Small Intestine
Λεπτό Έντερο
123 images
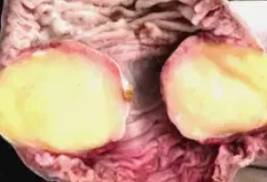






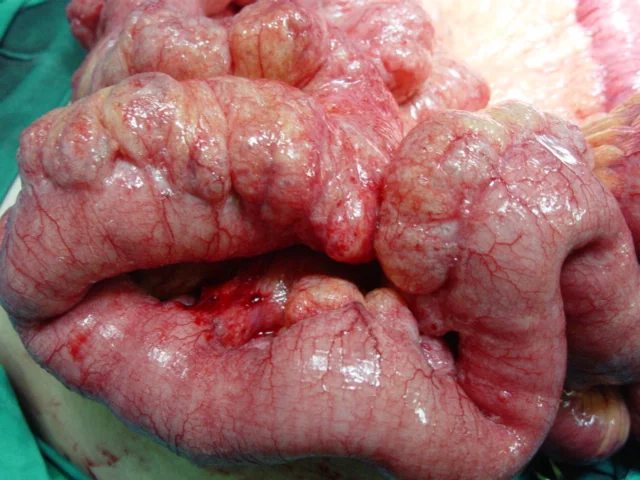










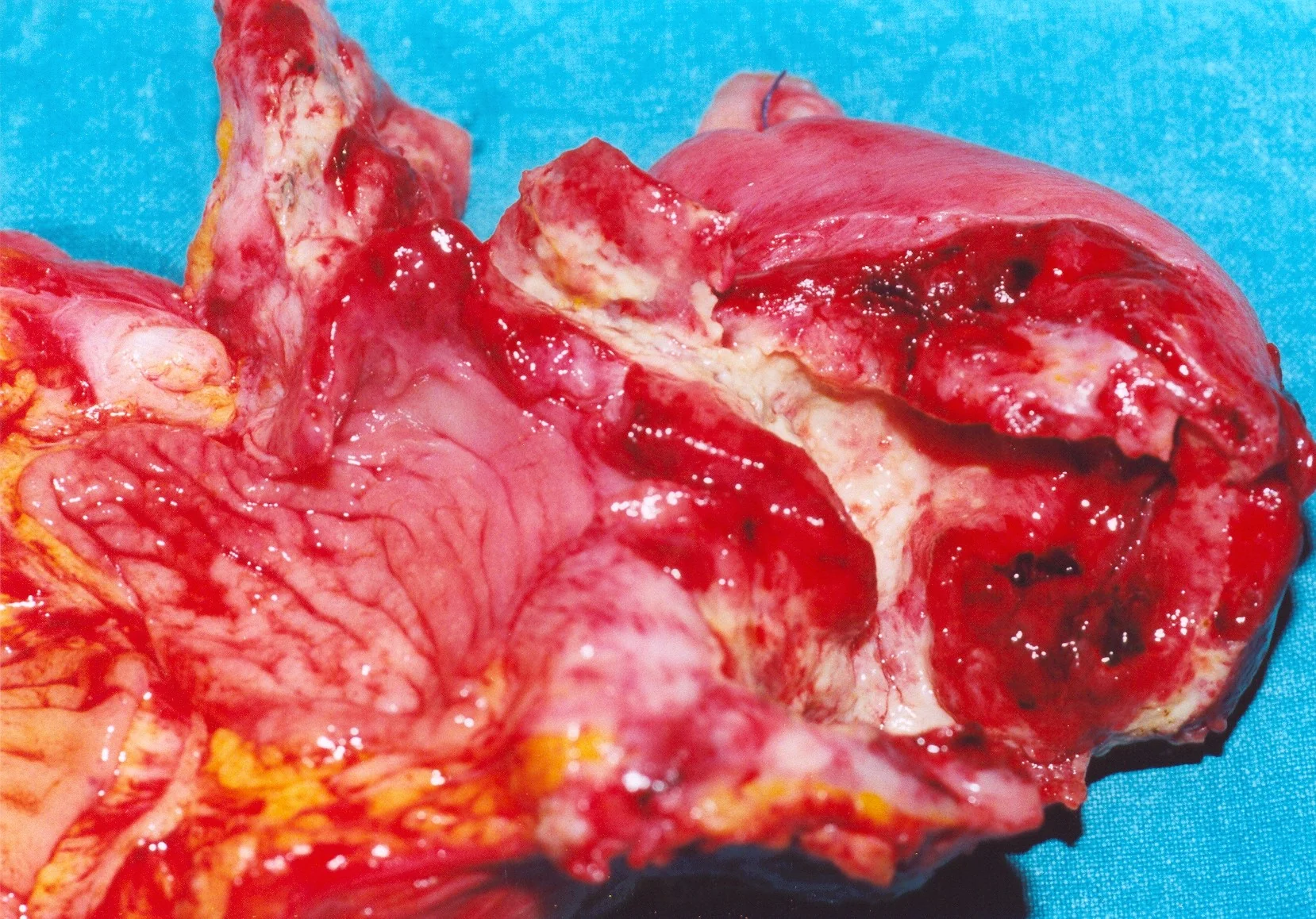







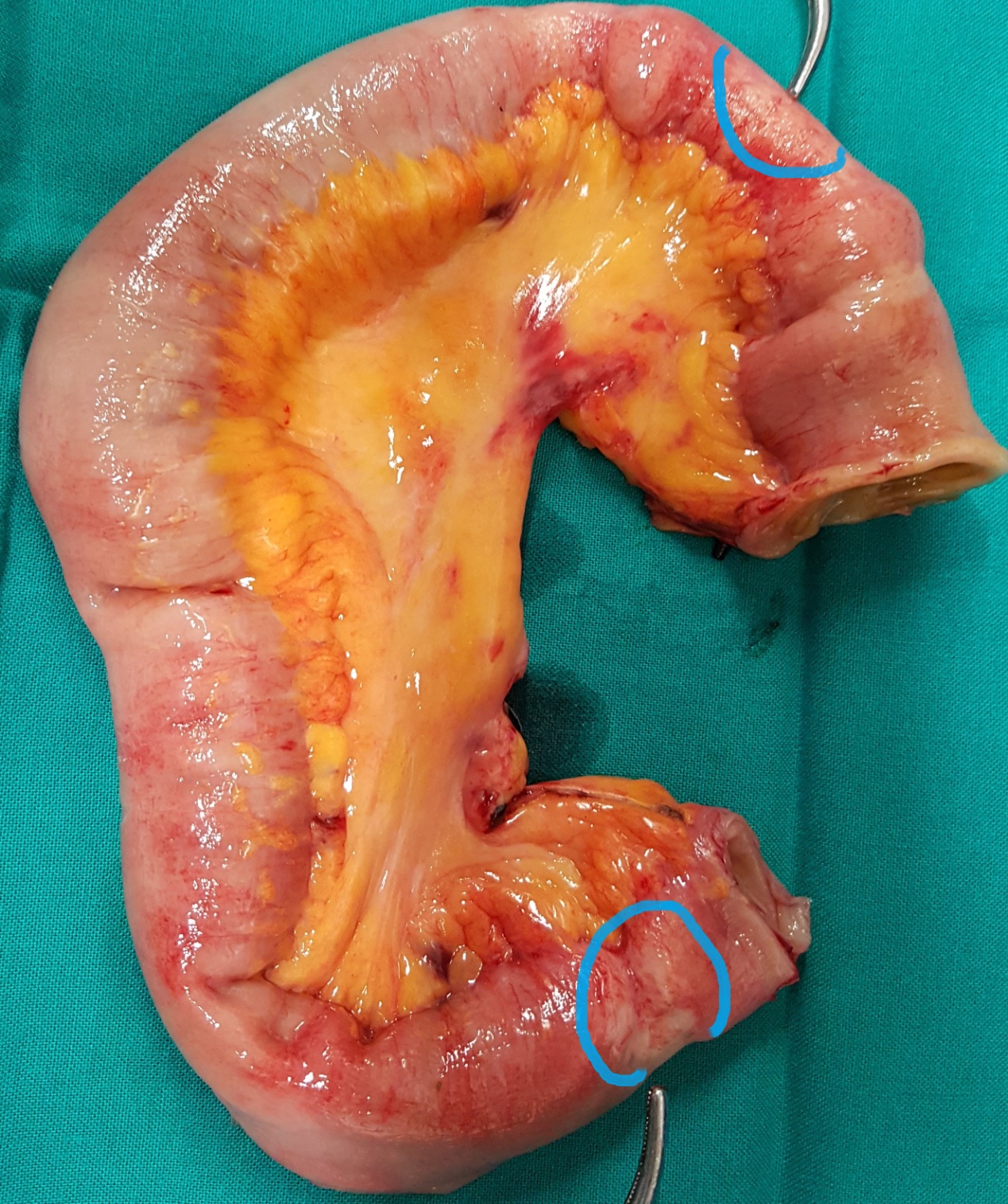
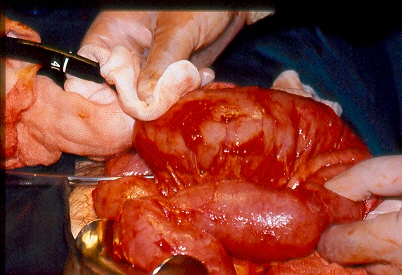
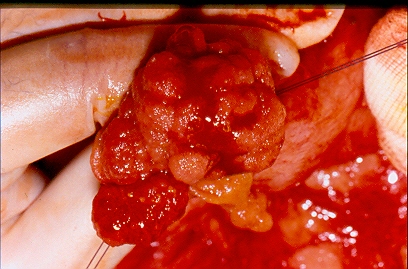
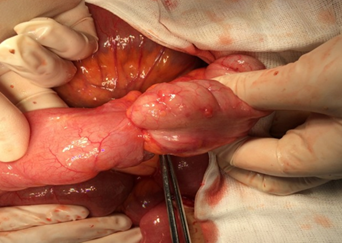
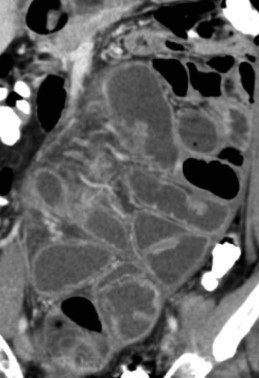
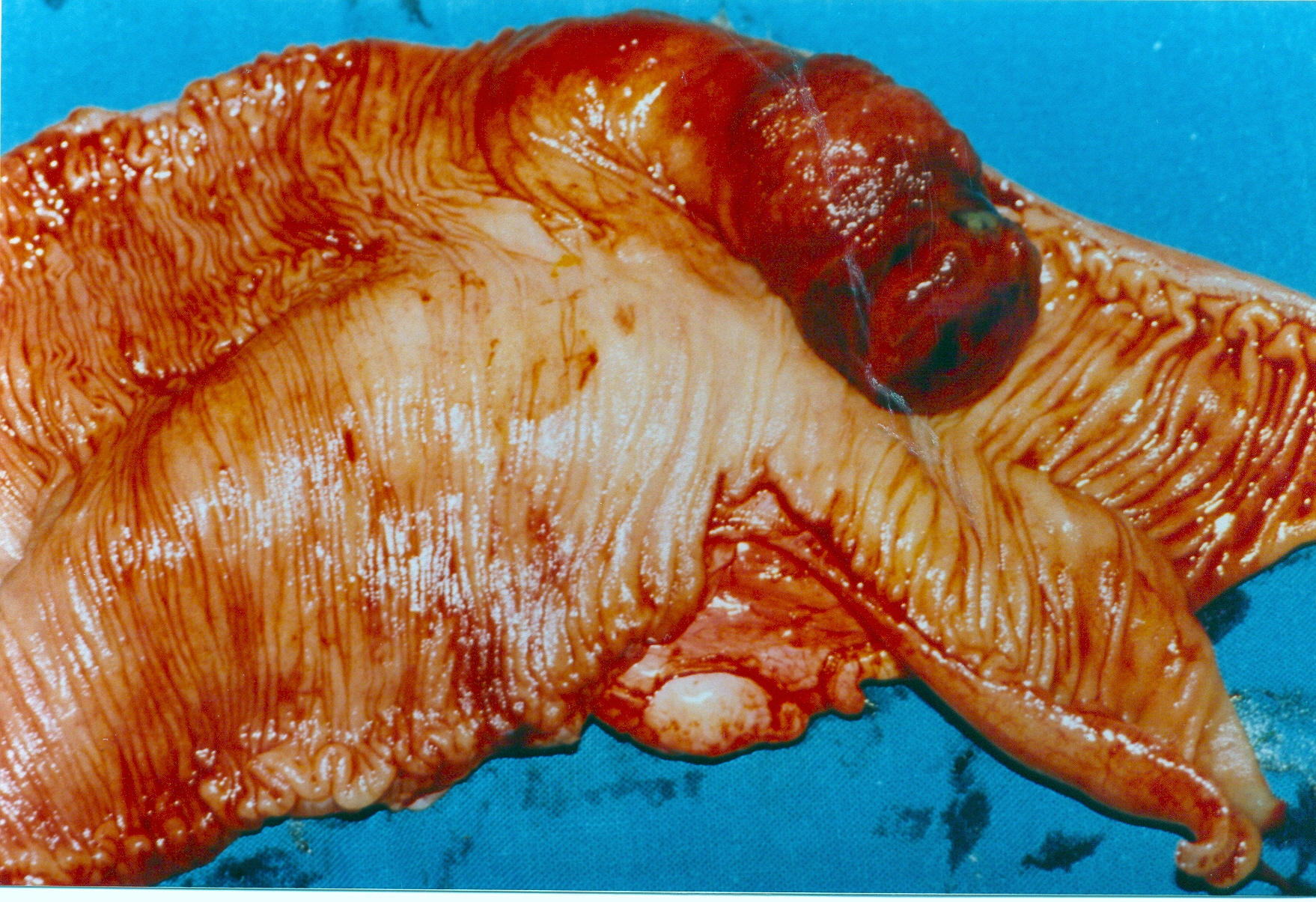
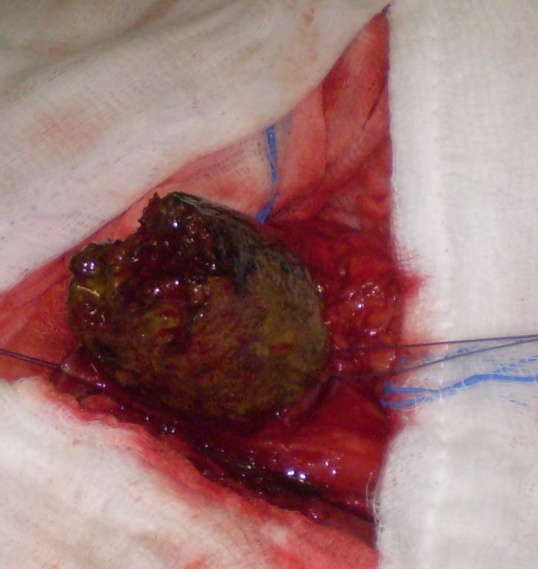
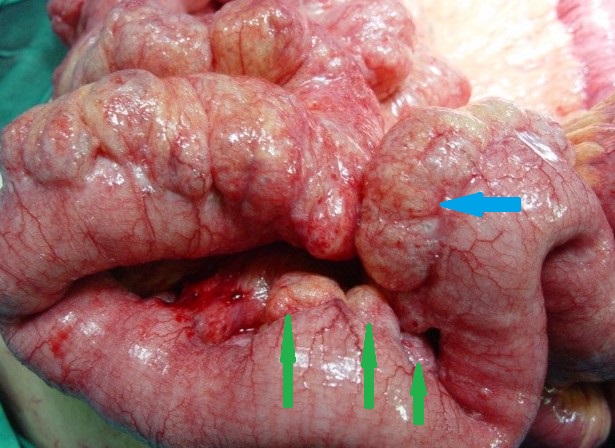
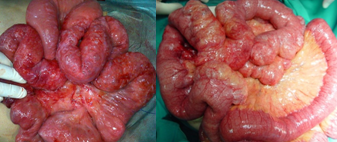
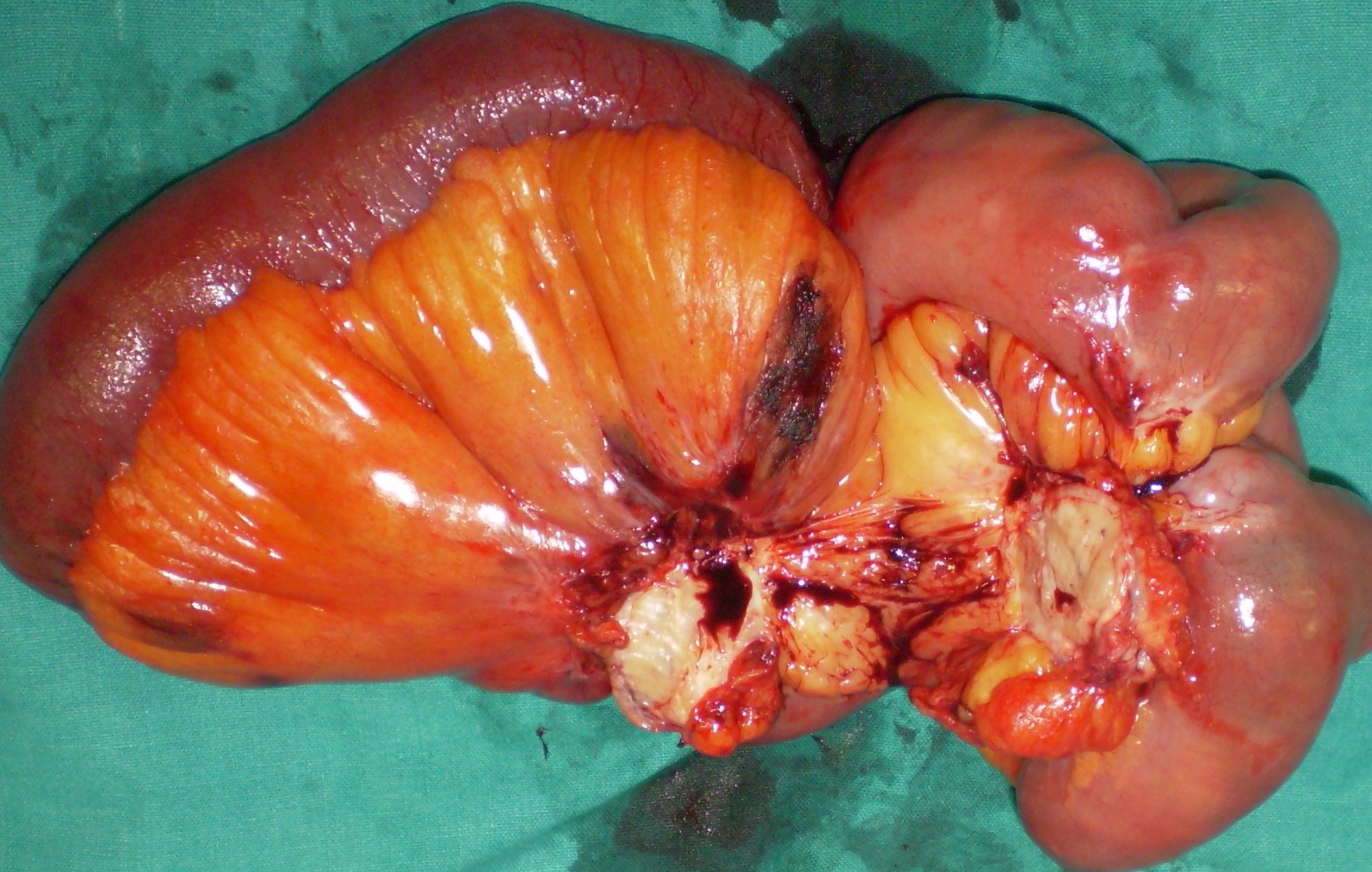
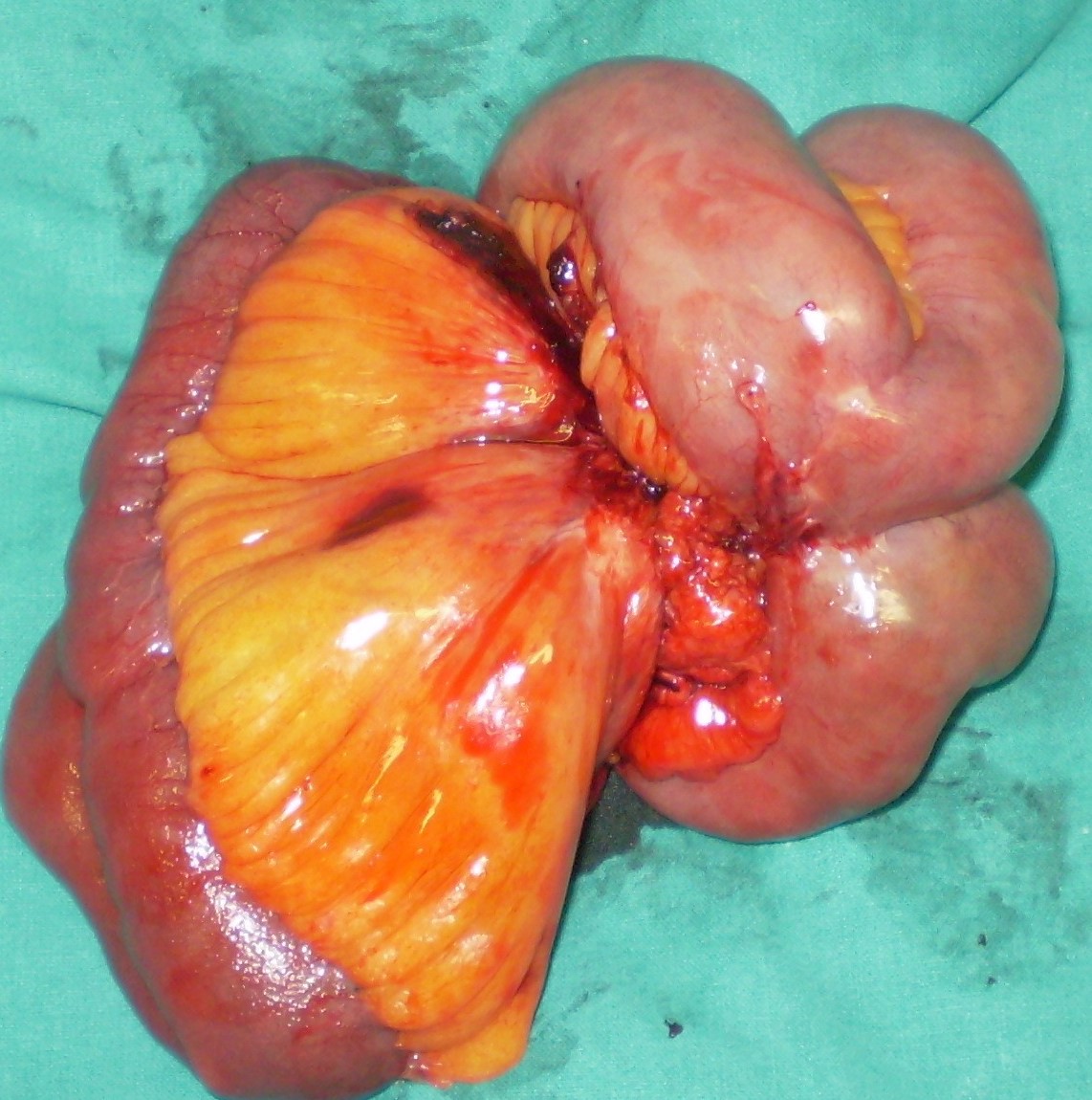
