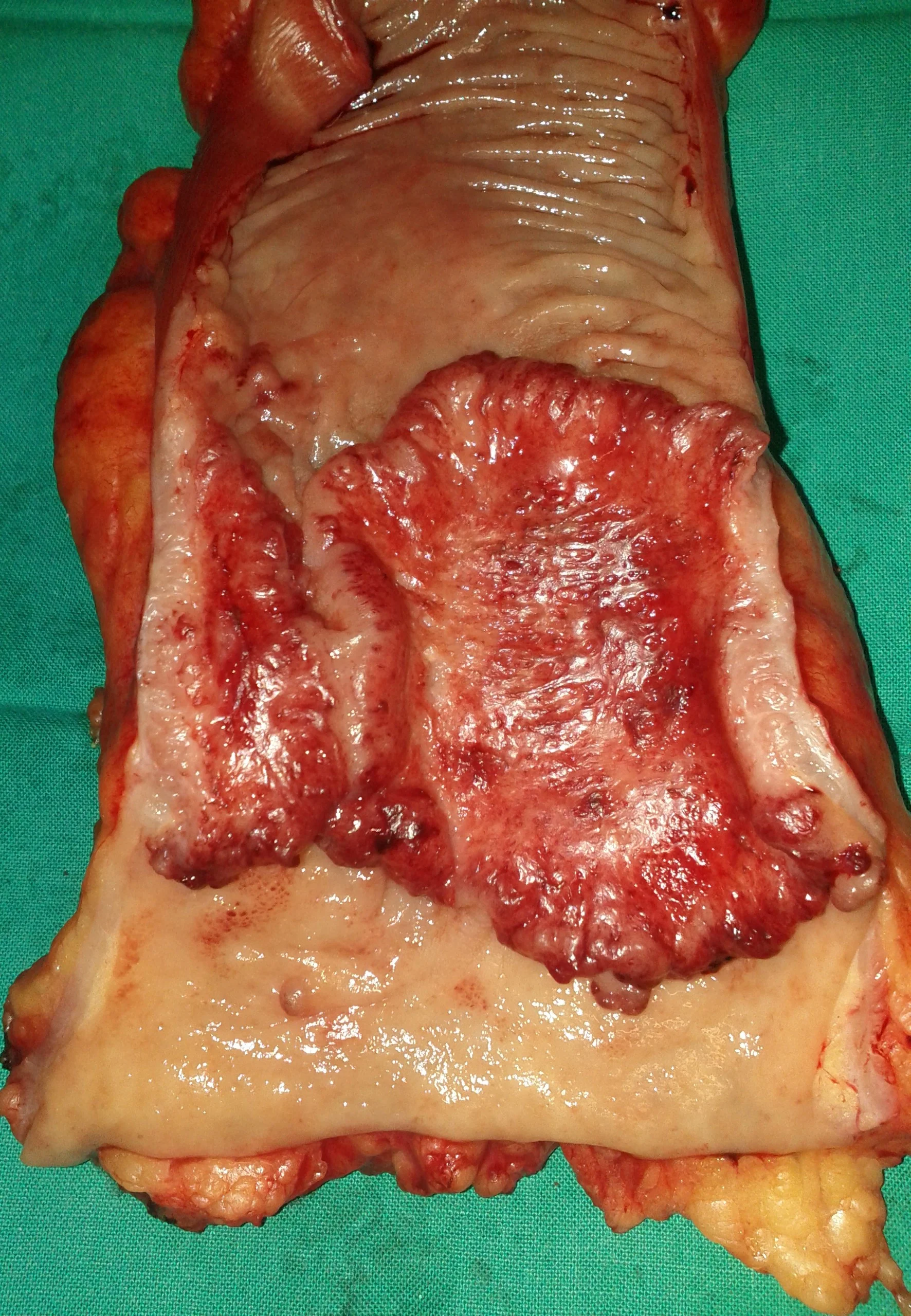
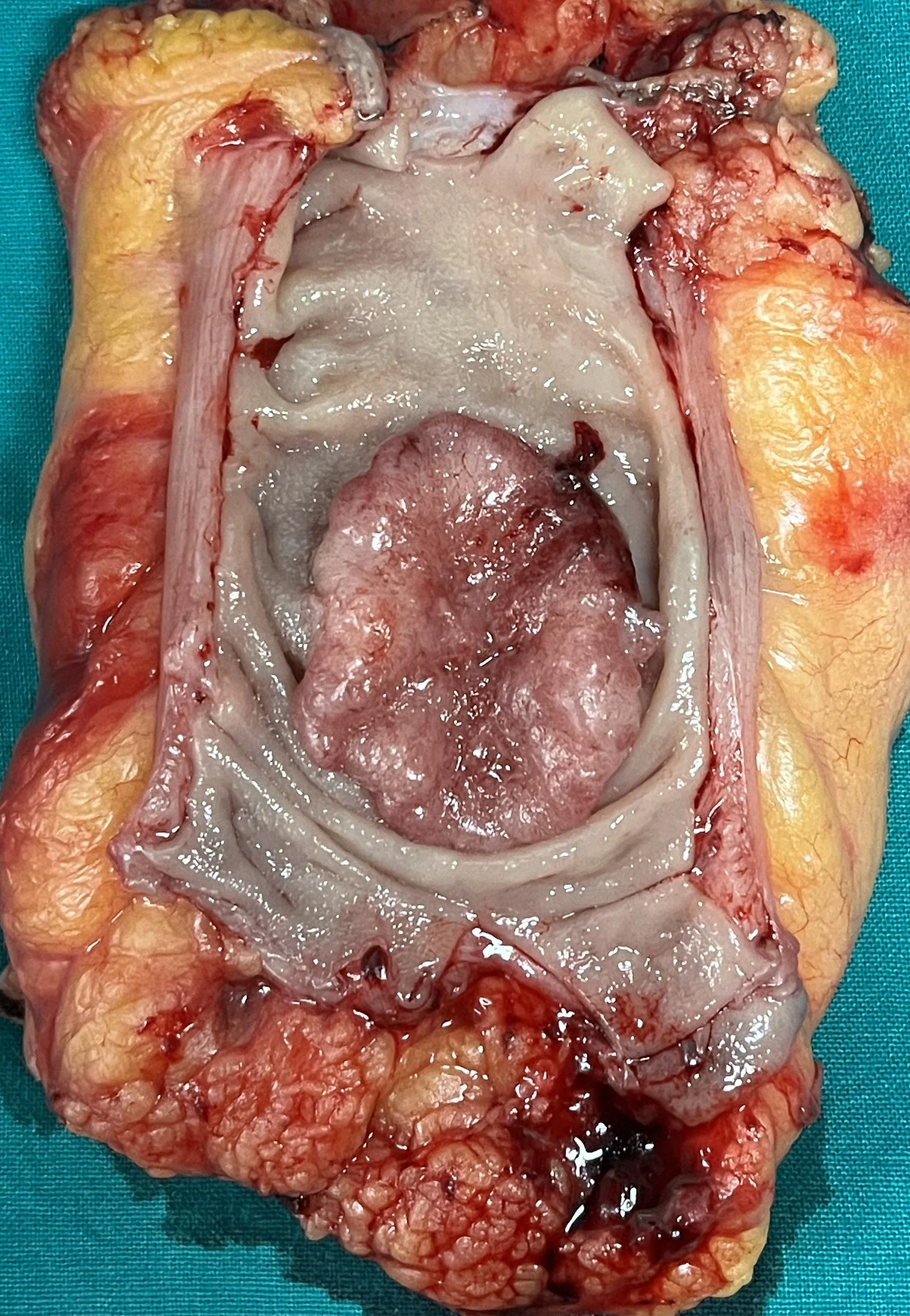
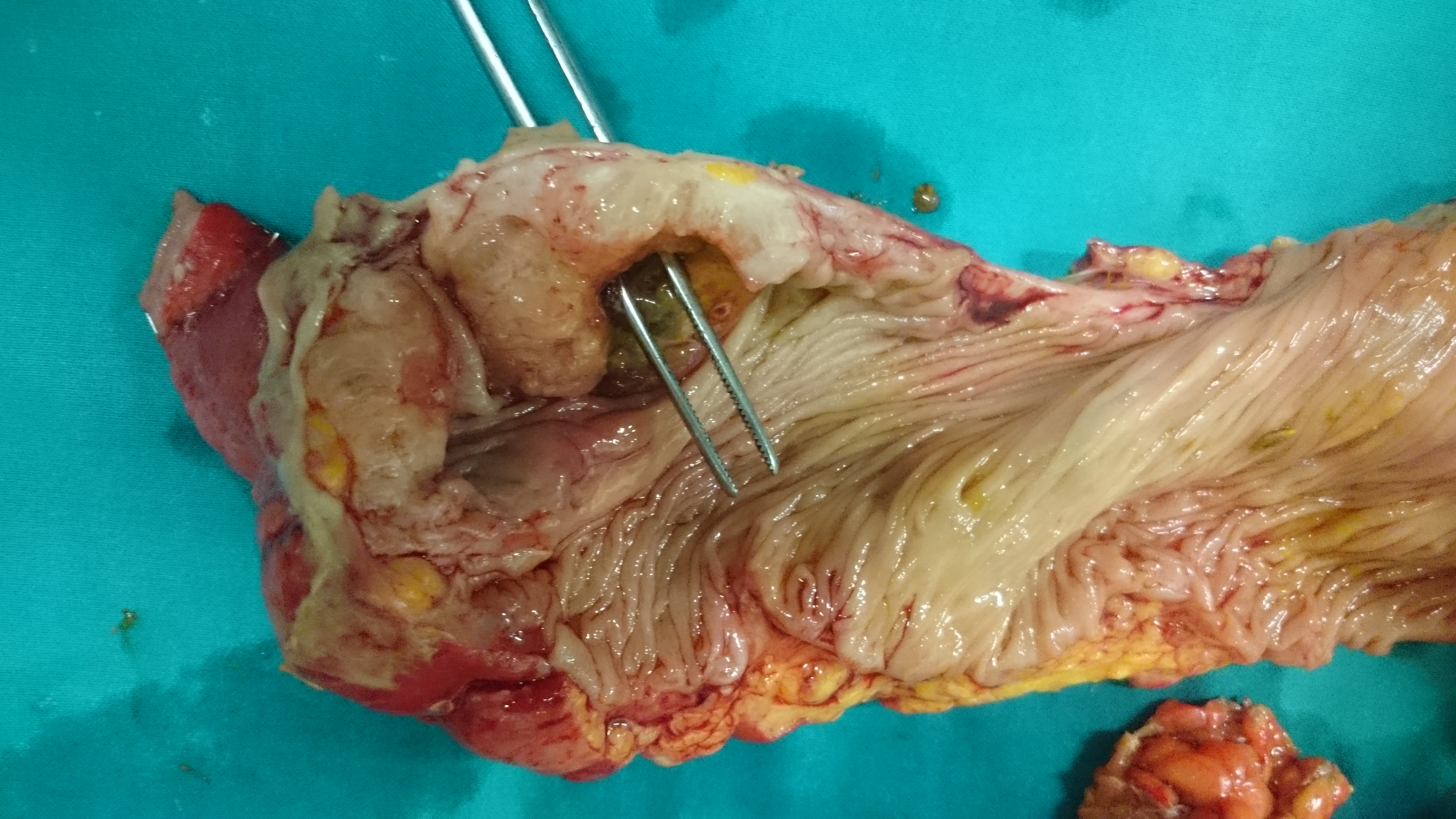
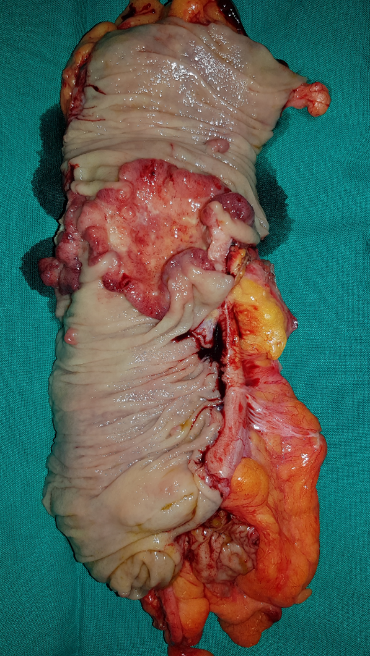
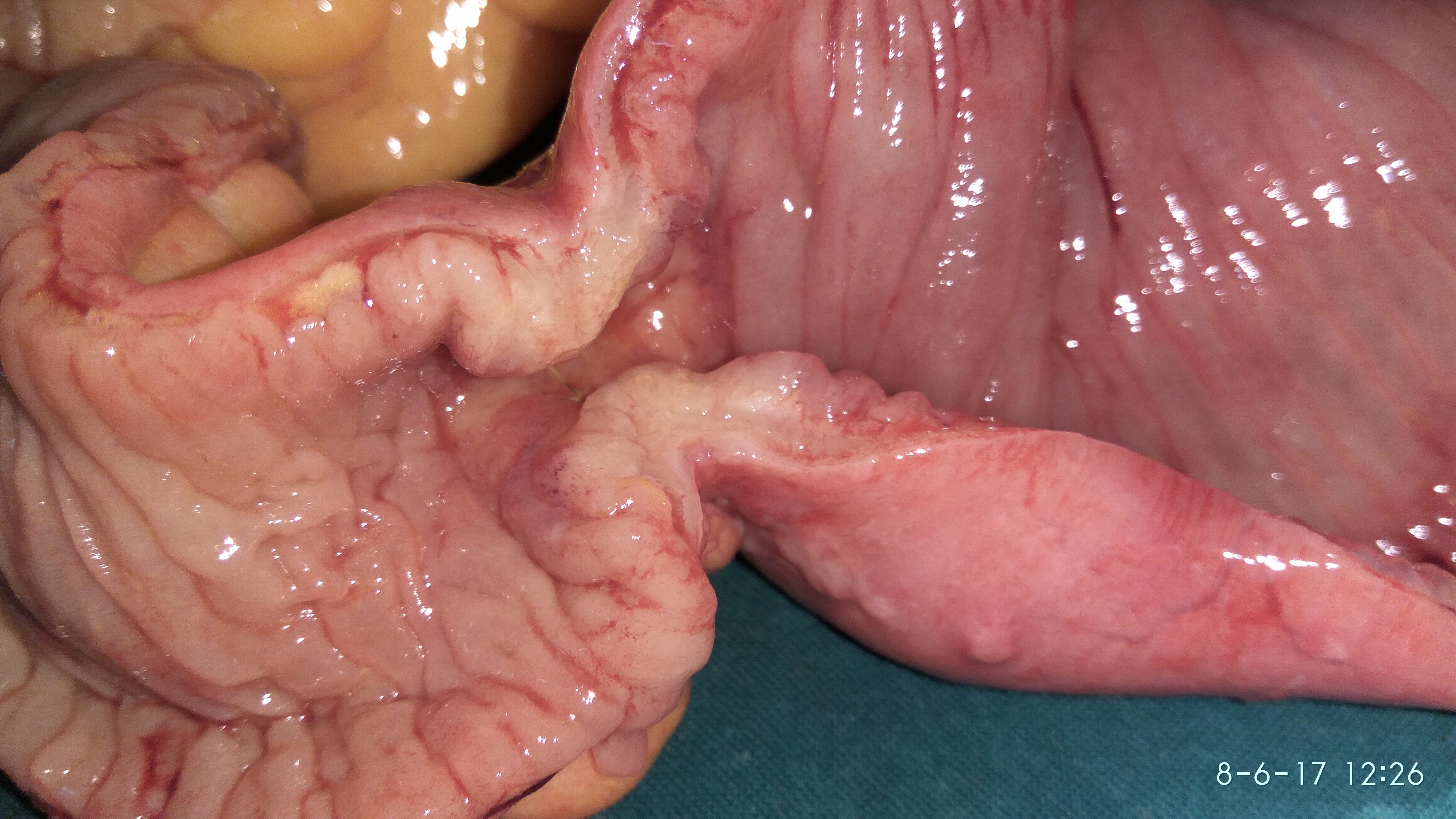
2017 : Metachronous jejunal adenocarcinoma with lymph nodes metastases (Courtesy Dr. V. Penopoulos)
2017 : Metachronous jejunal adenocarcinoma with lymph nodes metastases (Courtesy Dr. V. Penopoulos)




