Upper Abdomen
Άνω Κοιλία
623 images · 3 sub-chapters

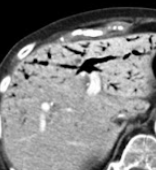
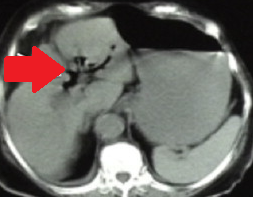
Plain abdominal X-Rays.Air in the portal venous system.(Courtesy Dr. V. Penopoulos).
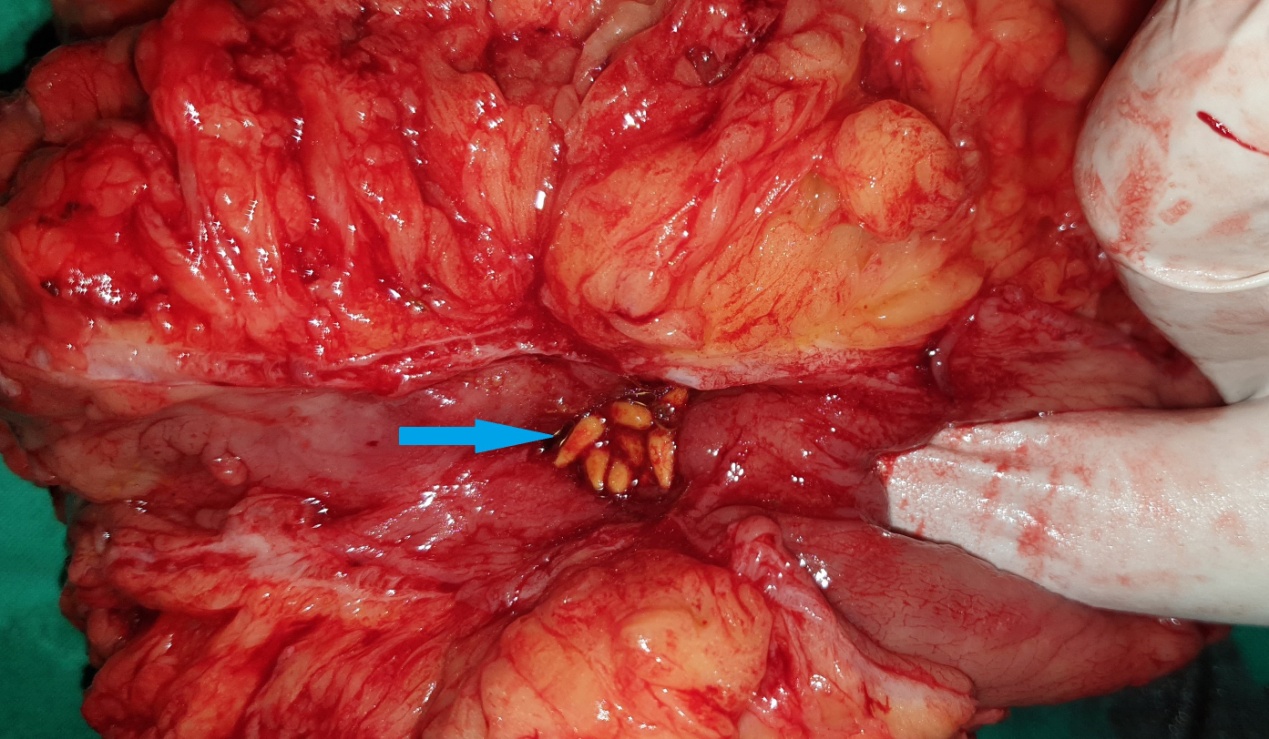
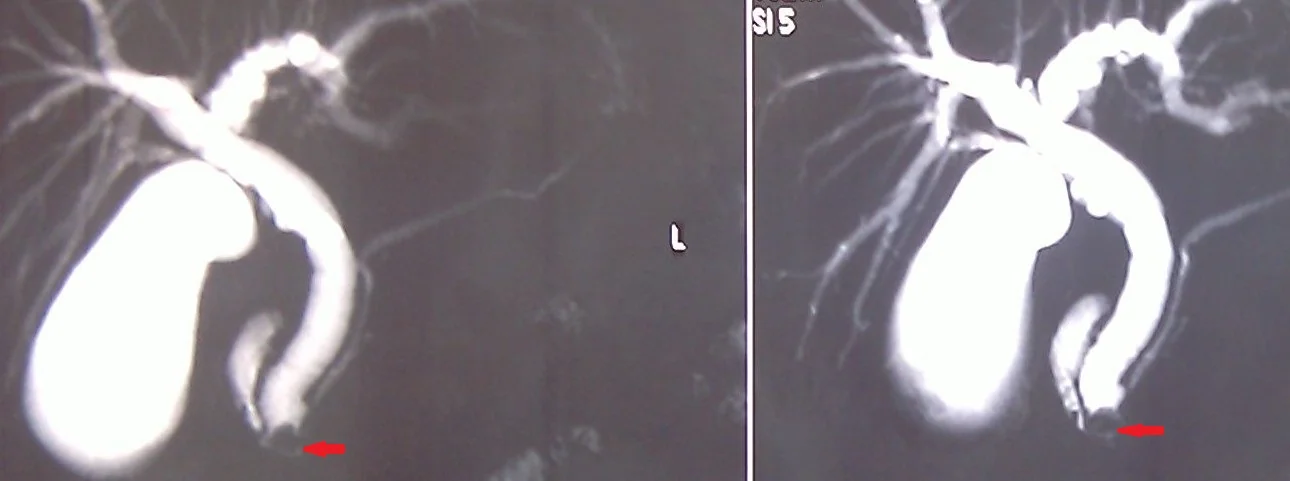
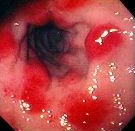
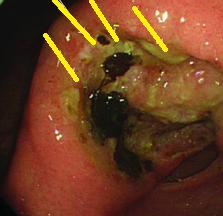
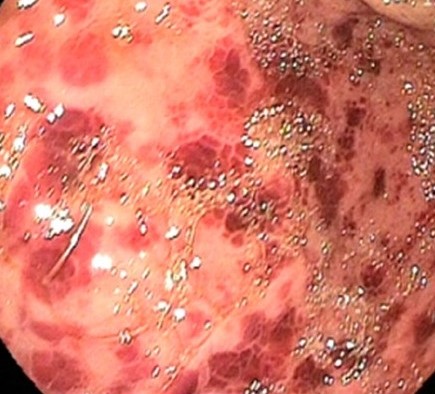
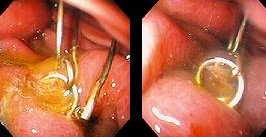
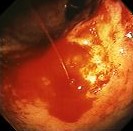
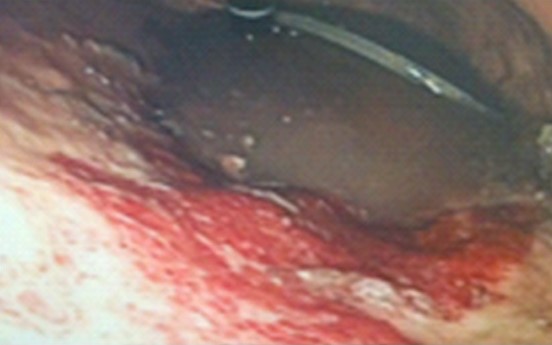
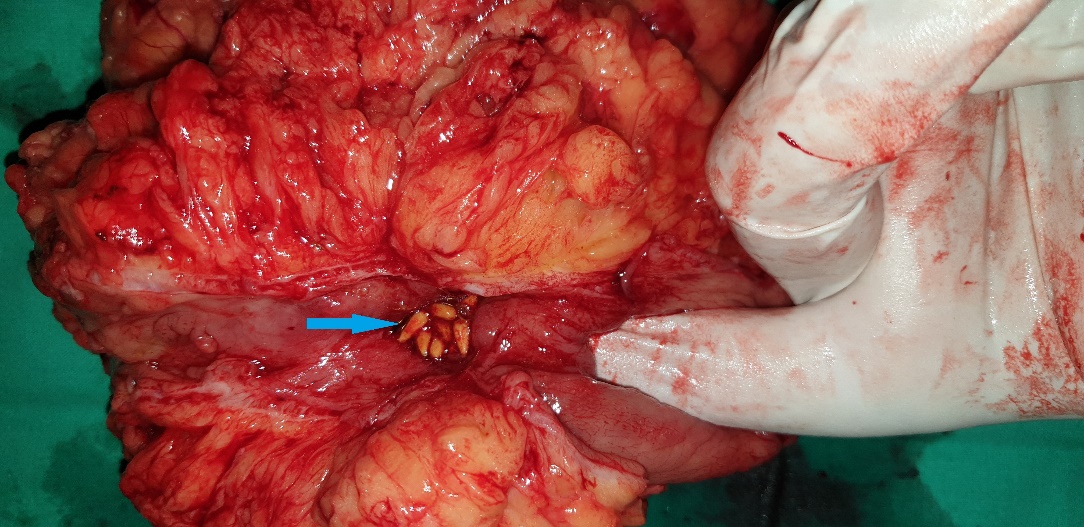
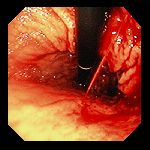
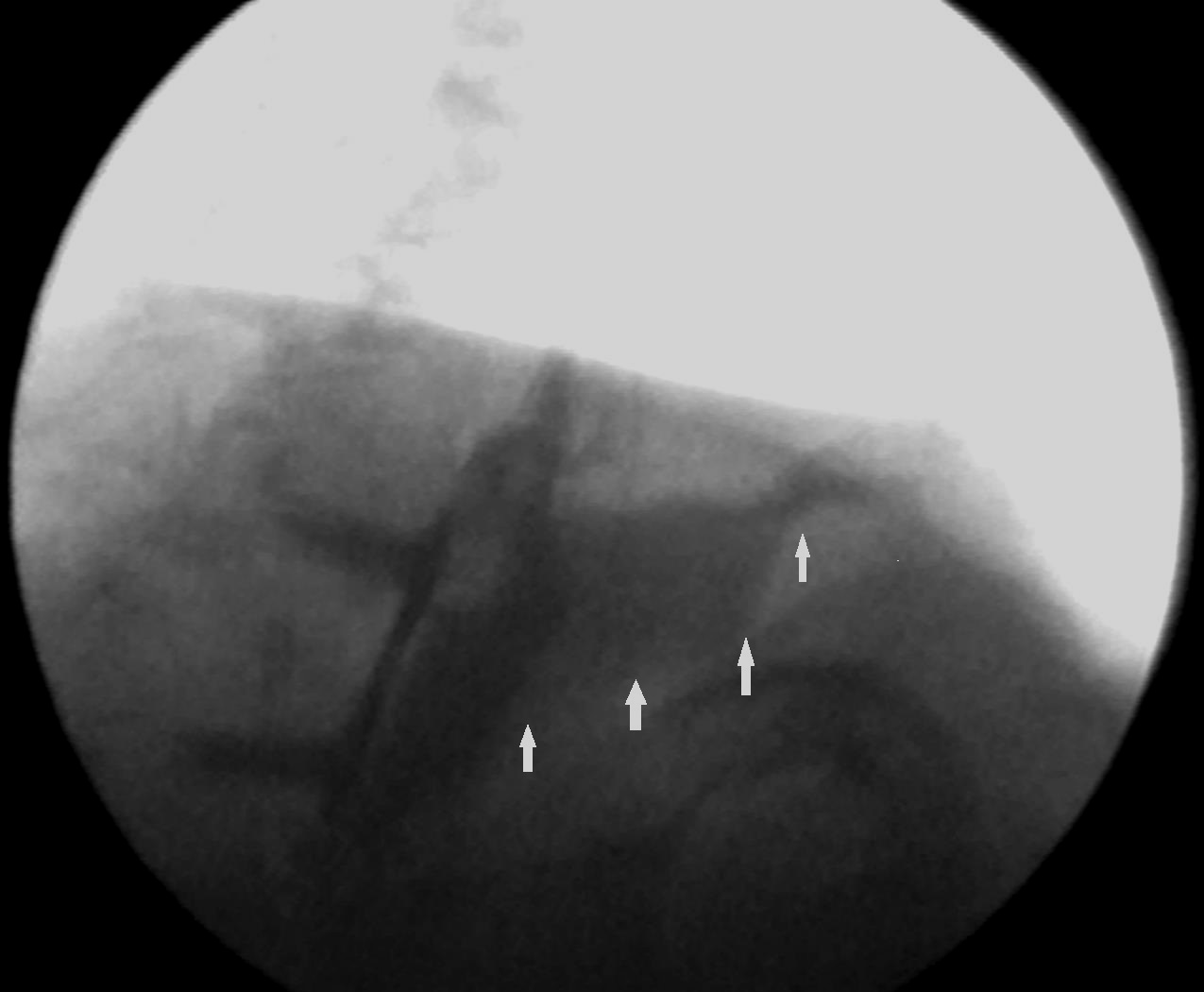
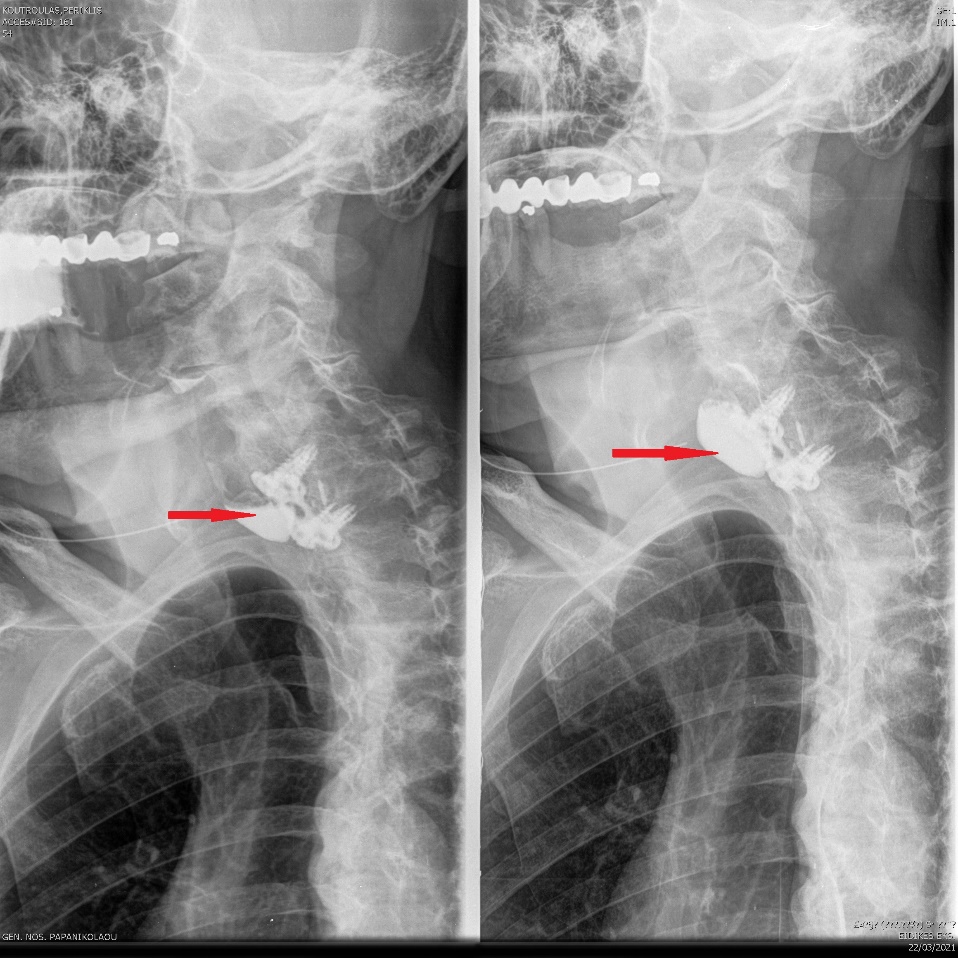
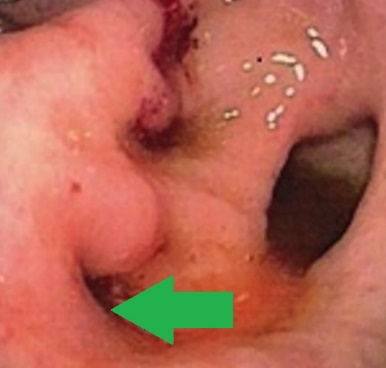
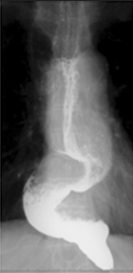
Highlighting of the fistula ,digitally.Visible seeds stuck at the fistula orifice.(Courtesy Dr.V.Penopoulos).
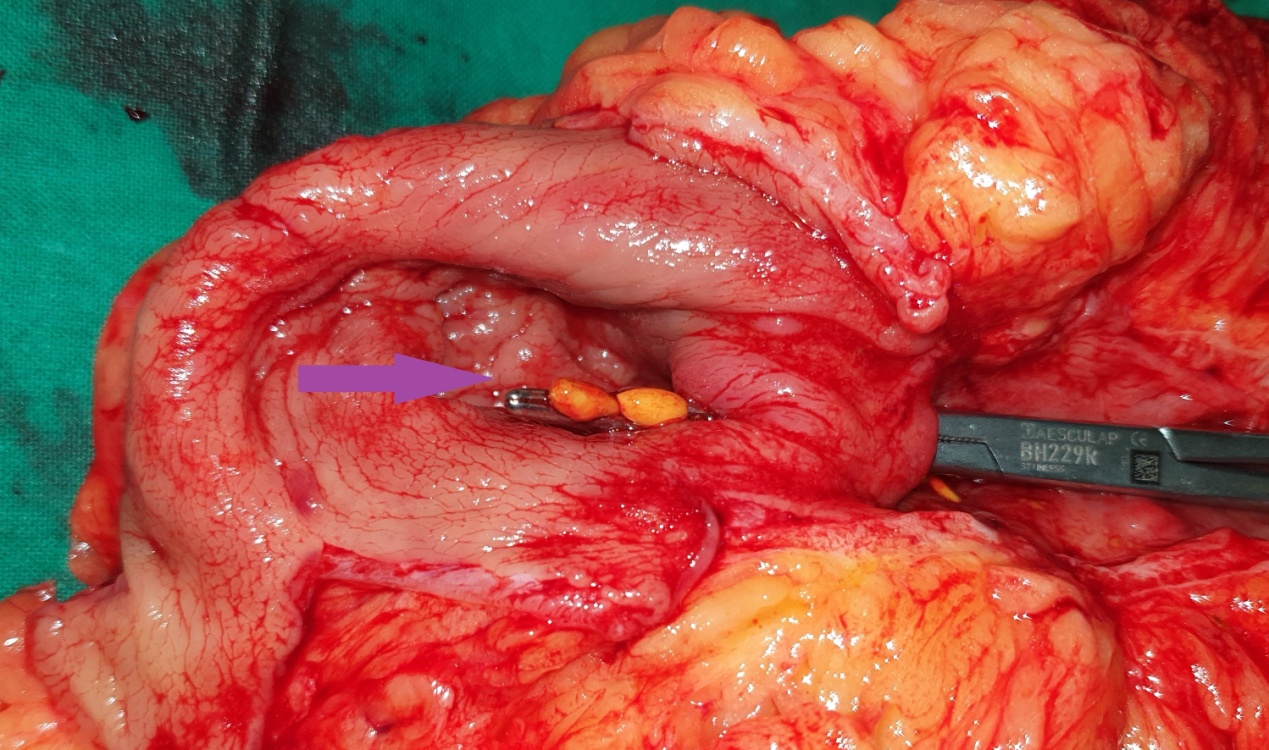
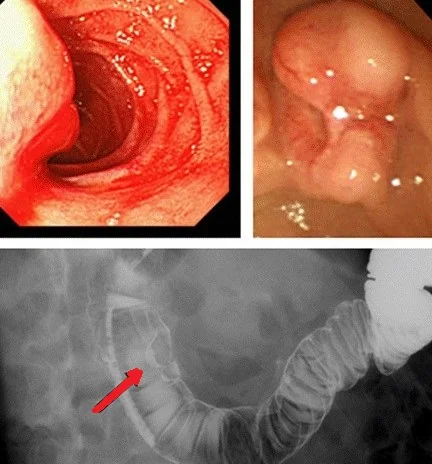
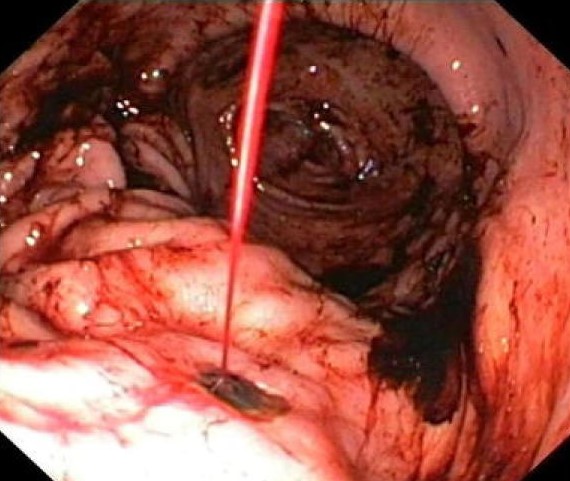
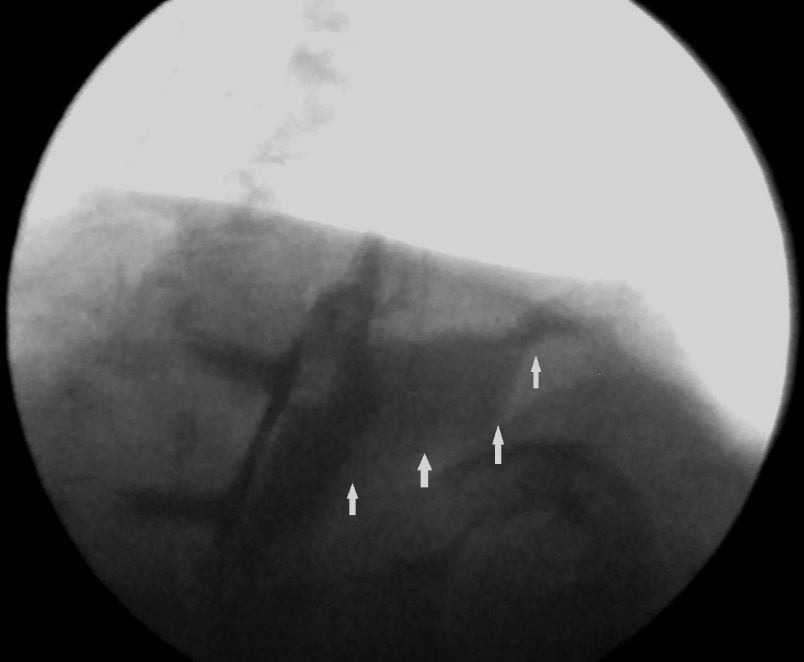
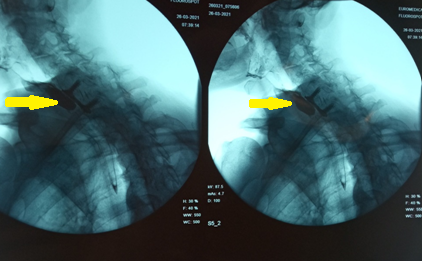
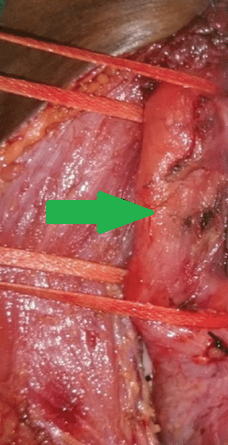
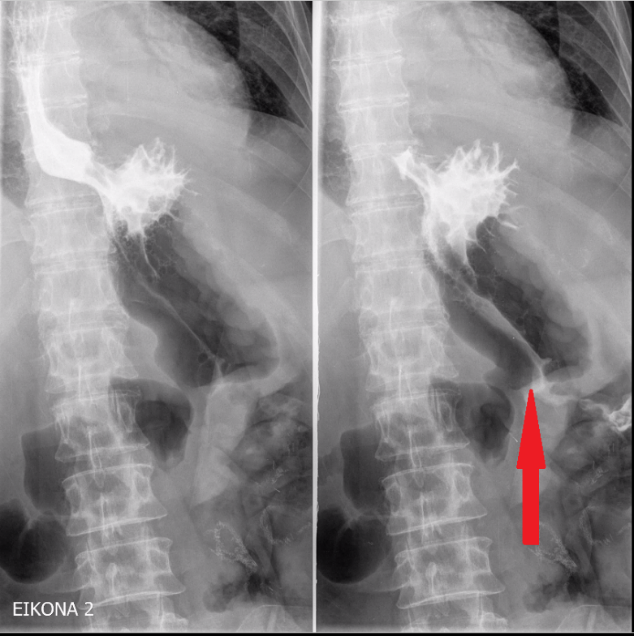
Highlighting of the fistula,both digitally and instrumentally.Visible seeds stuck at the fistula orifice.(Courtesy Dr.V.Penopoulos).