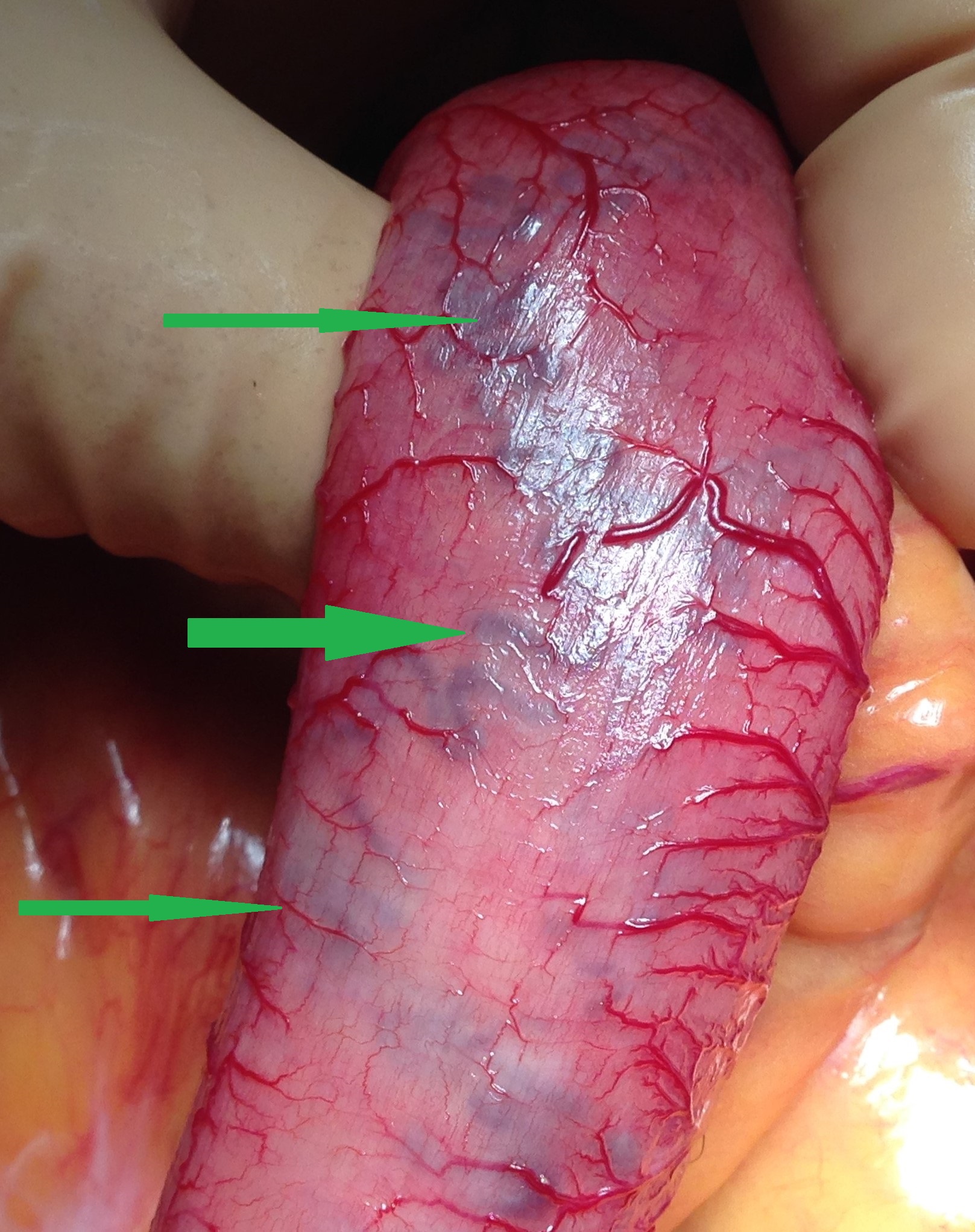
Resected obstructed ileal loop. Blue circles enclose the metastatic foci (Courtesy Dr. V. Penopoulos)
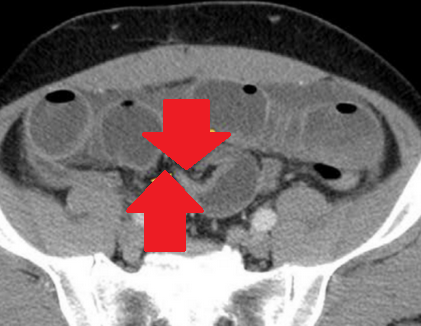
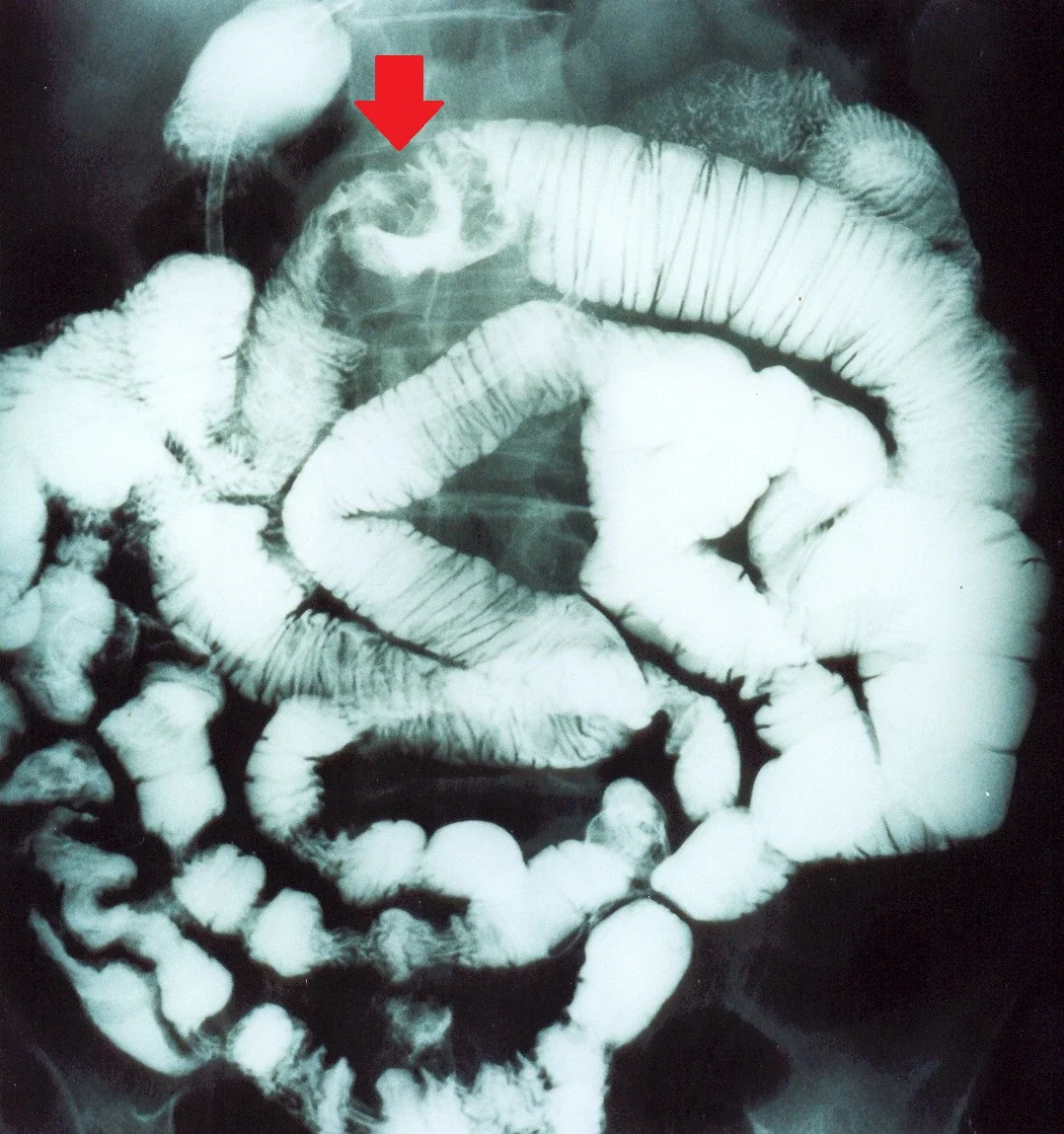
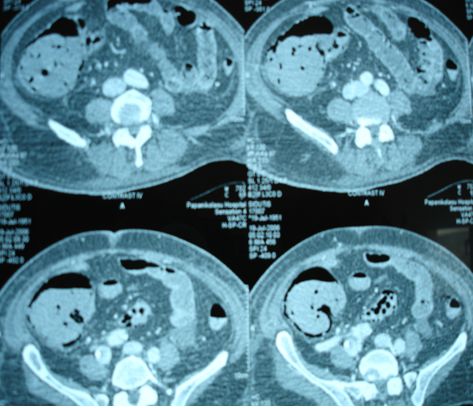
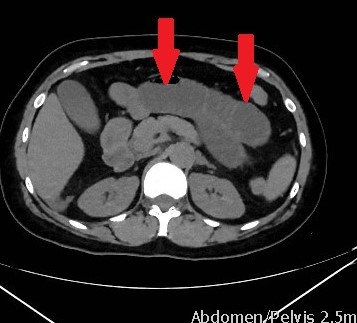
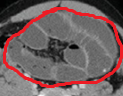
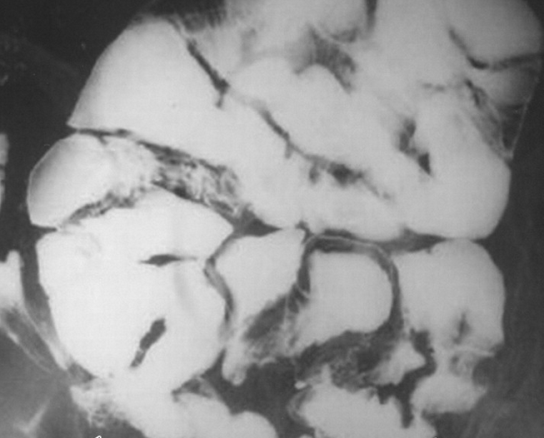
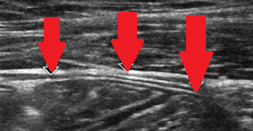
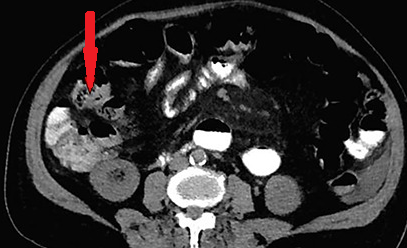
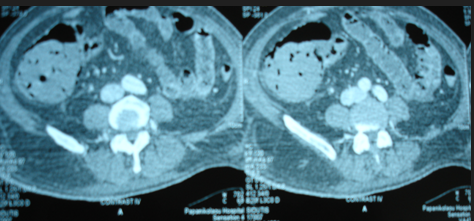
Red arrows — transition point. Multiple air-fluid levels (Courtesy Dr. V. Penopoulos)