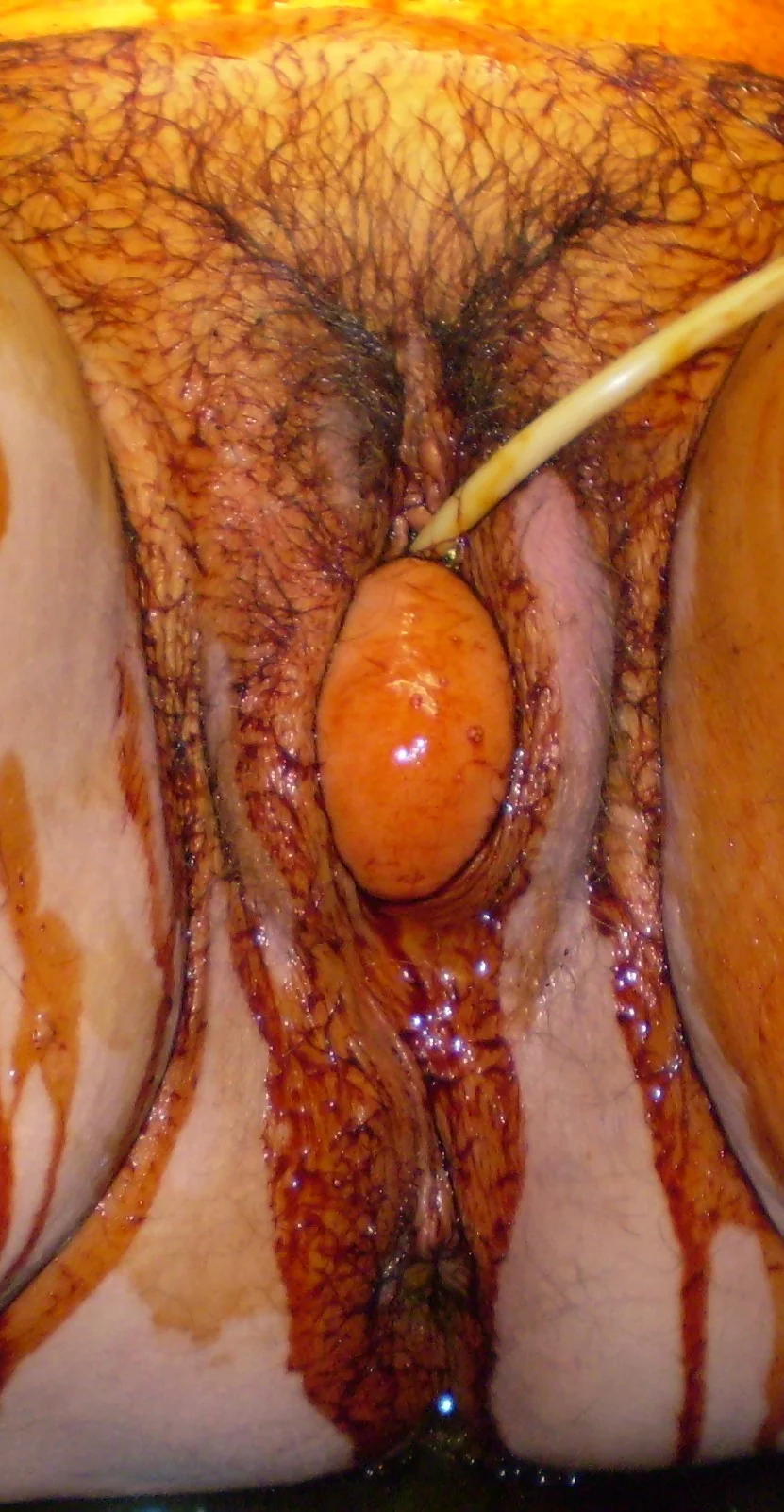
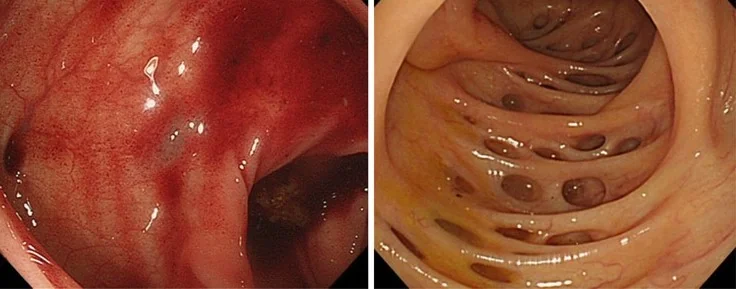
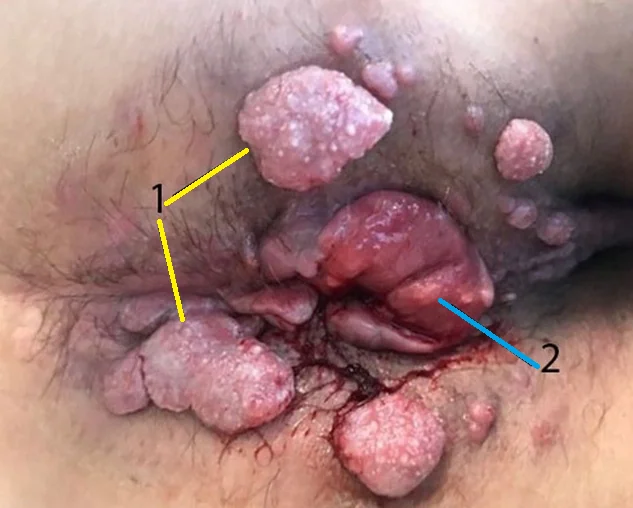
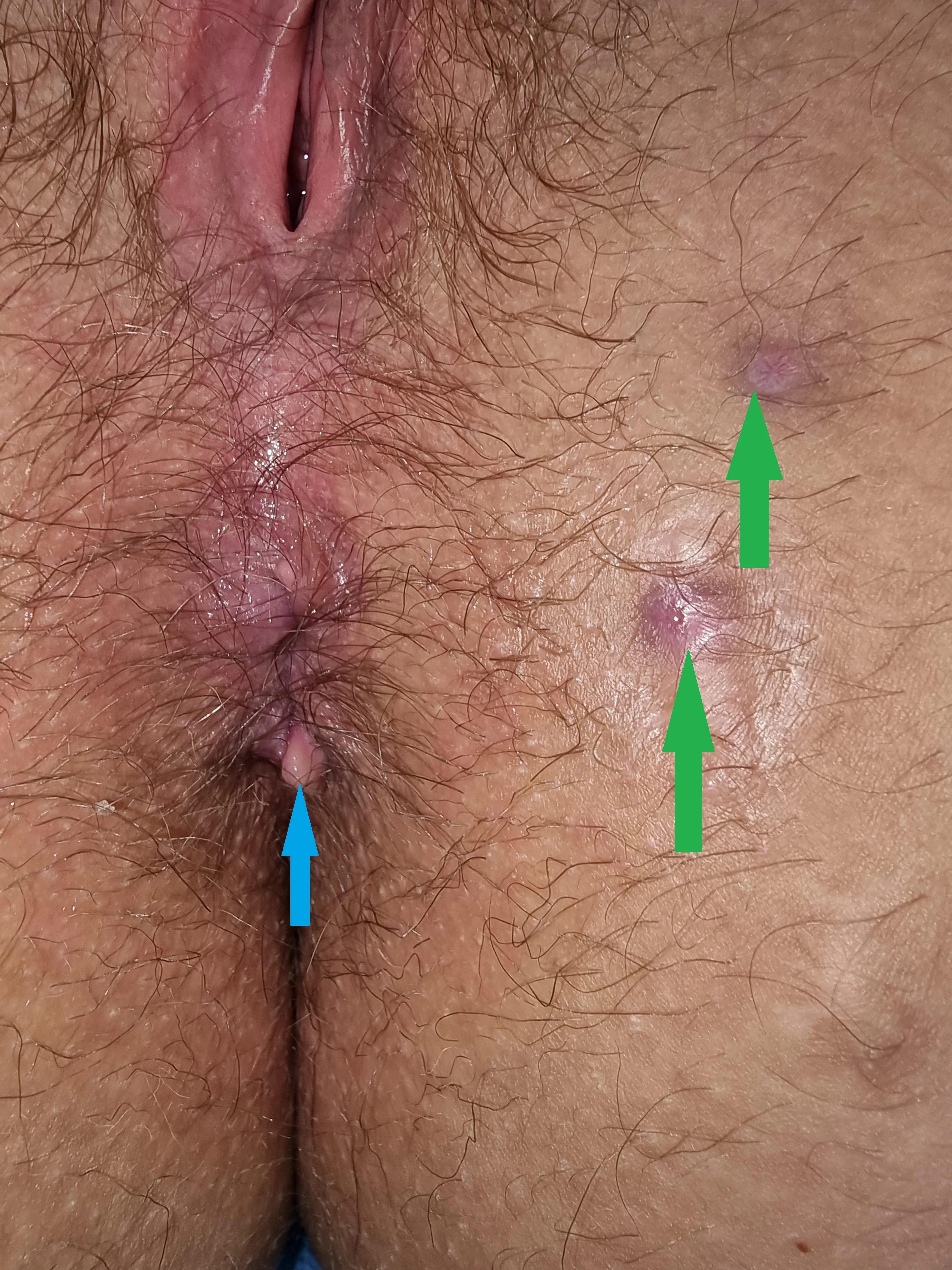
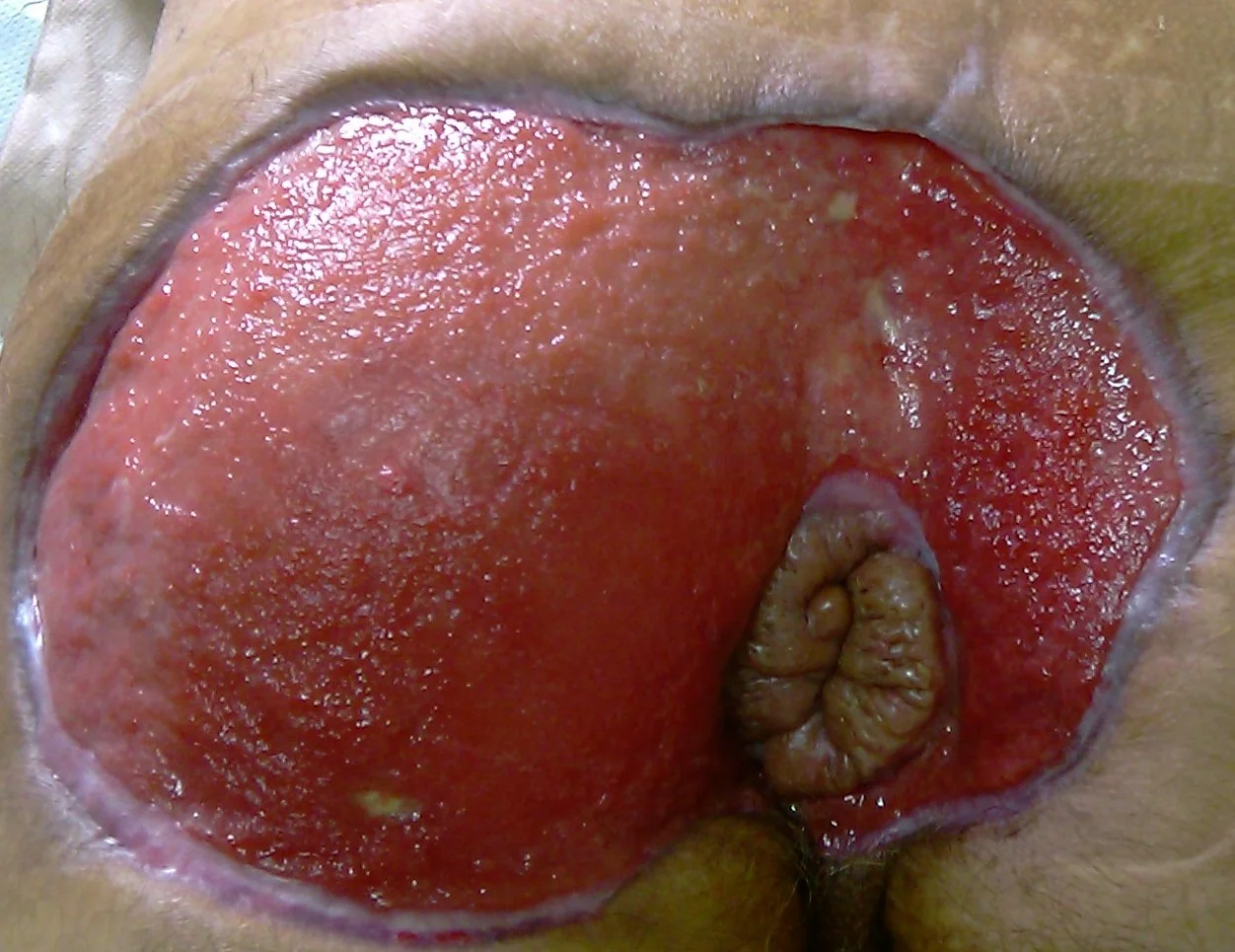
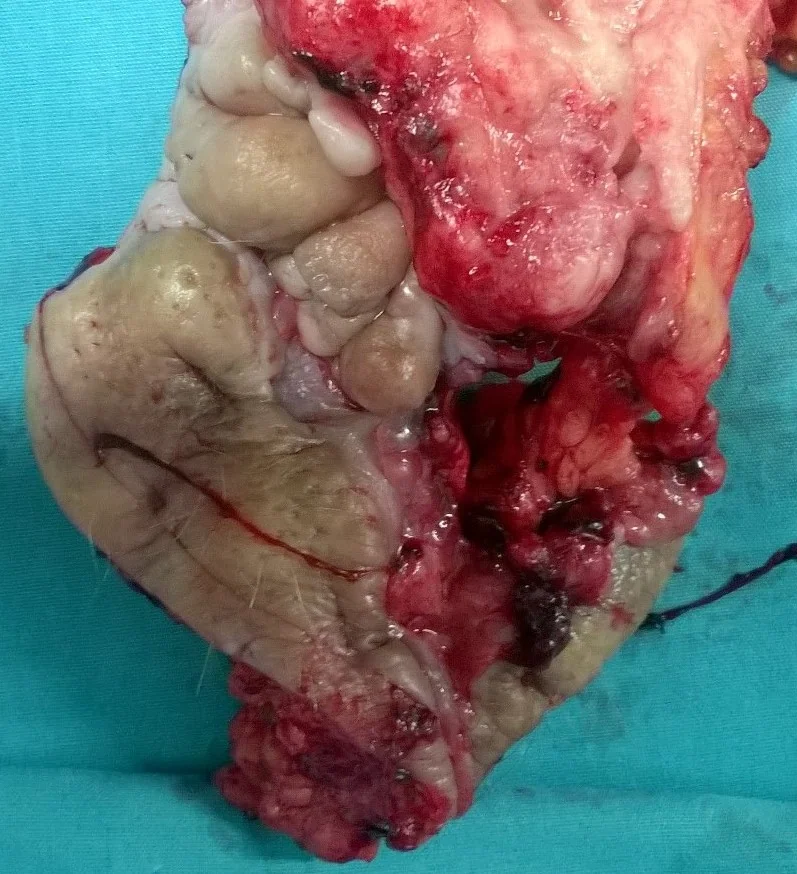
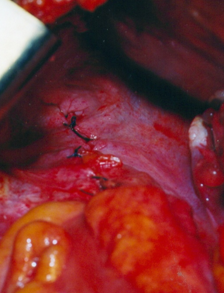
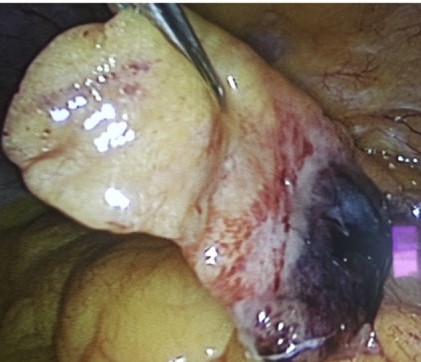
Varices of the anorectal region. Marked dilatation of the veins of the external hemorrhoidal plexus, with evident communication with the venous network of the rectal varices. An incipient rupture of a varix at the 12 o’clock position is noted.(Courtesy Dr.V.Penopoulos).

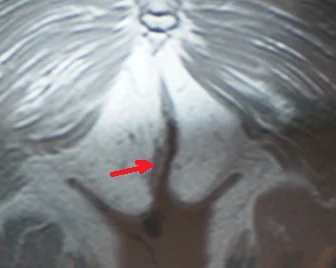
Liver cirrhosis.Red arrow - Portal vein obstruction.Ascites.(Courtesy Dr.V.Penopoulos).

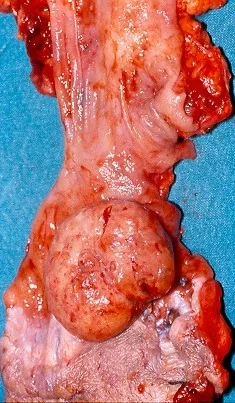
Pseudo-tumor of the mesenteric root - Mesenteric panniculitis (Courtesy Dr. V. Penopoulos)
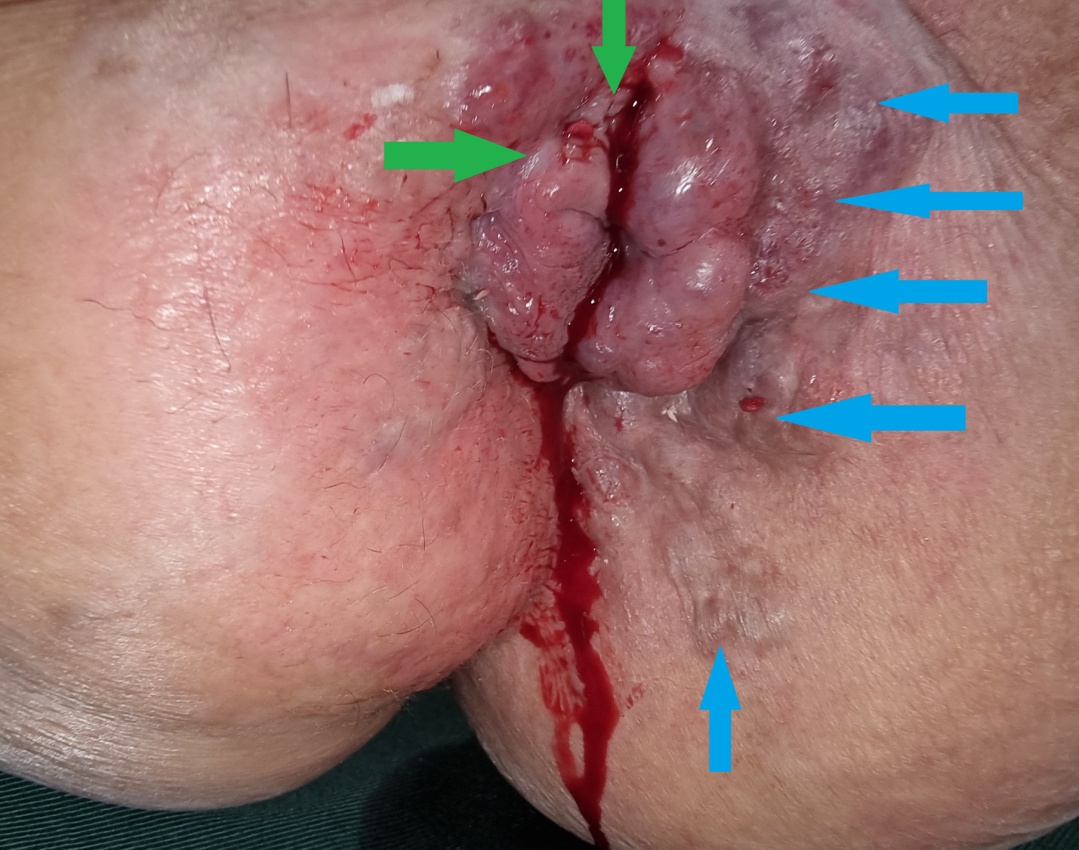
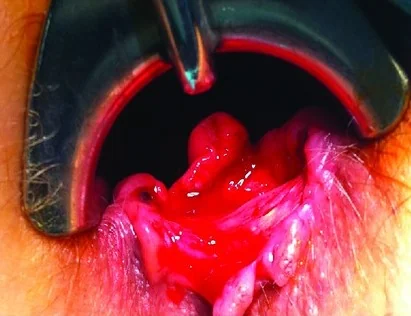
Bleeding anorectal varices . Marked dilatation of the external hemorrhoidal venous plexus . (Courtesy Dr. V. Penopoulos)
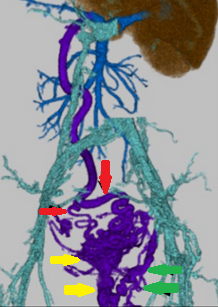
Massive dilatation of the right superior rectal vein.Collateral circulation superior rectal veins and the varices of the anorectal region.(Courtesy Dr.V.Penopoulos).
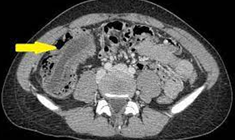
Abdominal CT scan. Red arrows - Inflamed epiploic appendage with hyperattenuated peripheral rim (Courtesy Dr. V. Penopoulos)
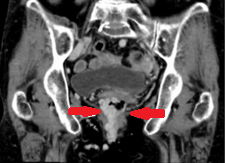
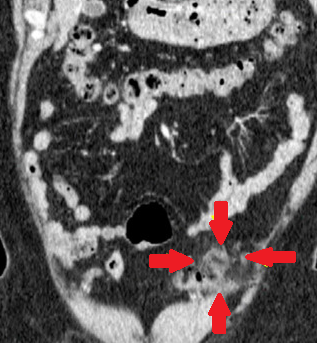
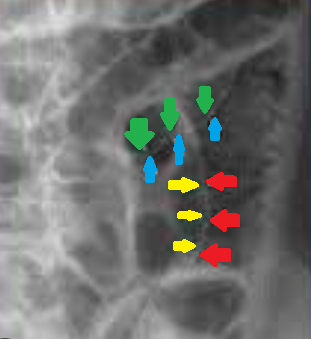
Red arrows: massive dilatation of the right superior rectal vein. Collateral circulation between the superior rectal veins (red arrows) and the anorectal varices (yellow and green arrows) (Courtesy Dr. V. Penopoulos)

Abdominal CT scan. Red arrows - Inflamed, ovoid-shaped epiploic appendage.(Courtesy Dr. V. Penopoulos).