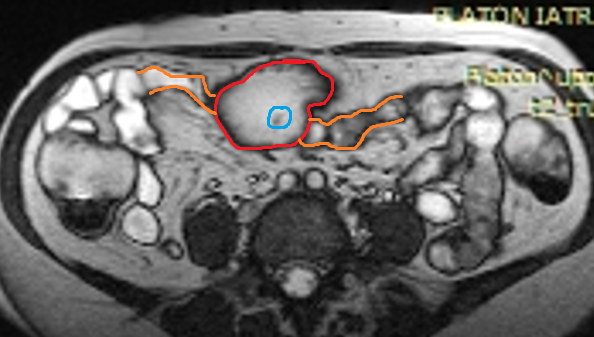
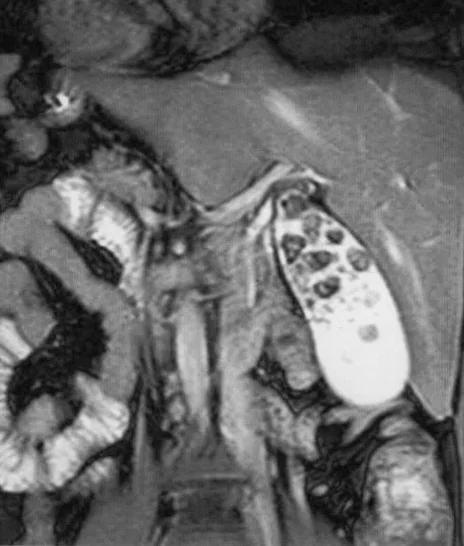
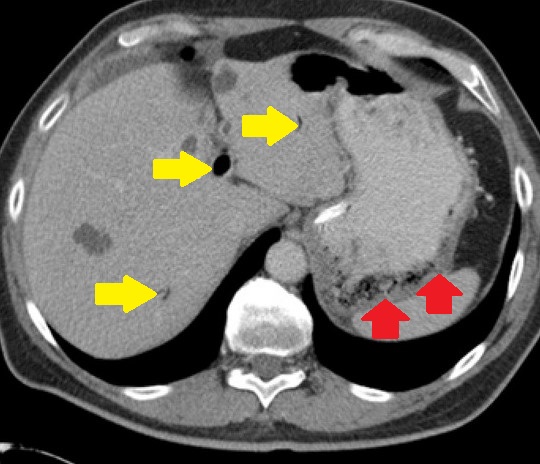
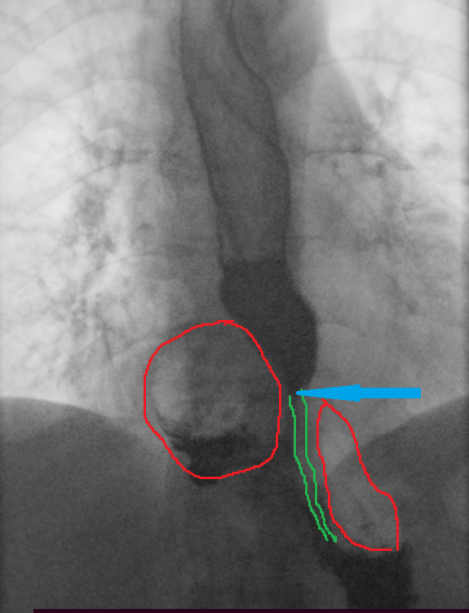
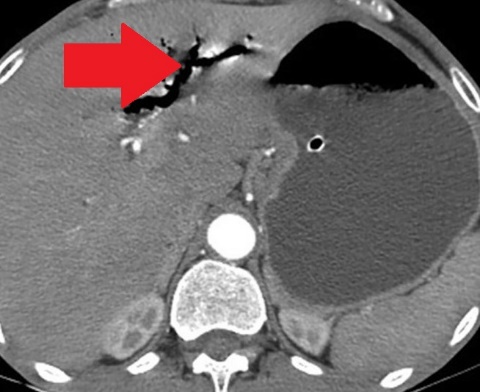
Abdominal MRI.Red outline-stomach.Orange outline-transverse colon.Light blue outline-Fistula orifice.(Courtesy Dr.V.Penopoulos).
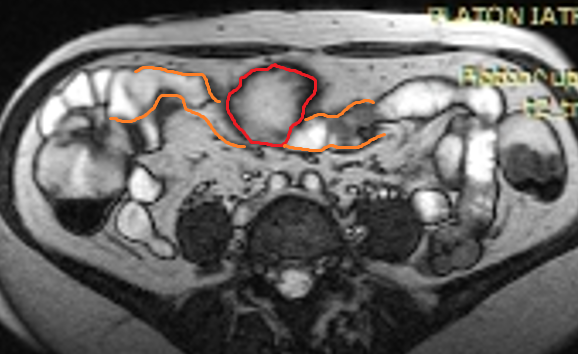
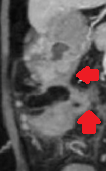
Abdominal MRI.Red outline-stomach.Orange outline-transverse colon .(Courtesy Dr.V.Penopoulos).
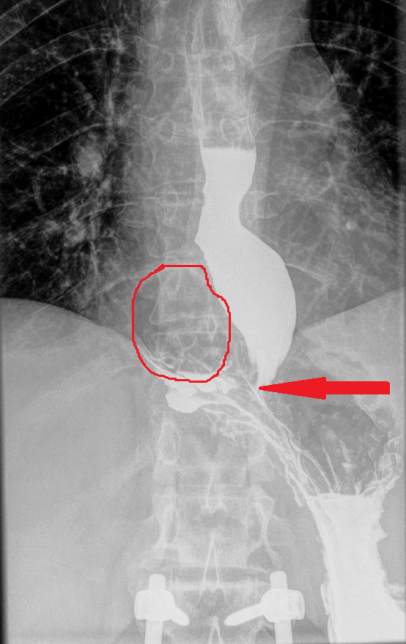
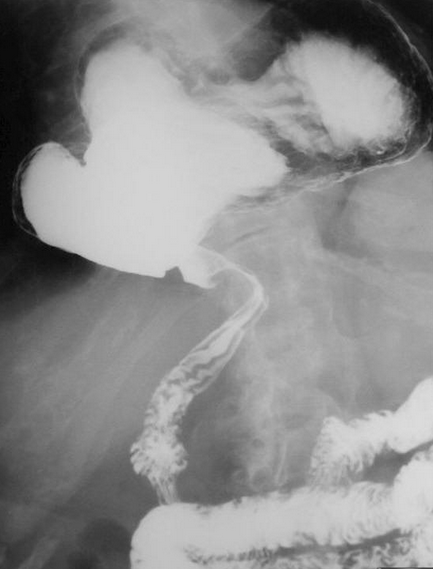
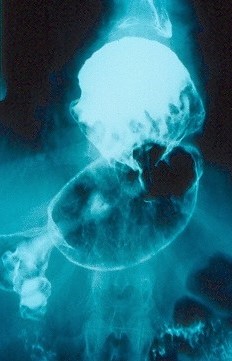
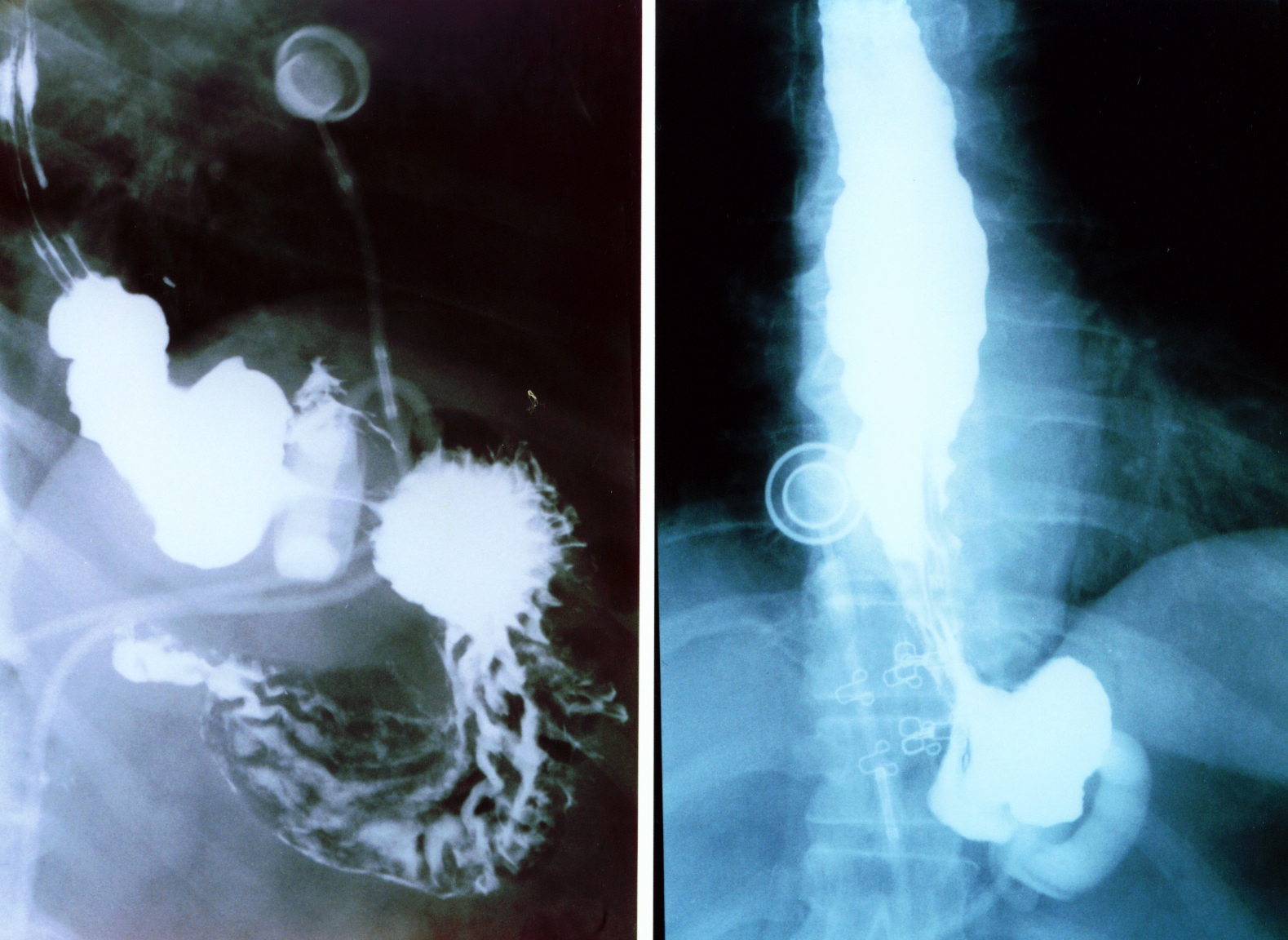
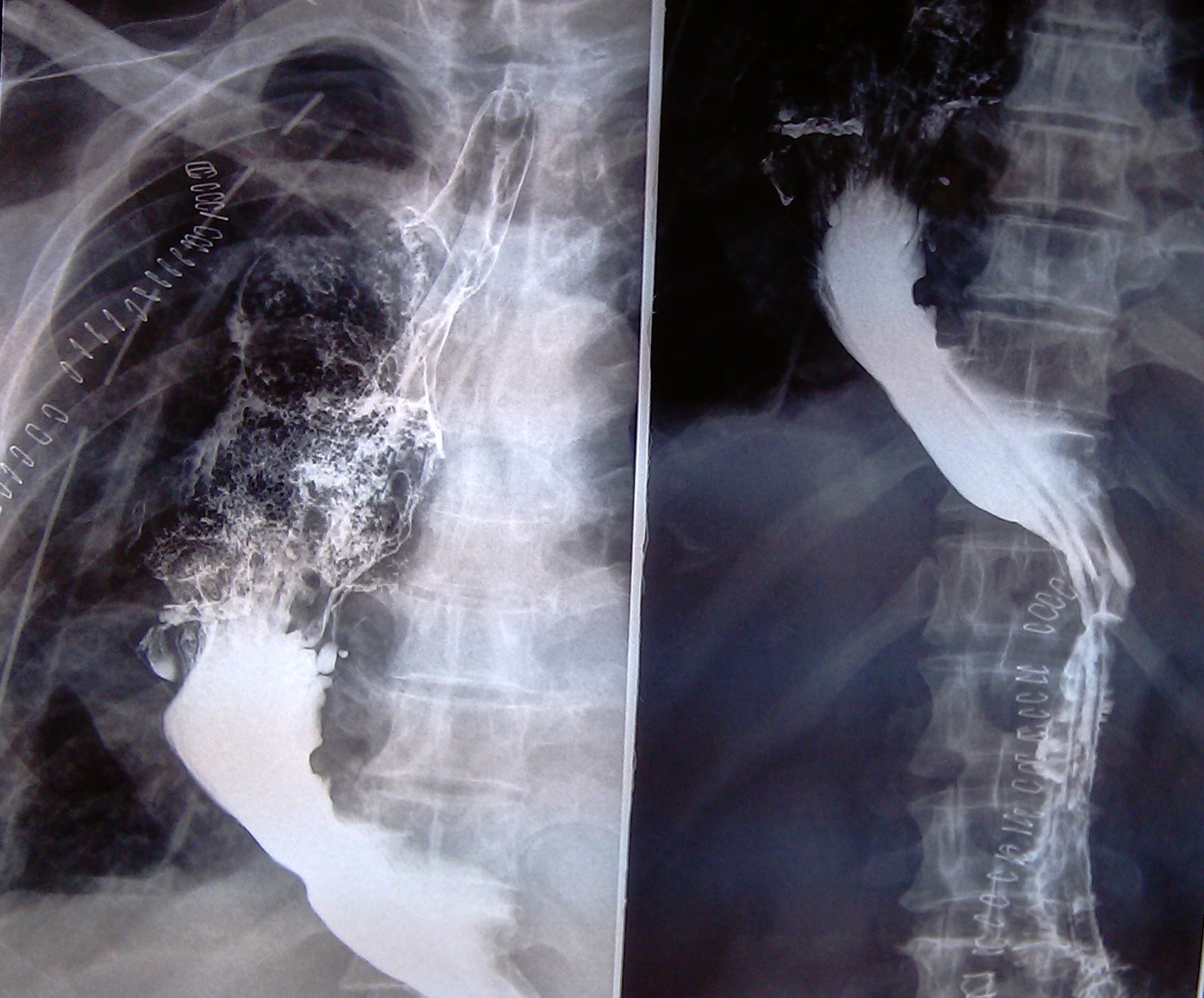
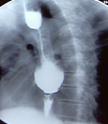
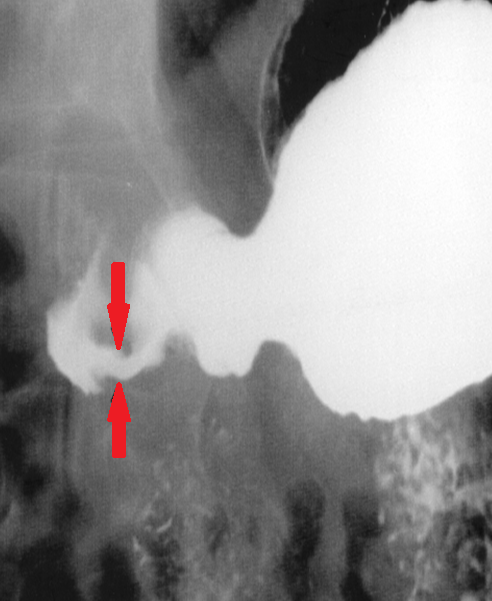
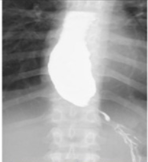
Barium swallow esophagography.Esophageal achalasia.(Courtesy Dr.V.Penopoulos).
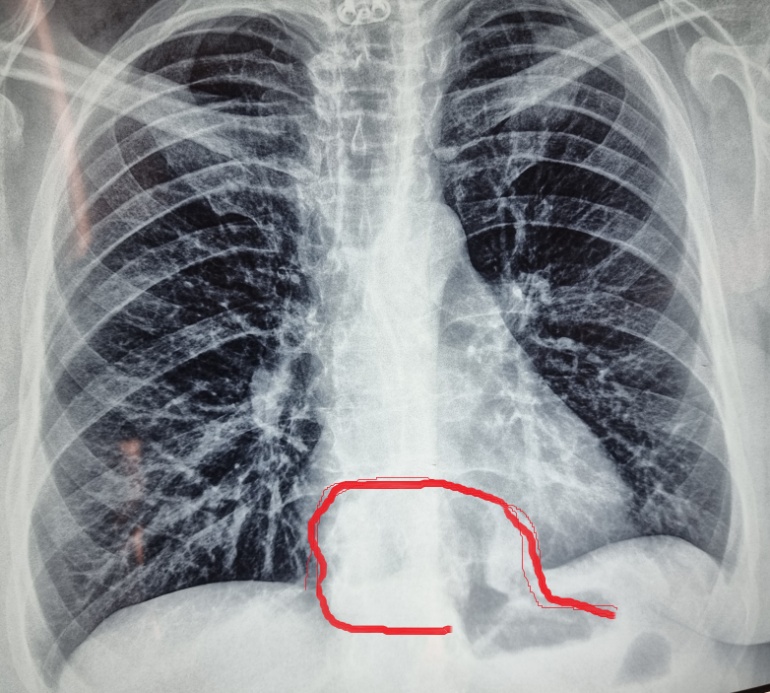
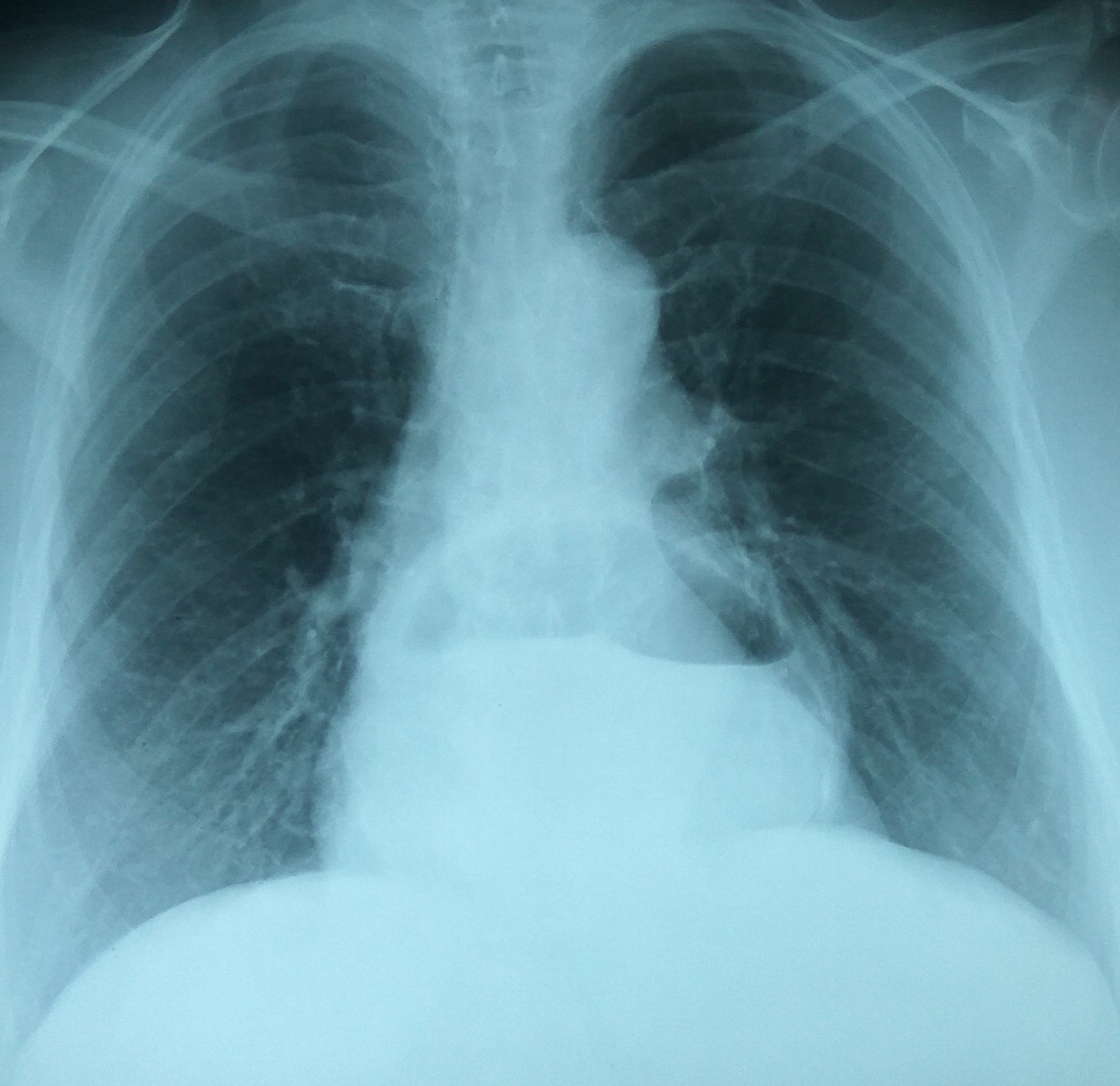
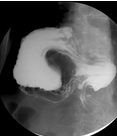
Chest X-Ray. Red outlines delineate the hiatal hernia.(Courtesy Dr.V.Penopoulos).

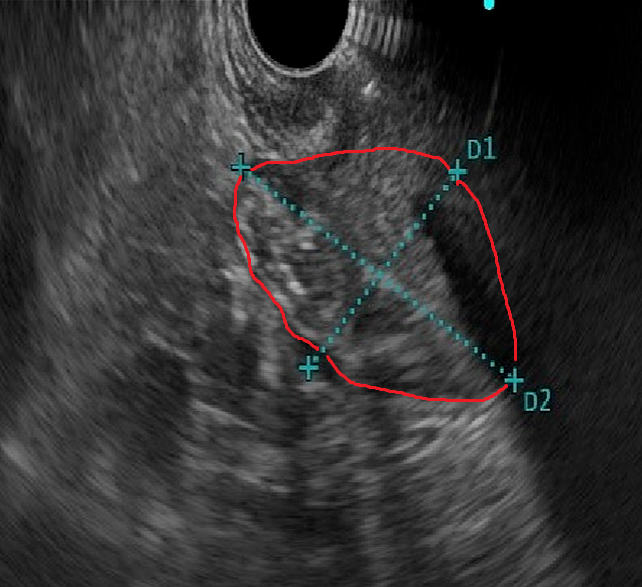
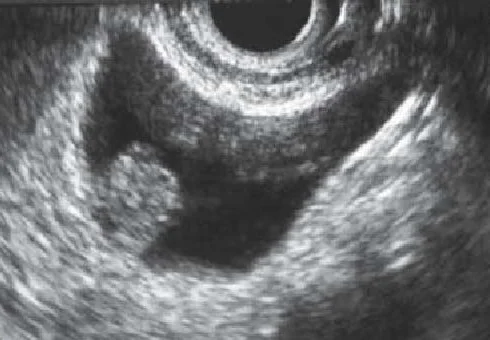
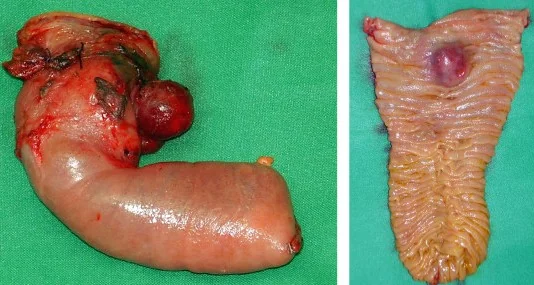
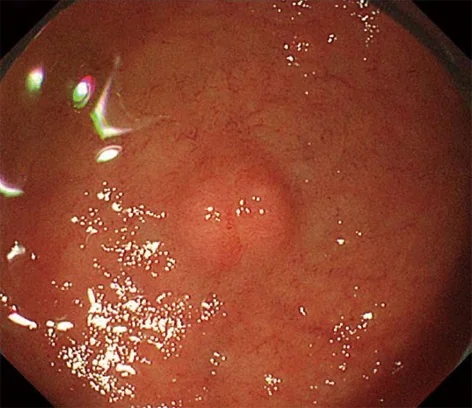
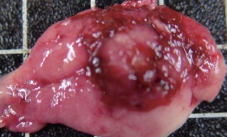
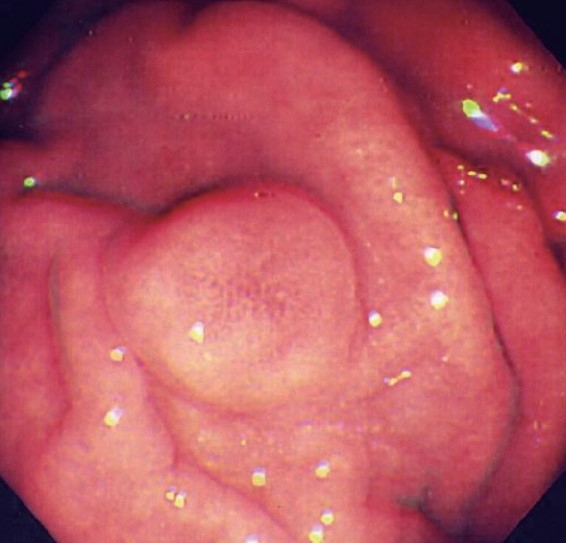
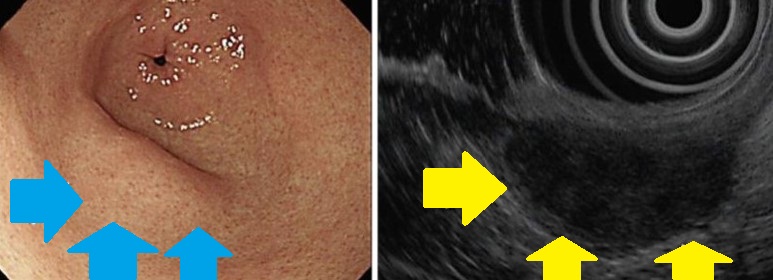
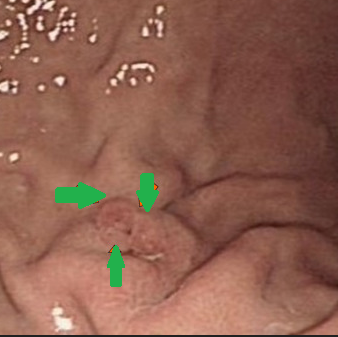
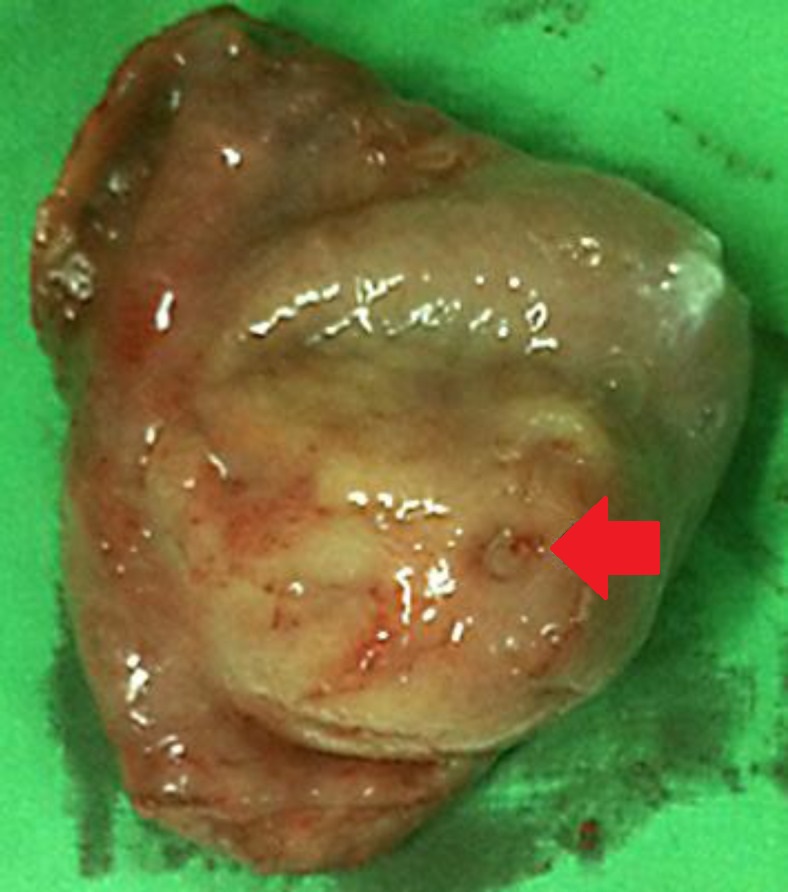
Endoscopic U/S. Duodenal Inflammatory Fibrous Polyp.(Courtesy Dr.V.Penopoulos).