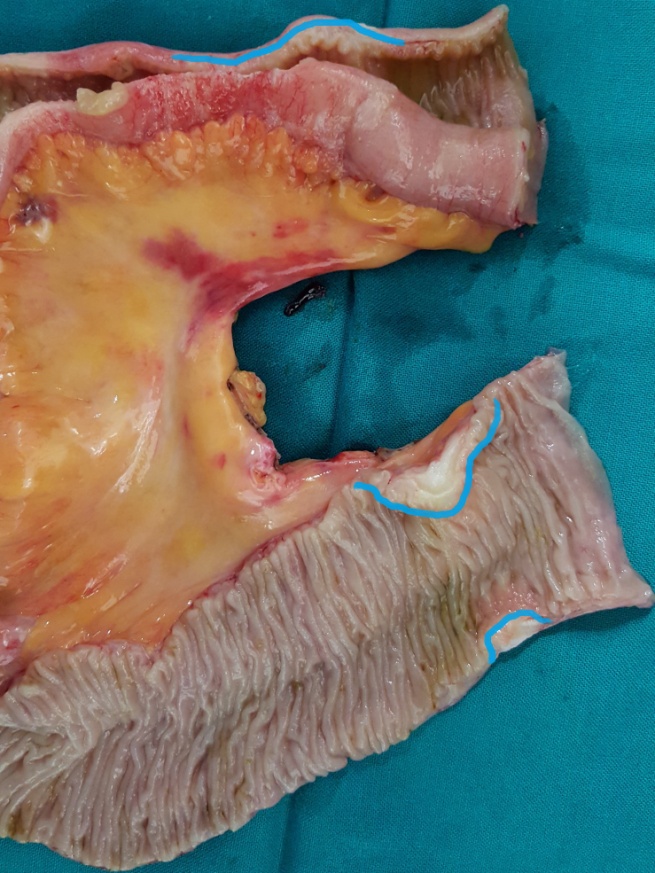
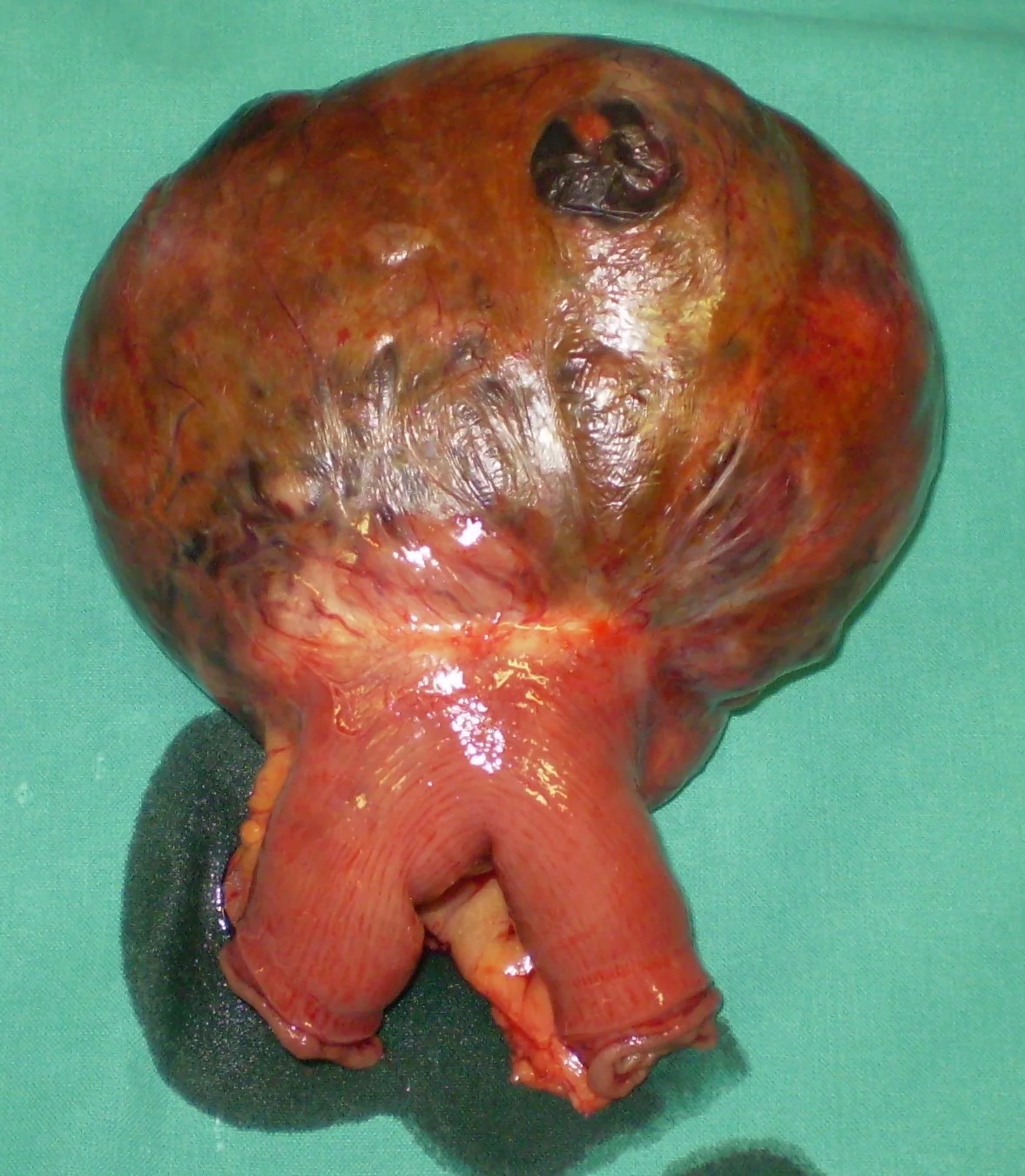
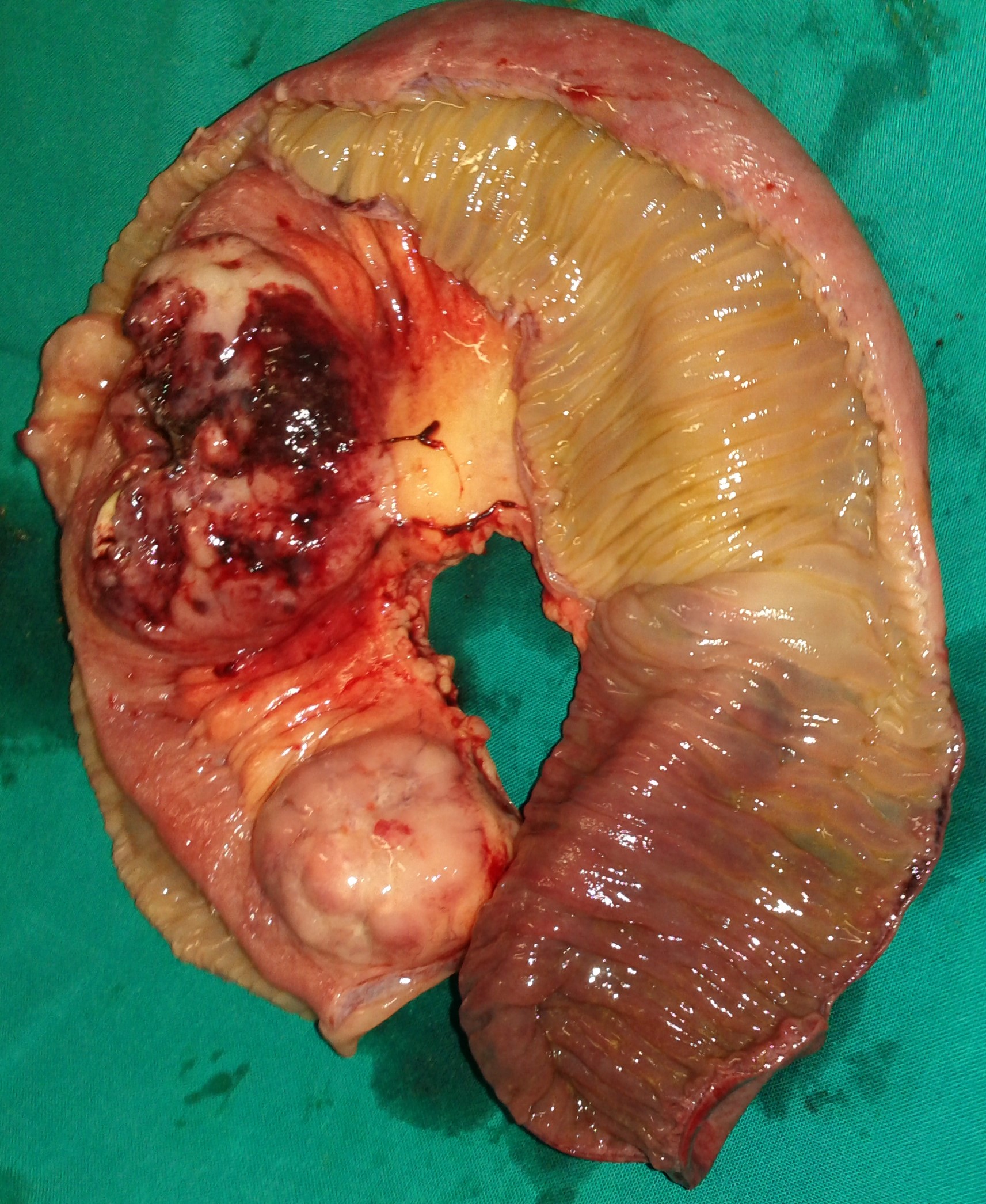
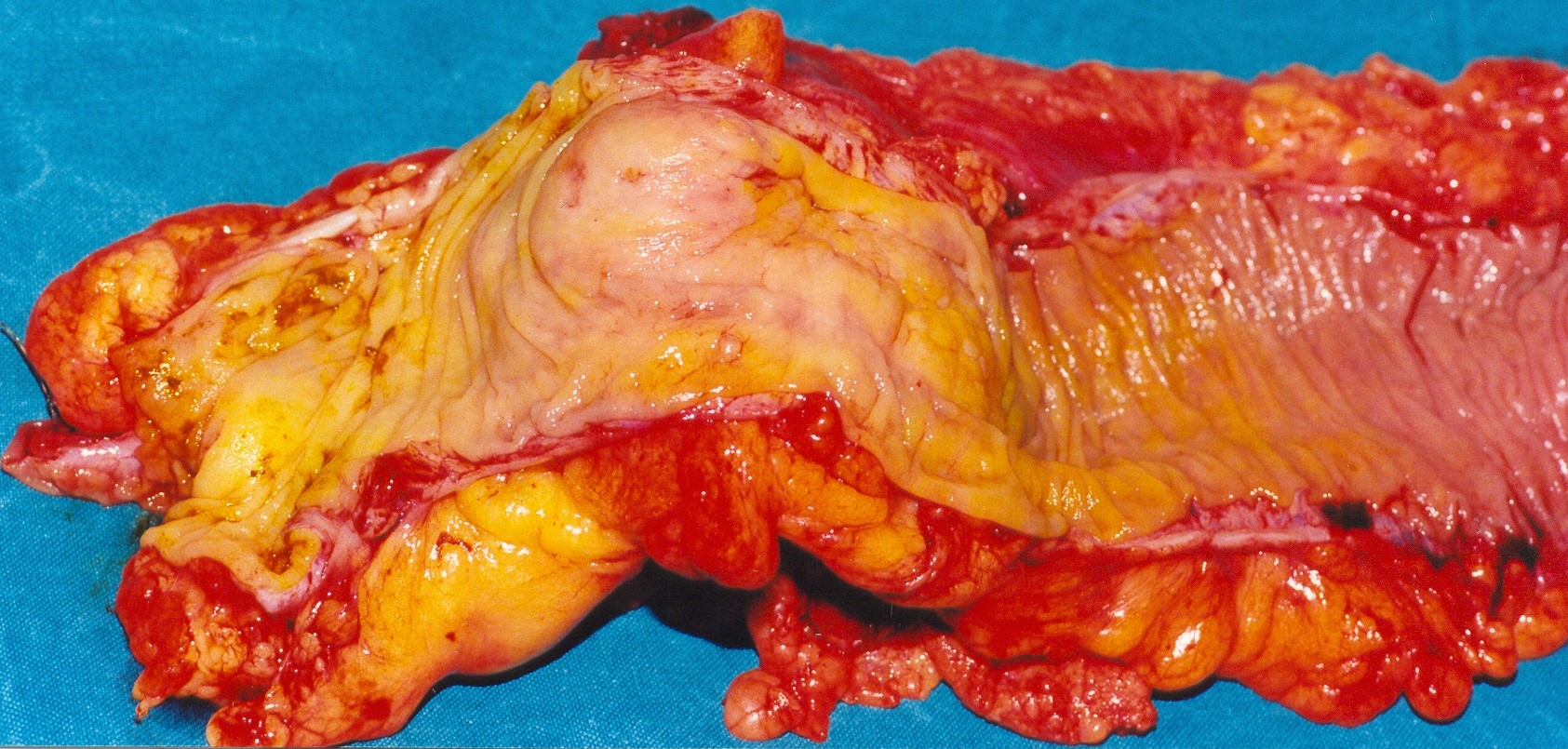
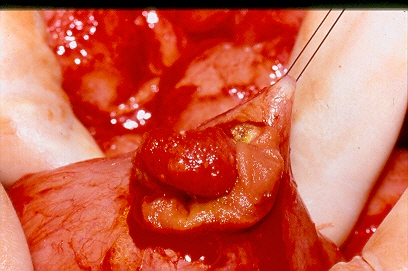
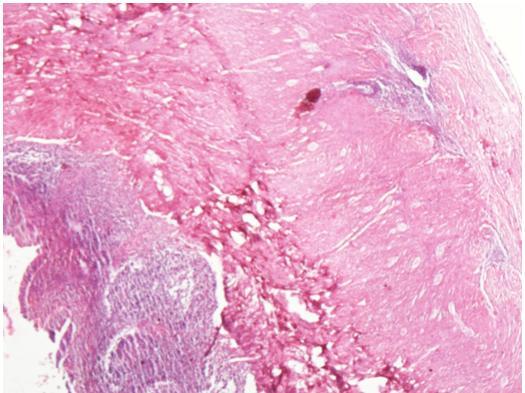
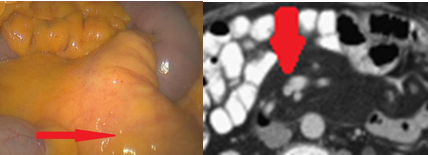
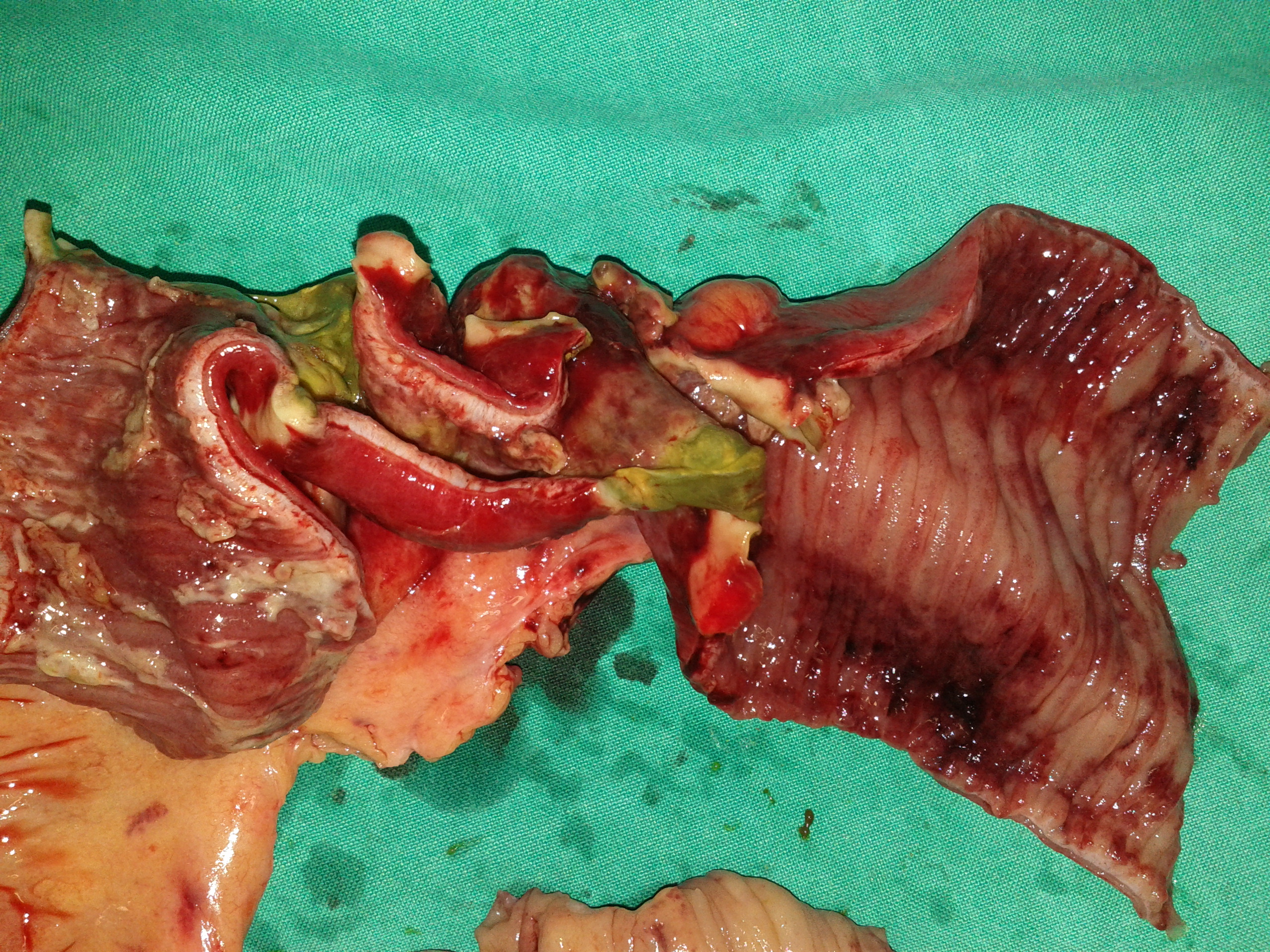
Metastatic Lesions from urothelial bladder carcinoma . (Courtesy Dr. V. Penopoulos)
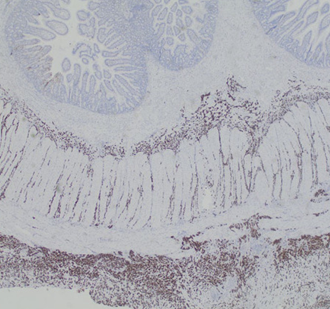
Immunohistochemical staining for Cytokeratin 7, demonstrating the diffusely infiltrating carcinoma in the submucosa, muscular wall, mesenteric adipose tissue, and serosa (Courtesy Dr. V. Penopoulos)