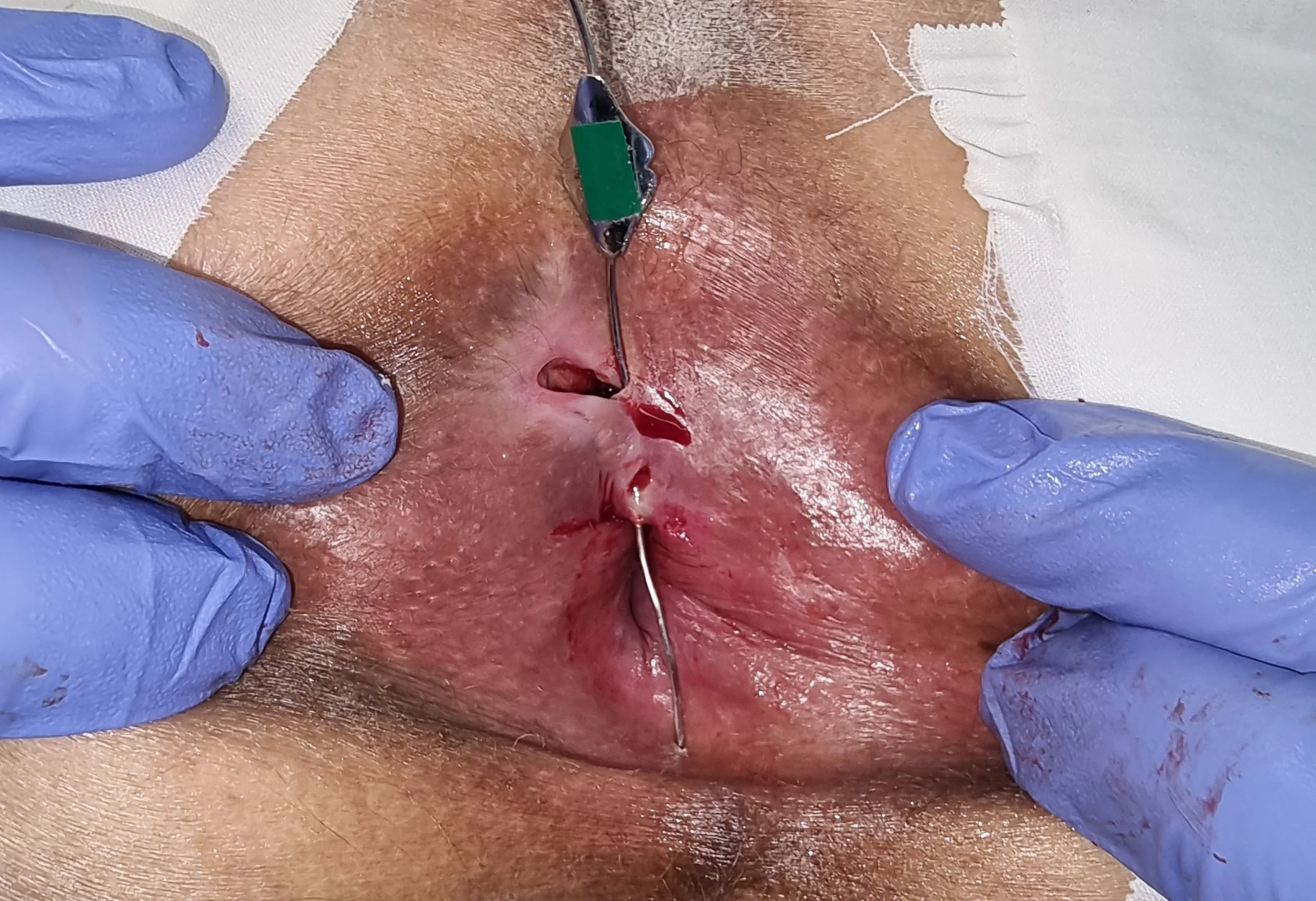
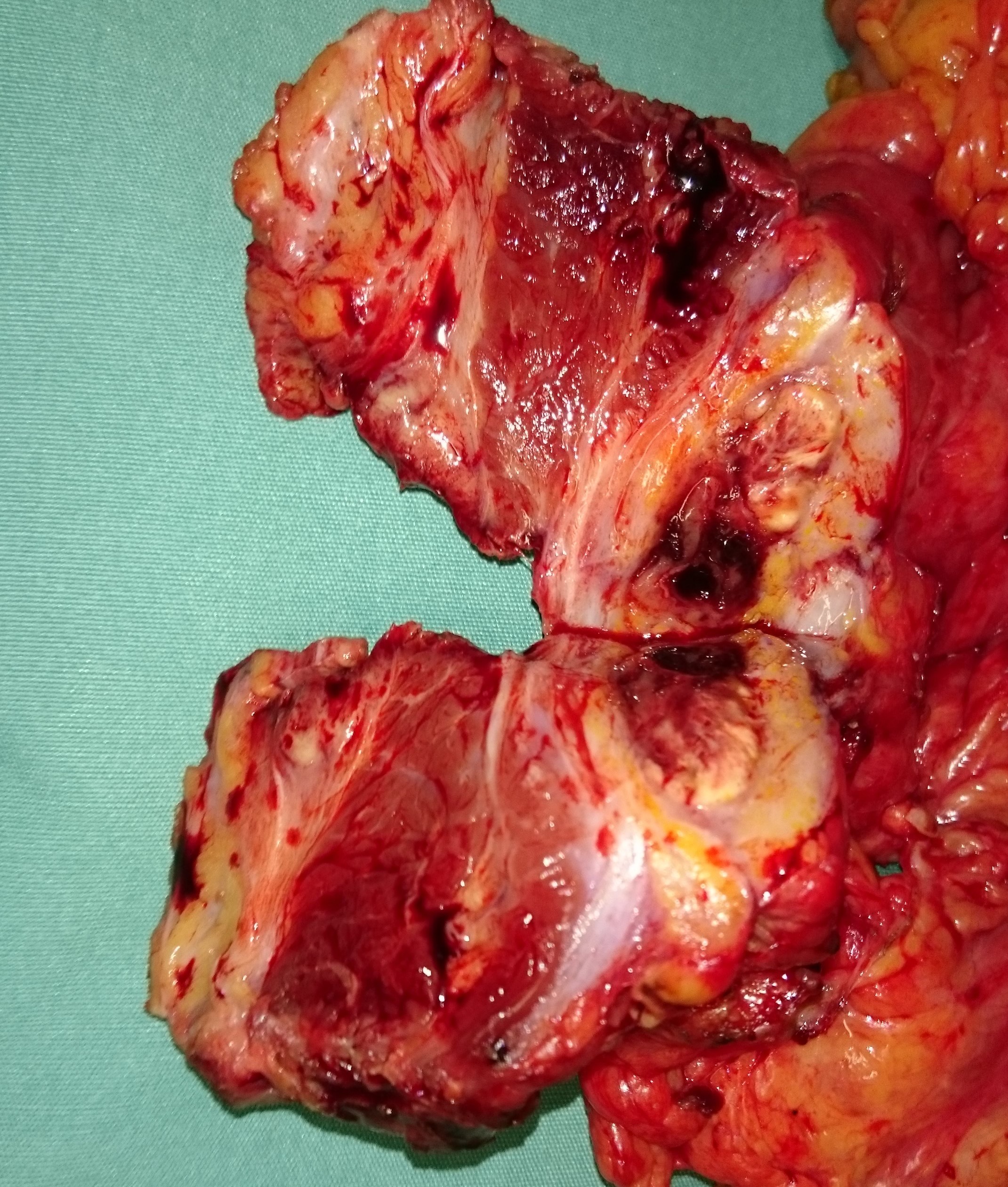
Macroscopic view on the 2nd postoperative day. Green outline: area of excised bleeding varices (Courtesy Dr. V. Penopoulos)