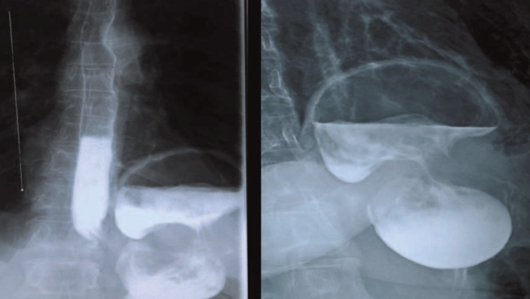
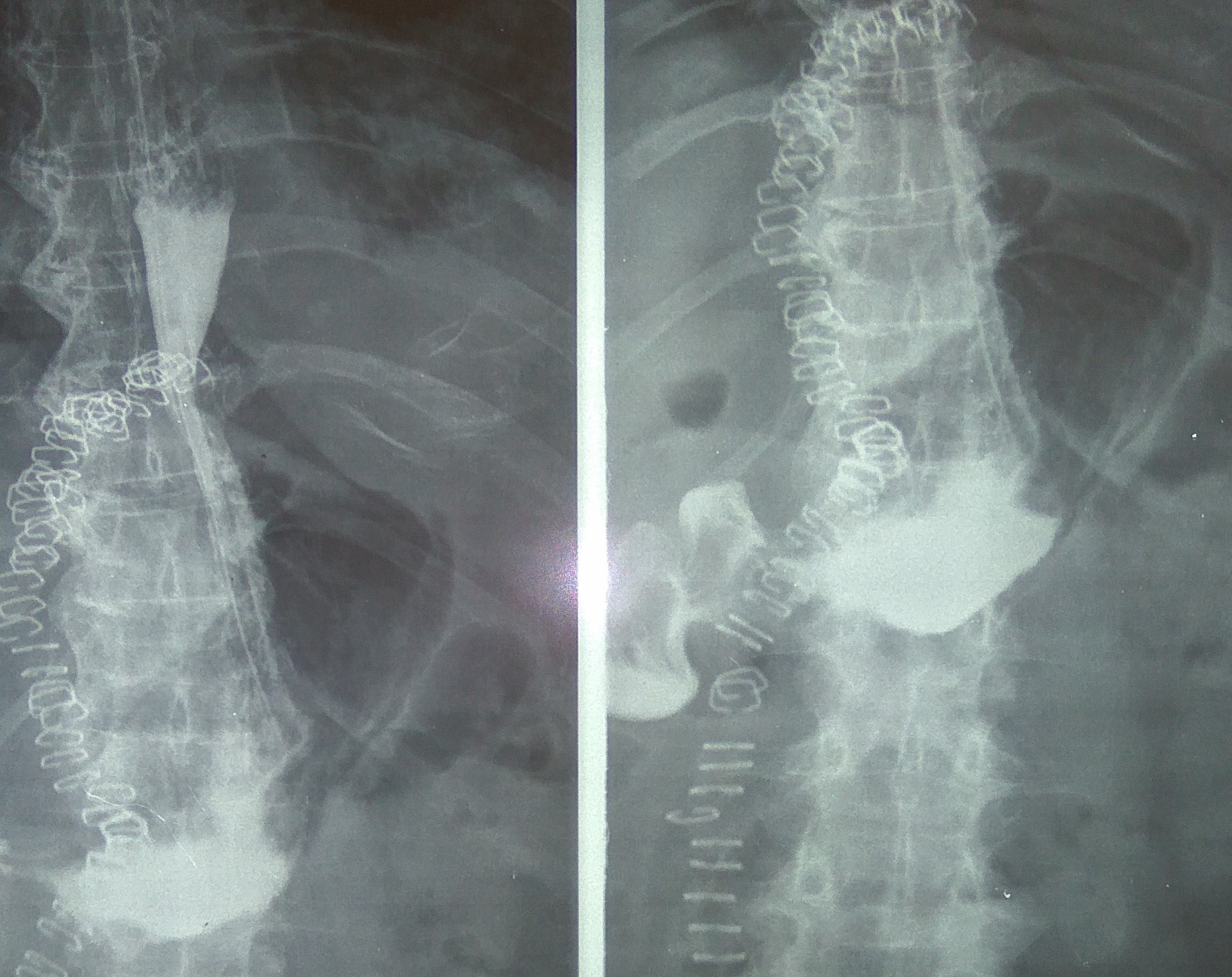
Gastrografin swallow studies.Red outlines delineate the hiatal hernia.(Courtesy Dr.V.Penopoulos).
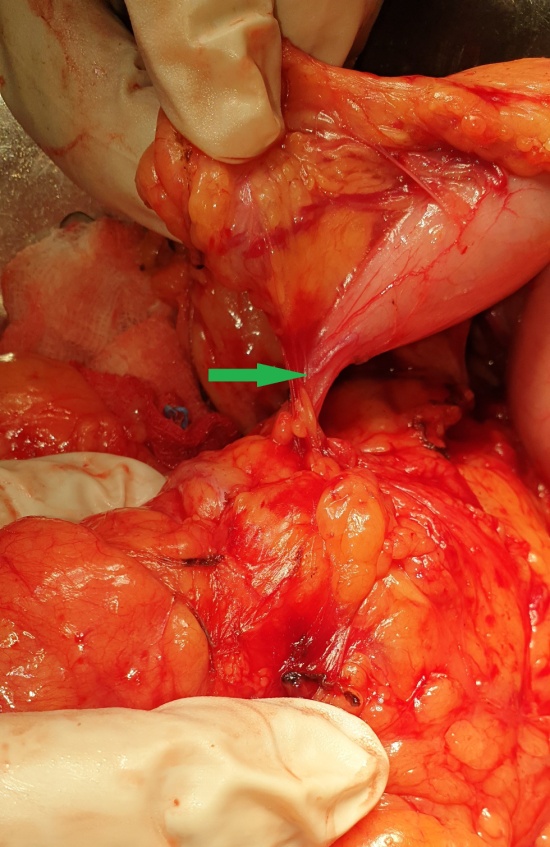
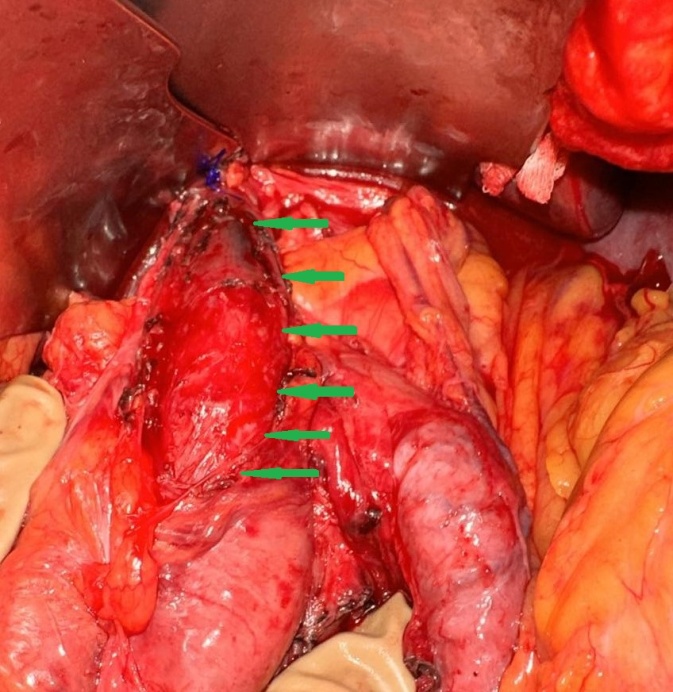
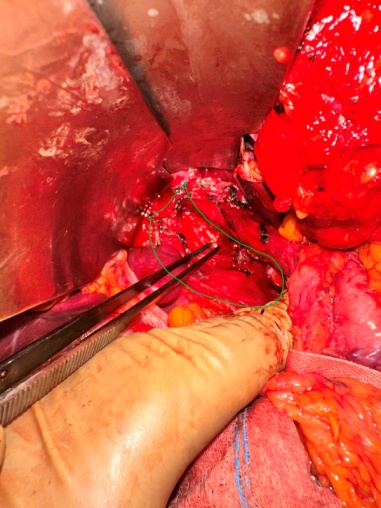
Separation of the esophagus from the hiatal hernia.(Courtesy Dr.V.Penopoulos).
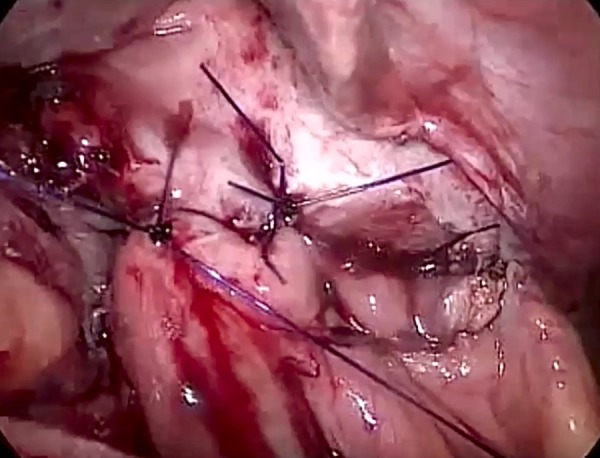
Hiatal hernia repair+cruroplasty without use of a mesh.(Courtesy Dr.V.Penopoulos).
Barium swallow esophagography.Esophageal achalasia.(Courtesy Dr.V.Penopoulos).
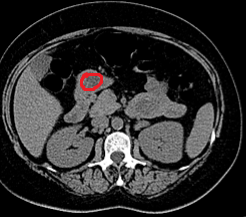
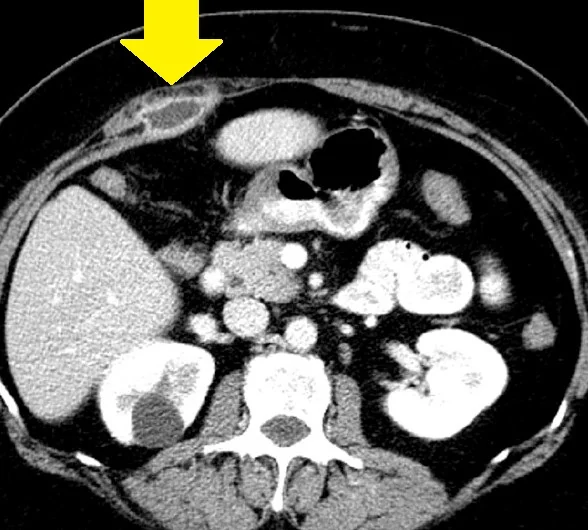
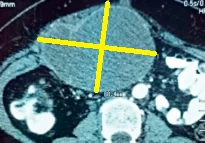
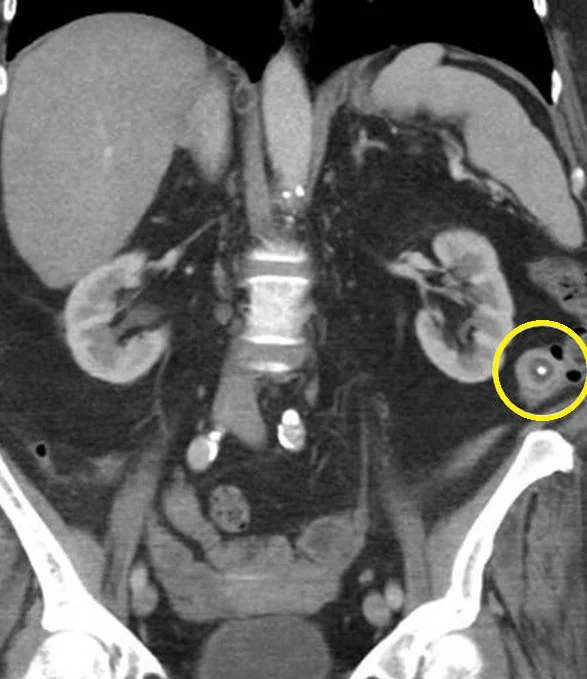
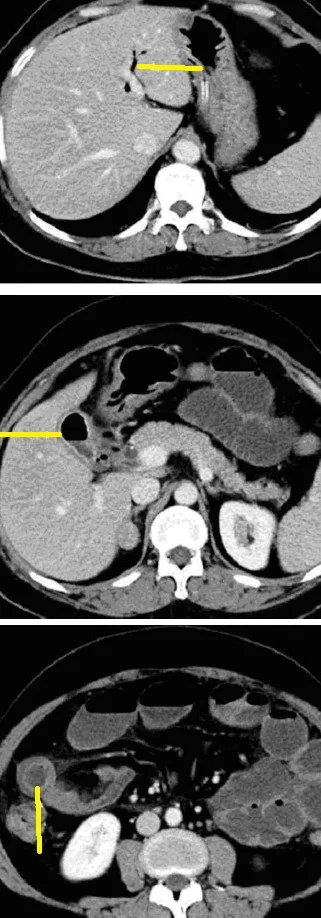
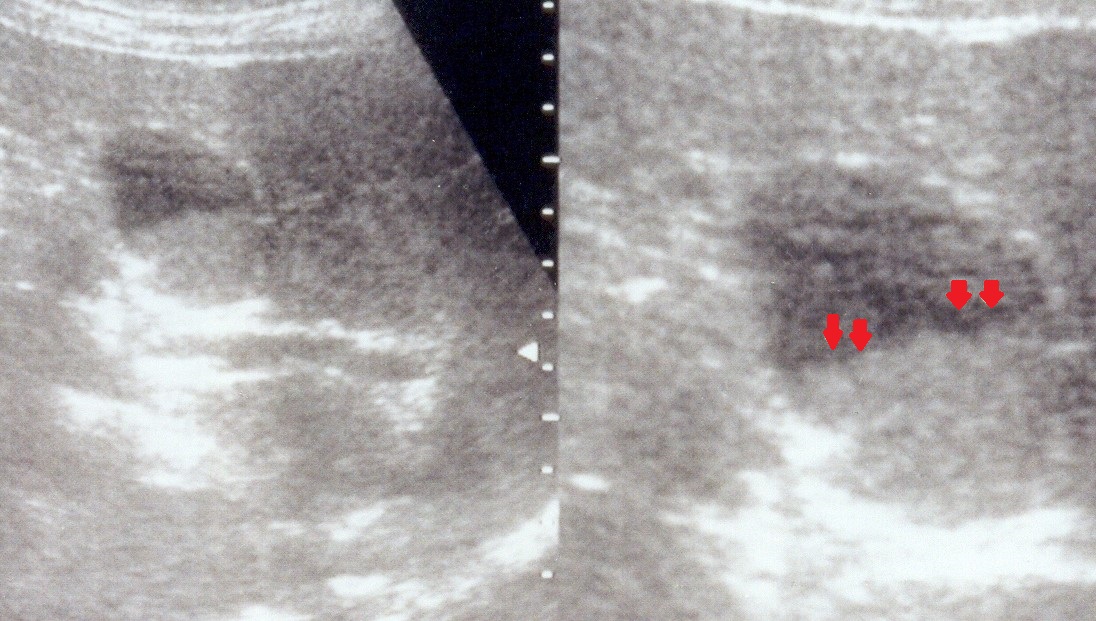
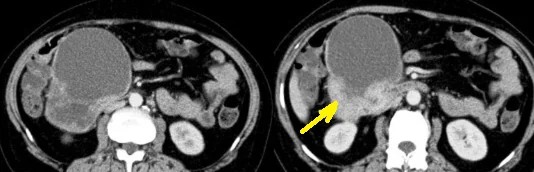
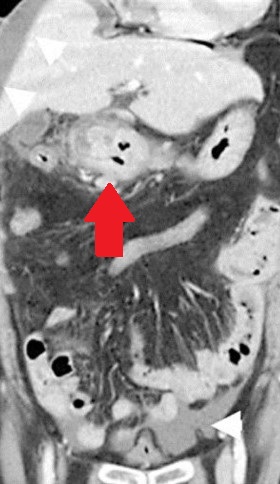
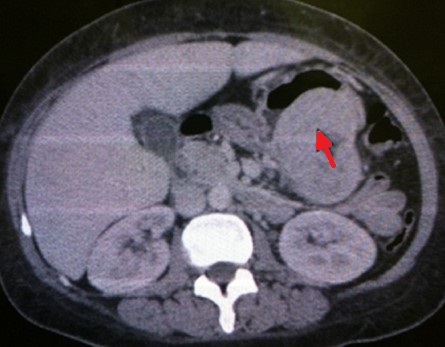
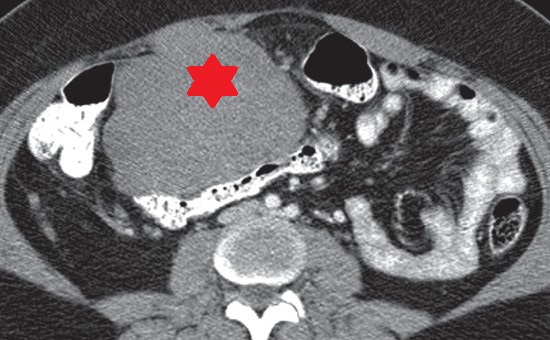
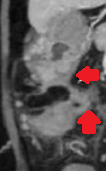
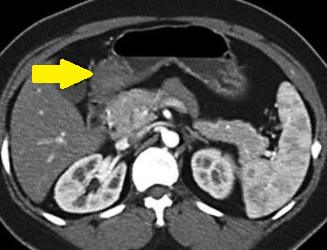
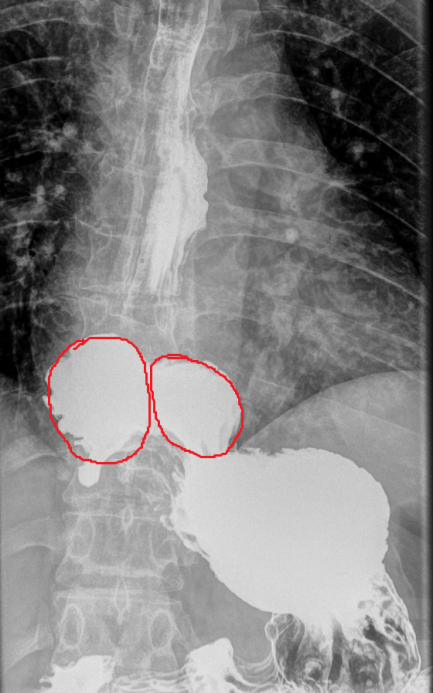
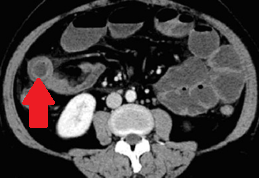
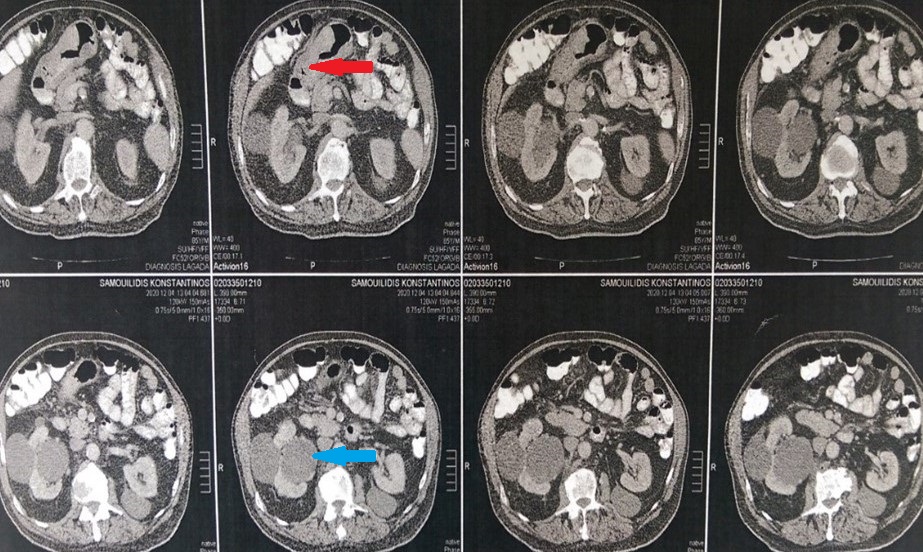