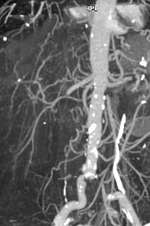
CT Angiography. Ischemic changes of the gastrointestinal tract (Courtesy Dr. V. Penopoulos)


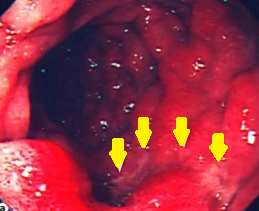
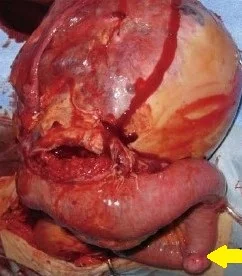
Duodenoscopy. Yellow arrows – Incipient ischemic changes of the third portion of the duodenum due to pressure from the obstruction. Courtesy Dr. V. Penopoulos.
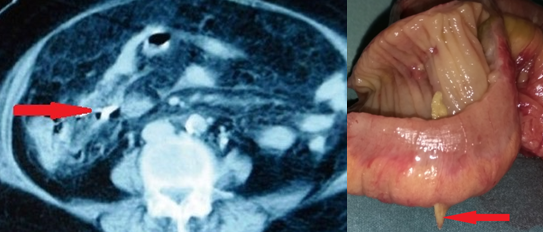
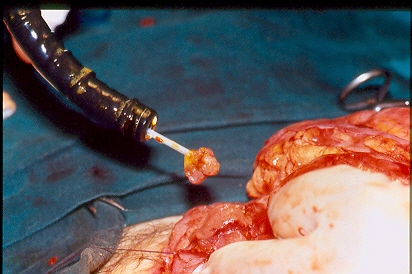
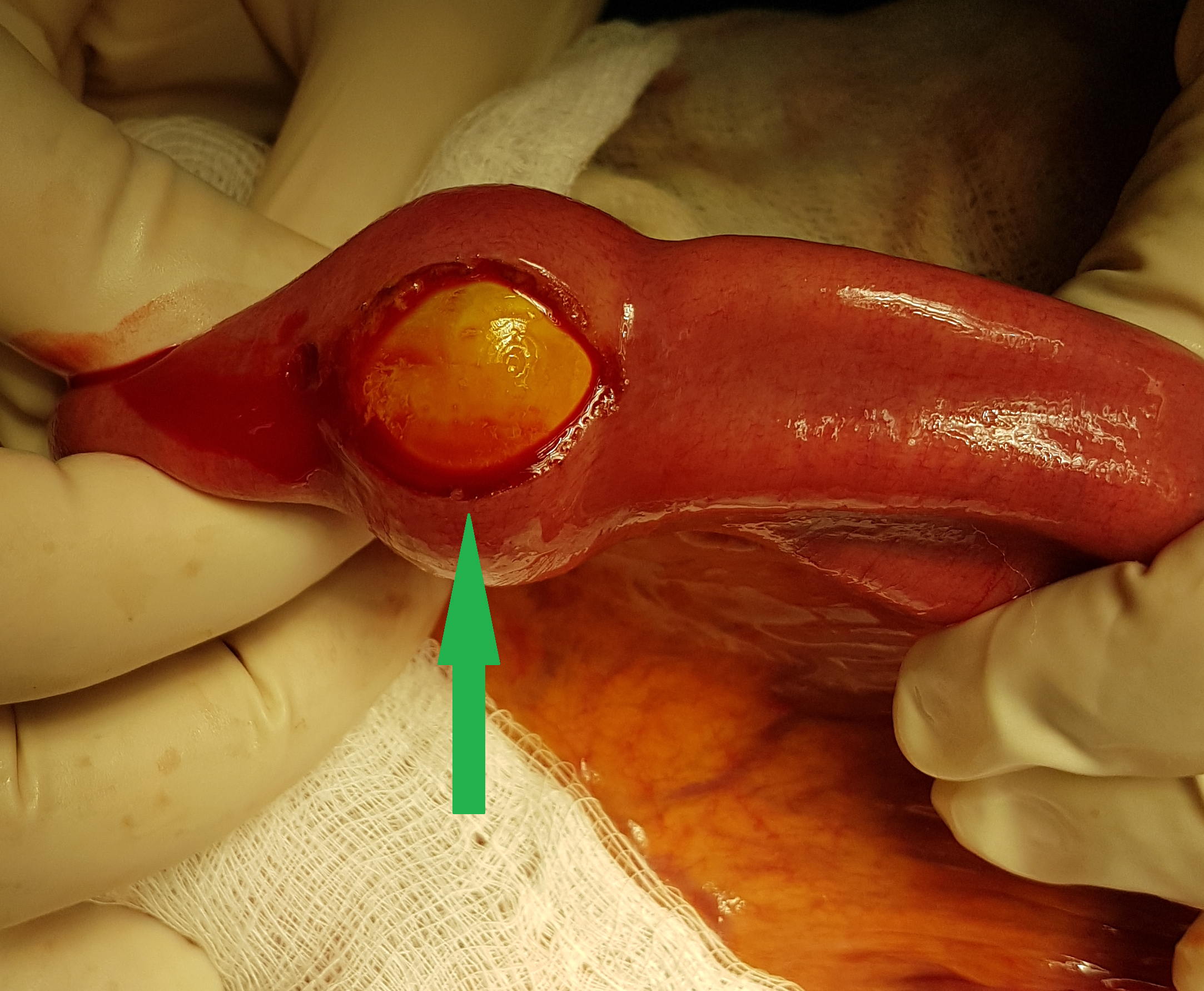
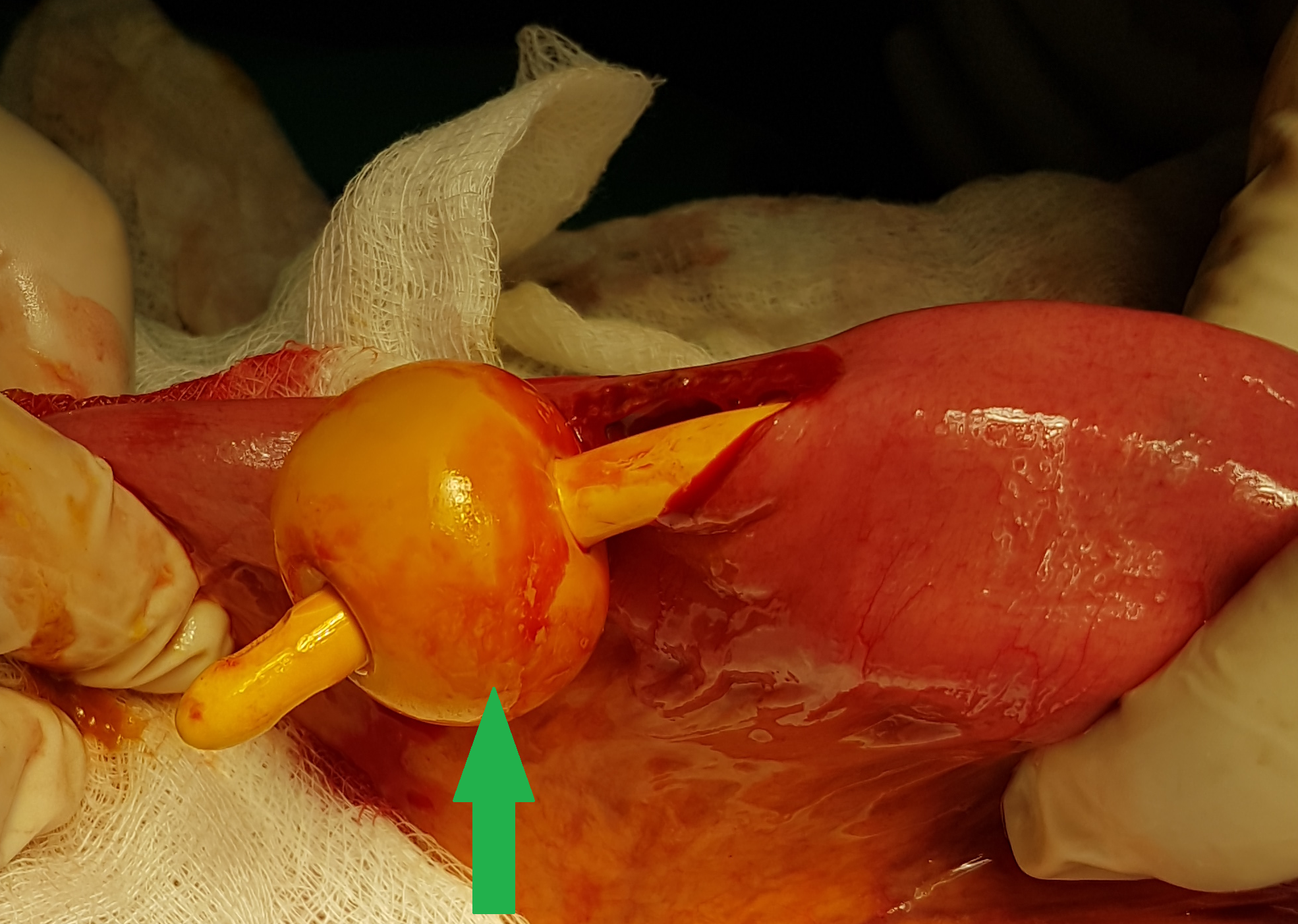
Figure 1 . Bone fragment penetrating the bowel wall . ( Courtesy Dr . V . Penopoulos ) .