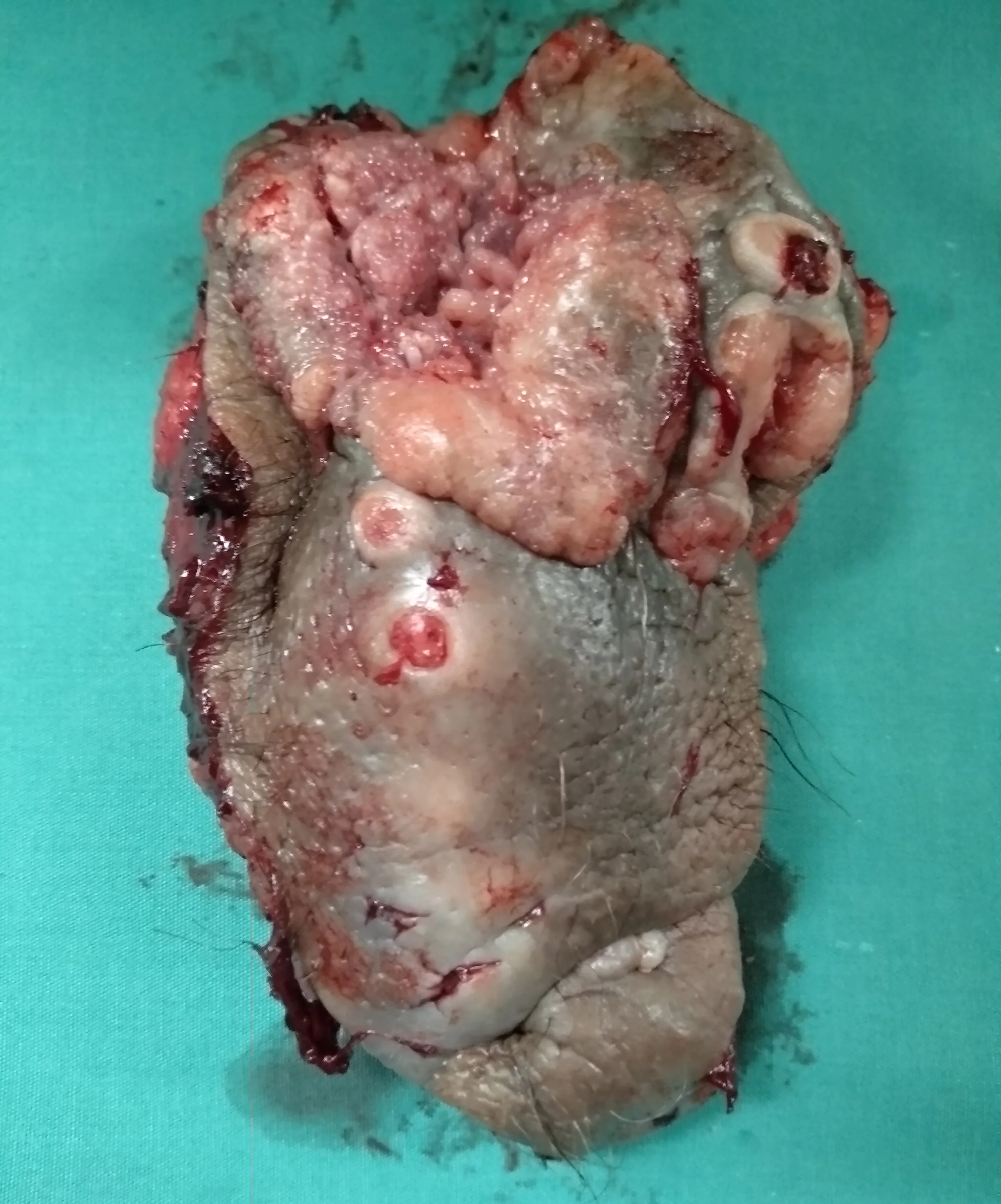
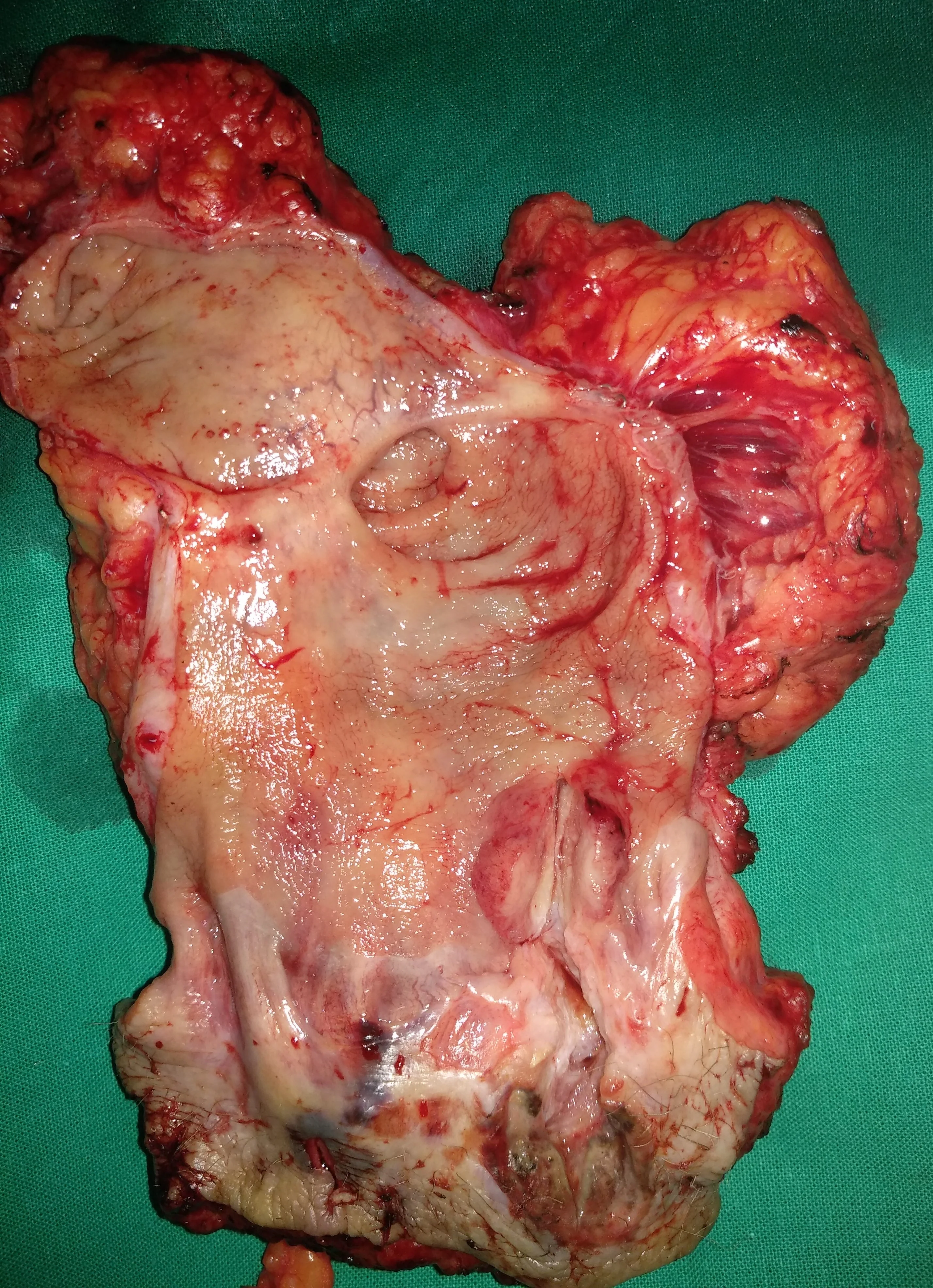
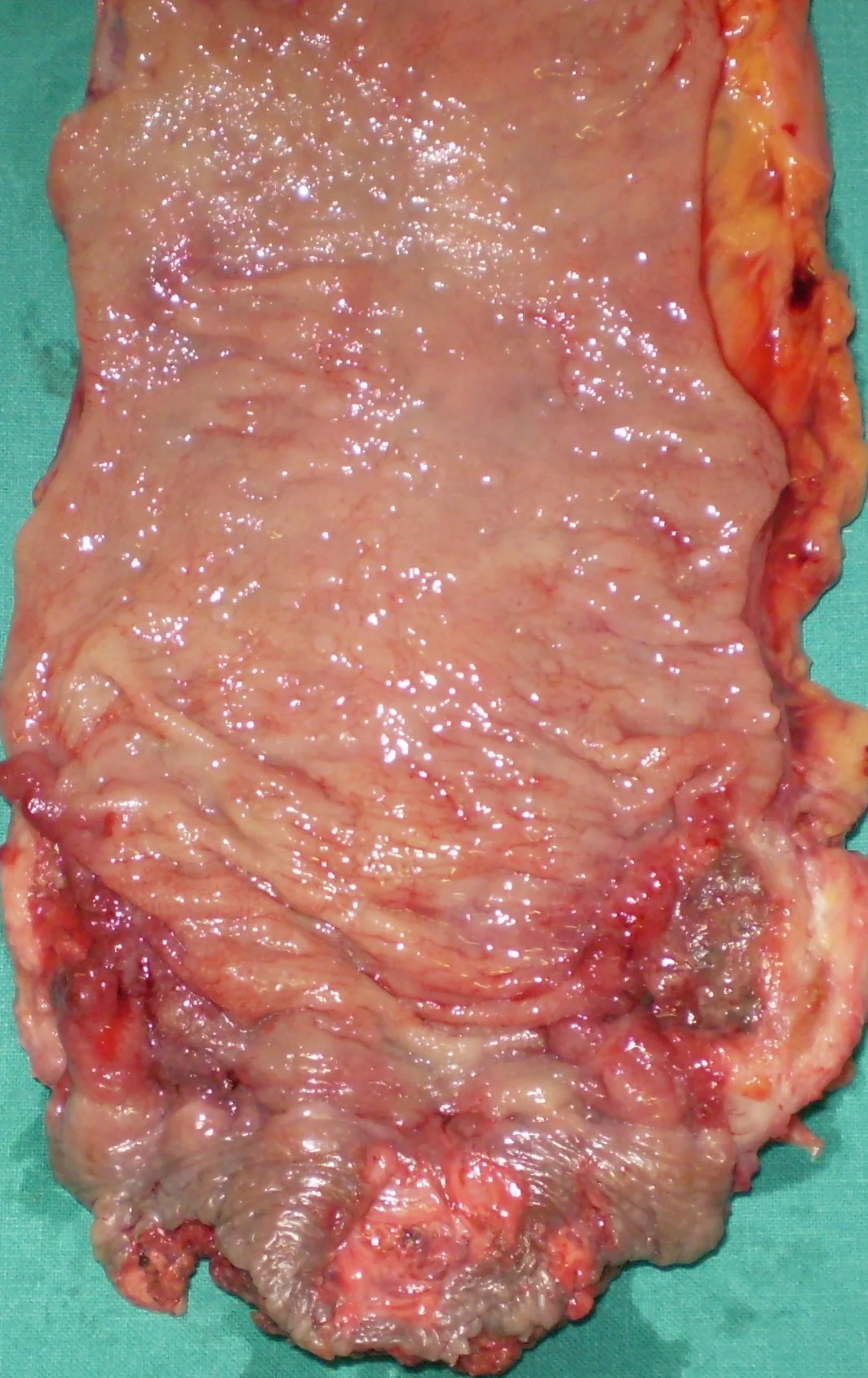
Adenocarcinoma — Abdominoperineal resection of the rectum. Yellow arrow — Site of excised neoplasm (Courtesy Dr. V. Penopoulos)
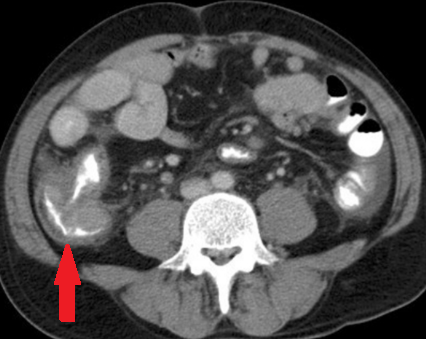
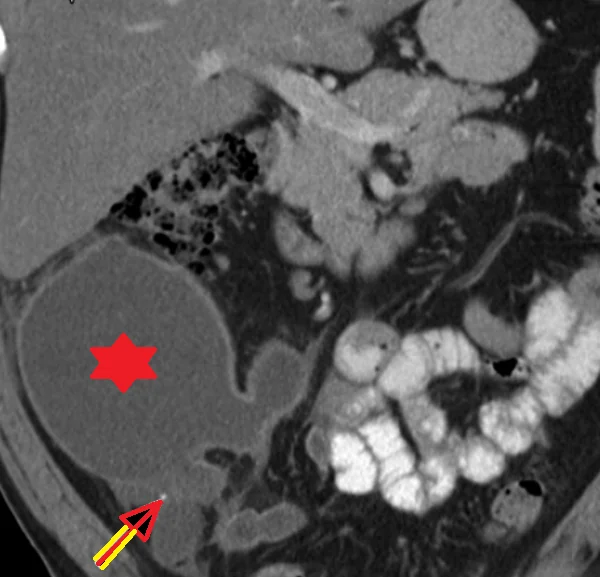
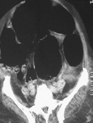
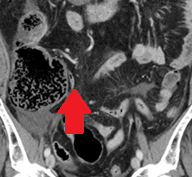
Abdominal CT scan - Cecal MALToma and paracolic lymph node (Courtesy Dr. V. Penopoulos)
Green arrow-Anal orifice.Blue arrow-Rectum.Light blue arrow-Tape surrounding the rectum.(Courtesy Dr.V.Penopoulos).
Adenocarcinoma — Abdominoperineal resection of the rectum. Yellow arrow — Site of transrectaly excised neoplasm (Courtesy Dr. V. Penopoulos)
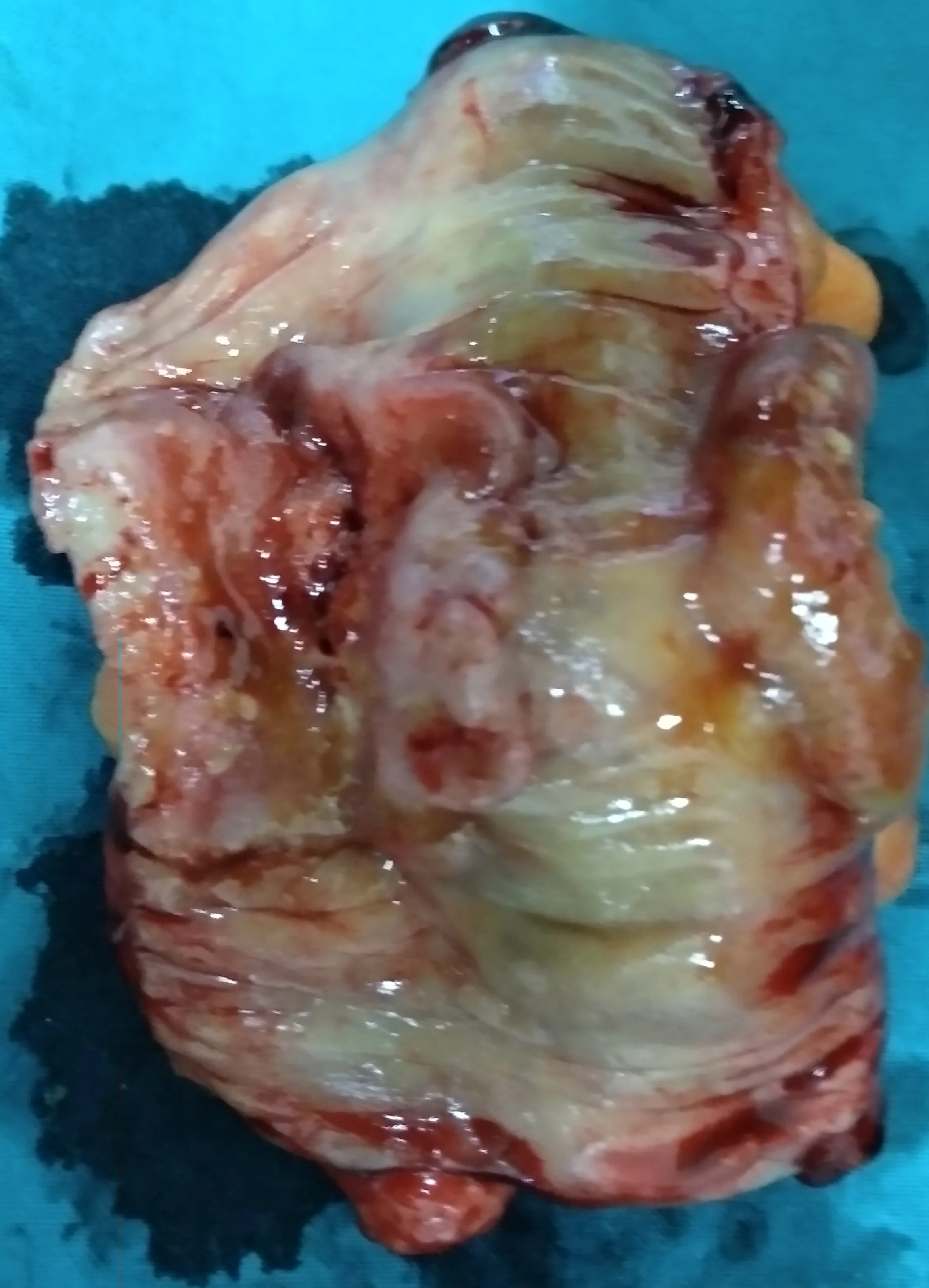
Pseudomyxoma peritonei — Complete involvement of the greater omentum (Courtesy Dr. V. Penopoulos)

Green arrow — Anus. Blue arrow — Rectum. Rose arrow — Tape encircling the rectum (Courtesy Dr. V. Penopoulos)

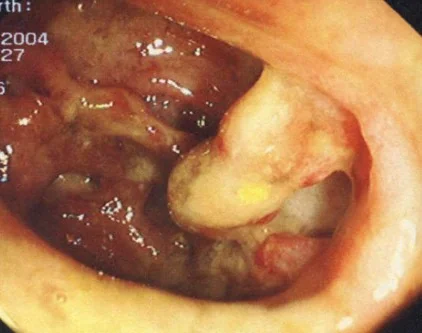
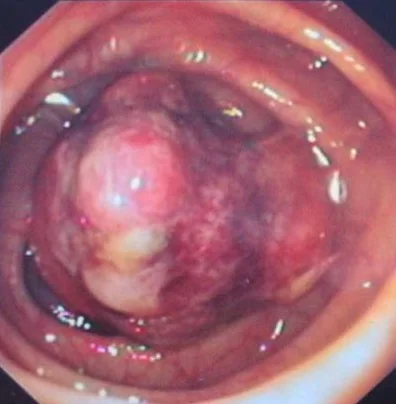
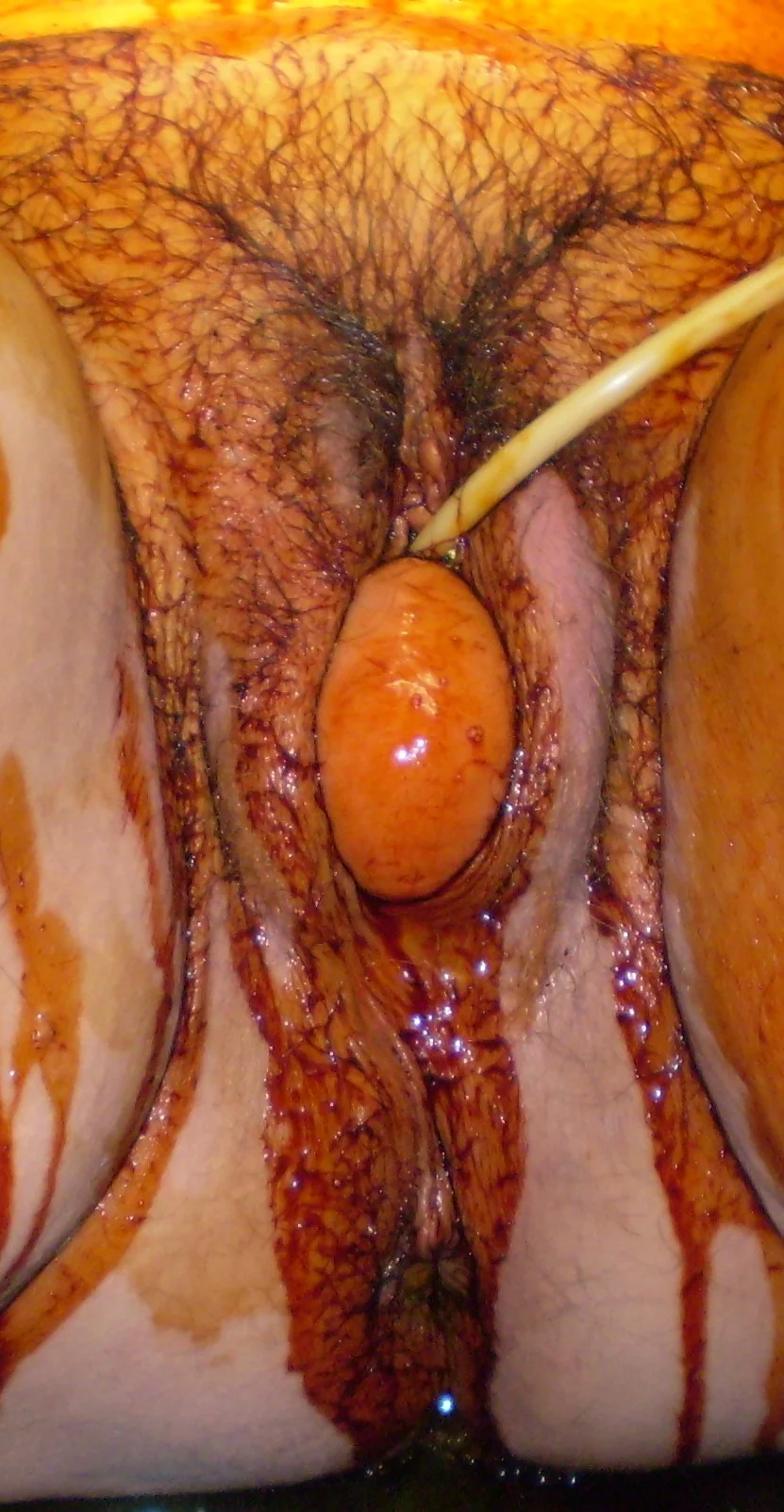
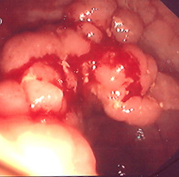
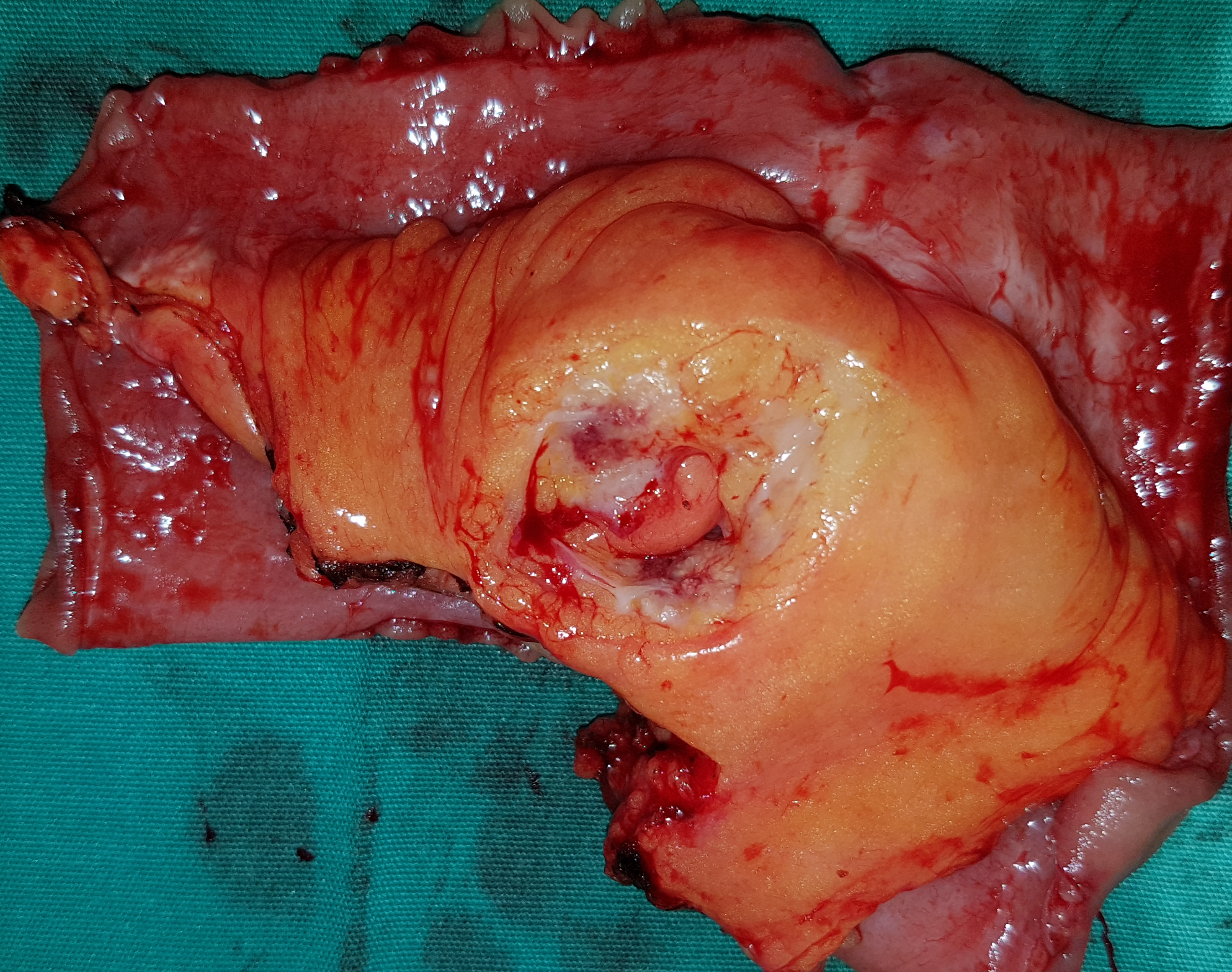
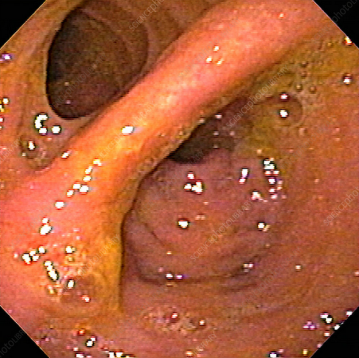
Colonoscopic image of appendiceal mucocele intussusception (Courtesy Dr. V. Penopoulos)
En bloc excision of right adnexa together with adjacent infiltrated peritoneum.(Courtesy Dr.V.Penopoulos).