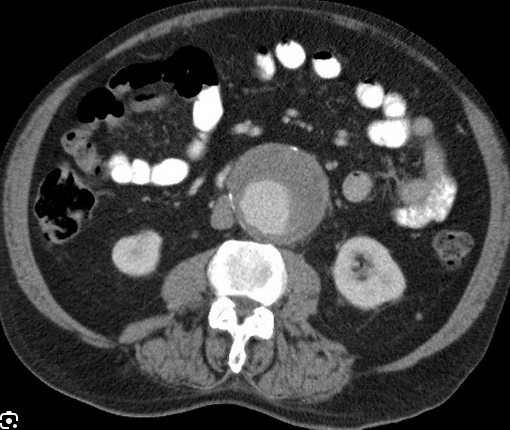
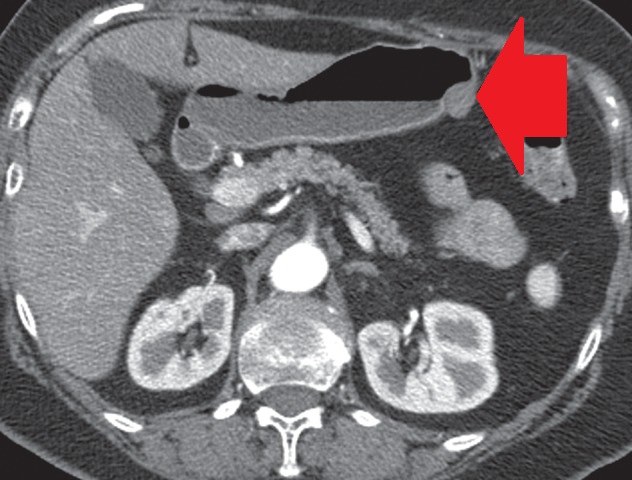
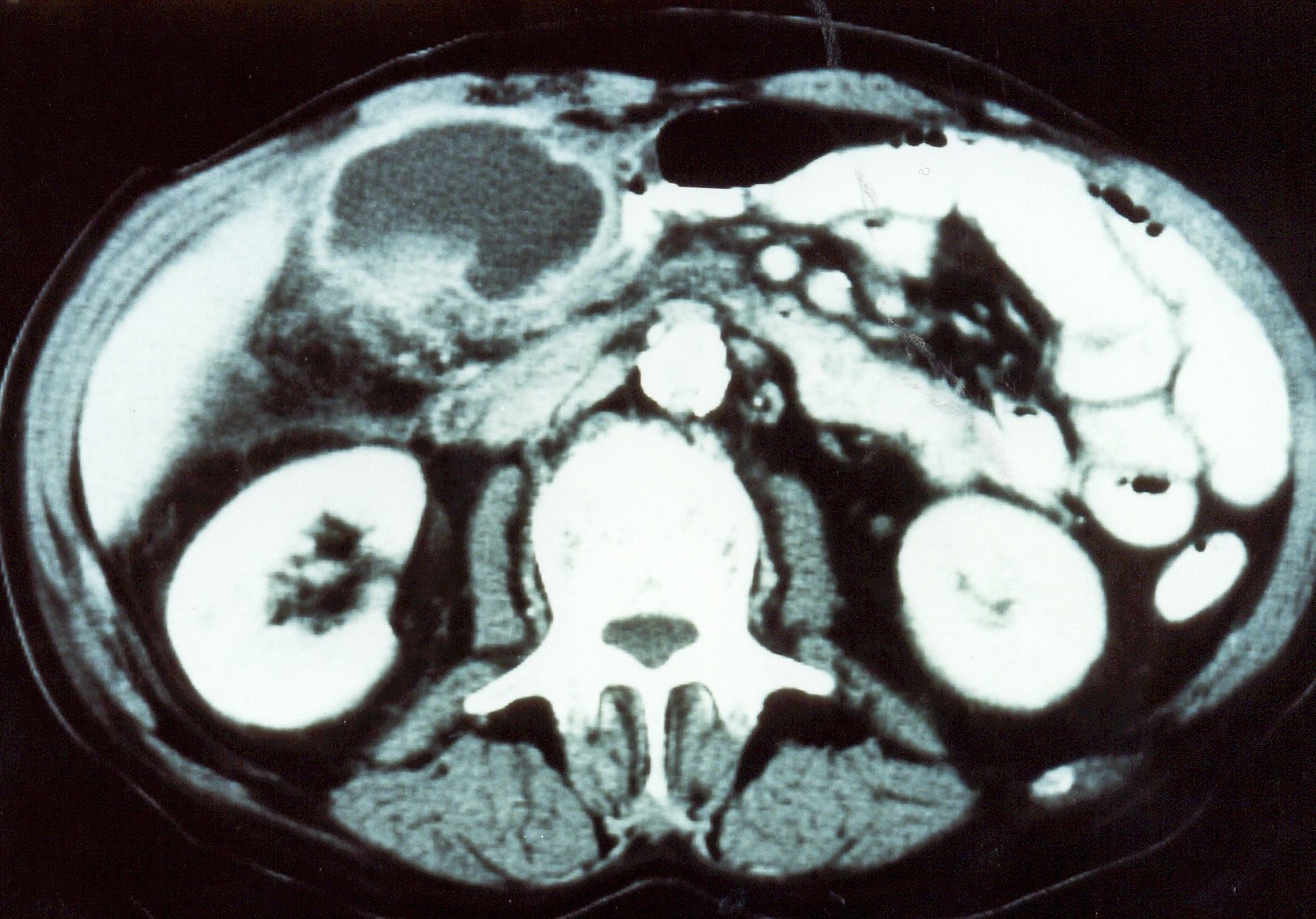
Abdominal CT scan. Red outline – Inflammatory fibroid polyp of the duodenum (Courtesy Dr. V. Penopoulos)
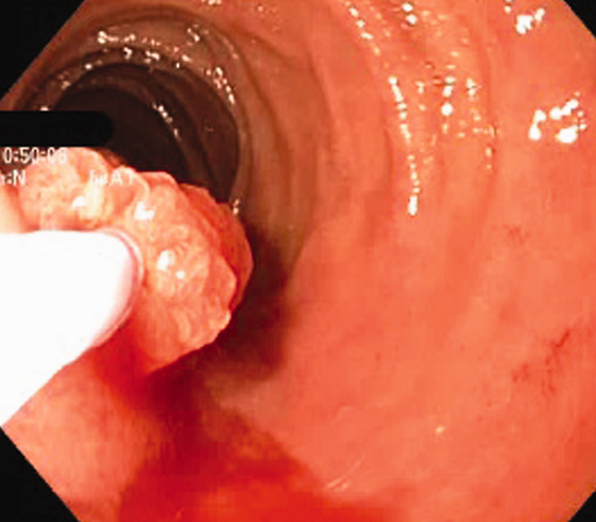
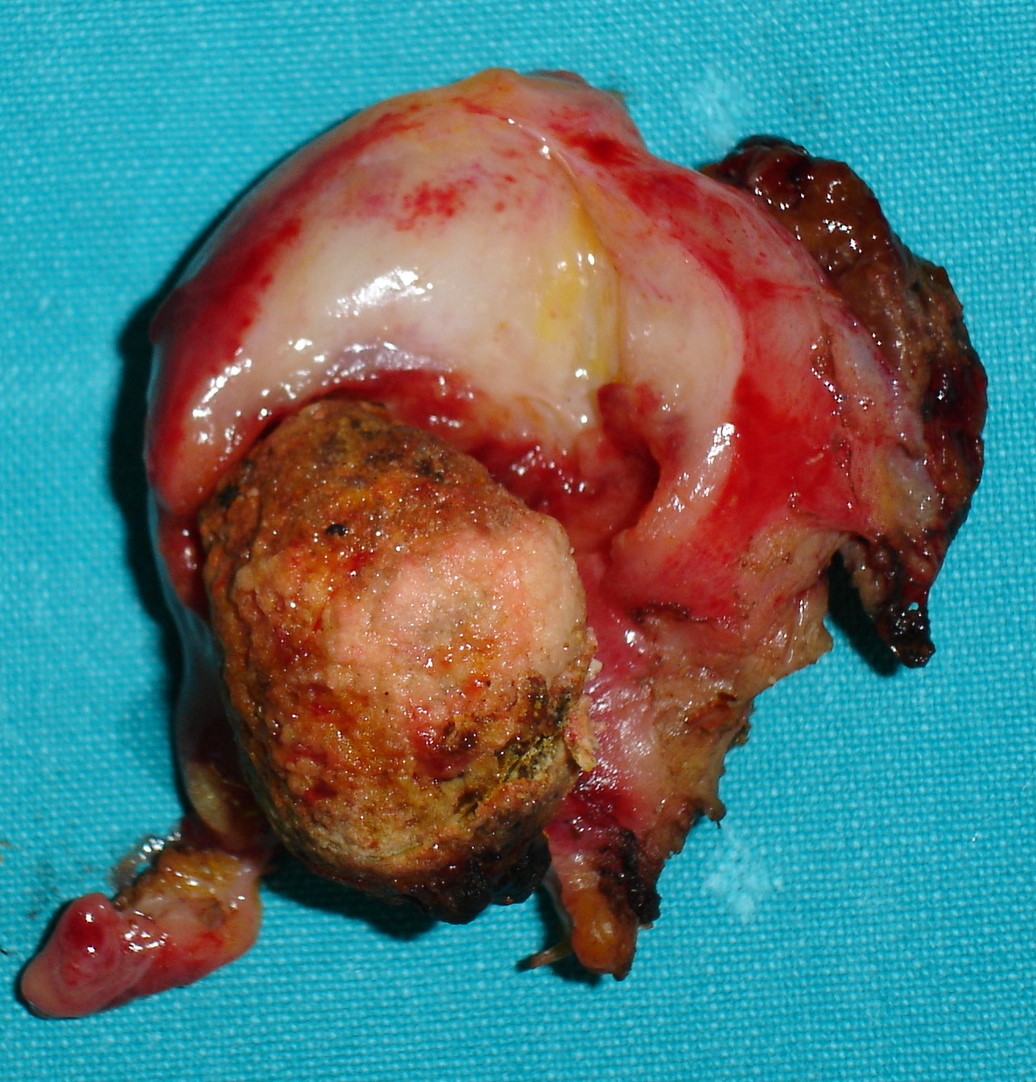
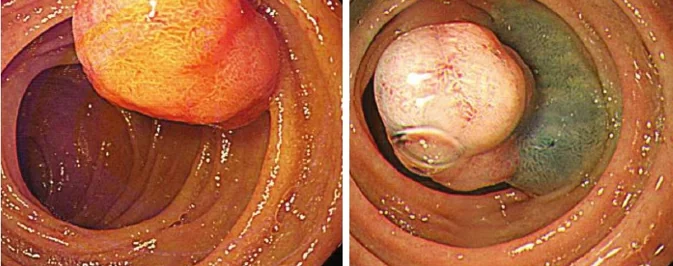
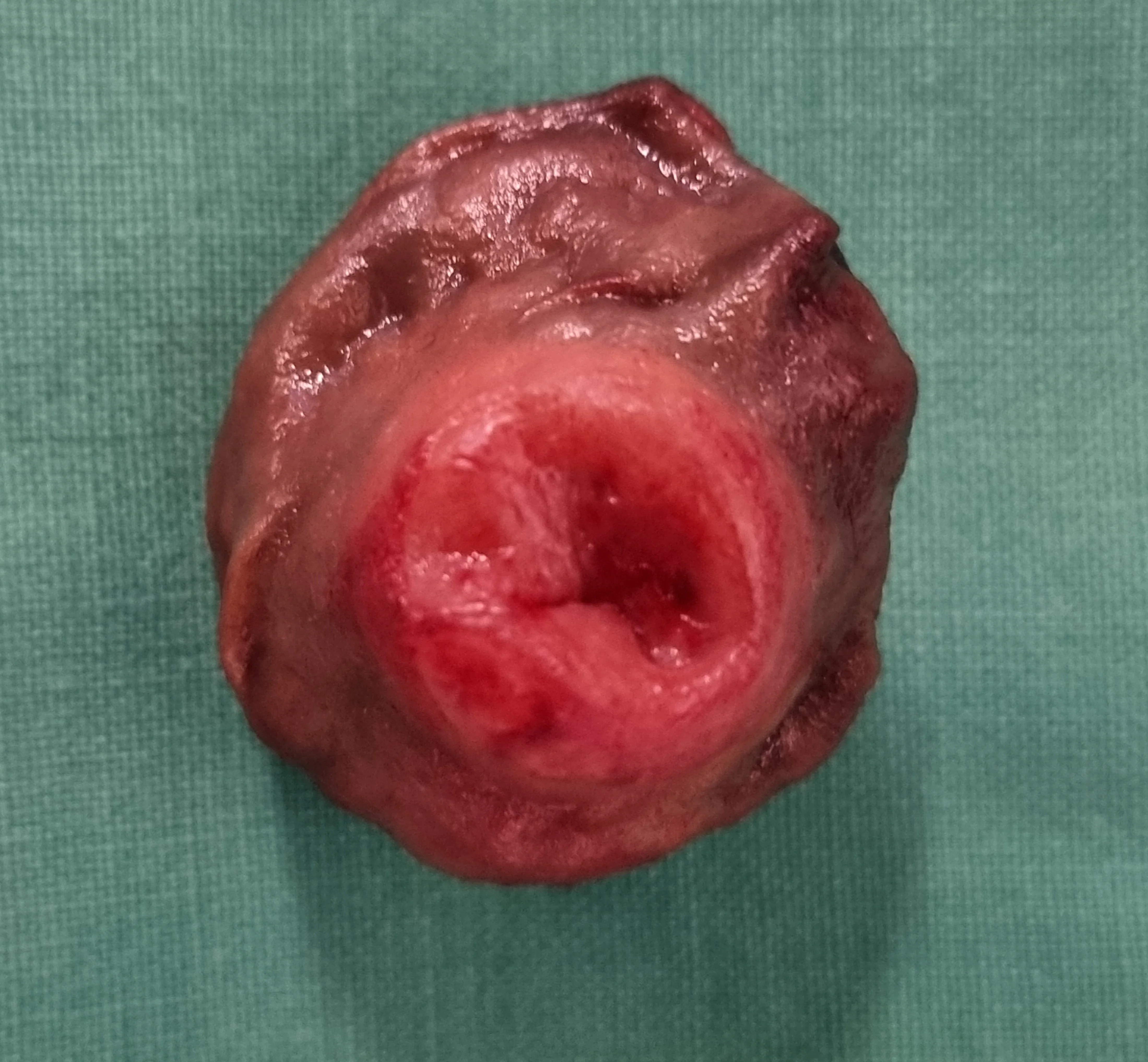
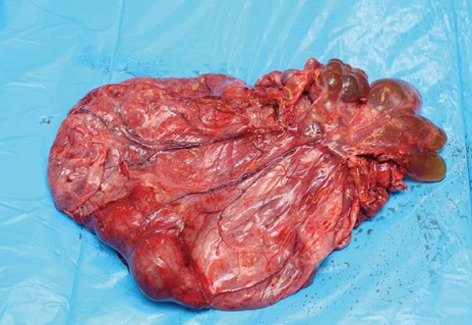
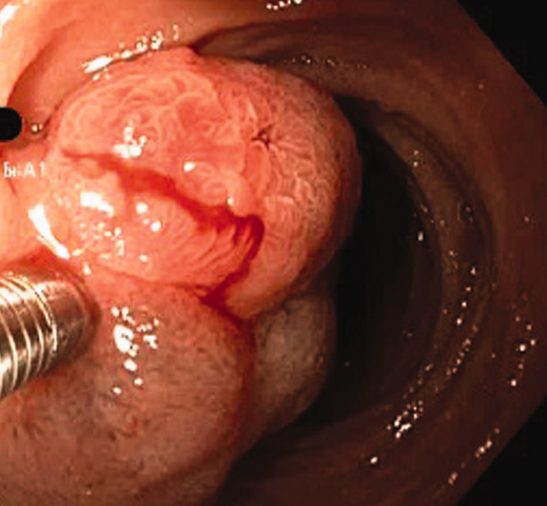
Duodenal Inflammatory fibroid polyp excised endoscopically. (Courtesy Dr.T.Maris).

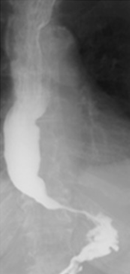
Postoperative esophagography.Smooth, unhindered passage of contrust through the myotomised esophagus.(Courtesy Dr.V.Penopoulos).

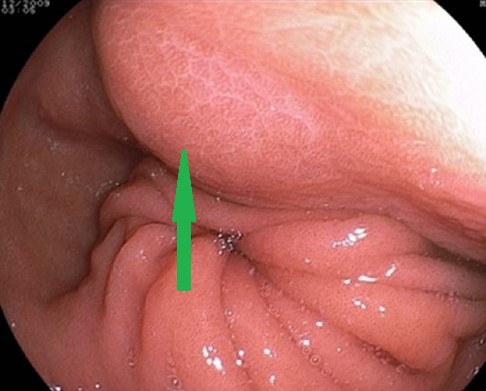
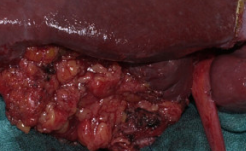
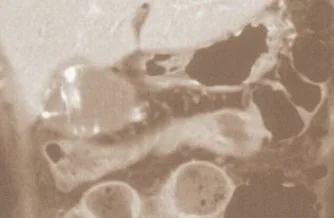
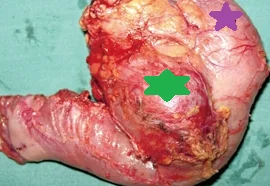
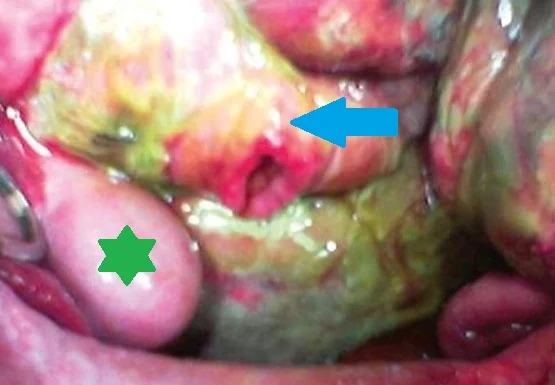
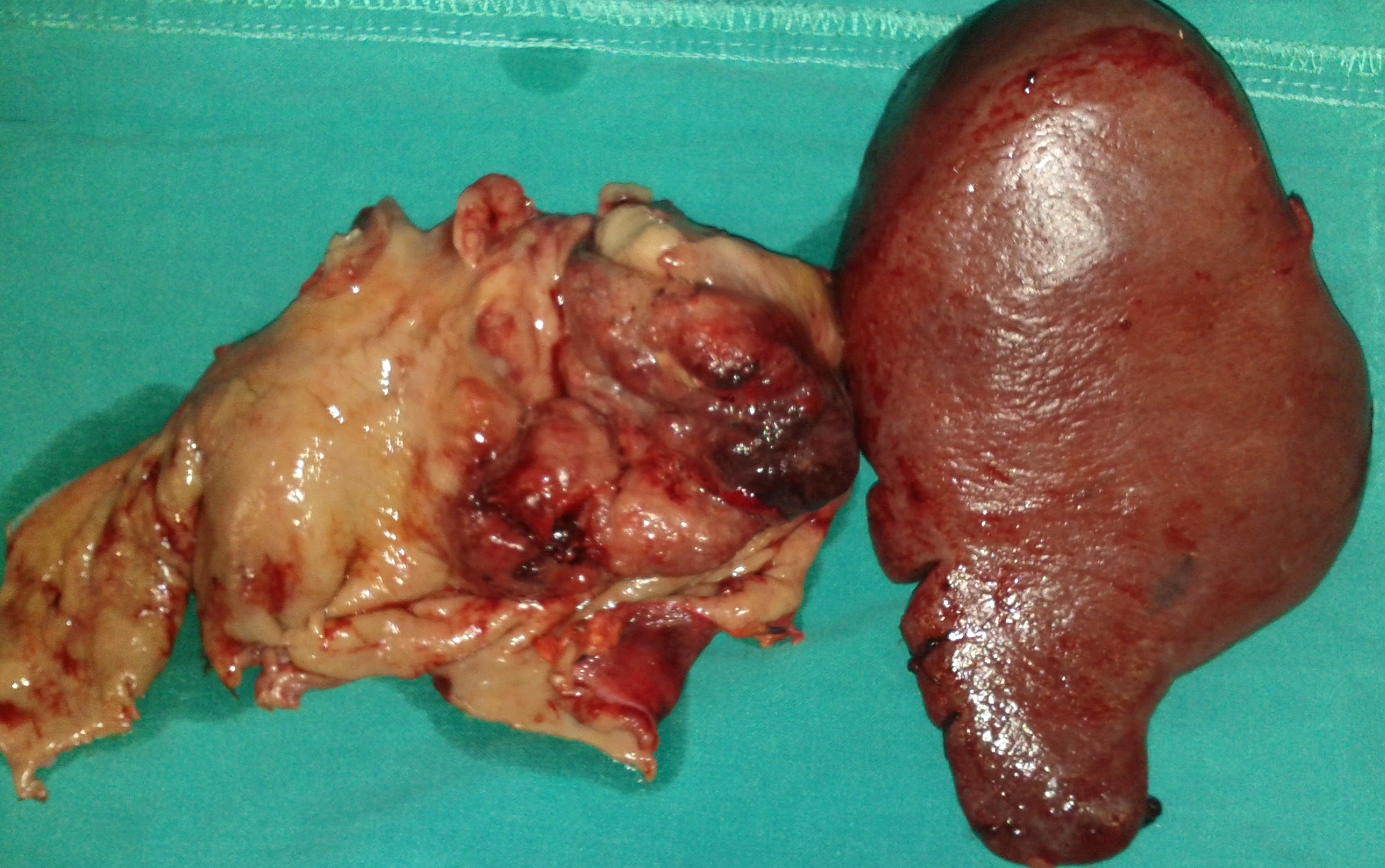
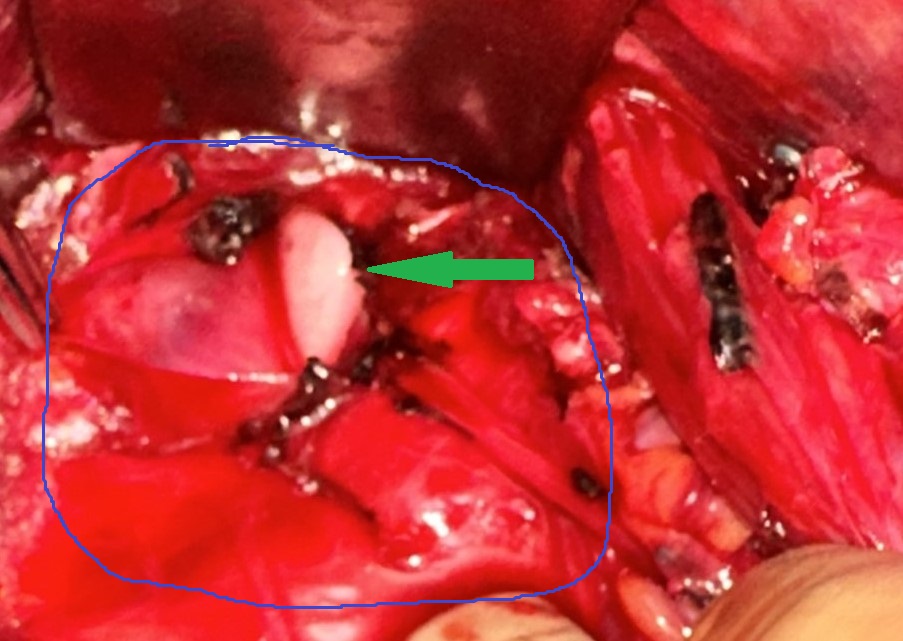
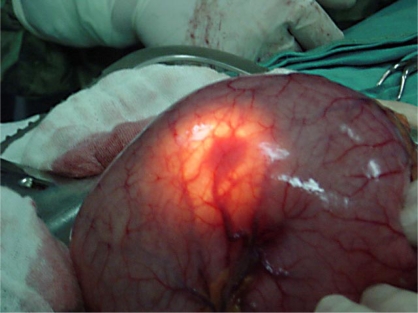
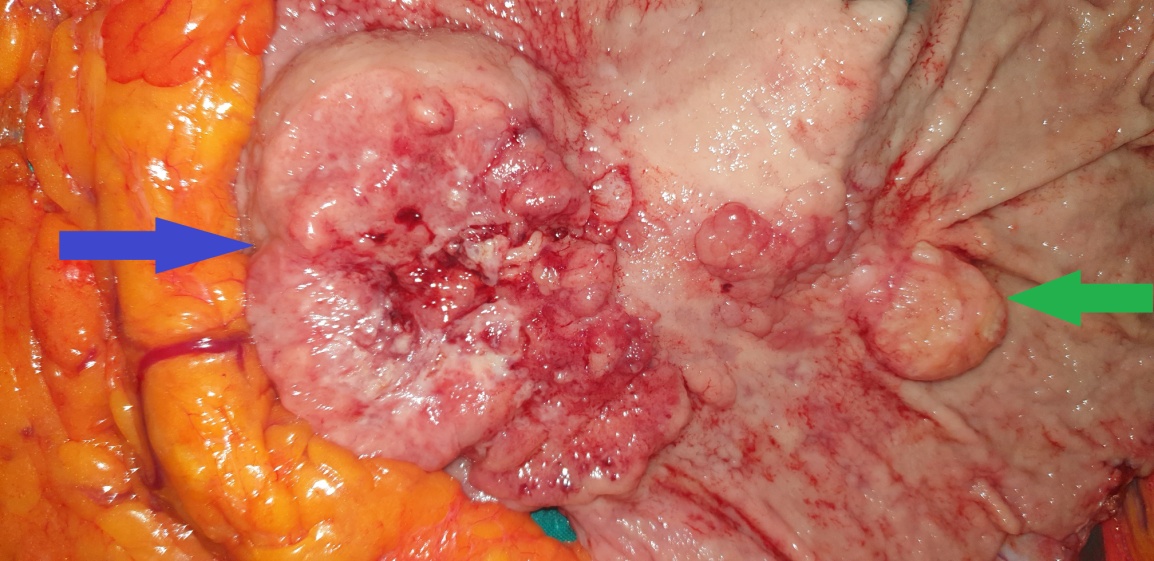
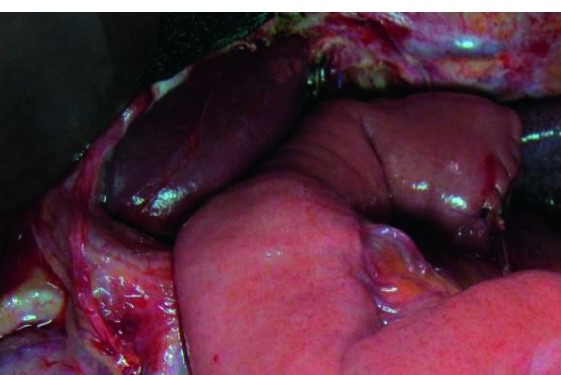
Blue arrow-stomach.Green arrow-gallbladder.Brown arrow-liver.(Courtesy Dr.V.Penopoulos).