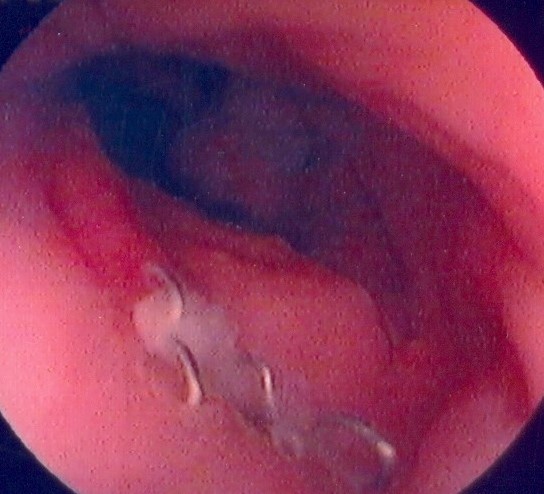
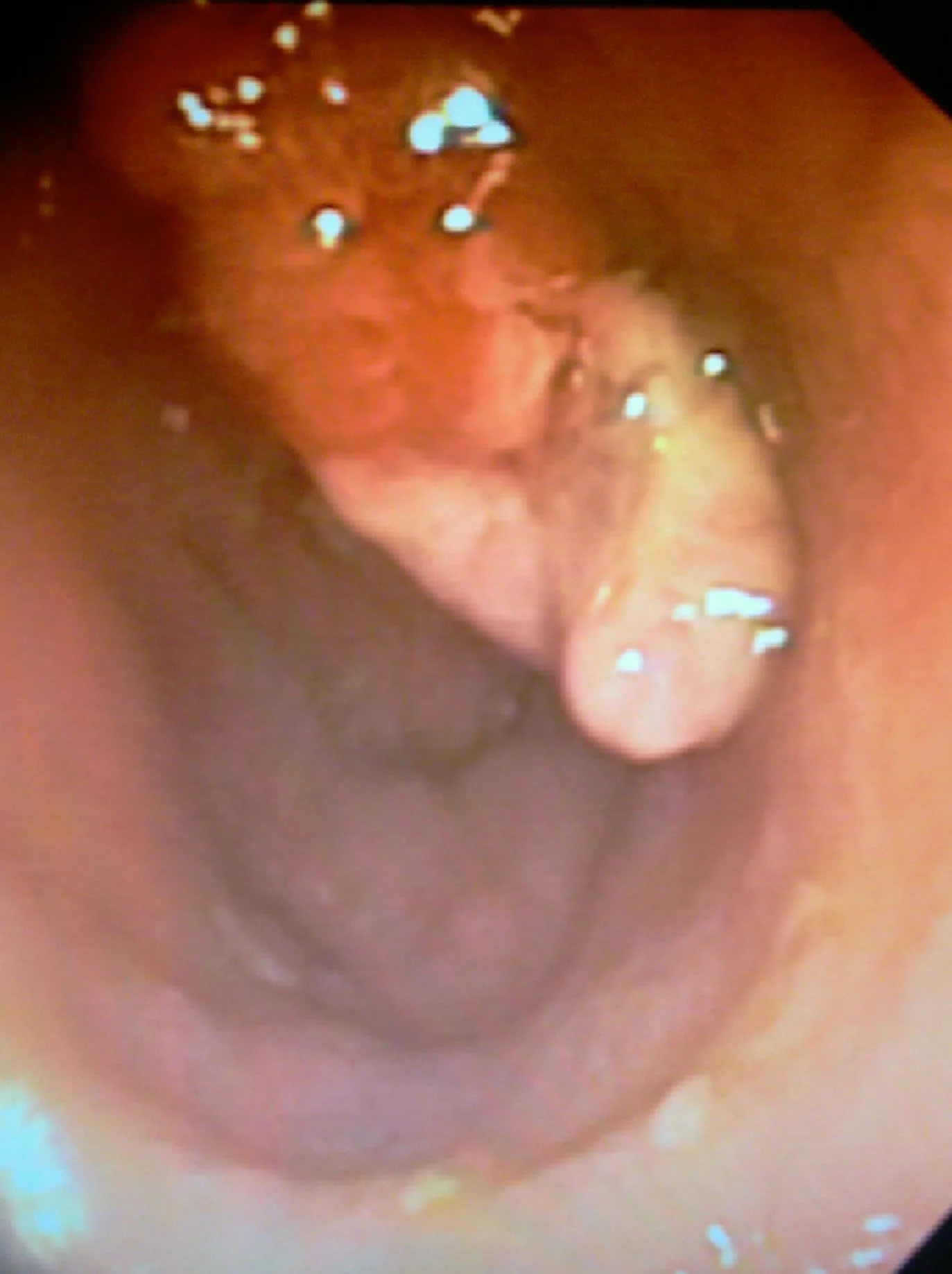
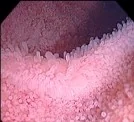
Endoscopic view of ileal pouch - anal anastomosis 3 years before the development of adenocarcinoma (Courtesy Dr. V. Penopoulos)
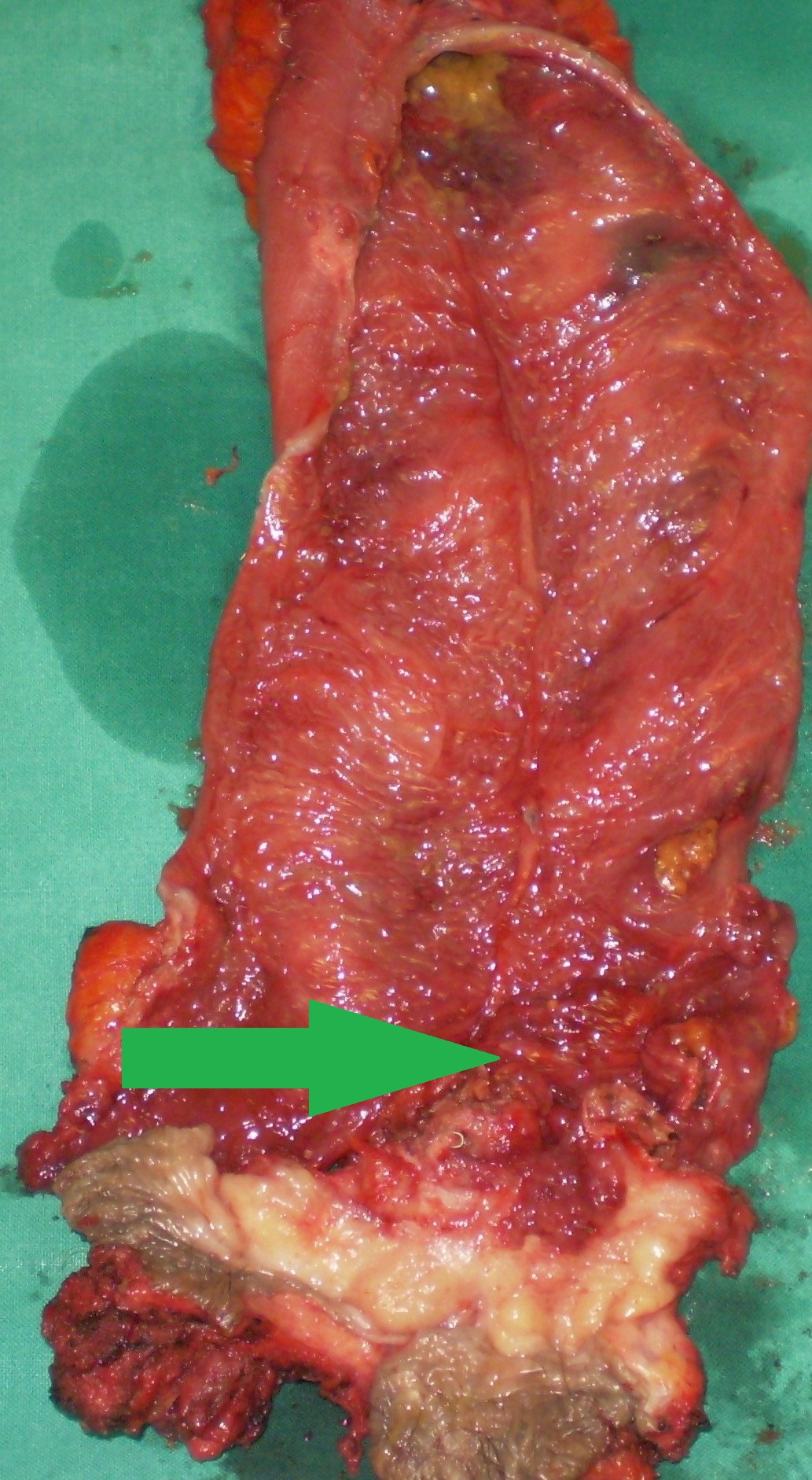
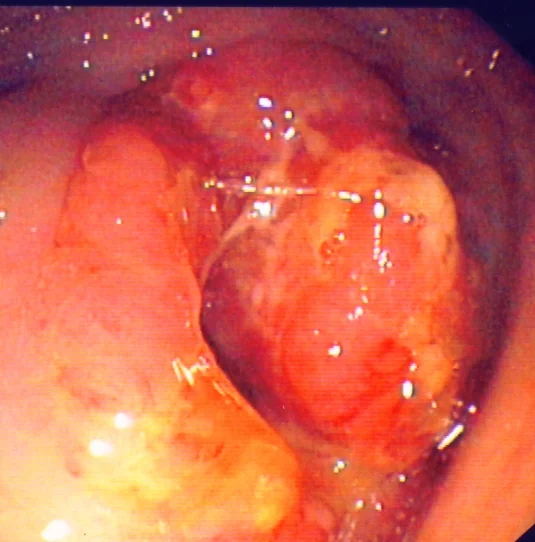
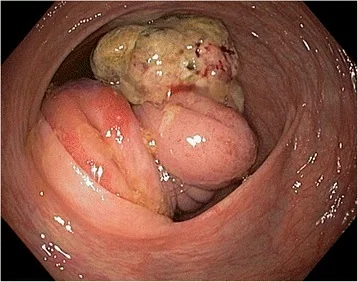
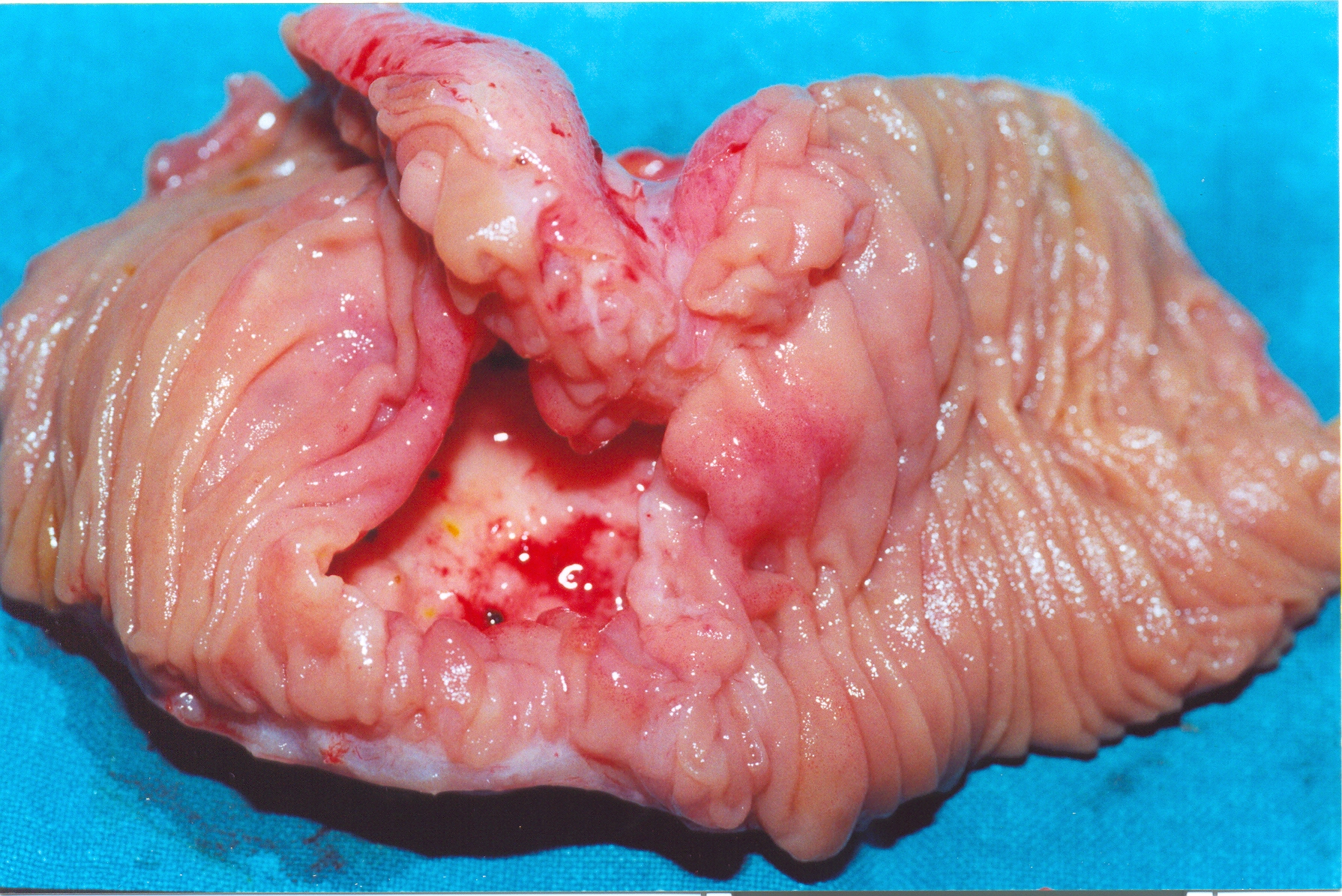
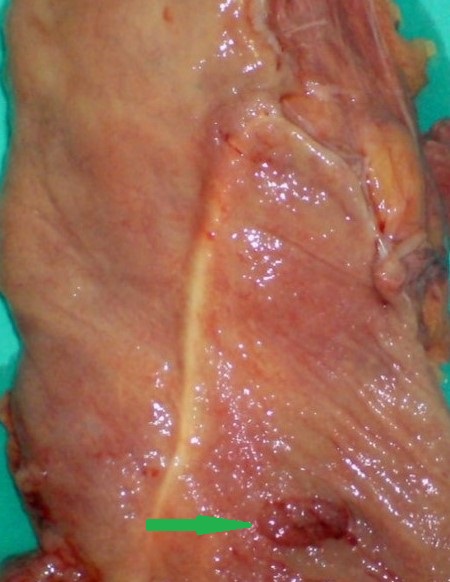
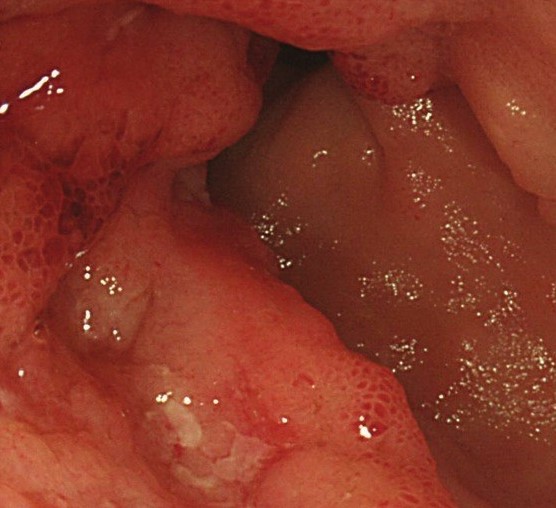
The adenocarcinoma is clearly seen nearby the ileal pouch anal anastomosis (Courtesy Dr. V. Penopoulos)