Abdominal CT scan - Cecal MALToma and paracolic lymph node (Courtesy Dr. V. Penopoulos)

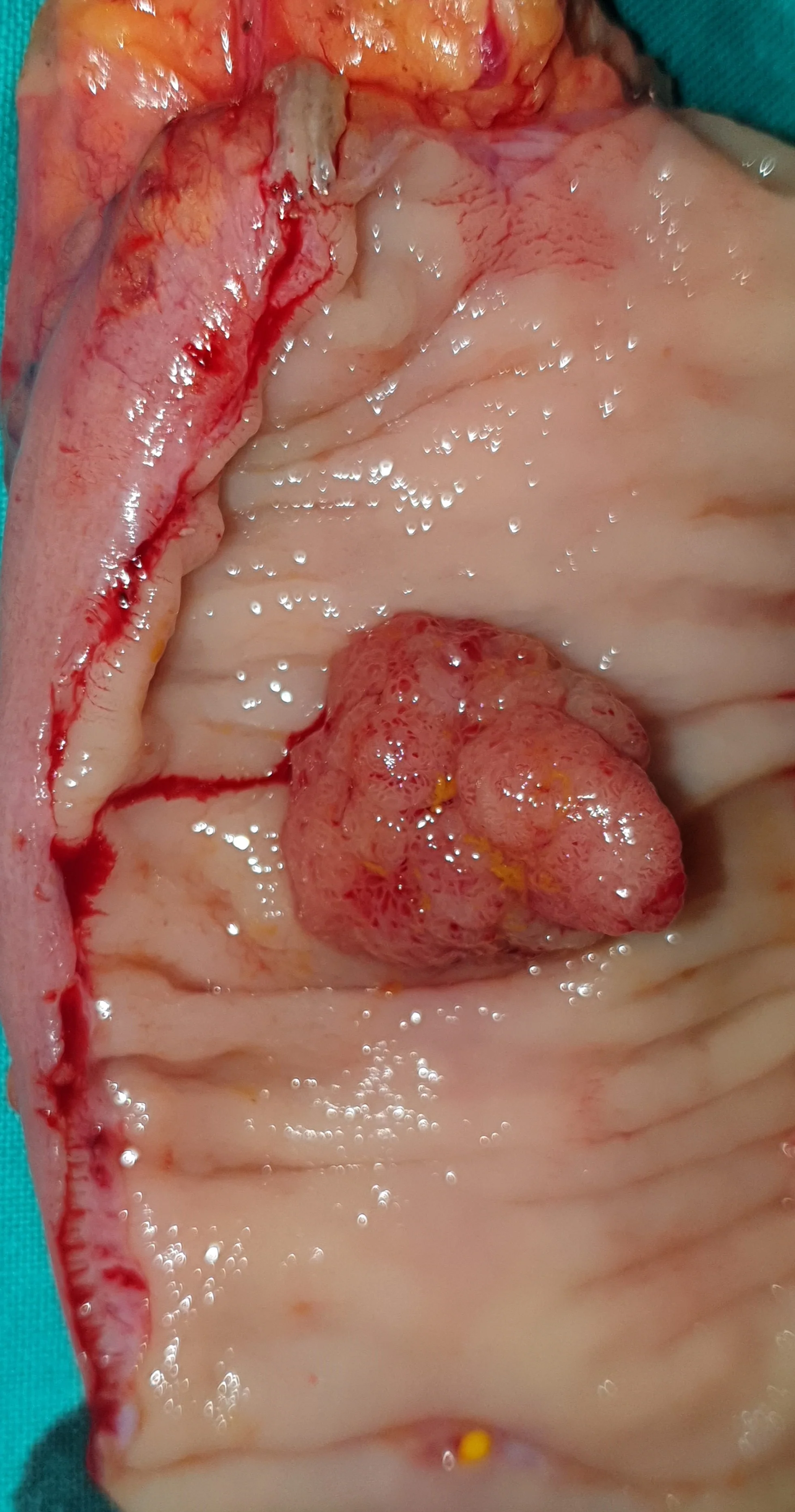
Blue arrow-upper border of rectotomy.Yellow arrow-Rectal adenomatous tumor.(Courtesy Dr.V.Penopoulos).

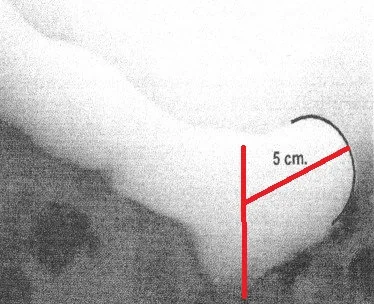
Plain Abdominal X-Ray.Significant distension of the colon and the inverted comma sign diagnostic of cecal volvulus.(Courtesy Dr.V.Penopoulos).
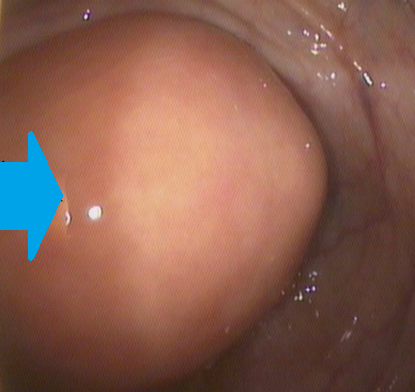
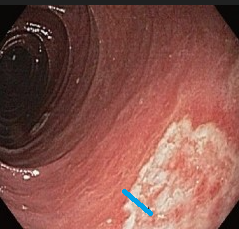
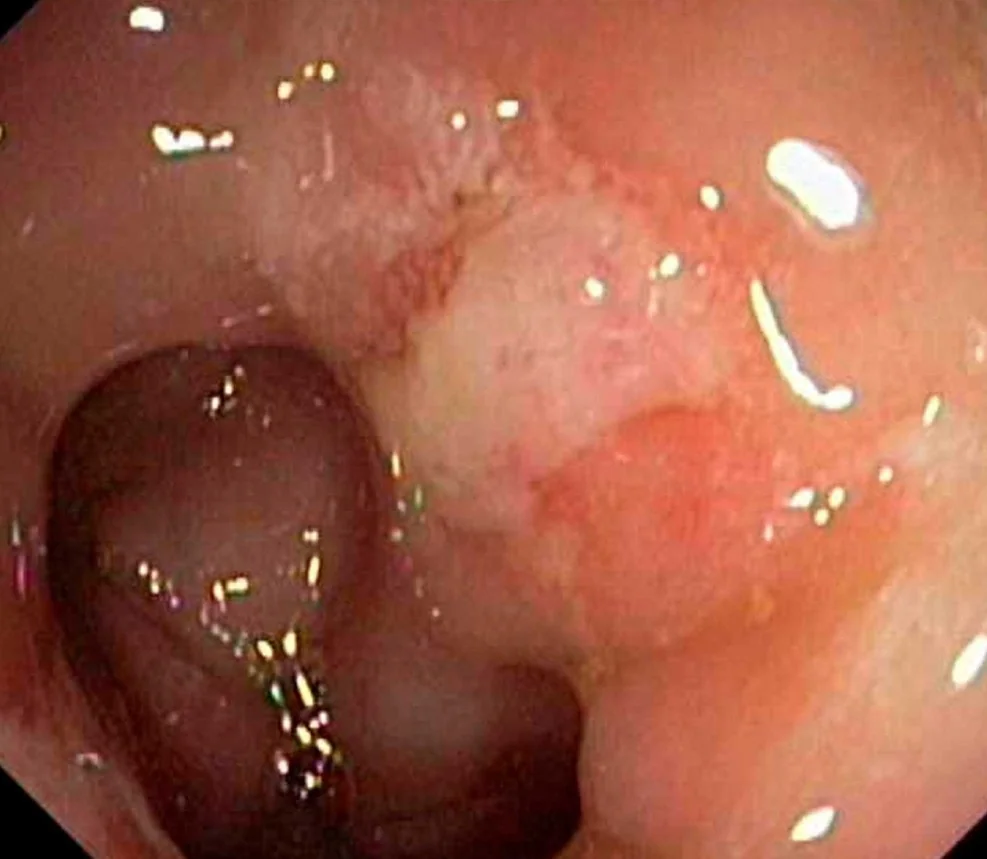
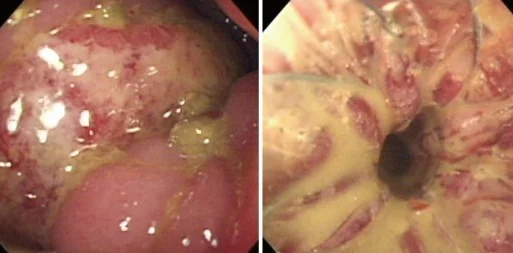
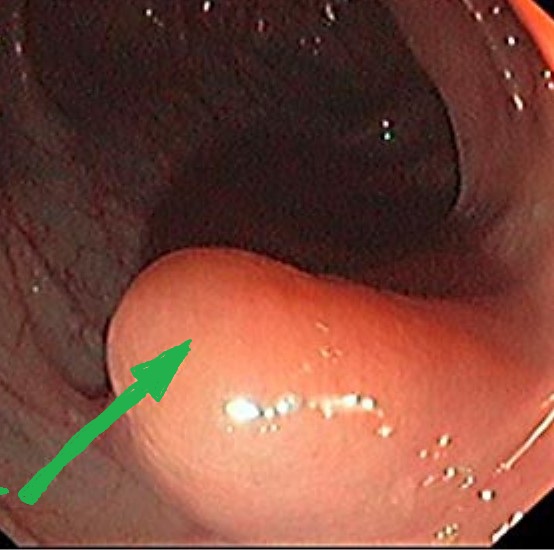
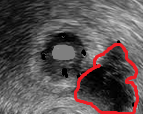
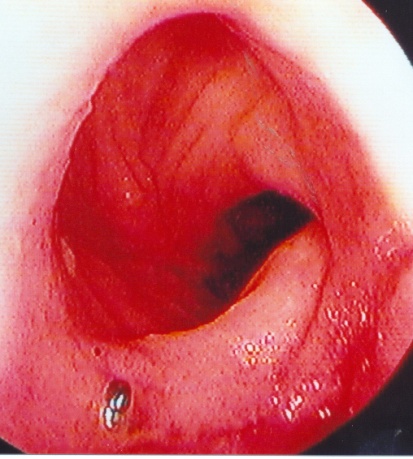
Colonoscopic image of mucocele — Submucosal mass. Blue arrow — "Volcano sign" (Courtesy Dr. V. Penopoulos)


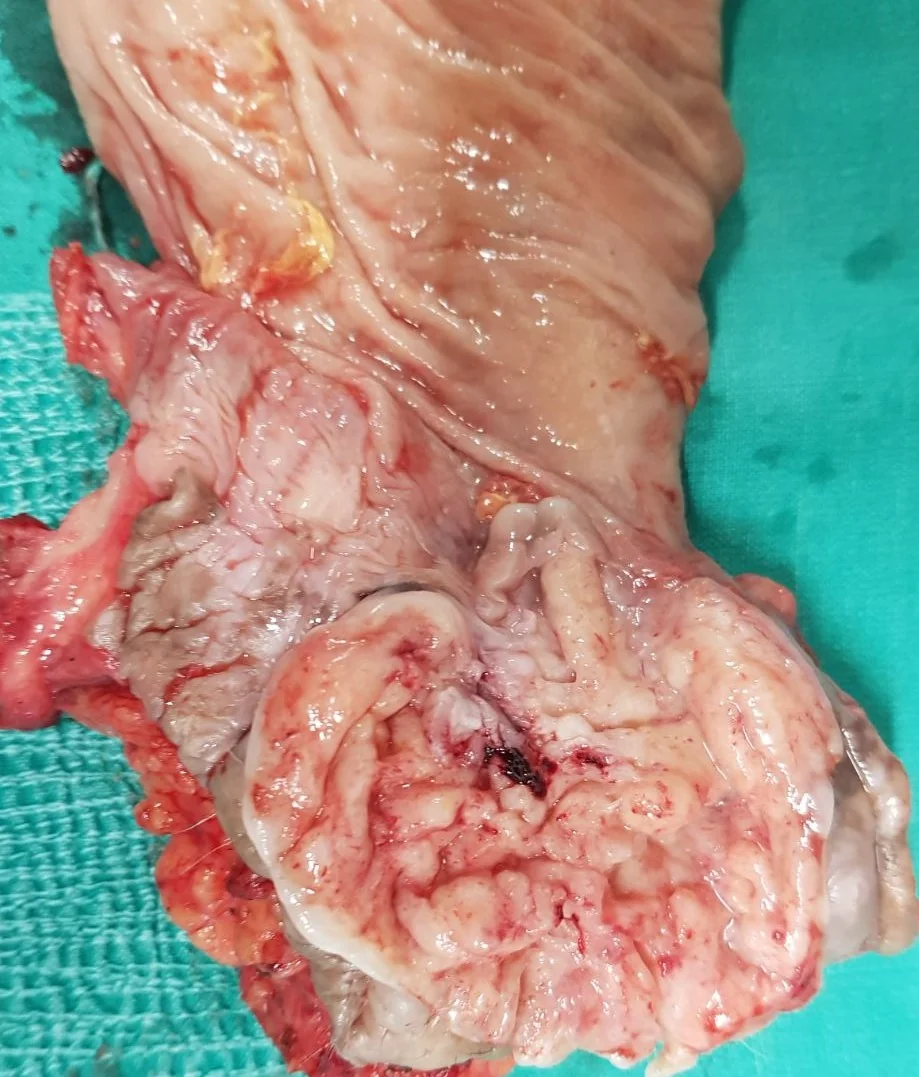
Right hemicolectomy specimen.Blue arrow-Local rupture of mucocele.(Courtesy Dr.V.Penopoulos).

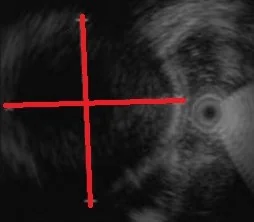
Abdominal U/S.Vague mass in the right iliac fossa.Failed to detect vermiform appendix.(Courtesy Dr.V.Penopoulos).