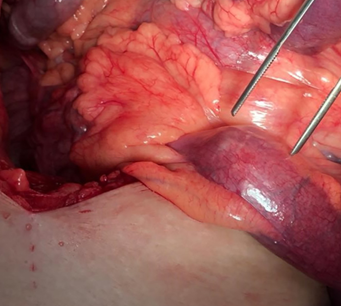
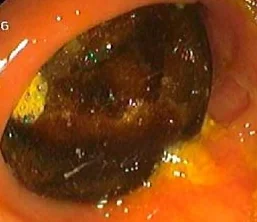
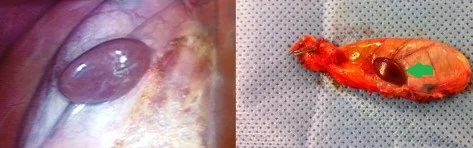
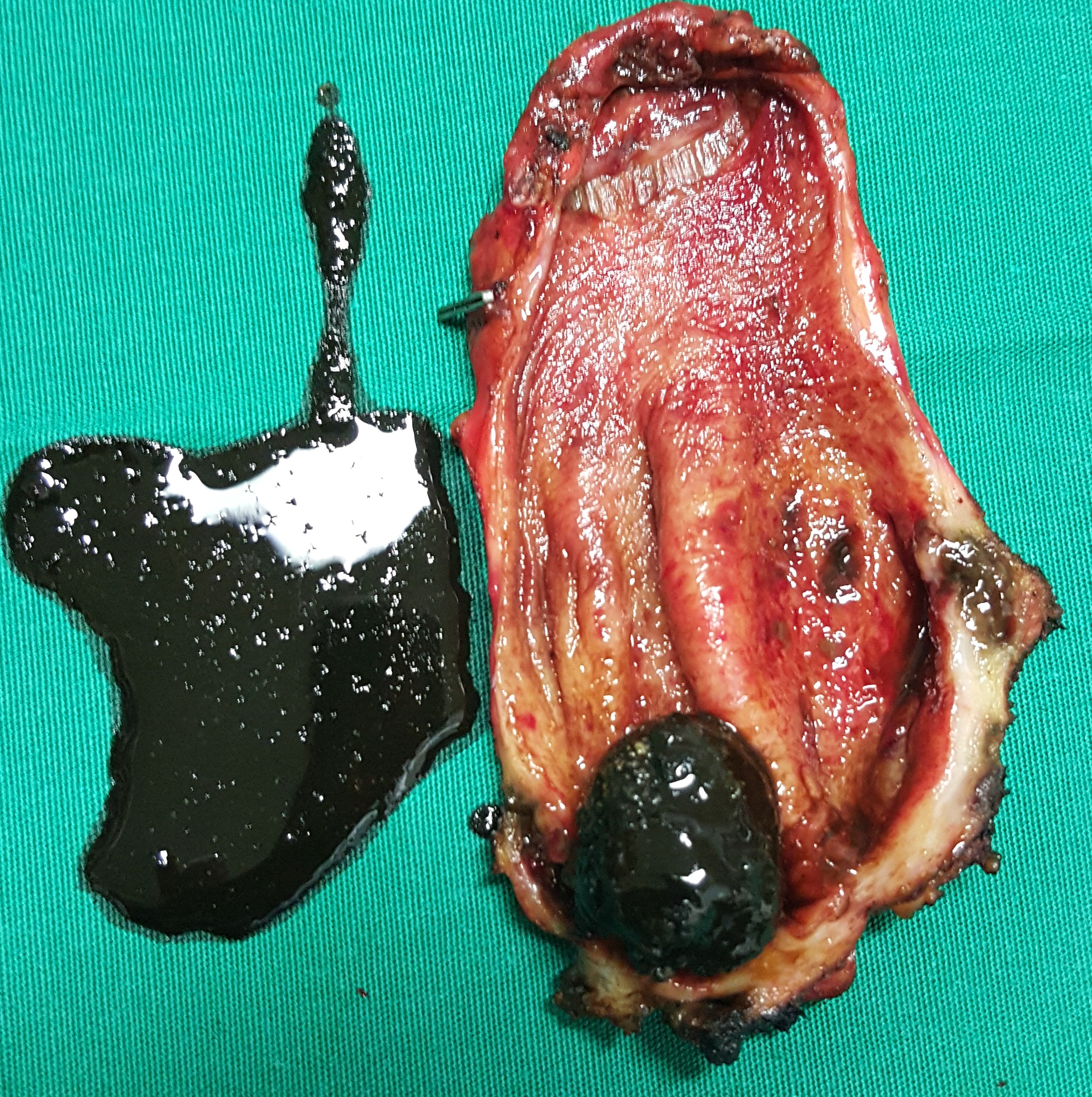
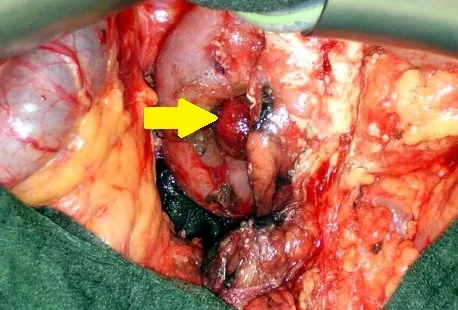
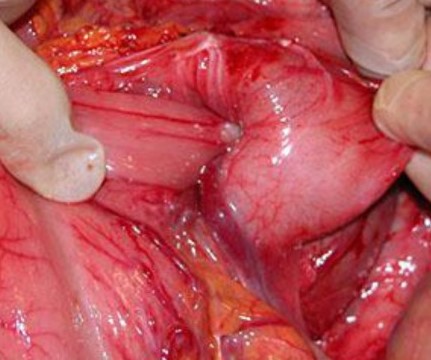
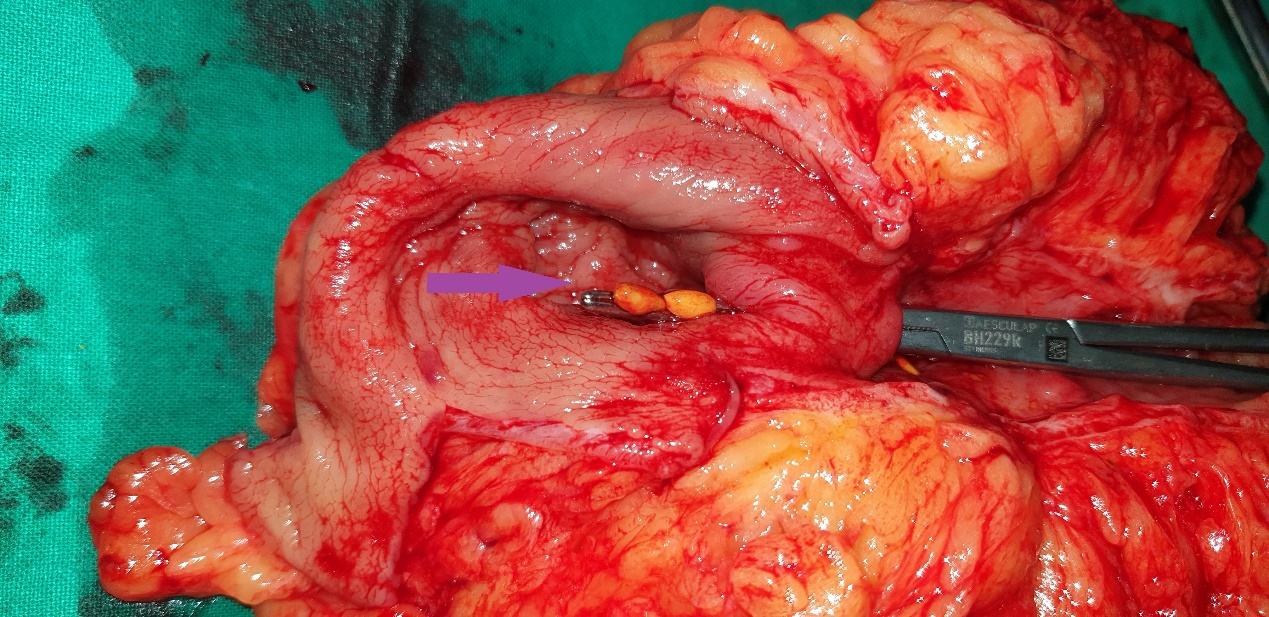
Forceps pointing towards gallstone impaction site in terminal ileum.(Courtesy Dr.V.Penopoulos).
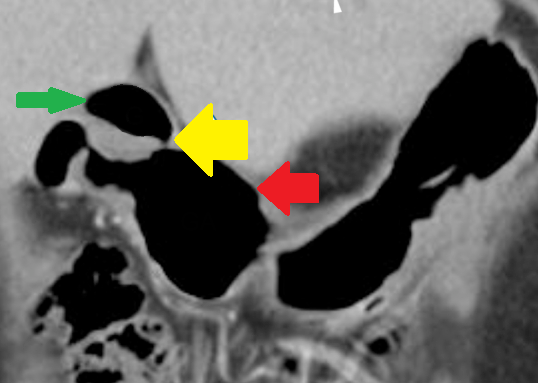
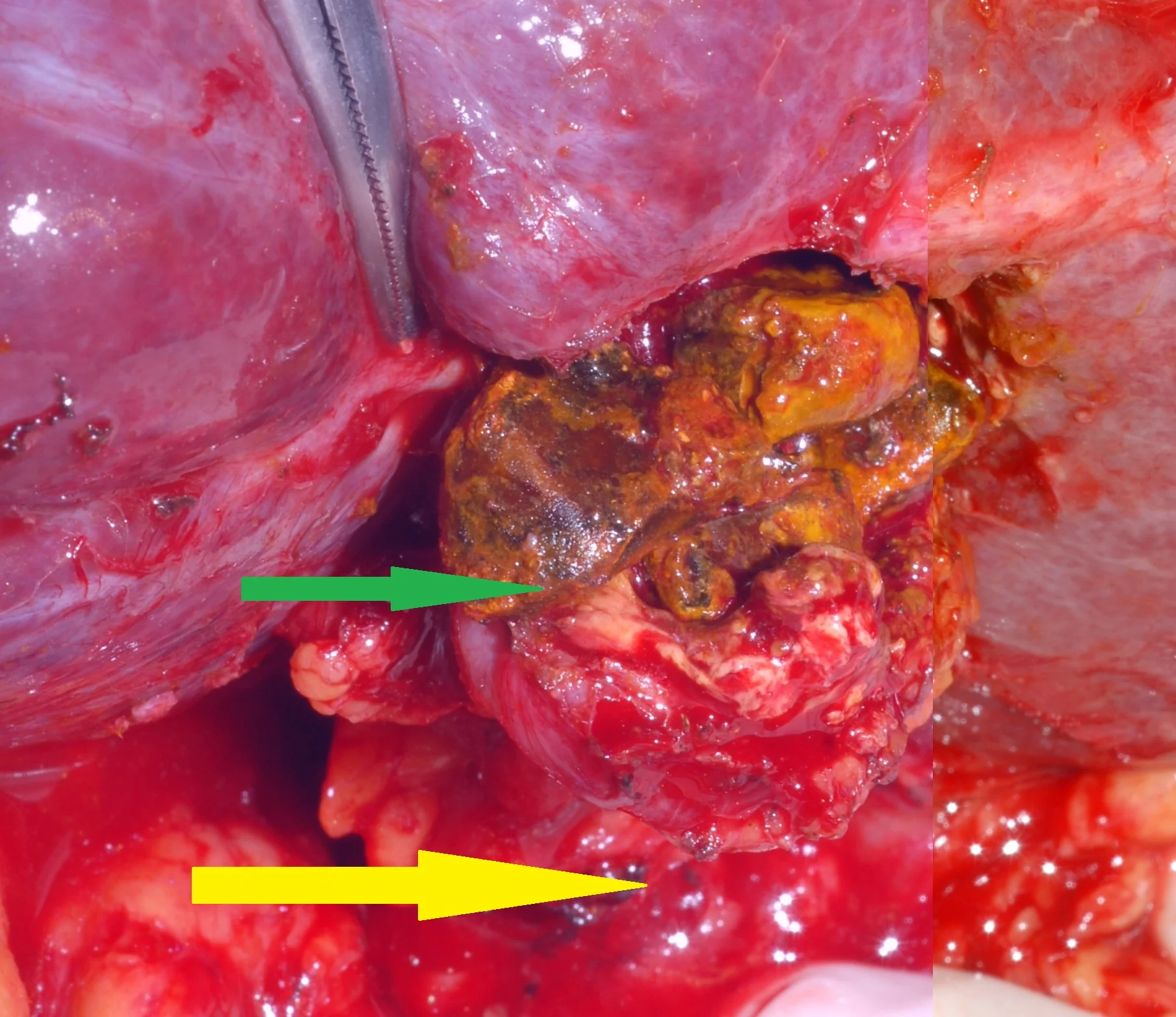
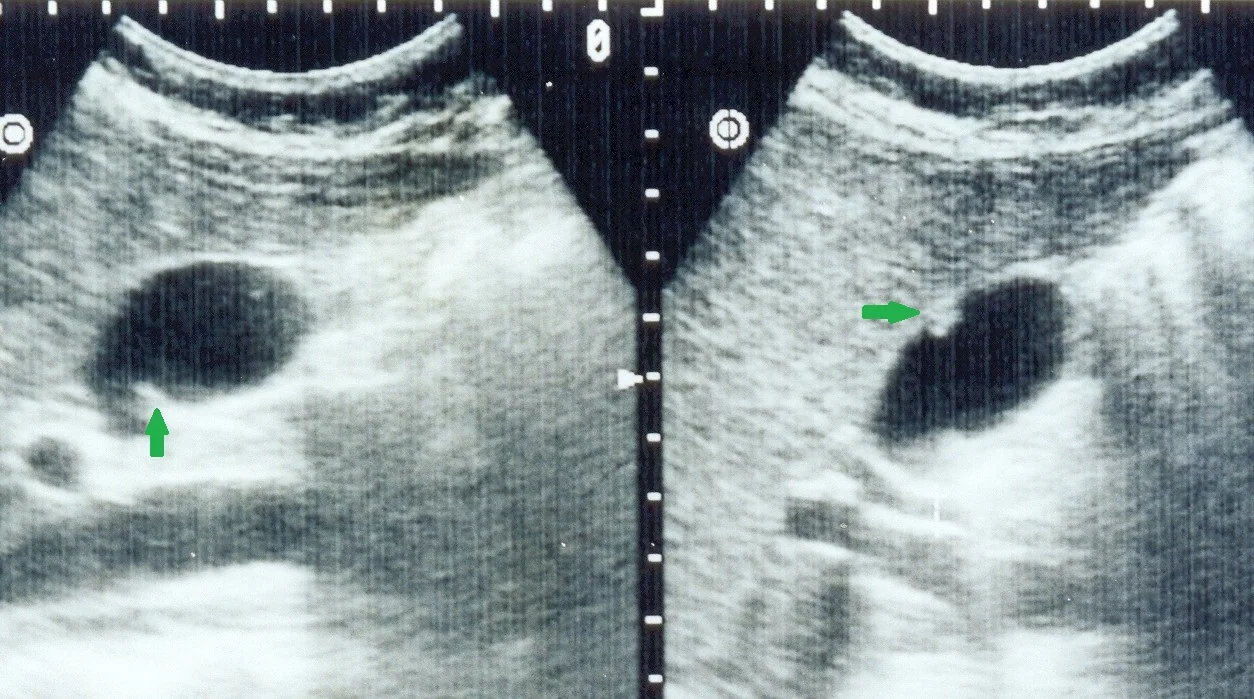
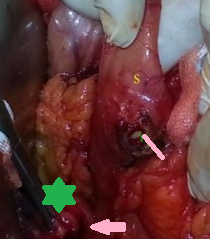
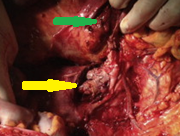