The adenocarcinoma is clearly seen nearby the ileal pouch anal anastomosis (Courtesy Dr. V. Penopoulos)
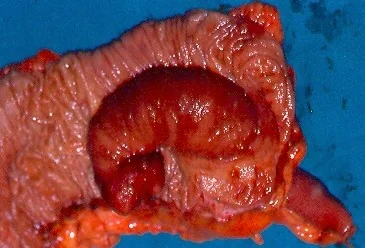
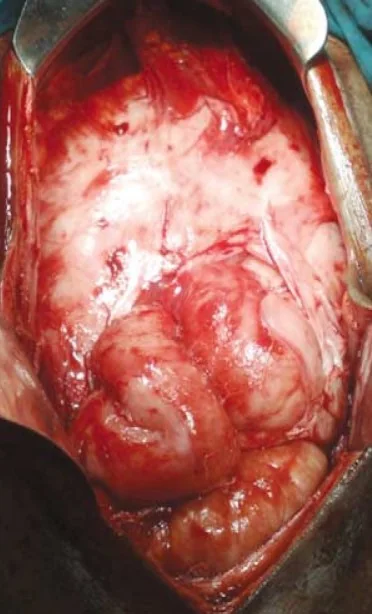
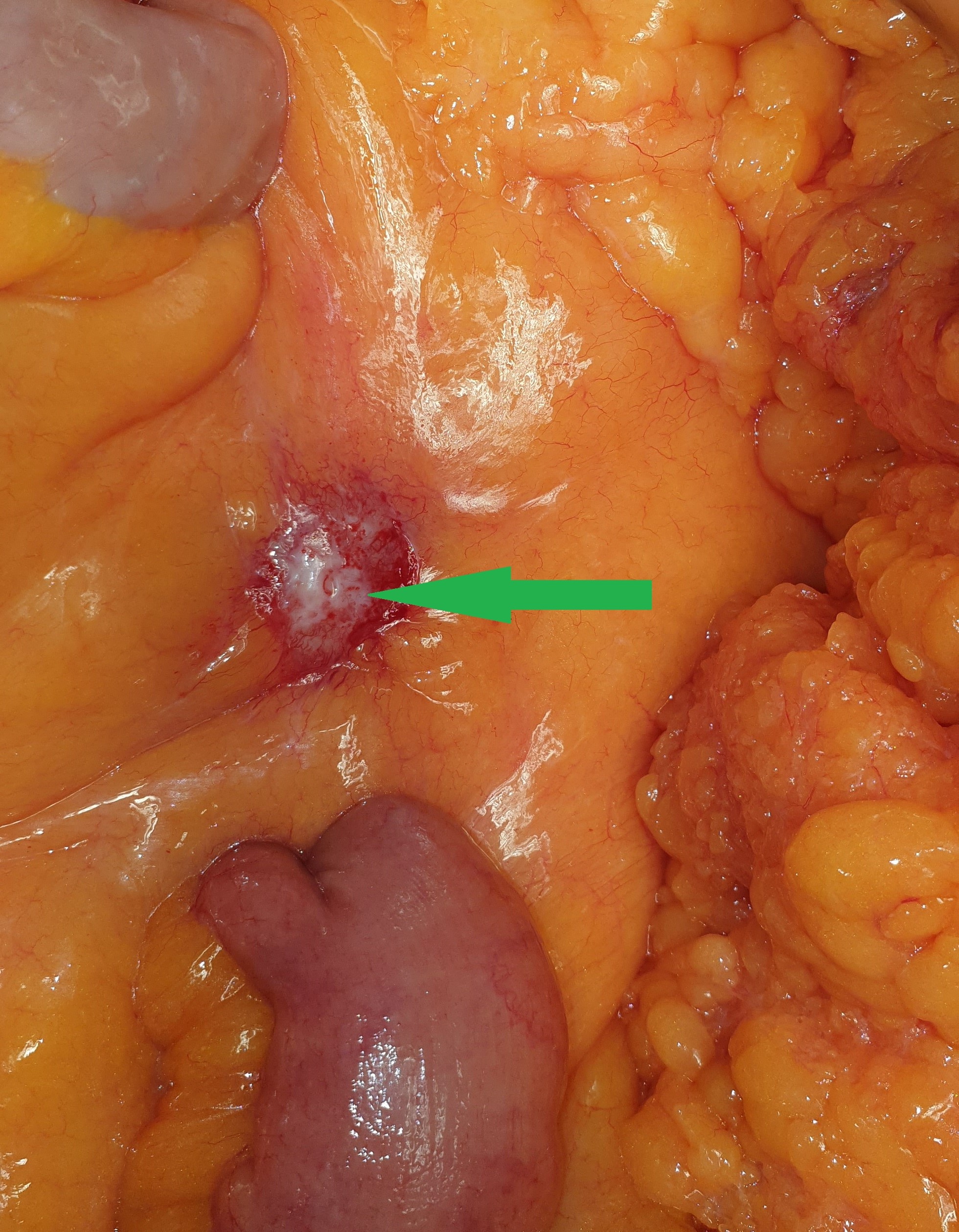
Small bowel obstruction (terminal ileum) - endometriosis . (Courtesy Dr . V . Penopoulos).
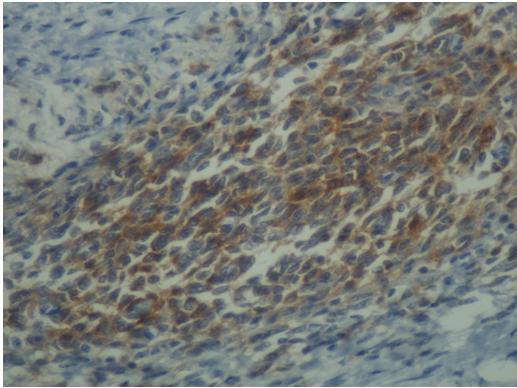