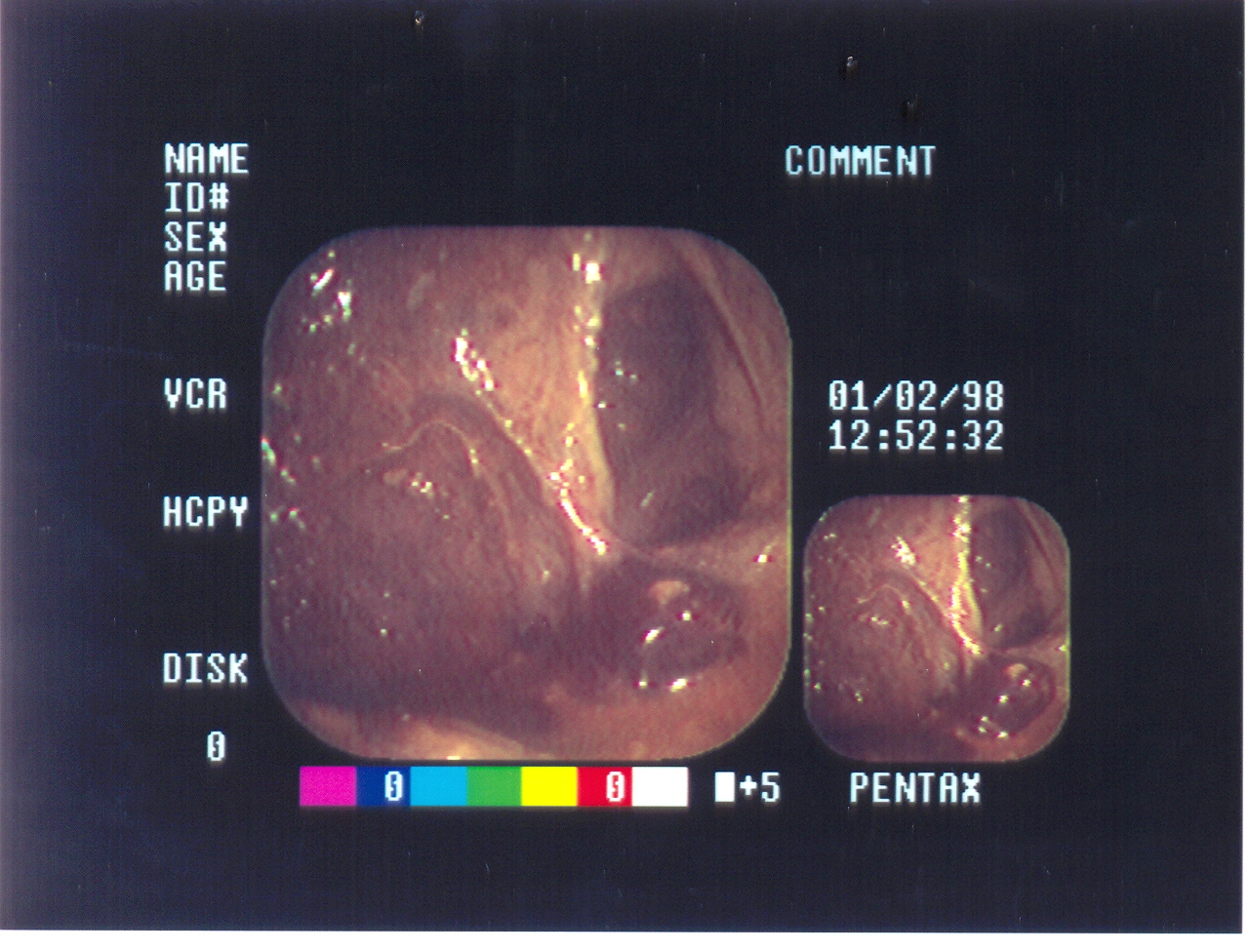
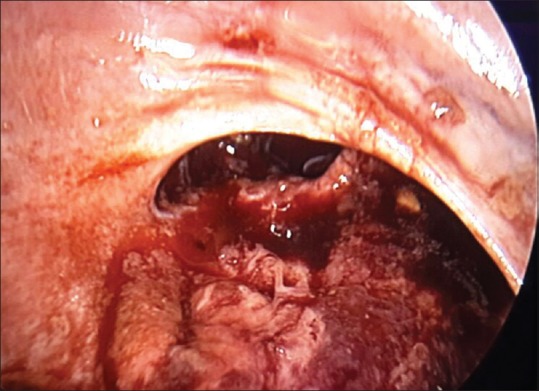
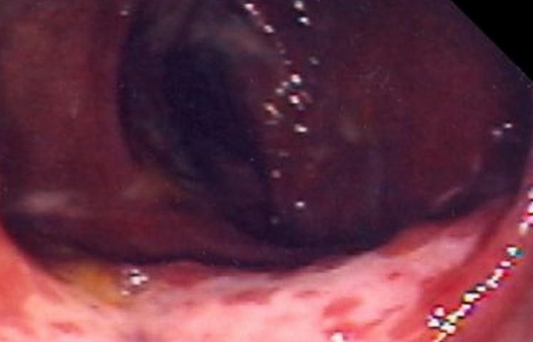
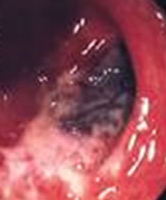
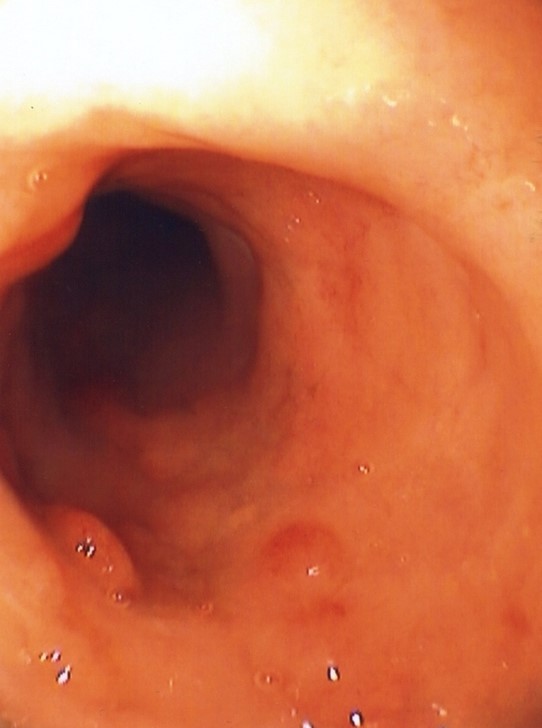
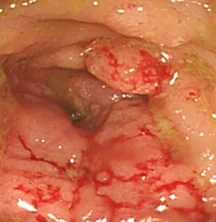
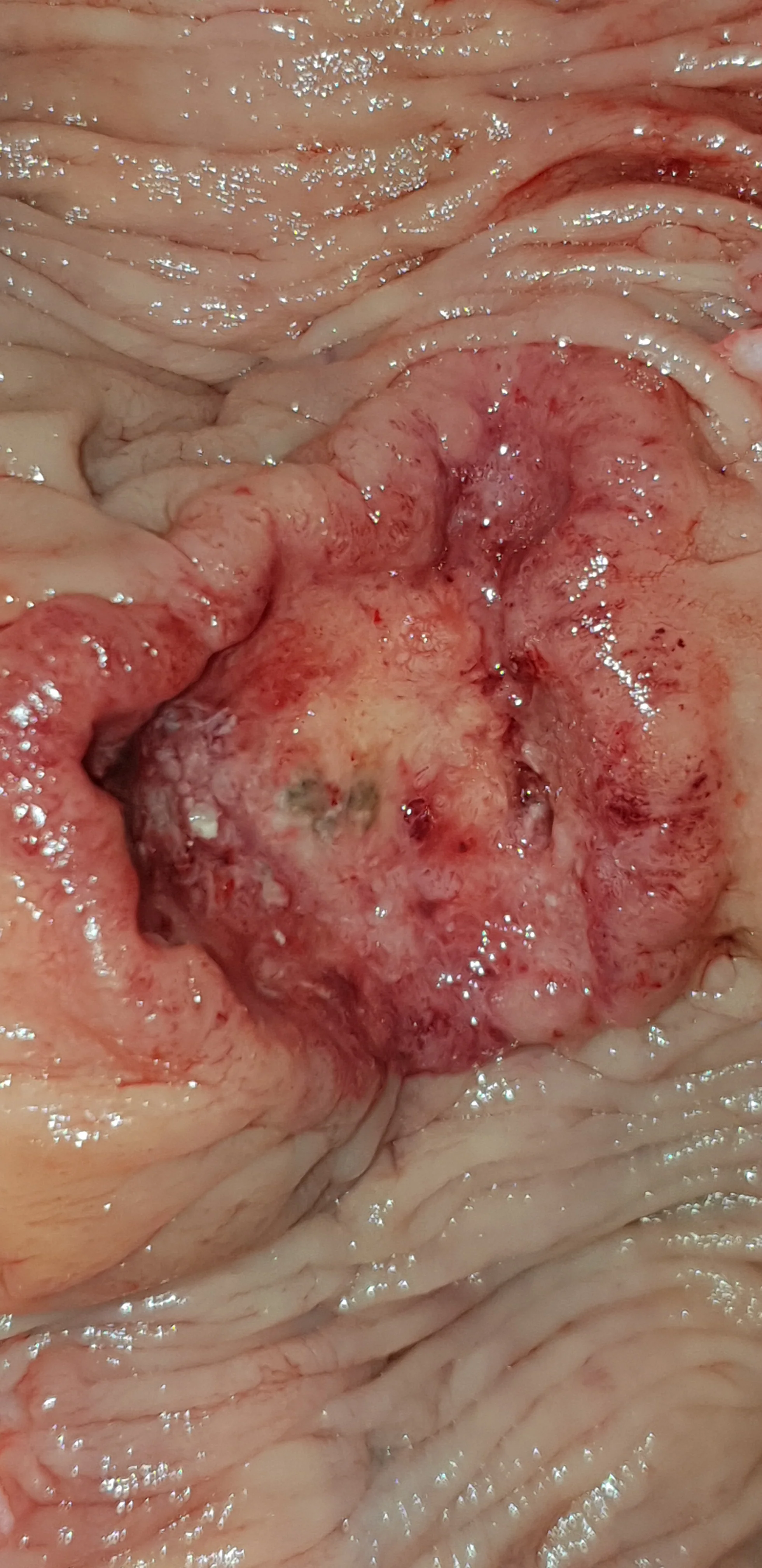
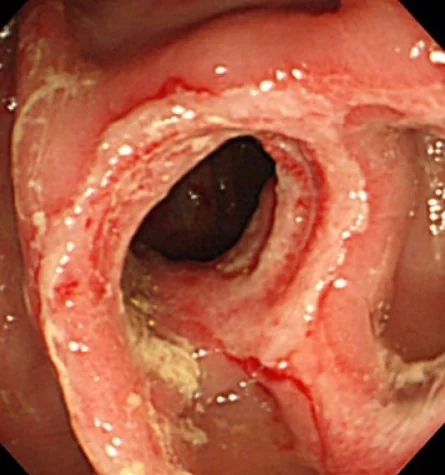
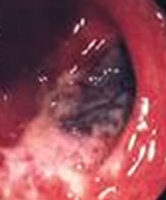
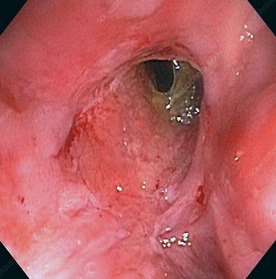
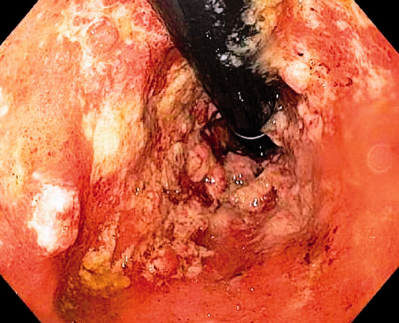
Endoscopic views of extra-peritoneal rectal rupture.(Courtesy Dr.V.Penopoulos).

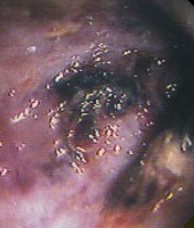
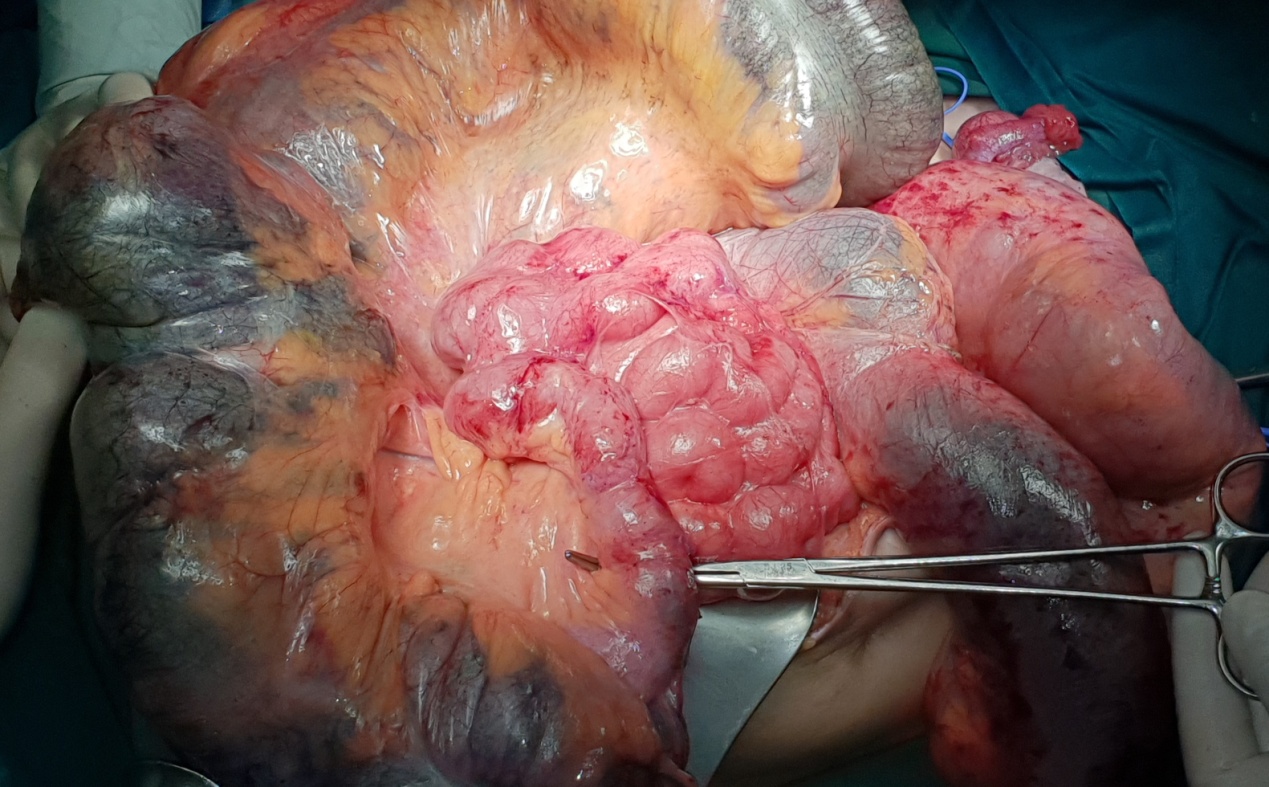
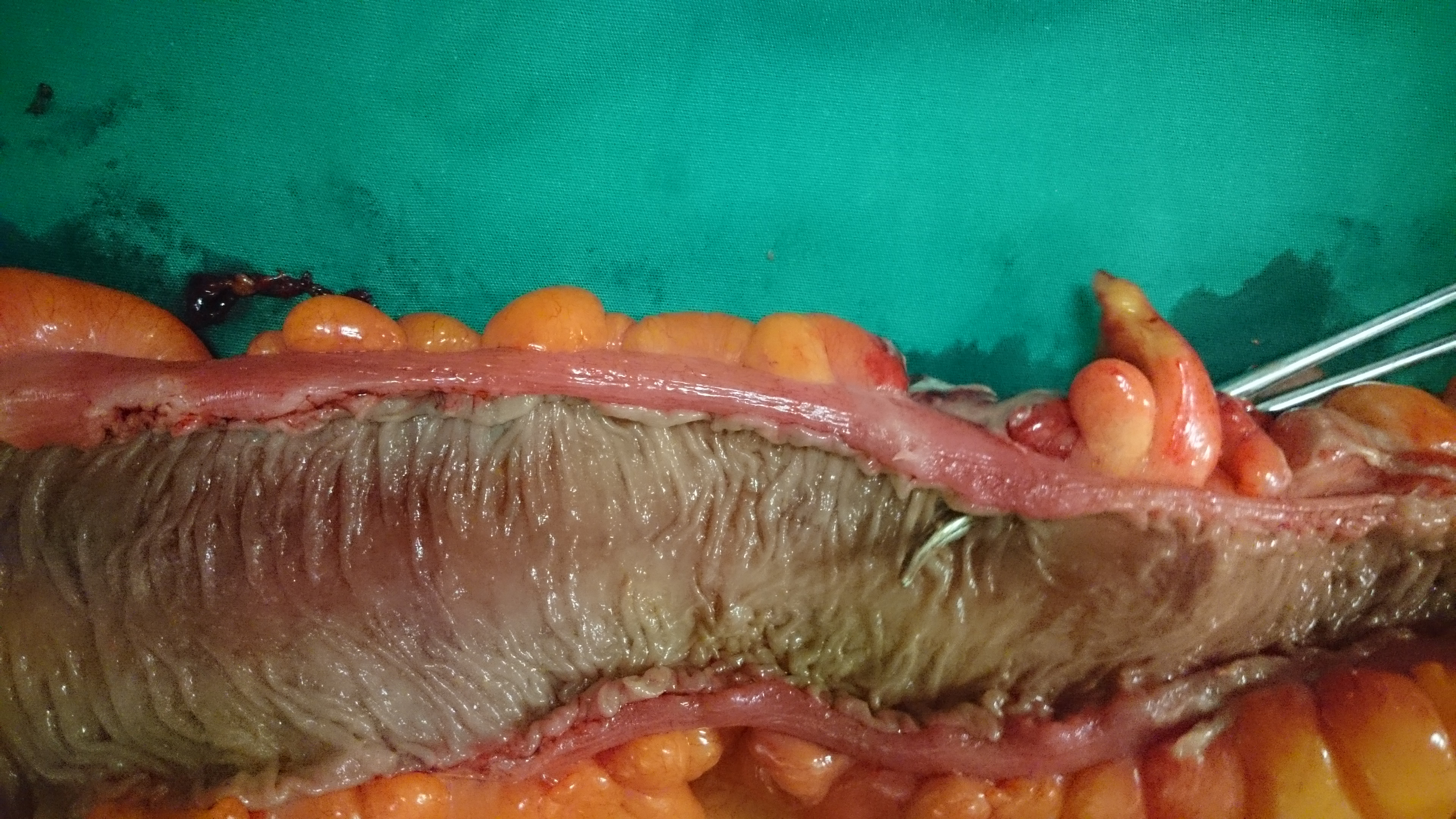
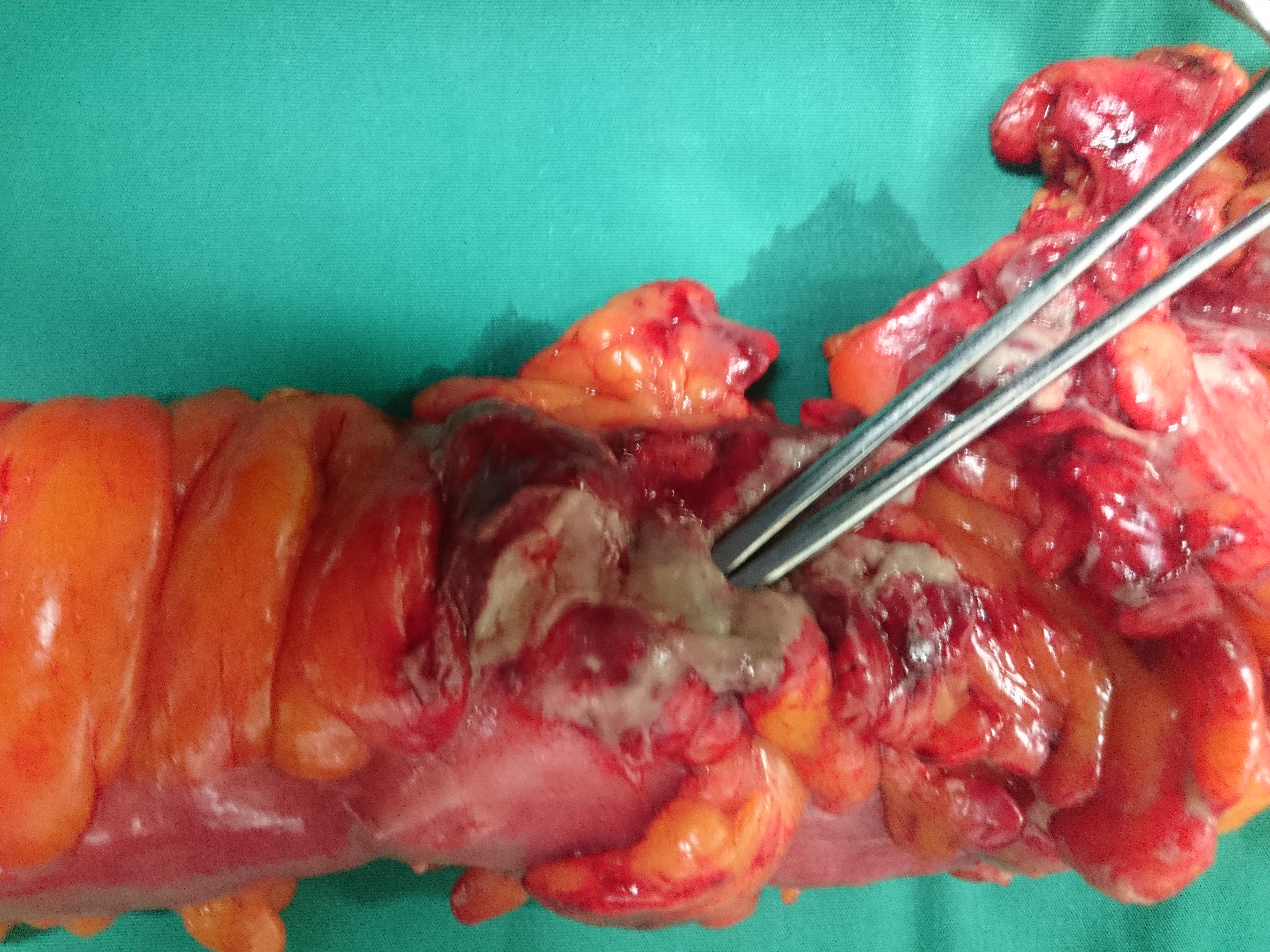
Pseudo-obstruction of a pitch-black Colon . Subtotal colectomy specimen (Courtesy Dr. V. Penopoulos)
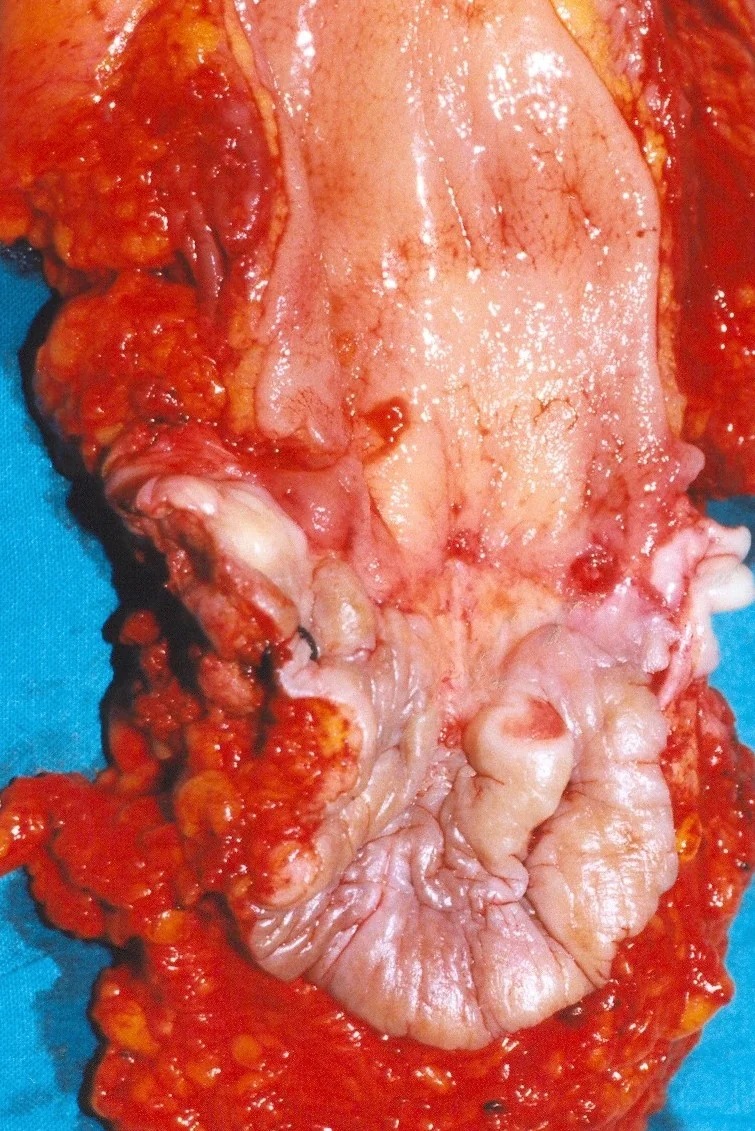
Resected rectosigmoid colon. The site of the perforated diverticular abscess is evident