Red arrow-stomach.Green arrow-gallbladder.Yellow arrow-Fistula.(Courtesy Dr.V.Penopoulos).


Plain abdominal radiographs. Small bowel loop distension. (Courtesy Dr. V. Penopoulos)

Abdominal plain X-Rays.Dilatation/distention of small bowel loops + radiopaque structure (gallstone).(Courtesy Dr.V.Penopoulos).


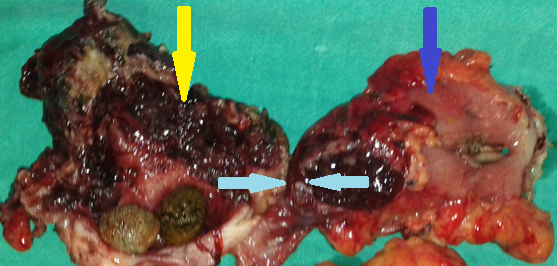
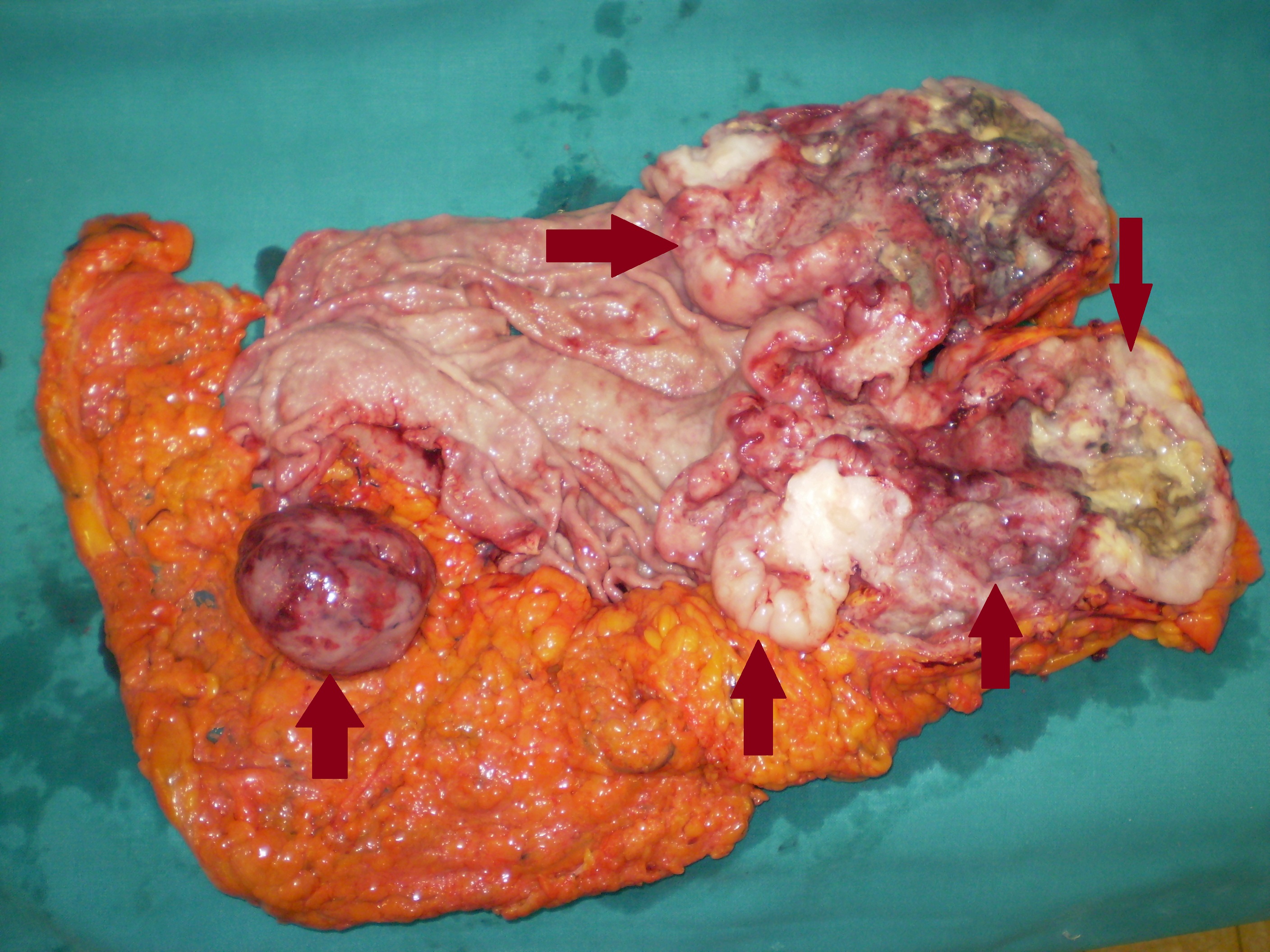
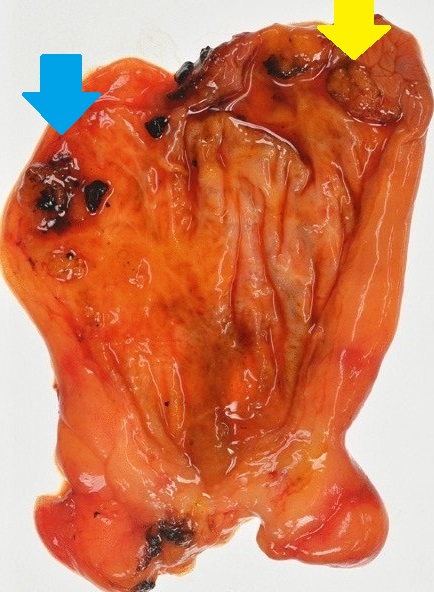
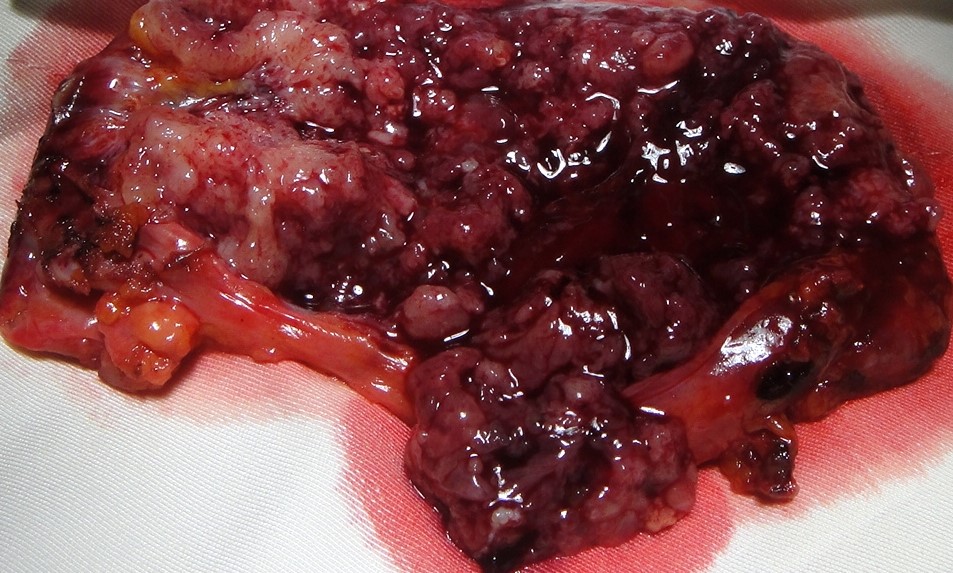
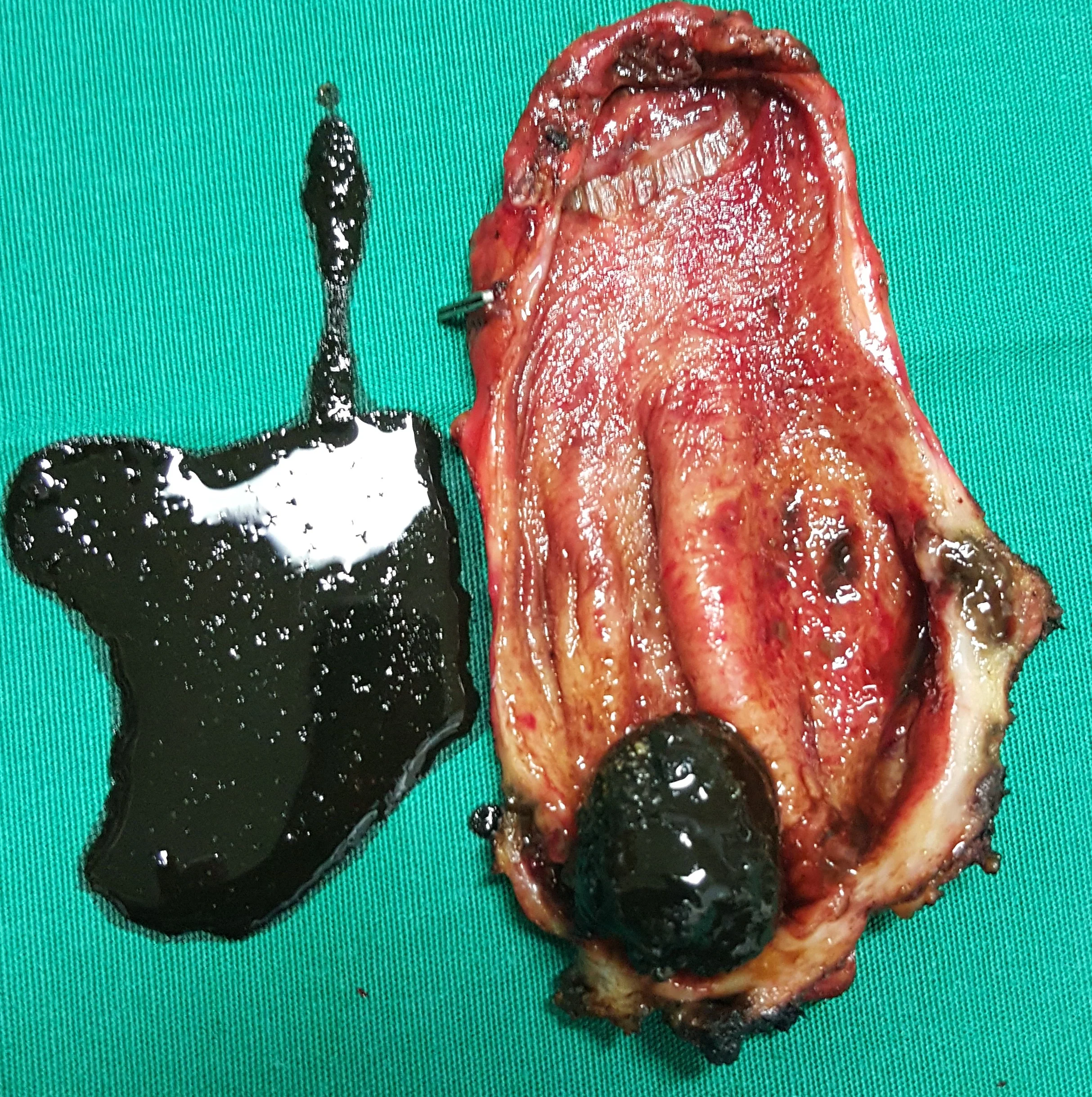
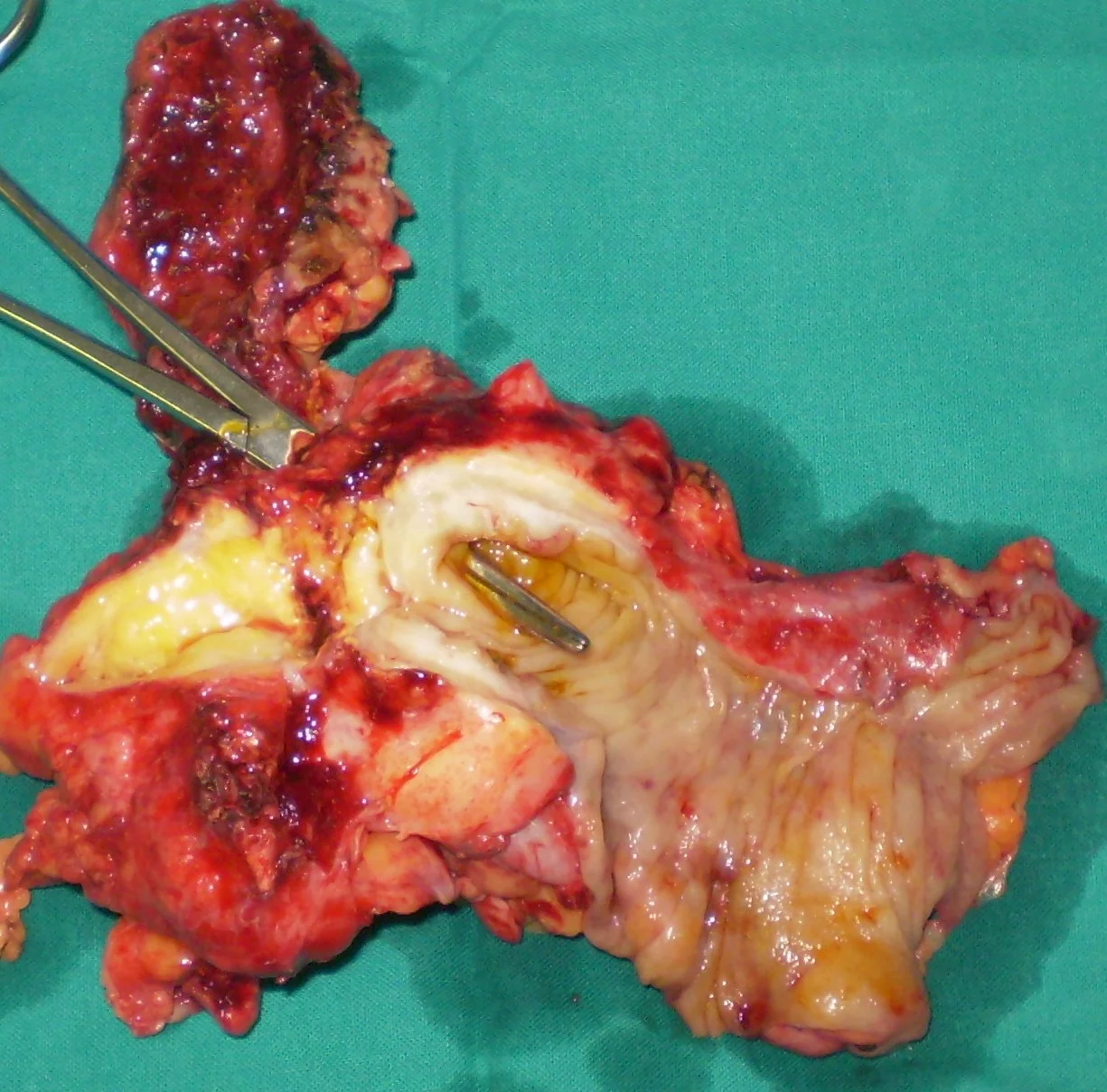
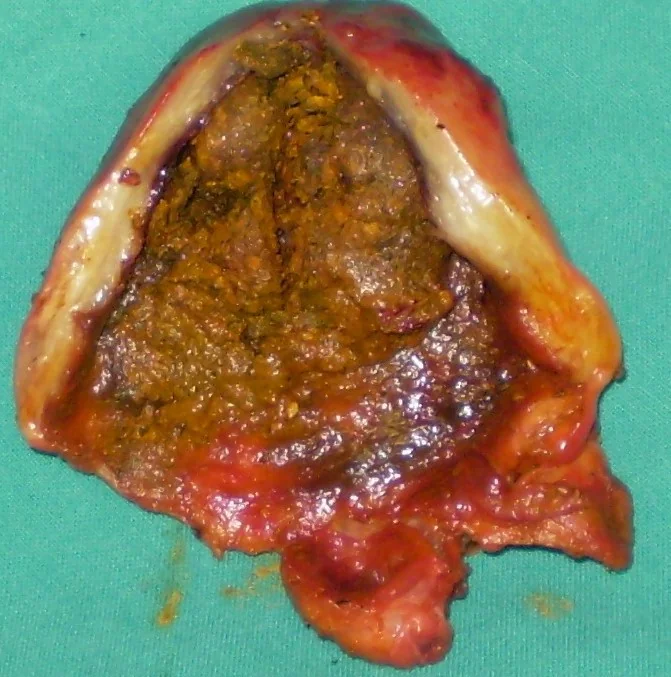