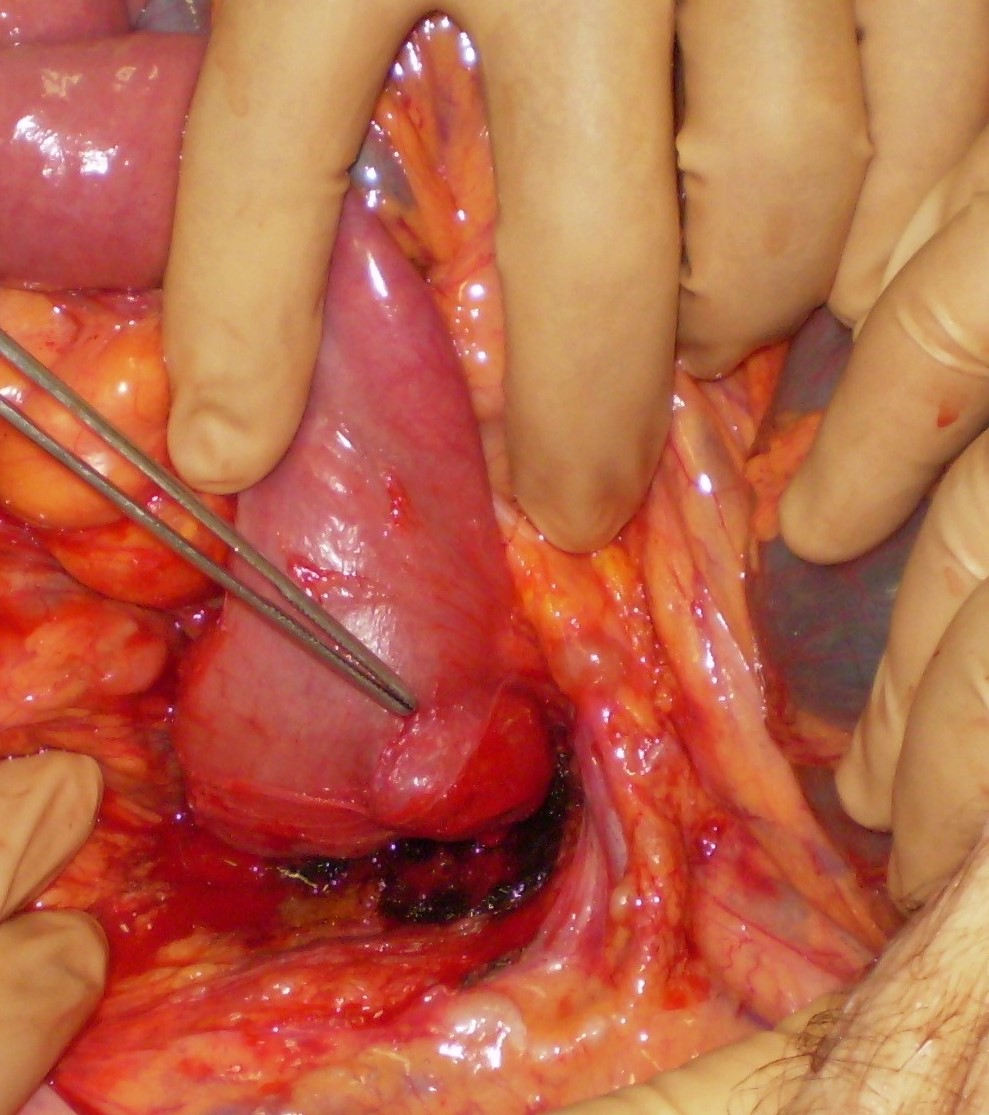
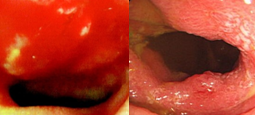


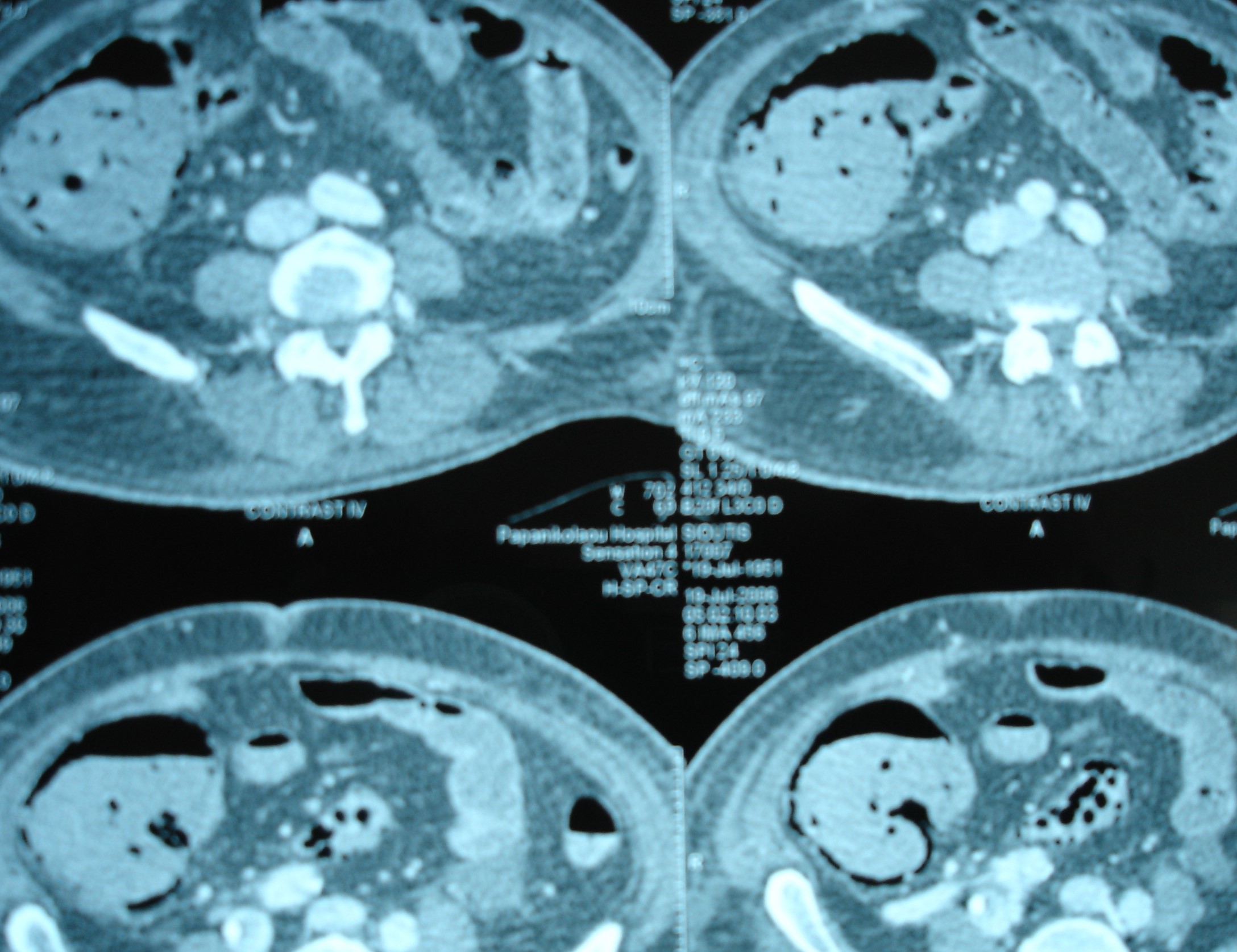
Figure 2 . Abdominal CT Scan indicative of intestinal ischemia . ( Courtesy Dr . V . Penopoulos ) .

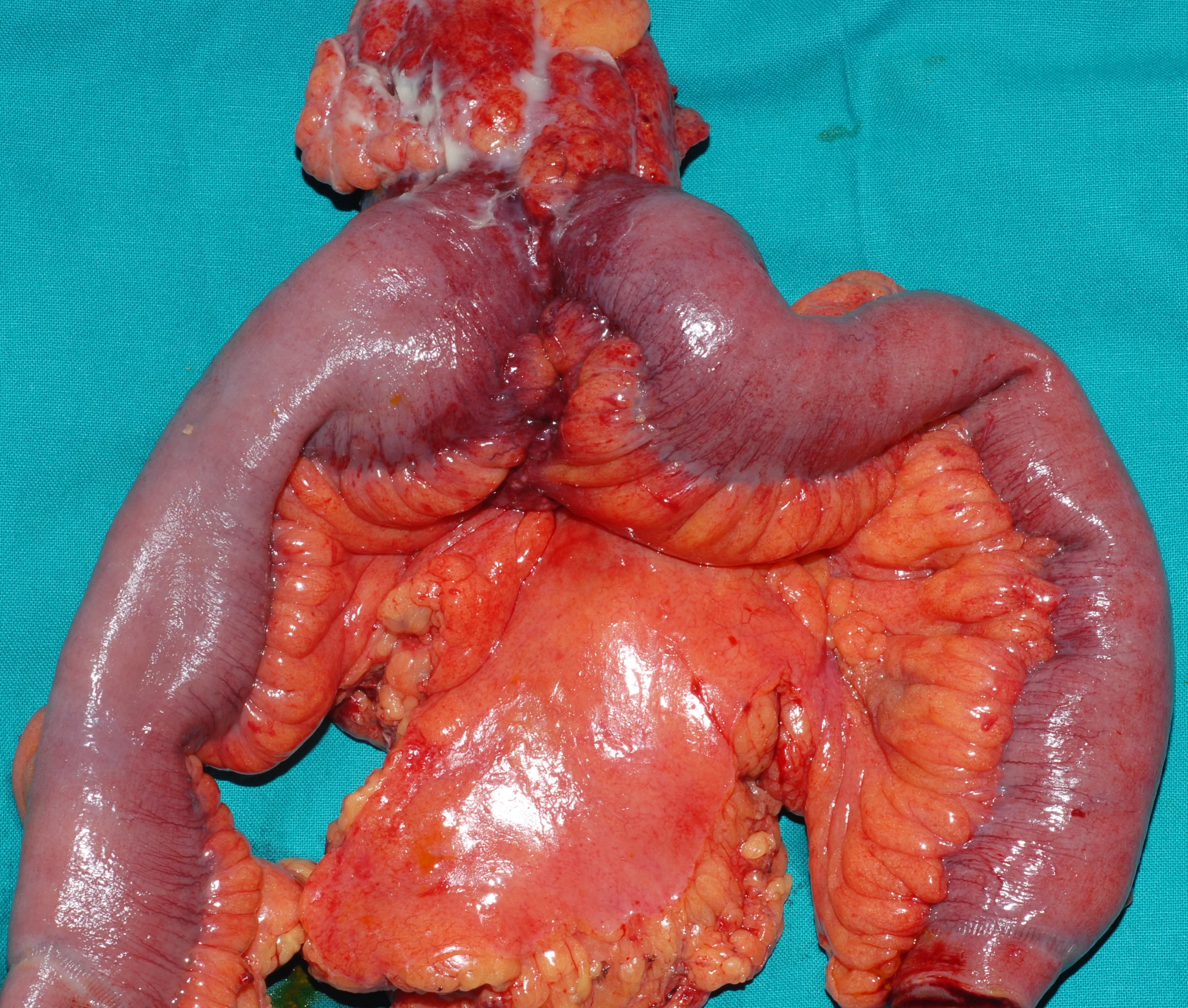
Green shading: Complete occupation of the abdomen by the peritoneal "cocoon" (Courtesy Dr. V. Penopoulos)
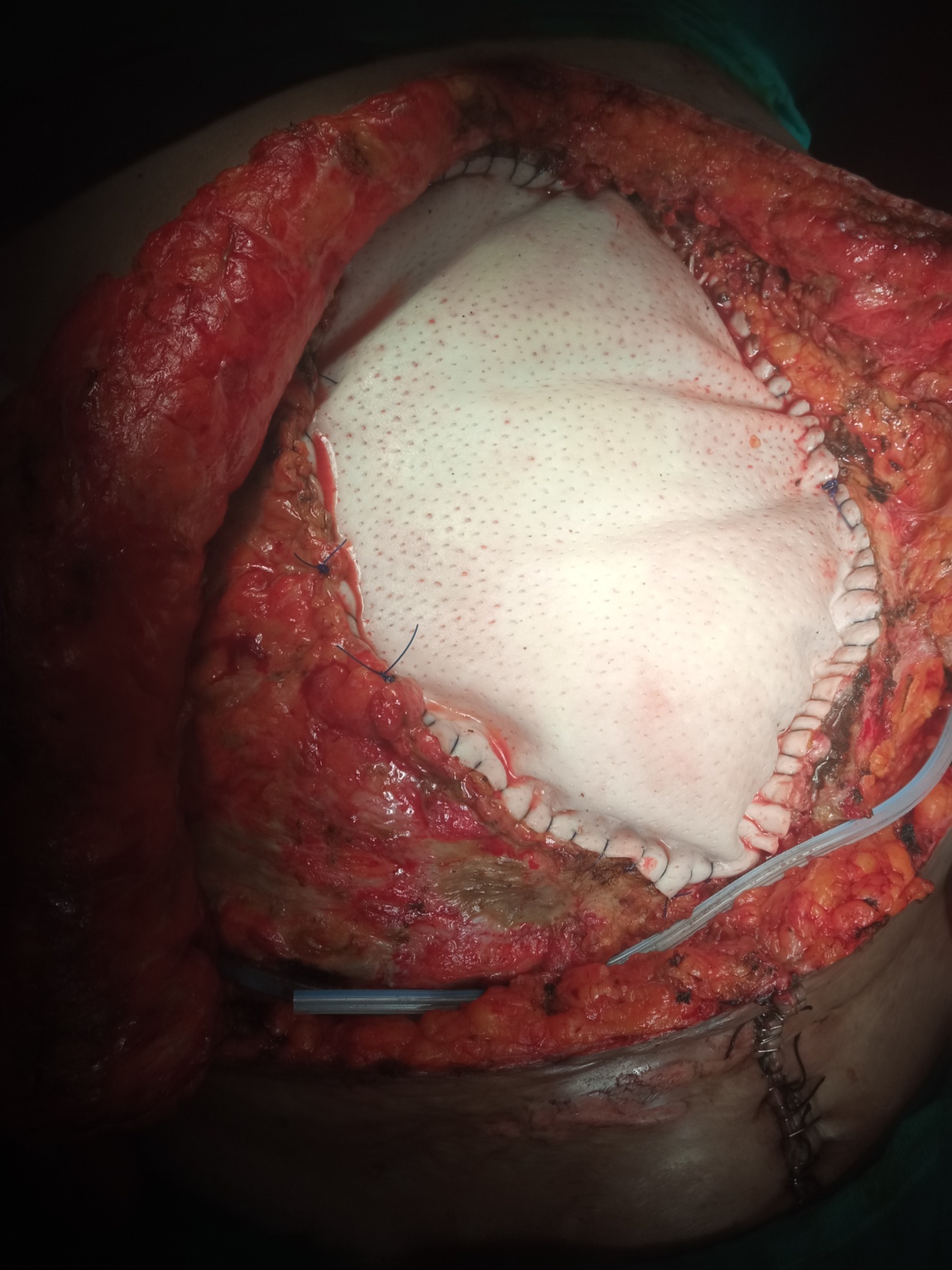
Coverage of the abdominal wall defect with Permacol mesh.(Courtesy Dr. V. Penopoulos).