Plain abdominal X - Ray showing large bowel dilatation - Toxic Megacolon.( Courtesy Dr . V . Penopoulos ).
The site of the perforated diverticular abscess is evident.(Courtesy Dr.V.Penopoulos).


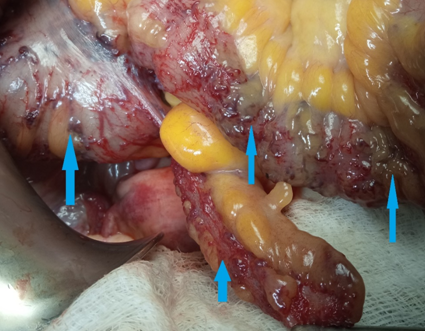
Figure 3 . Subserosal ileocolic varices of no significance . ( Courtesy Dr . V . Penopoulos ) .
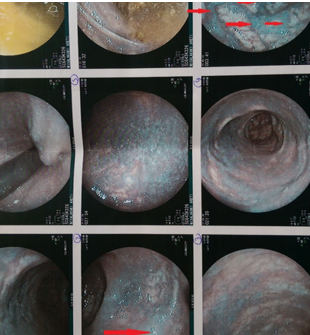
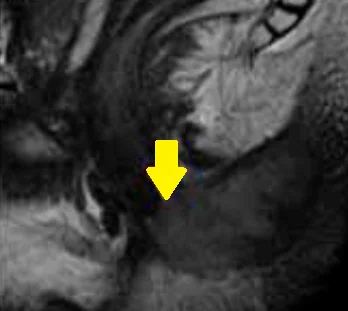
Figure 1 . Rectal submucosal varices are clearly seen . ( Courtesy Dr . V . Penopoulos ) .
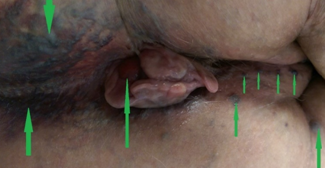
Figure 5 . Lumbar region and perianal varices together with prolapsed hemorrhoids prior to surgery . No anomaly in the iliac vessels was detected . (Courtesy Dr . V . Penopoulos) .
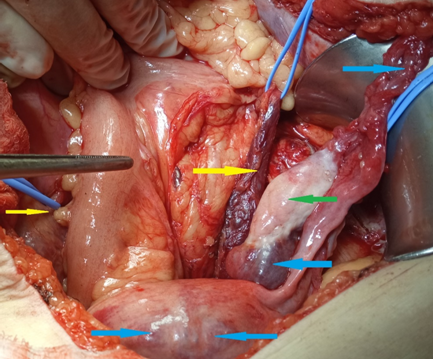
Figure 2 . Pelvic congestion syndrome . Dilated left ovarian veins , left ureteric veins , ovarian varix and para-uterine veins . ( Courtesy Dr . V . Penopoulos ) .

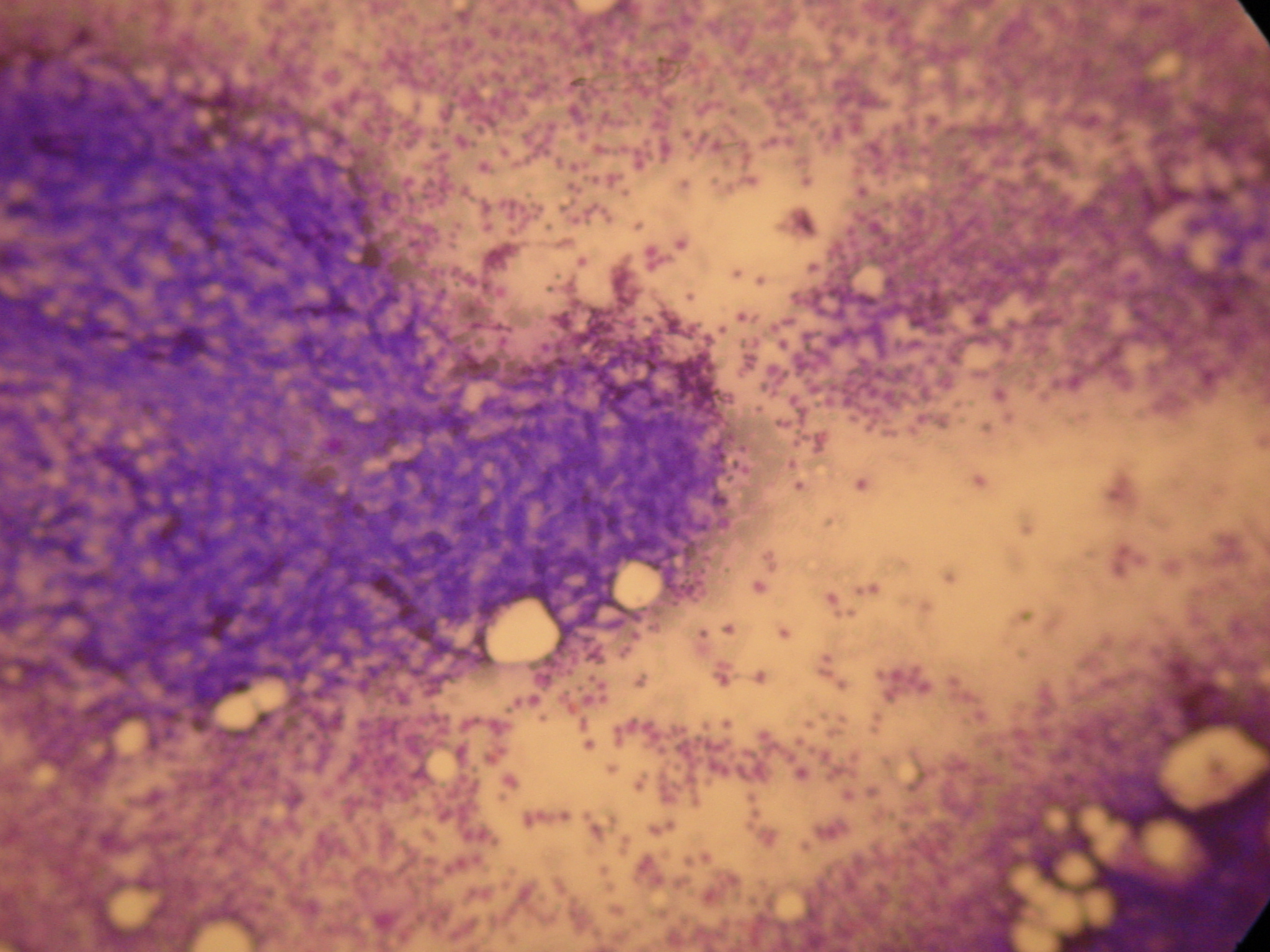
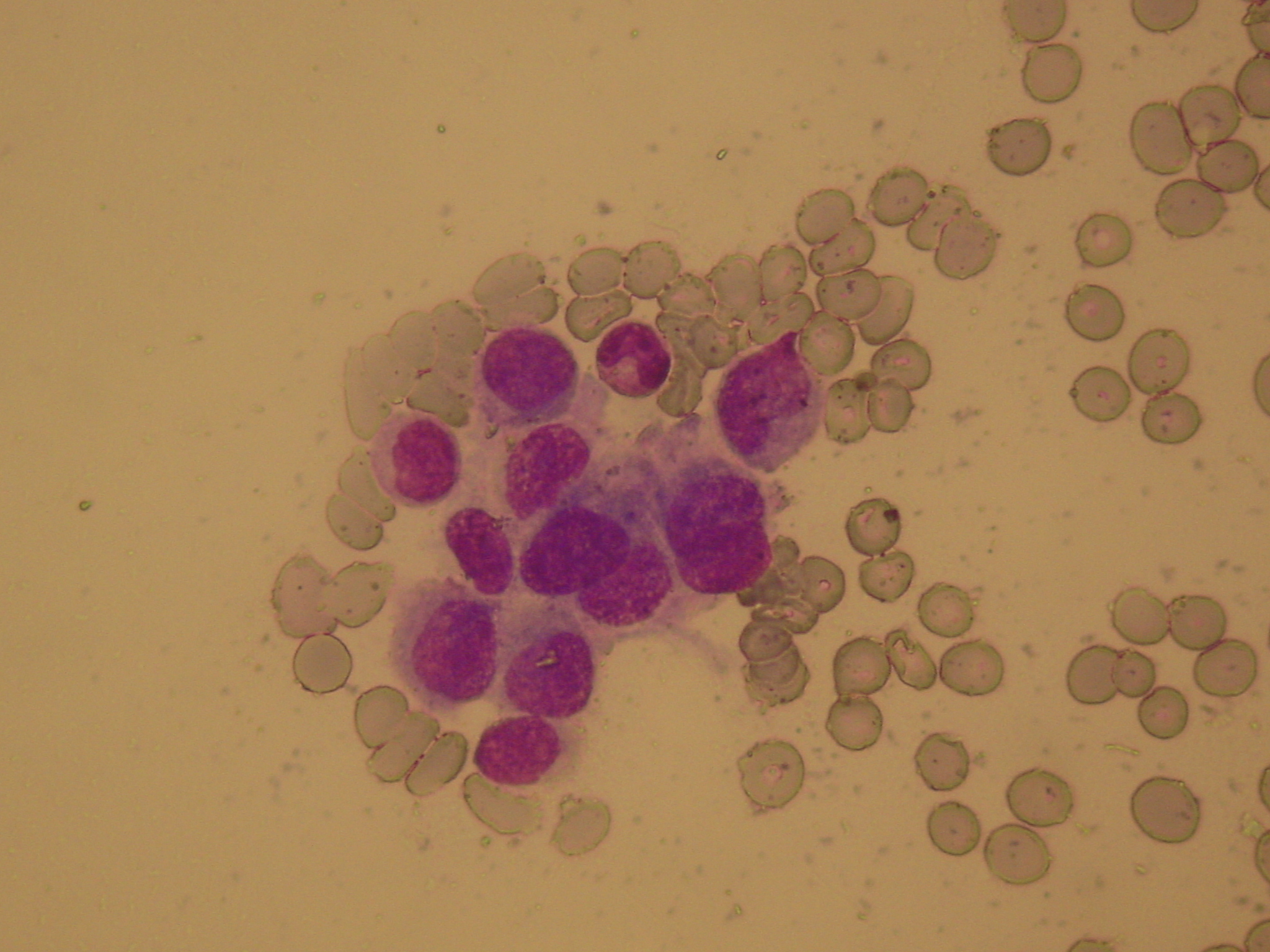
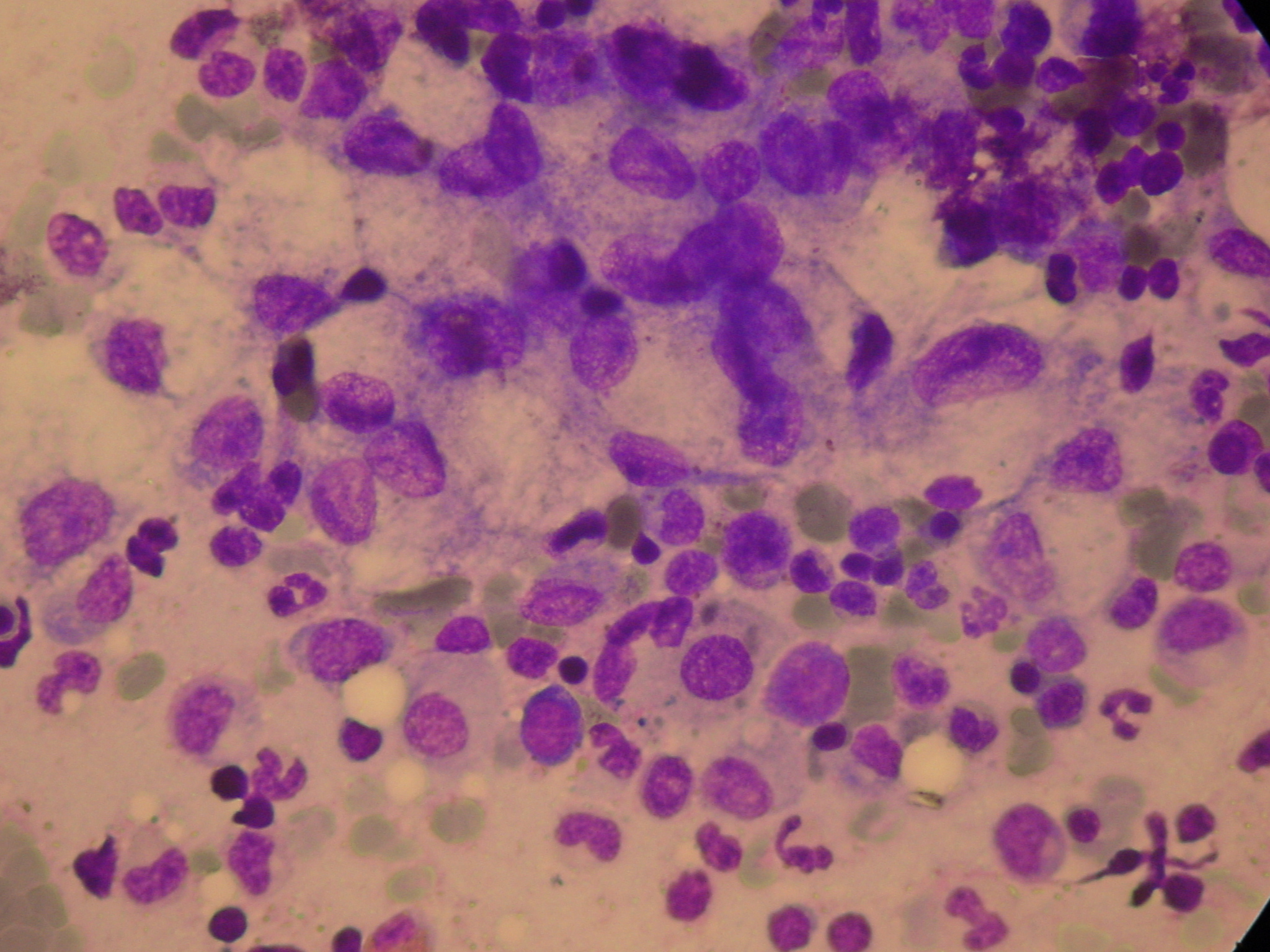
Infiltrated lymph nodes with both cancerous and atypical lymphocytes (Courtesy Dr. V. Penopoulos)
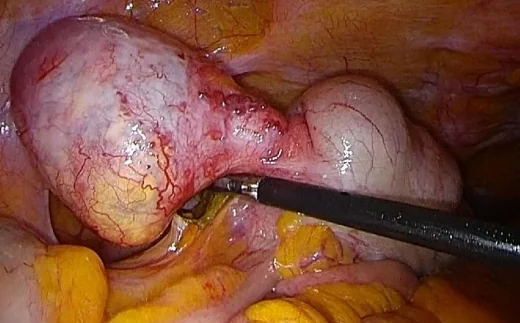
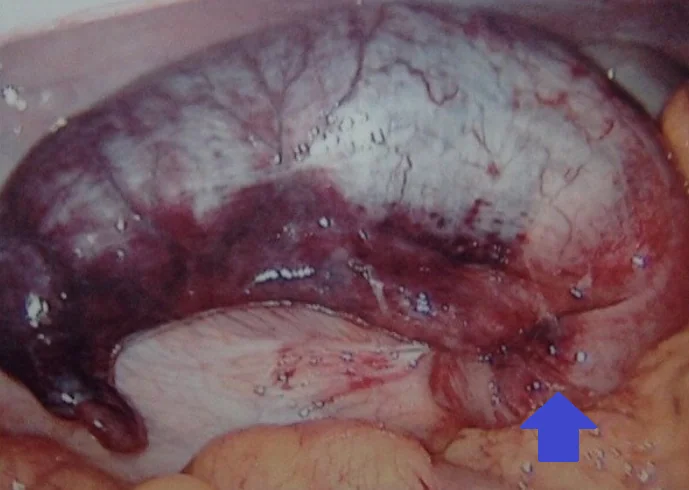
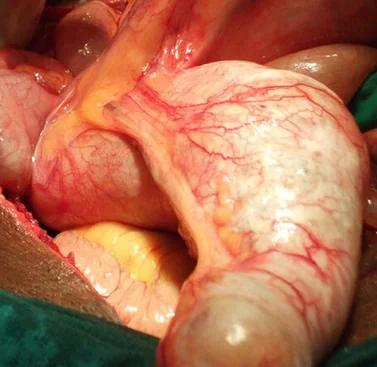
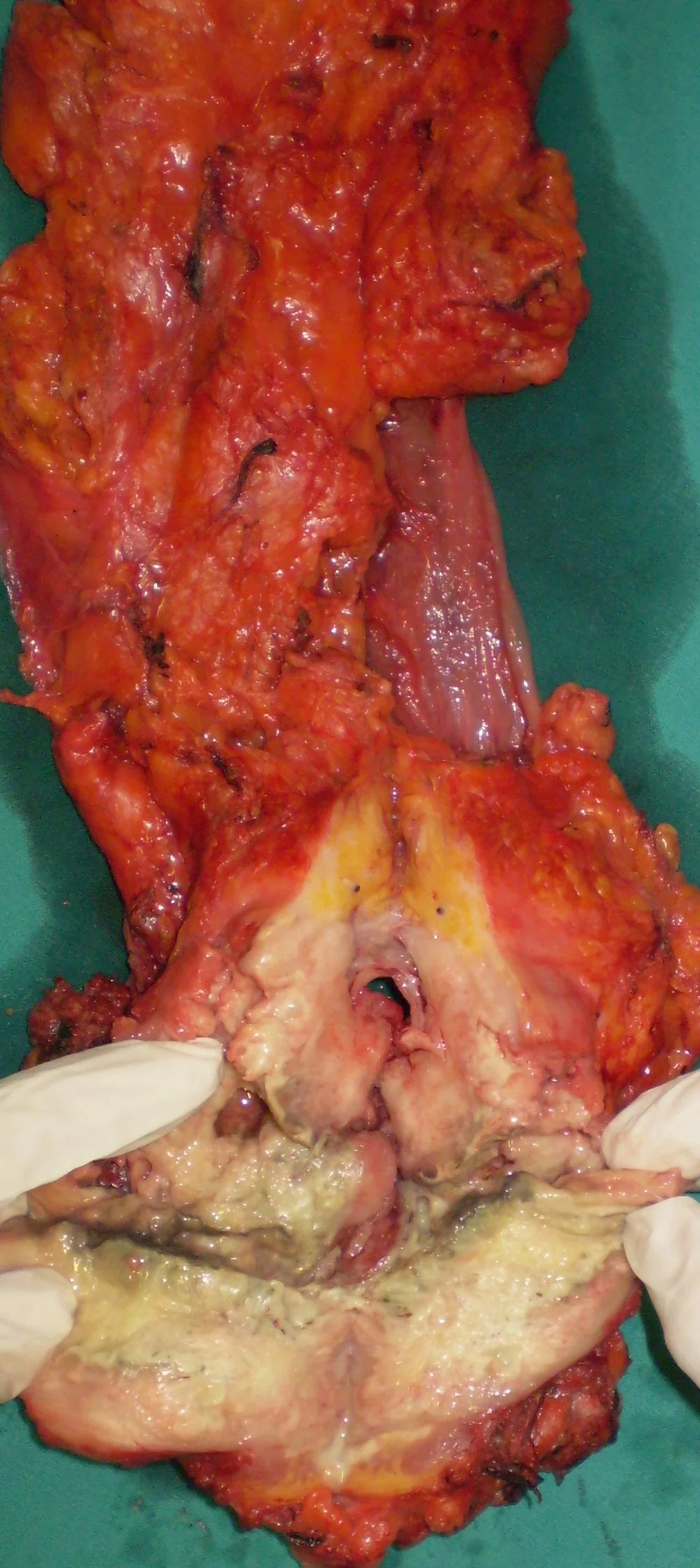
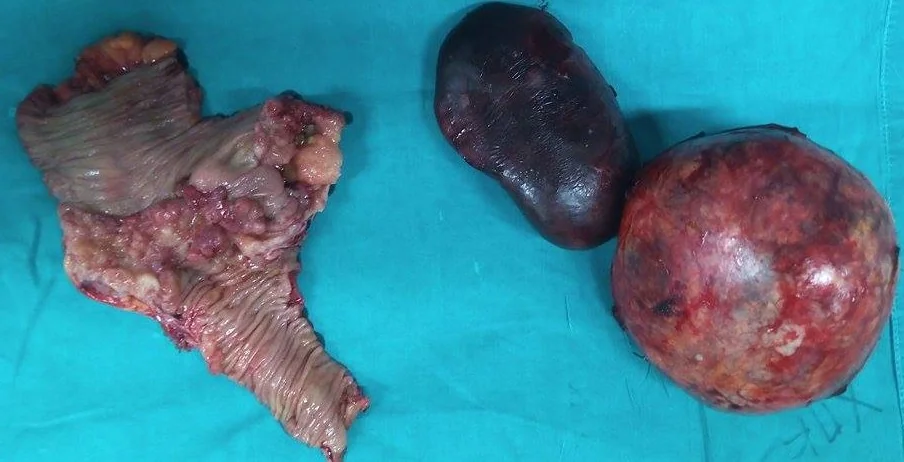
The excised mass together with right hemi colon and abdominal wall (Courtesy Dr. V. Penopoulos)