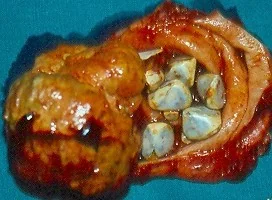
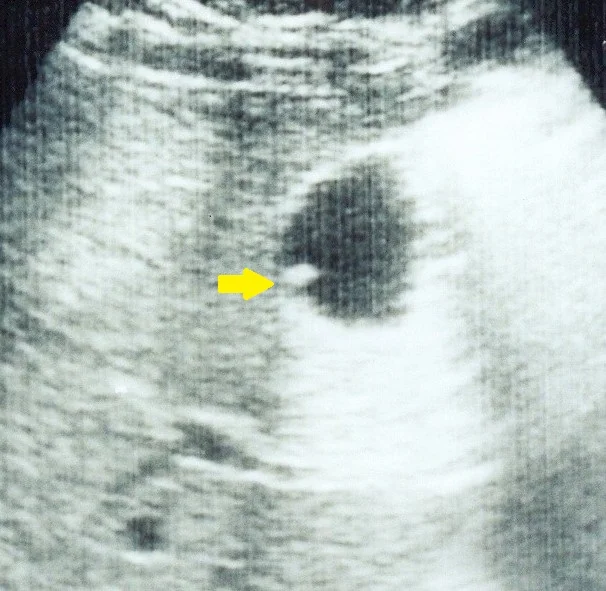
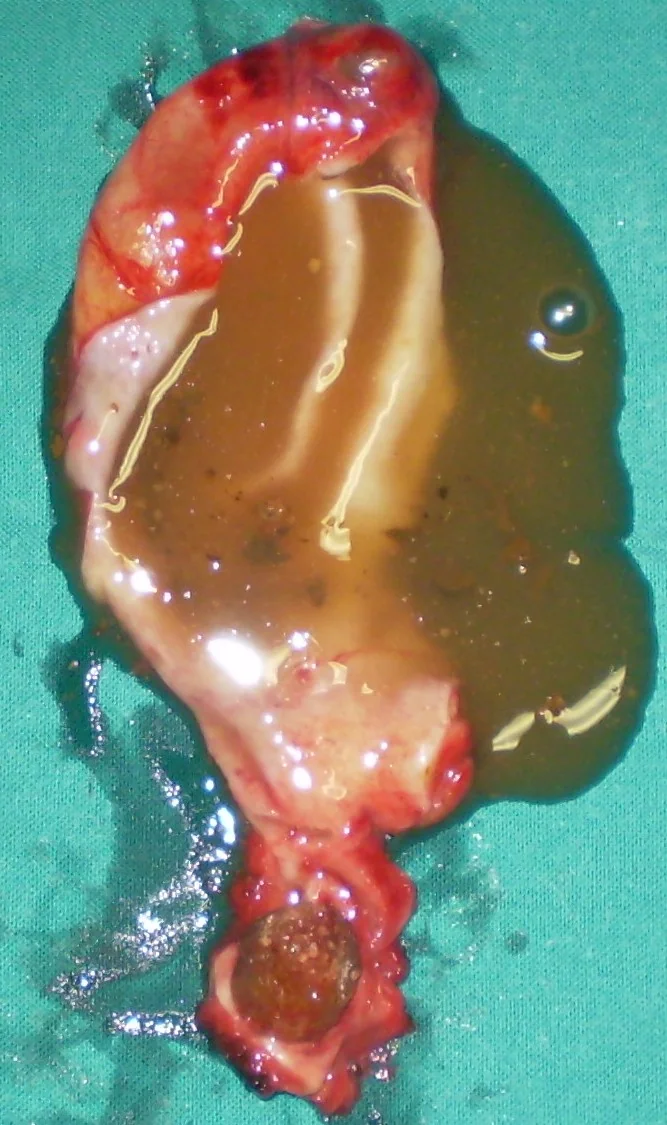
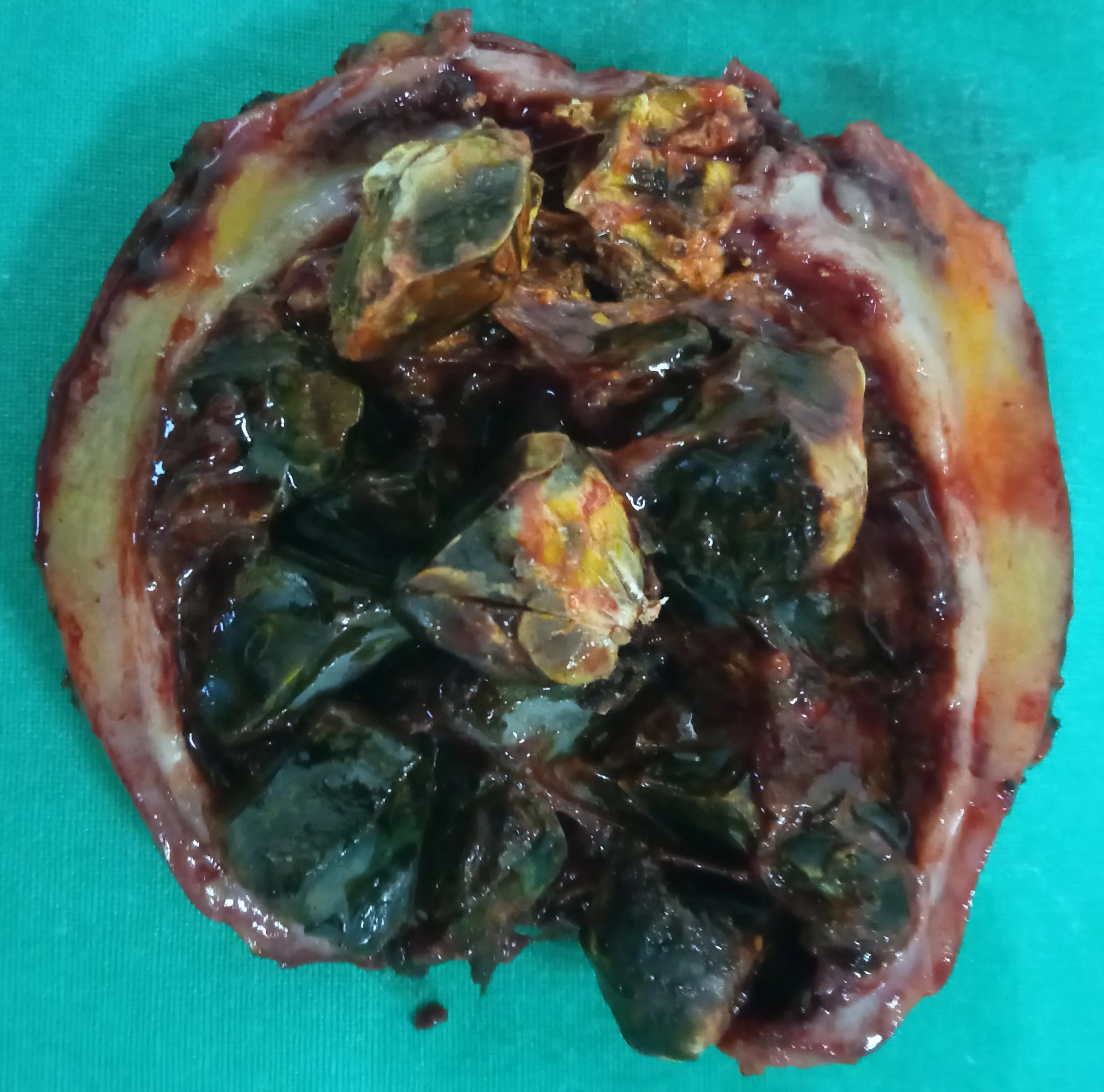
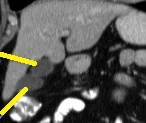
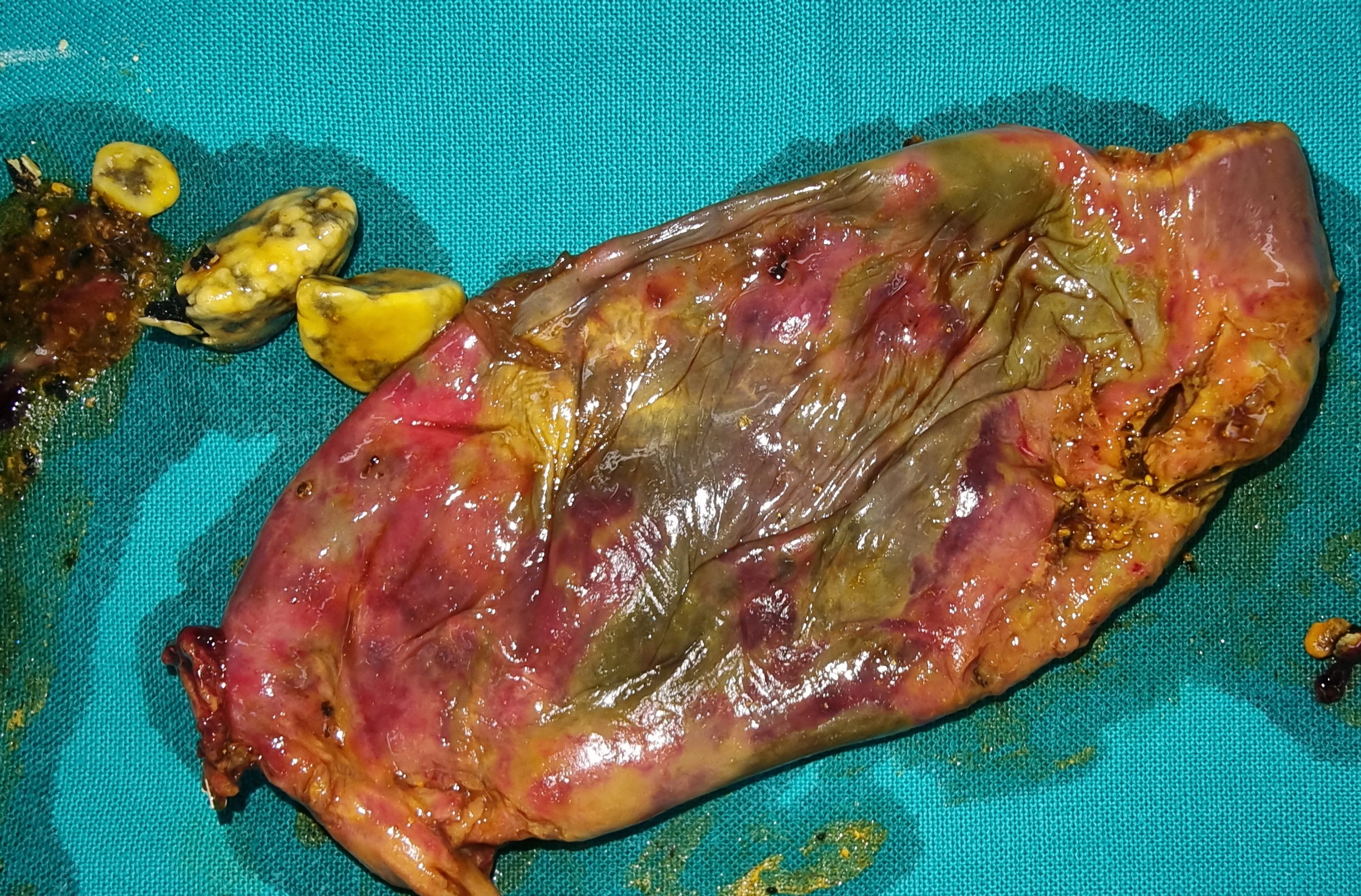
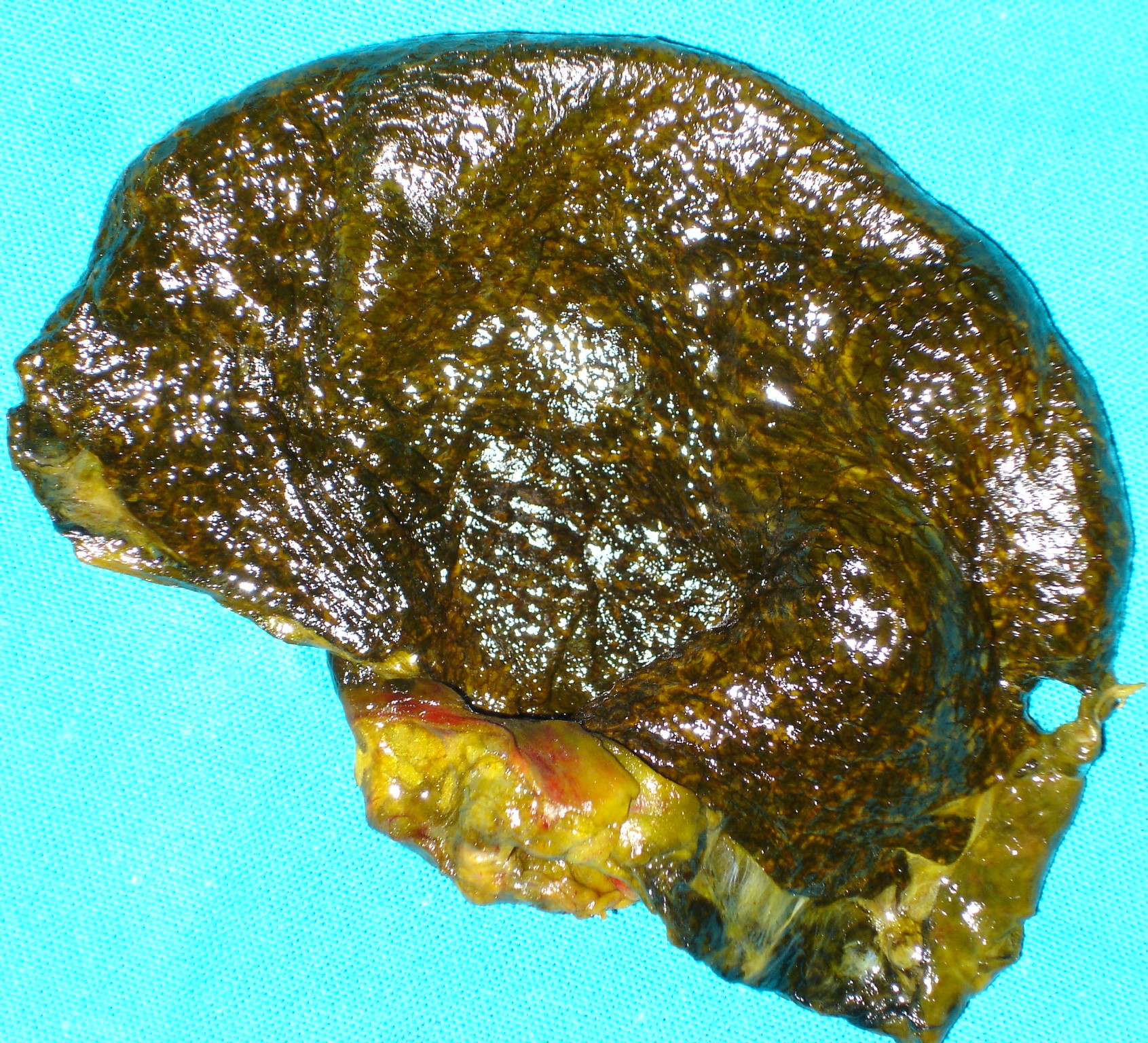
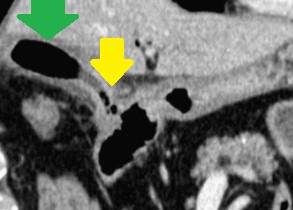
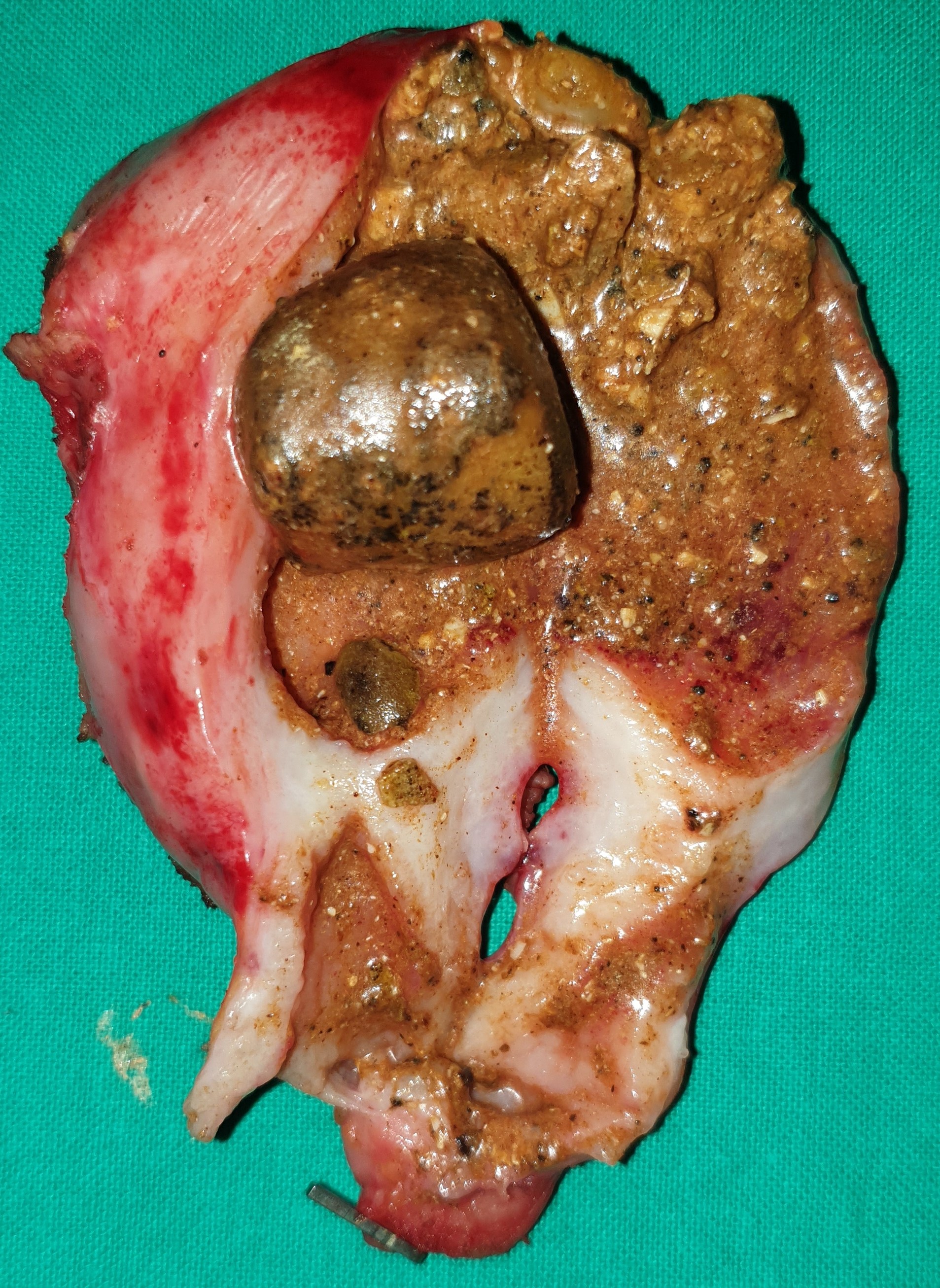
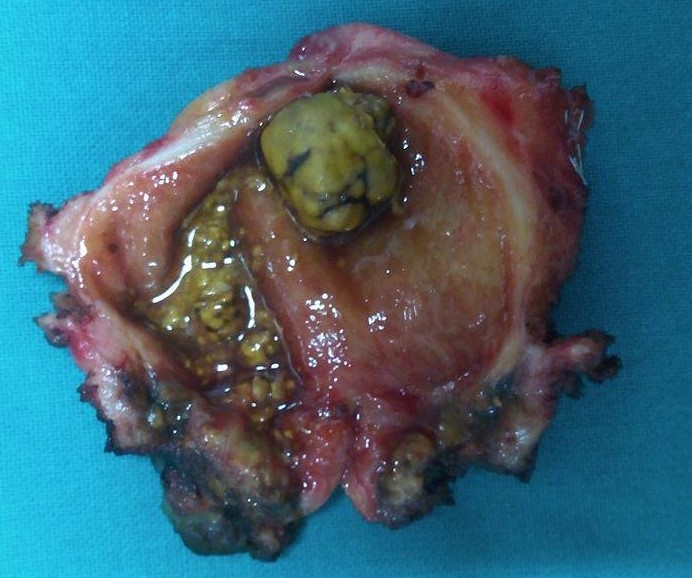
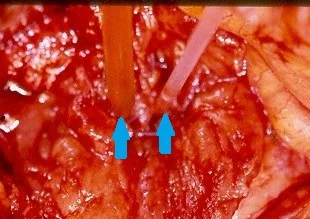
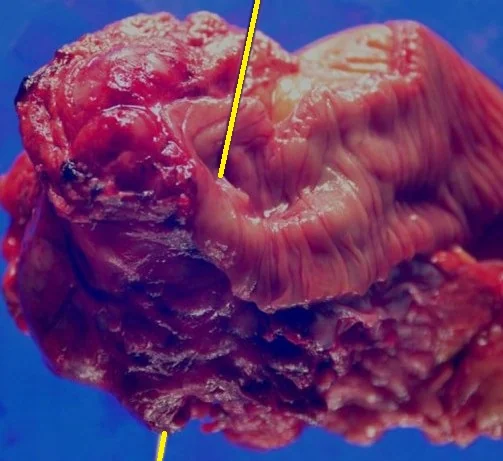
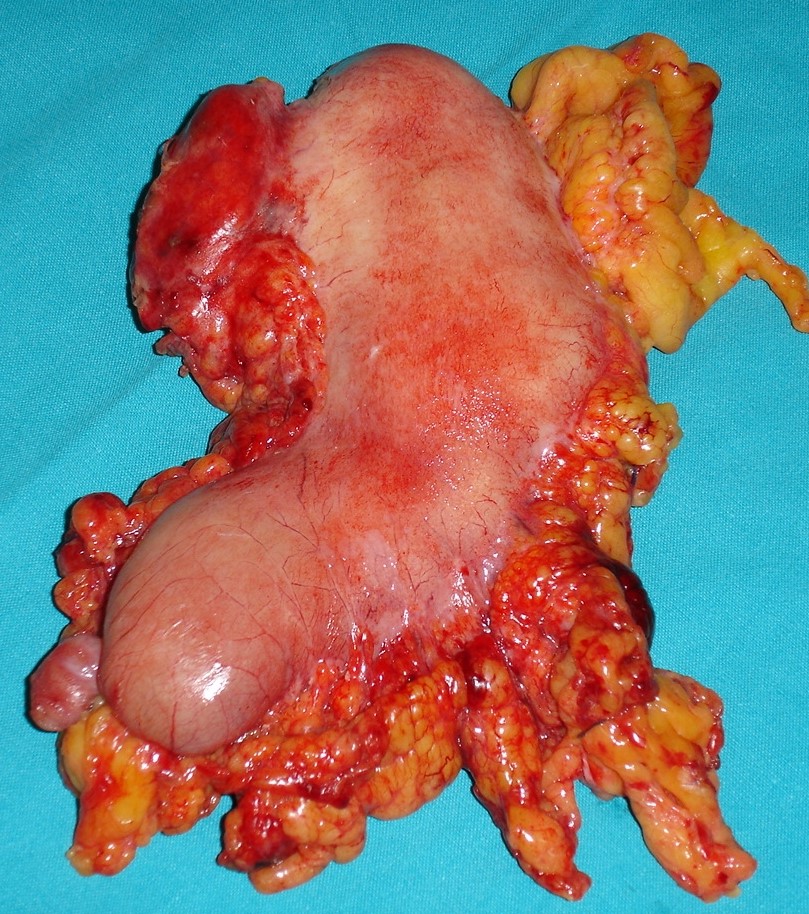
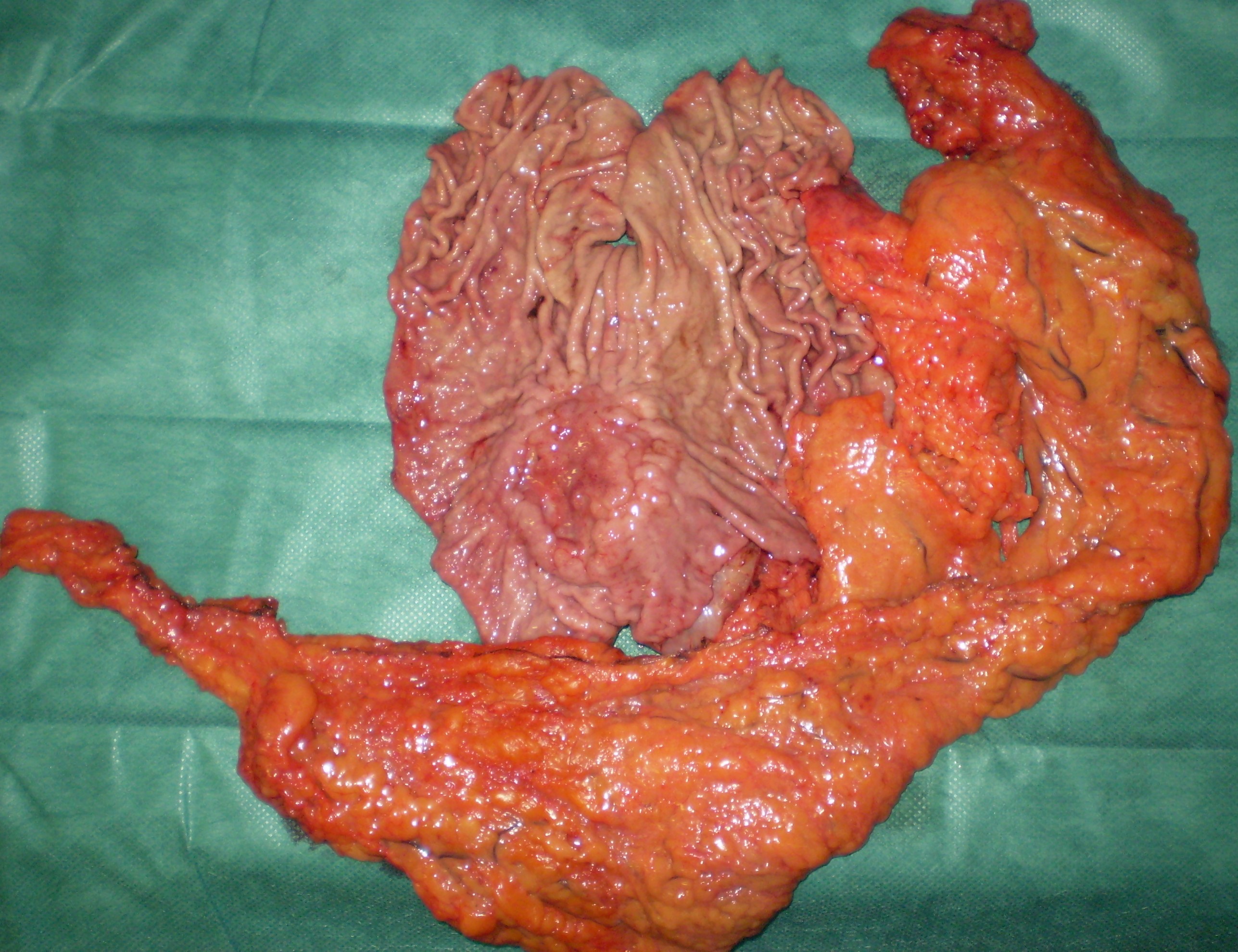
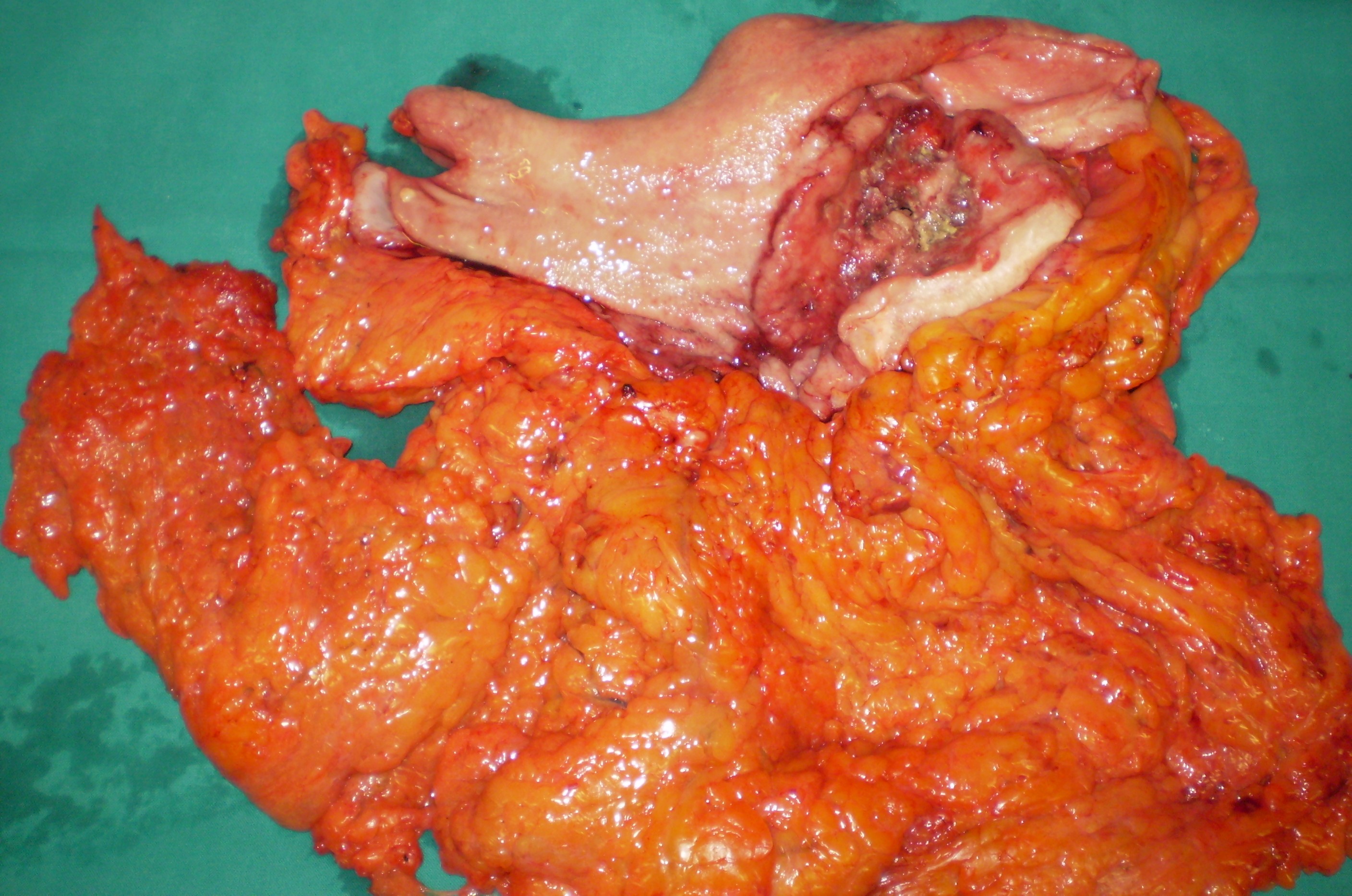