Purple arrows: Sites of small bowel perforation. Encapsulation of the entire peritoneal cavity (Courtesy Dr. V. Penopoulos)
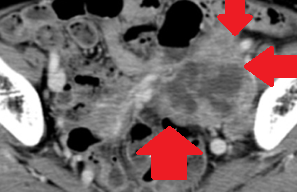
Abdominal CT scan.Red arrows-Mass in the left pelvic wall.(Courtesy Dr. V. Penopoulos).
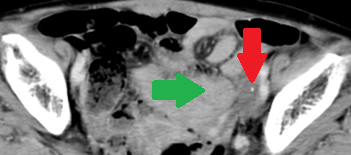
Abdominal CT scan after a 2-year interval. Red arrow – small residual neoplasm. Green arrow – small bowel loops (Courtesy Dr. V. Penopoulos)


Perforation of the terminal ileum - CMV infection . (Courtesy Dr . V . Penopoulos).


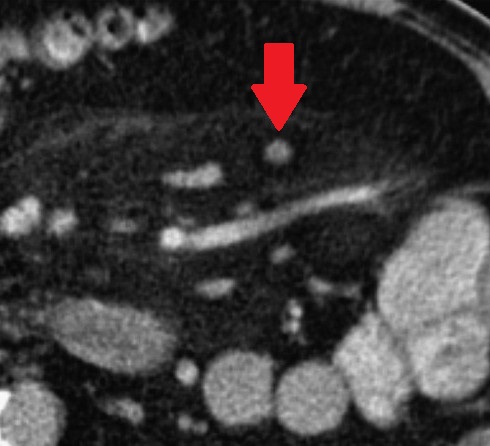
Abdominal CT Scan. Red arrow - Bezoar within the small bowel.(Courtesy Dr. V. Penopoulos).

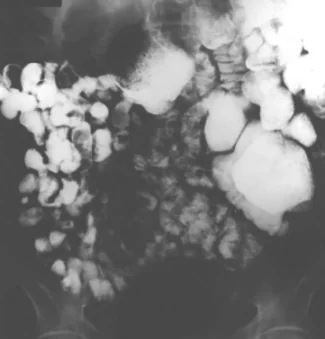
Chest X-Rays .Pneumatosis intestinalis - Pseudo-pneumoperitoneum.Courtesy Dr.V.Penopoulos).
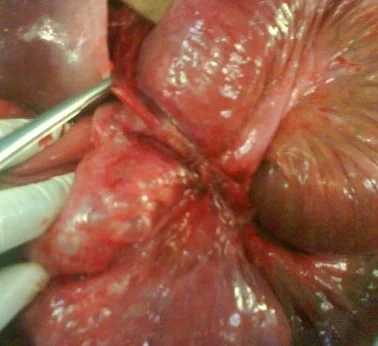
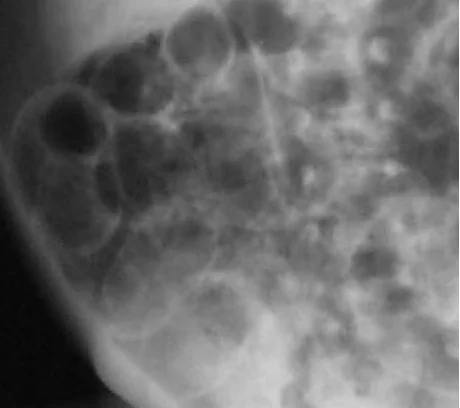
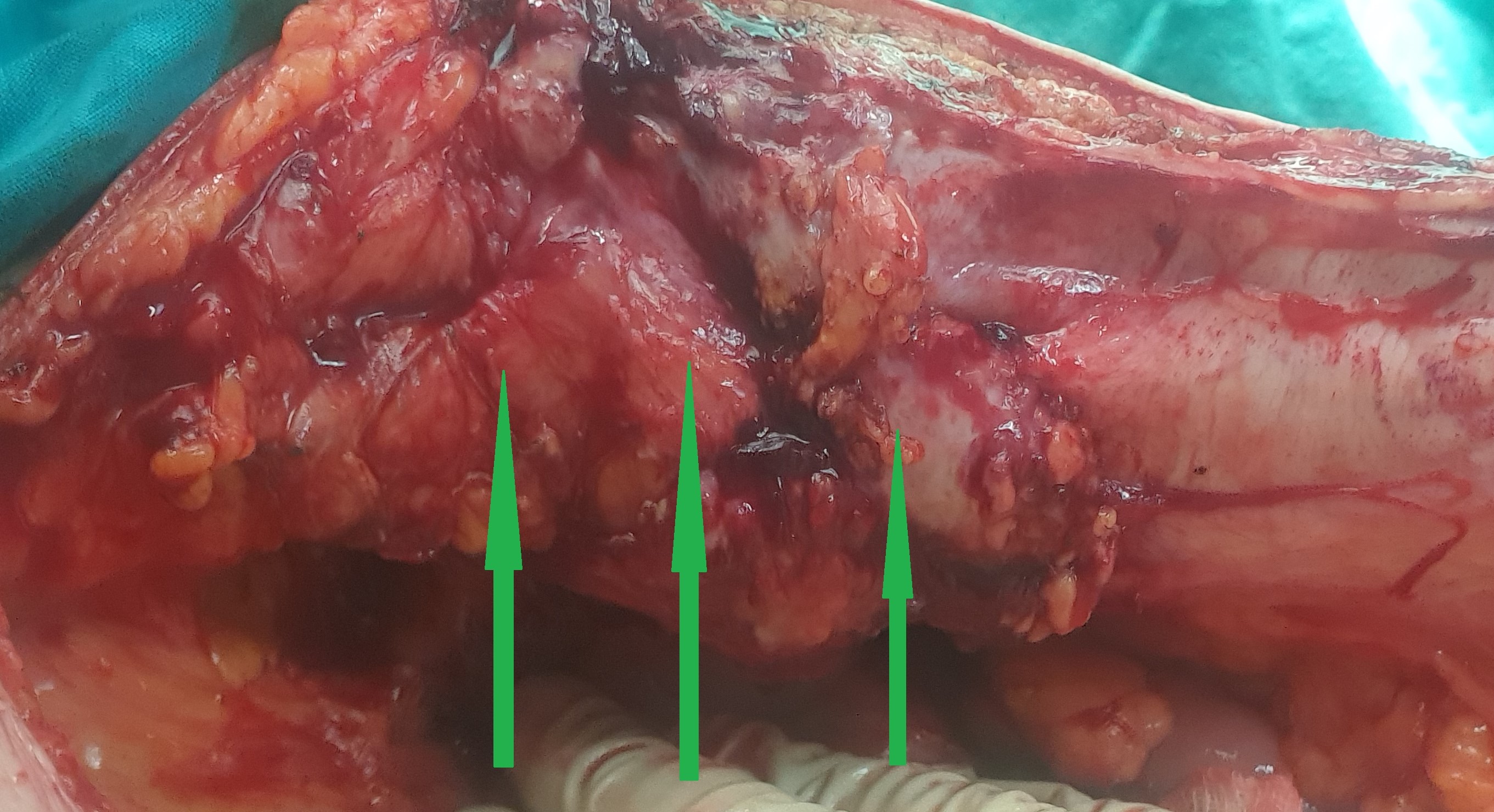
Operative view of pneumatosis intestinalis. Blue arrow - Pneumatosis. Green arrows - Diverticula

Light blue arrow-Distended proximal intestinal loops.Purple arrow-Collapsed intestinal loops.Yellow arrow-Transition point.(Courtesy Dr. V. Penopoulos).(Courtesy Dr. V. Penopoulos)


Gaseous overdistention of the small bowel and air in the gastric wall (red arrow).(Courtesy Dr.V.Penopoulos).

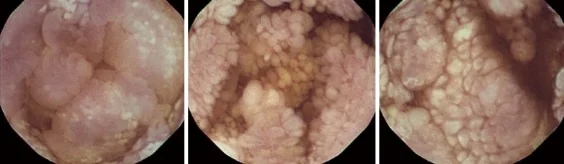
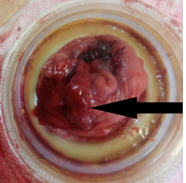
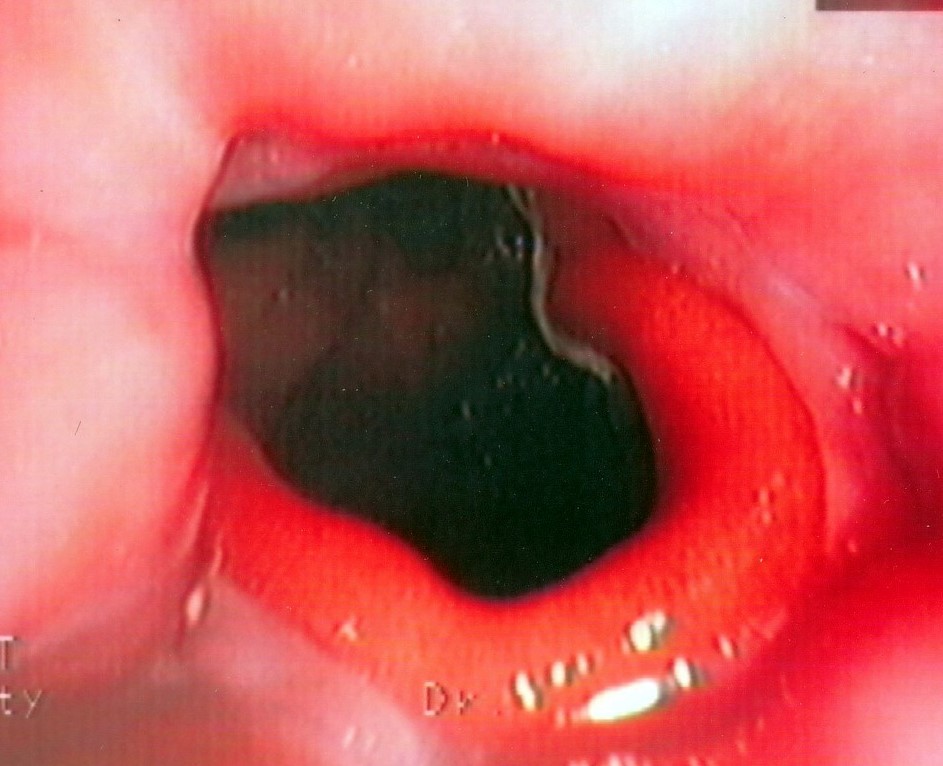
Endoscopic view . A bulky, rounded congestive mass is seen in the stomach . ( Courtesy Dr . V . Penopoulos ) .

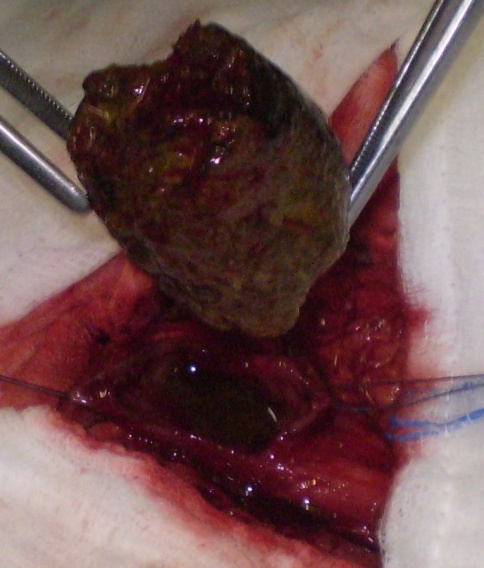
Gross surgical specimen shows the necrotic changed intussusception (red arrow).(Courtesy Dr.V.Penopoulos).
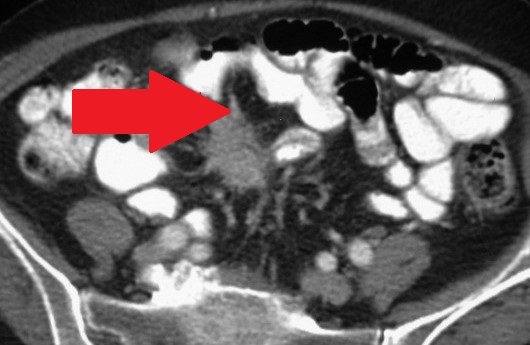


Figure 2 . Abdominal CT scan shows markedly dilated stomach with mass-like, thick-walled bowel loops (red arrow). ( Courtesy Dr . V . Penopoulos ) .