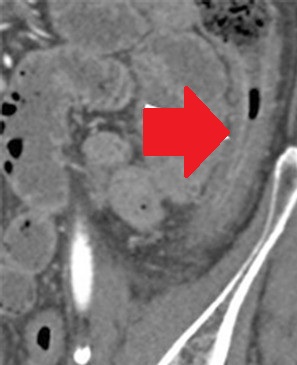
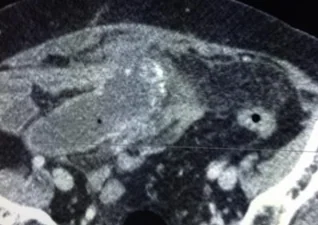
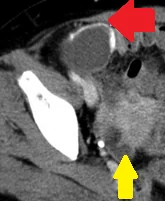
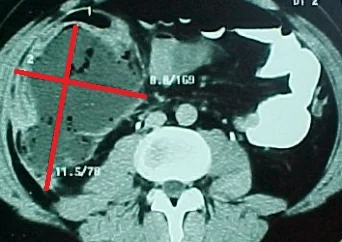
Abdominal CT Scan pictures, showing cystic type lesion, between liver and colonic hepatic flexure, in contact with the bowel outer layer expressing enriched wall and low density centre (Courtesy Dr. V. Penopoulos)

Plain abdominal radiograph. Distension of the ileal pouch and its displacement to the right side of the abdomen (Courtesy Dr. V. Penopoulos)
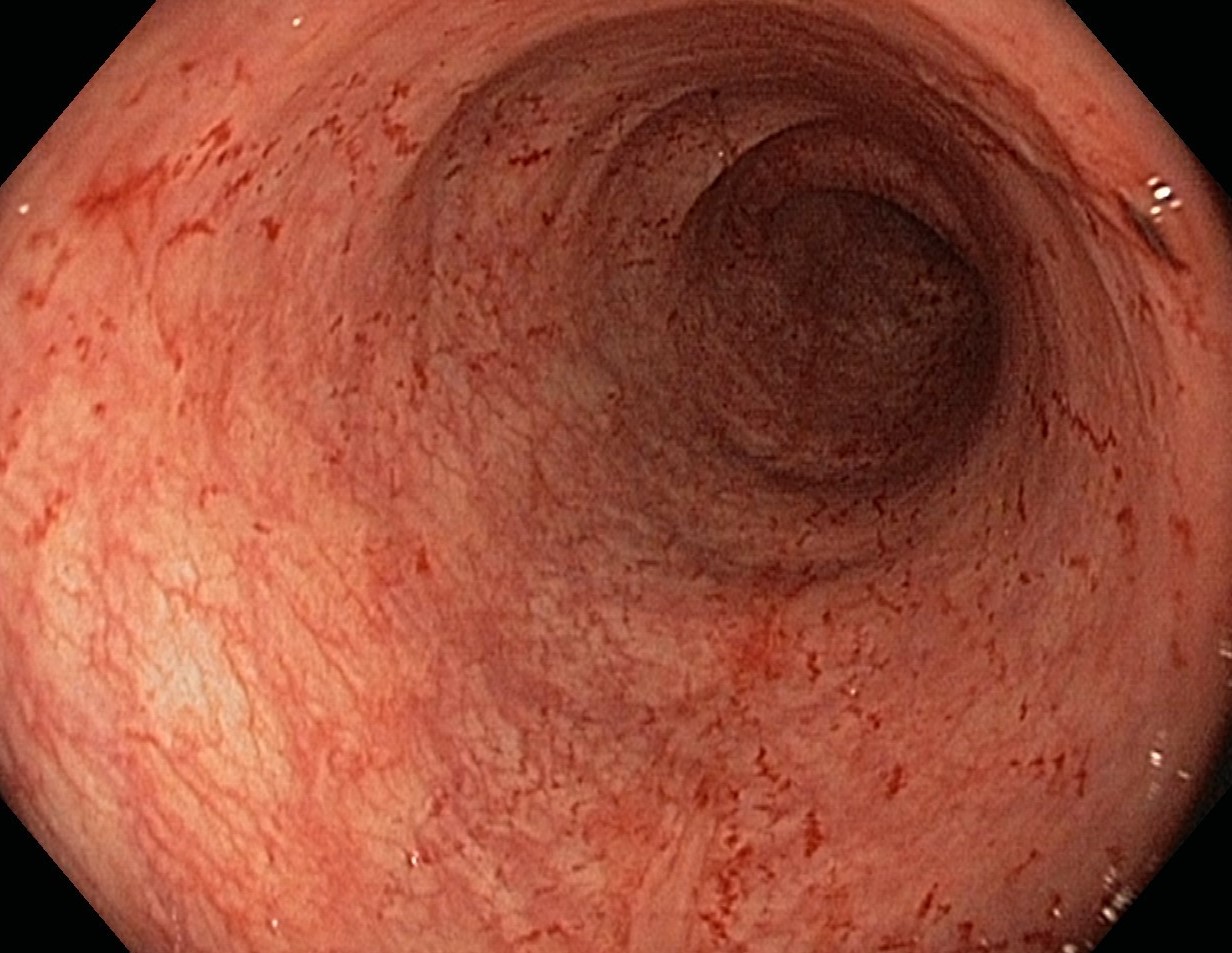
Postoperative biopsies of ileal pouch - Pouch adaptation (Courtesy Dr. V. Penopoulos)
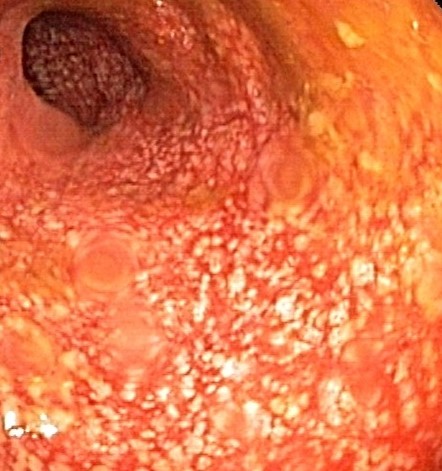
Intraoperative image of chronically inflamed, distended, dysfunctional pouch with associated proximal small bowel distension (Courtesy Dr. V. Penopoulos)
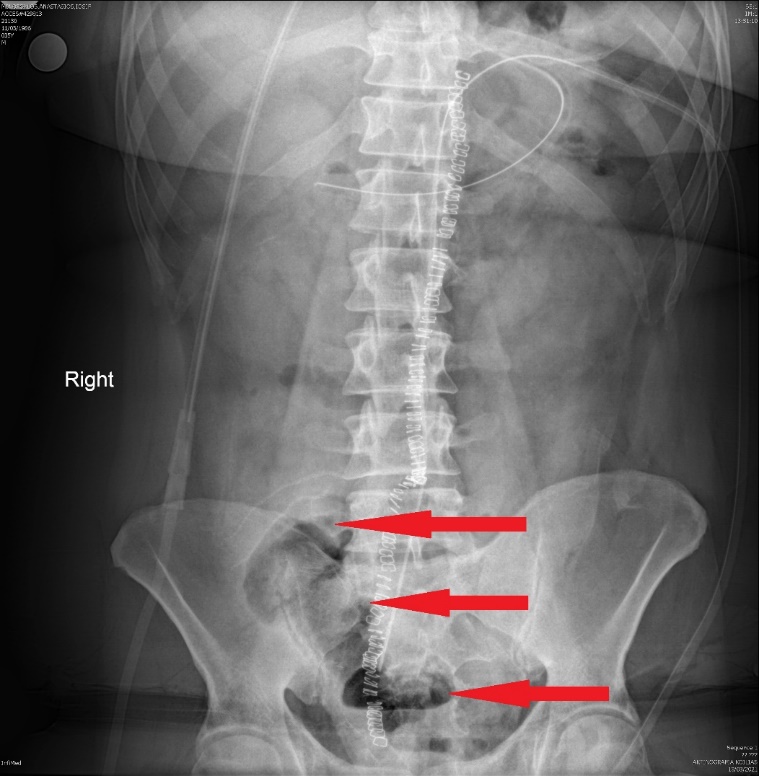
Plain abdominal radiograph - Multicolored arrows - Rigler sign (Courtesy Dr. V. Penopoulos)
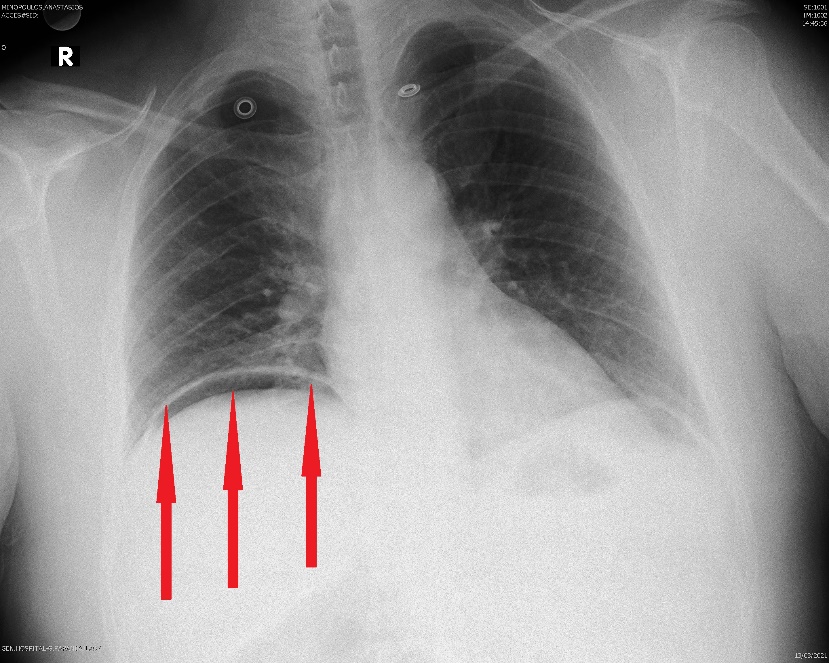
Plain chest X-Ray.Red arrows.Free subdiaphragmatic air on the right.(Courtesy Dr.V.Penopoulos).