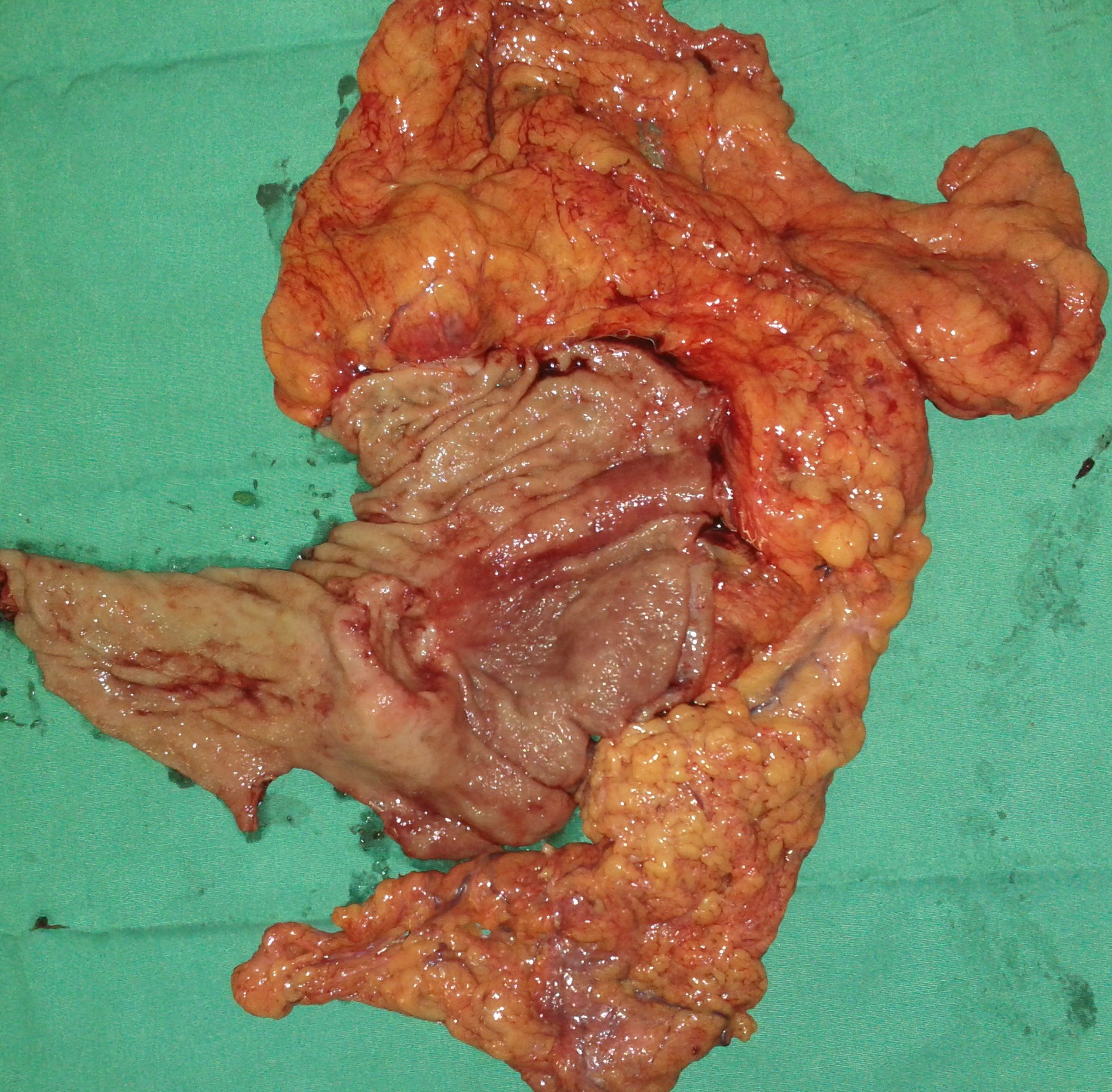
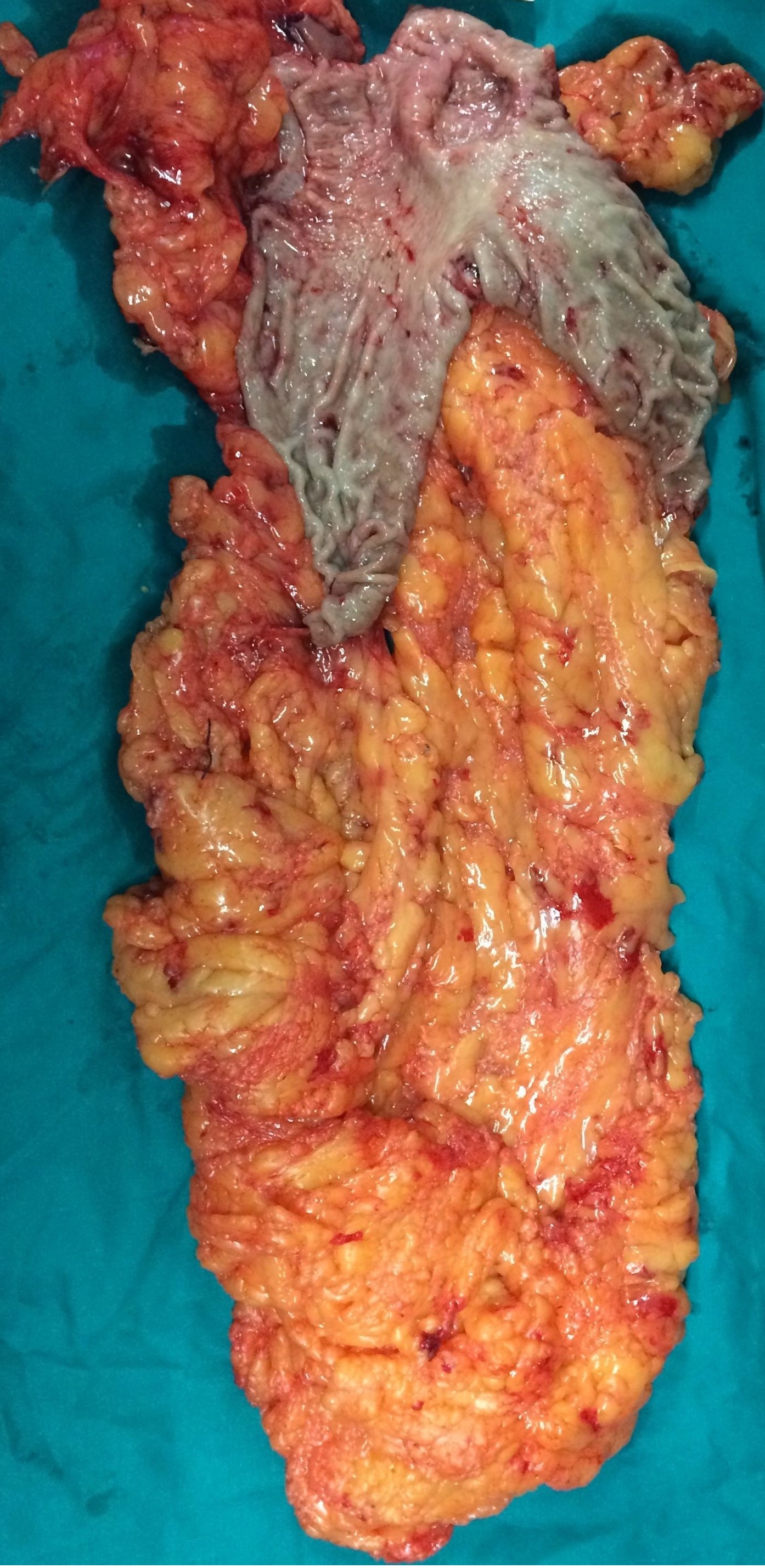
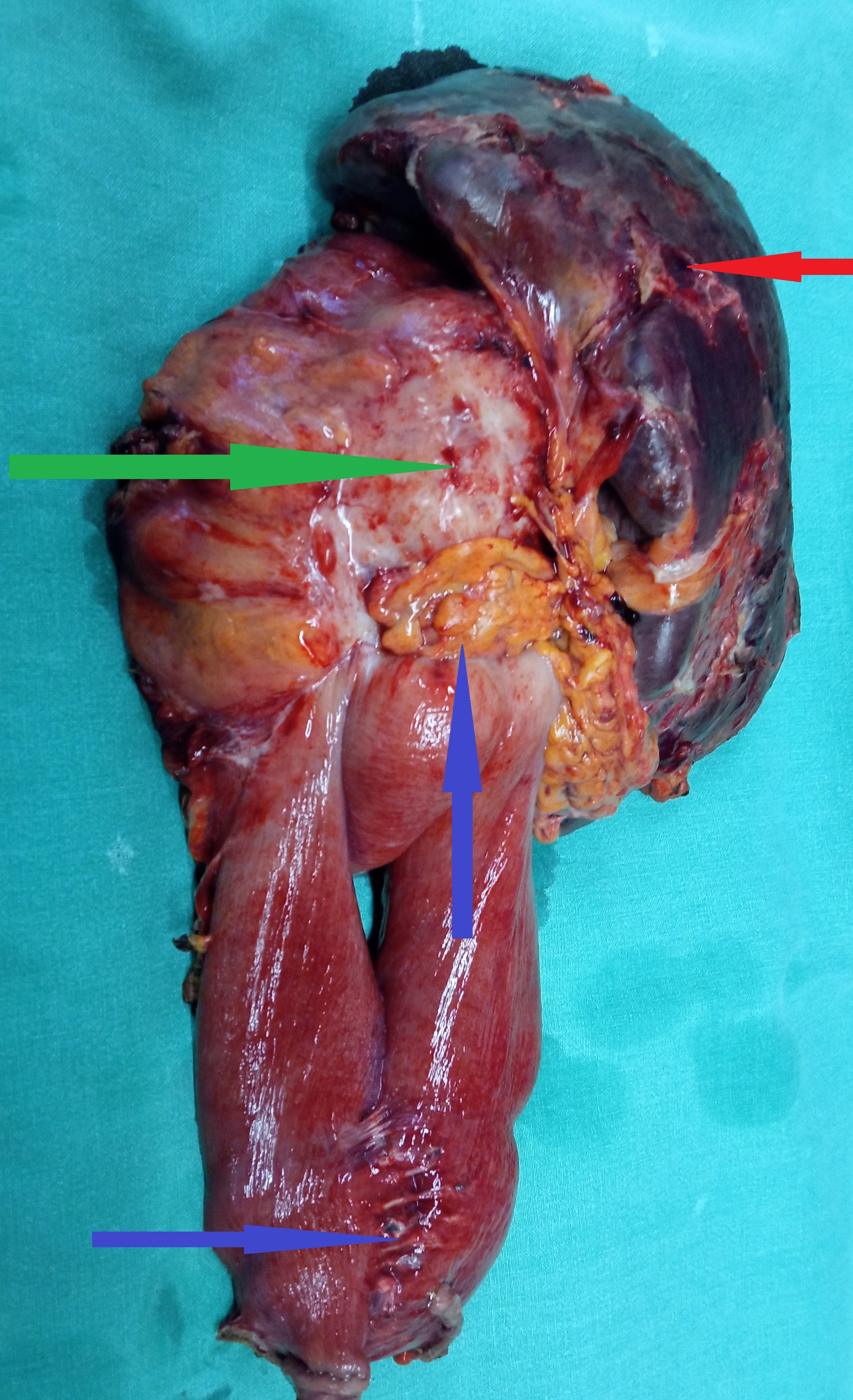
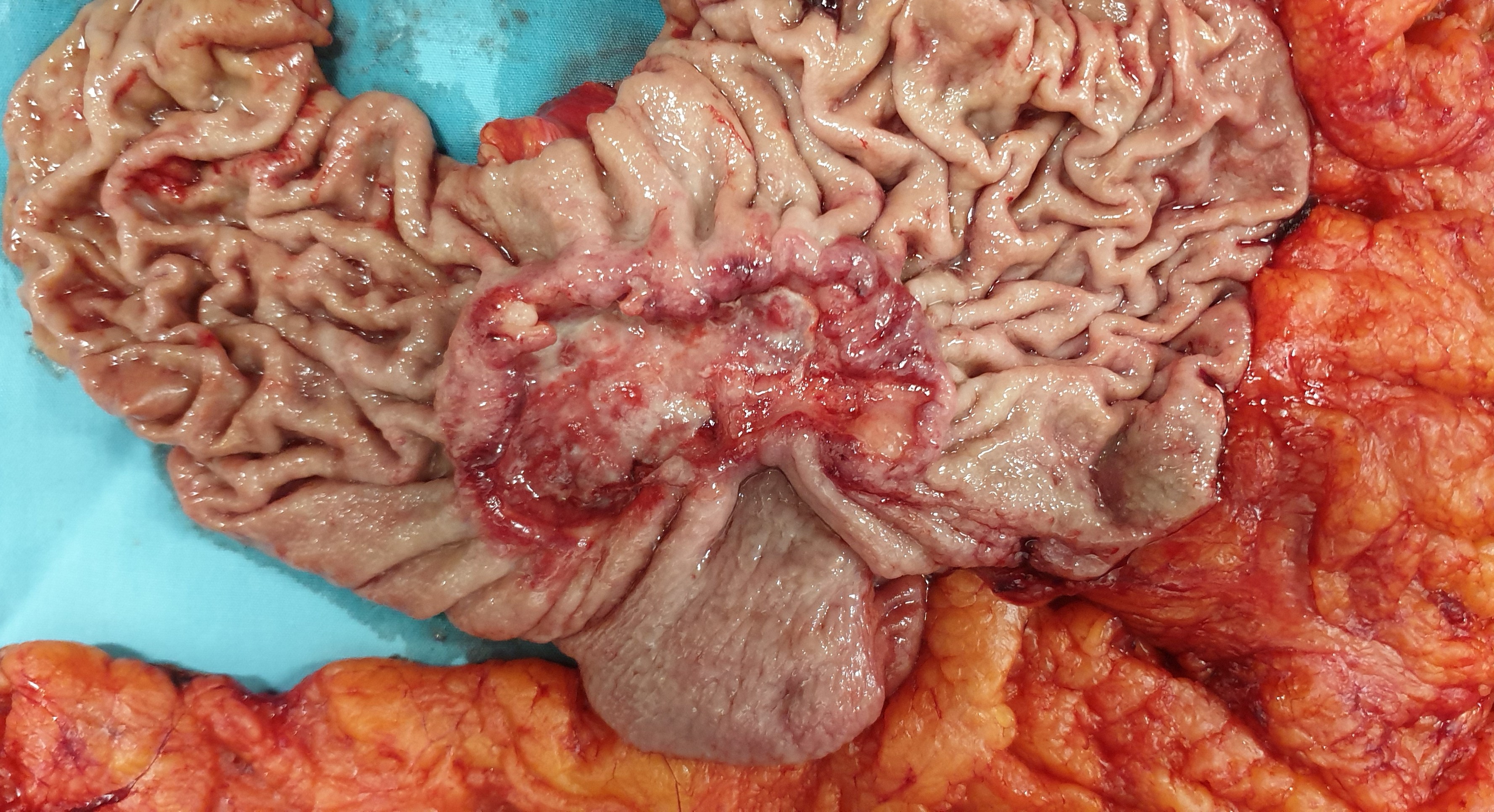
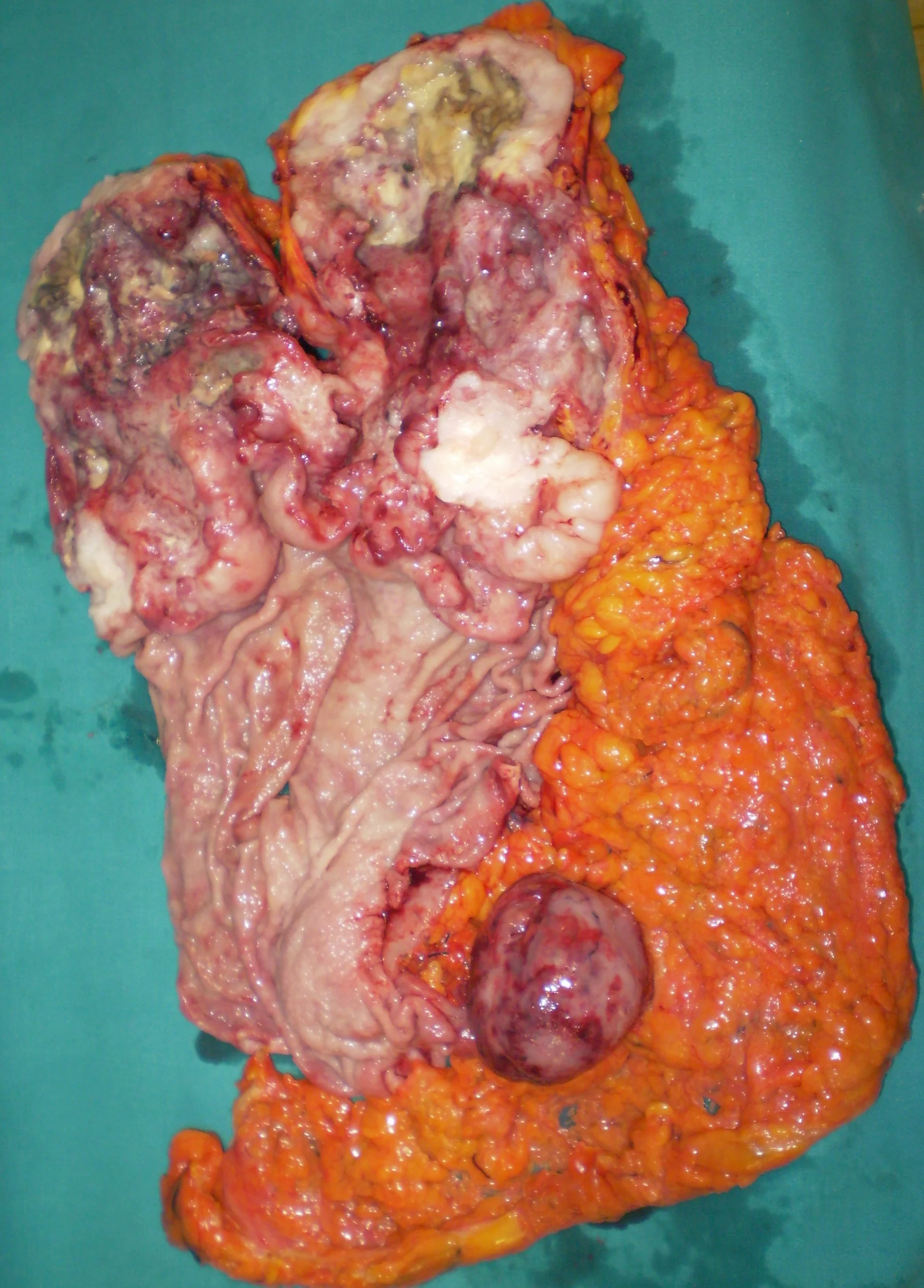
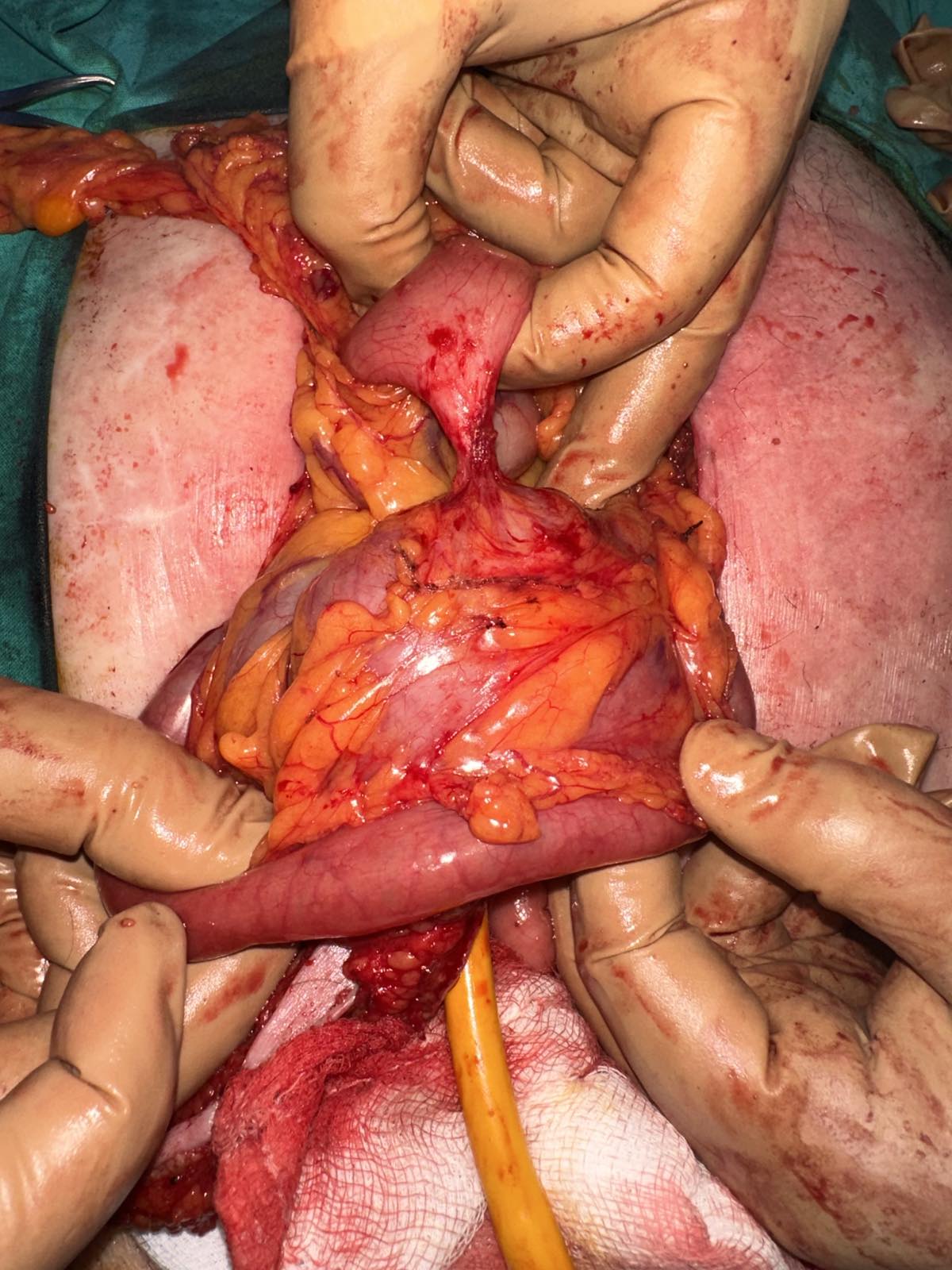
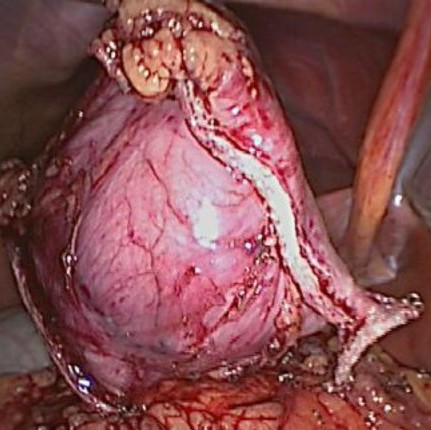
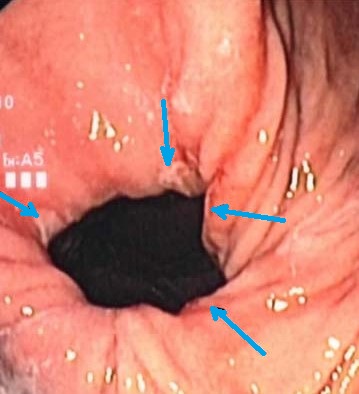
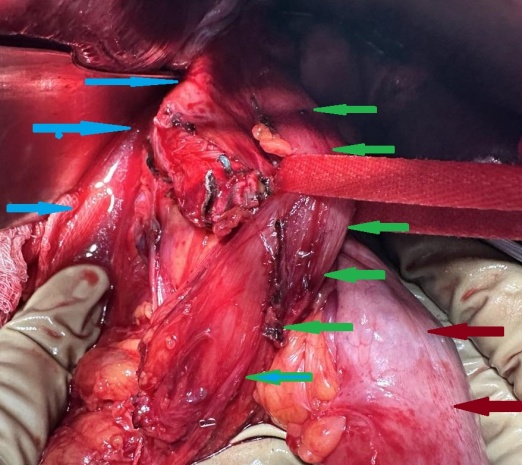
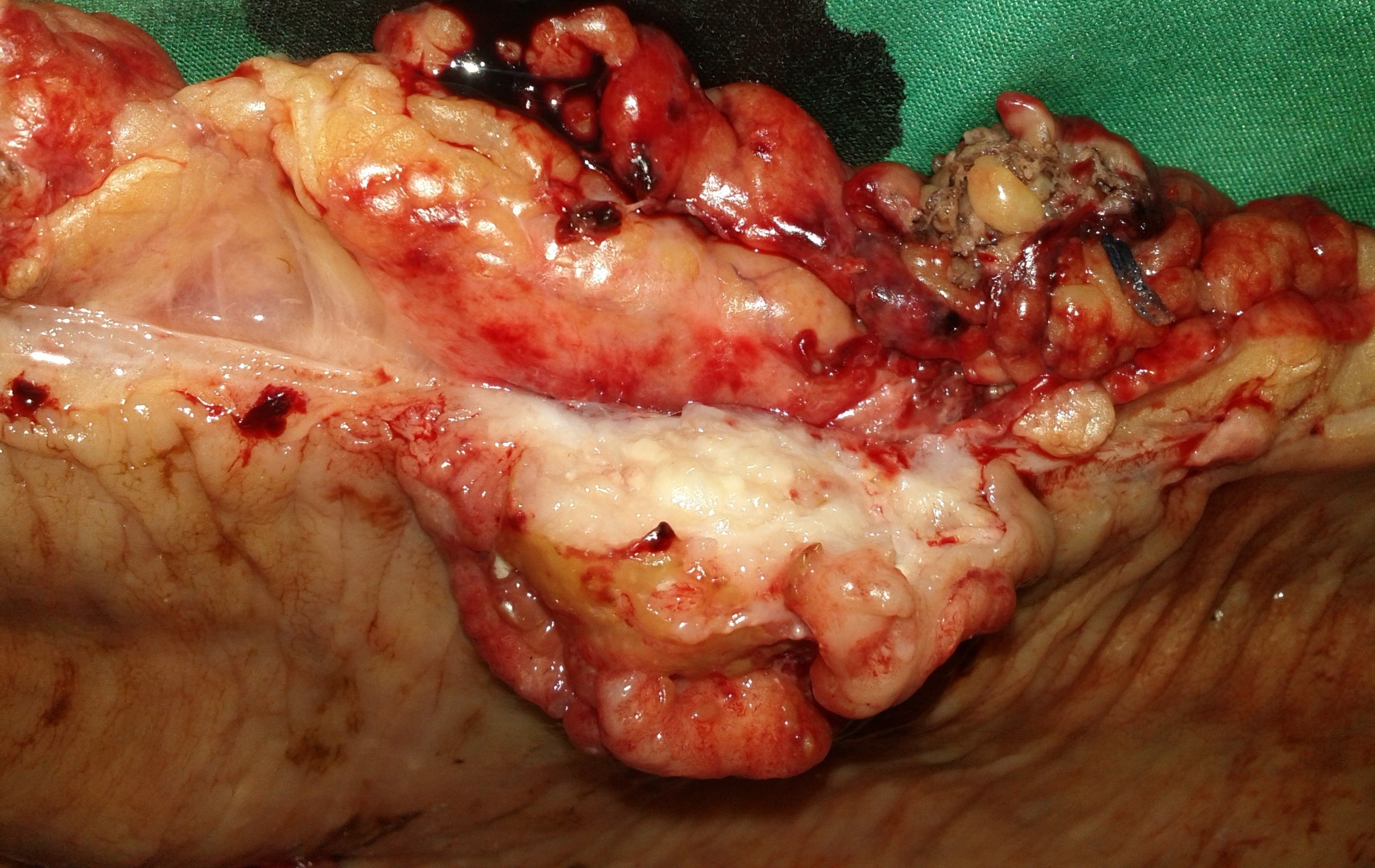
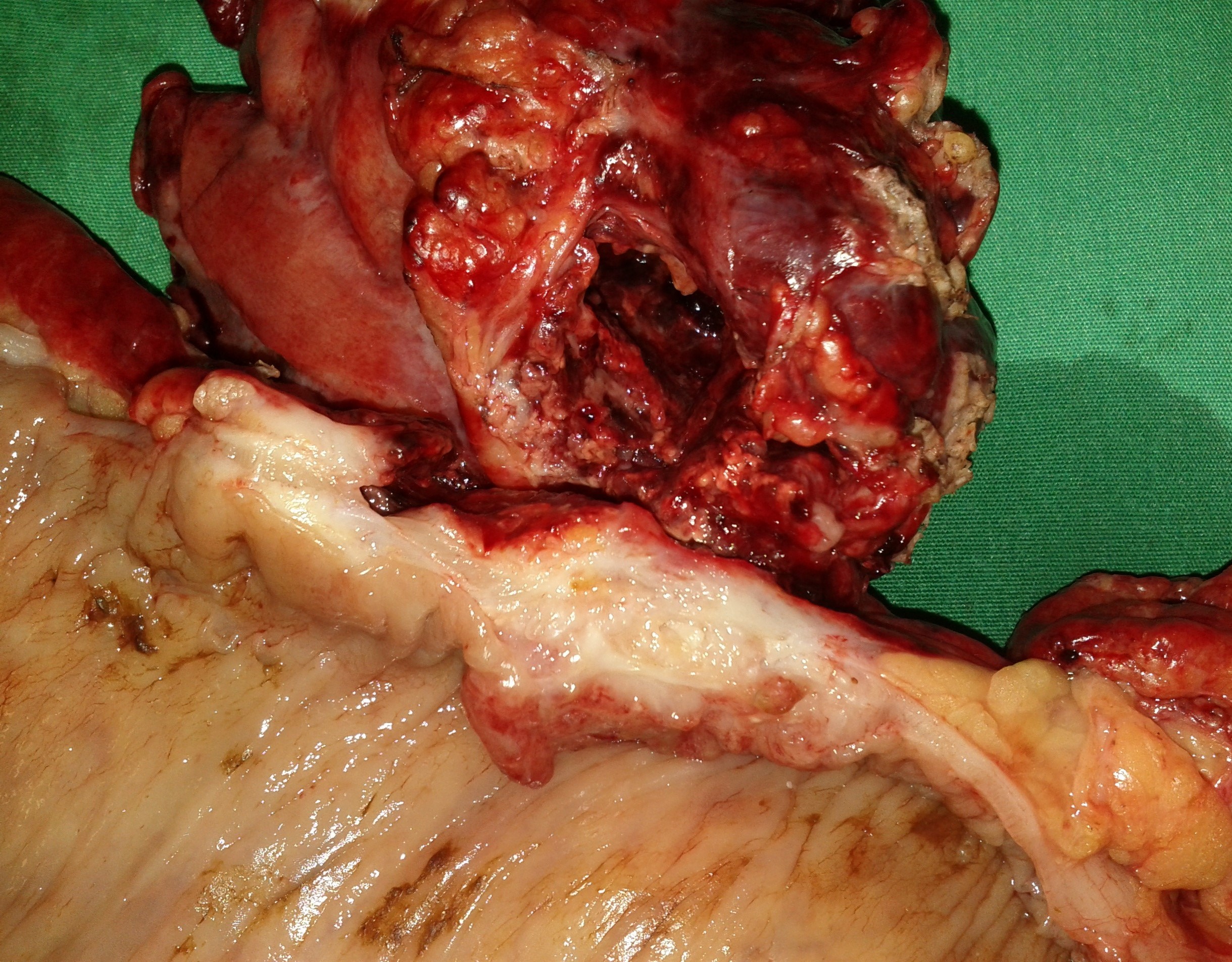
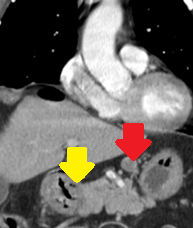
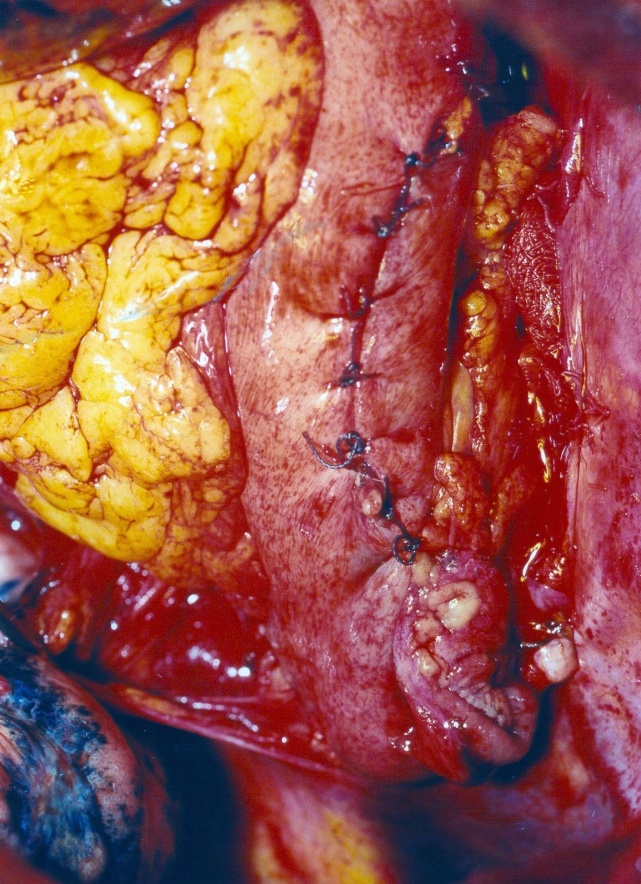
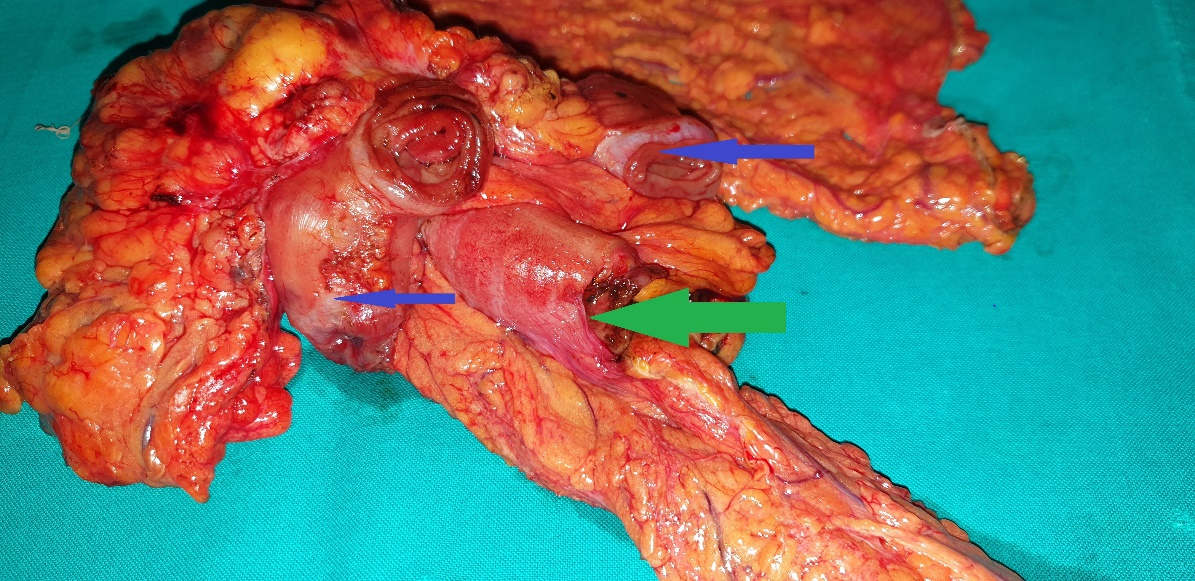
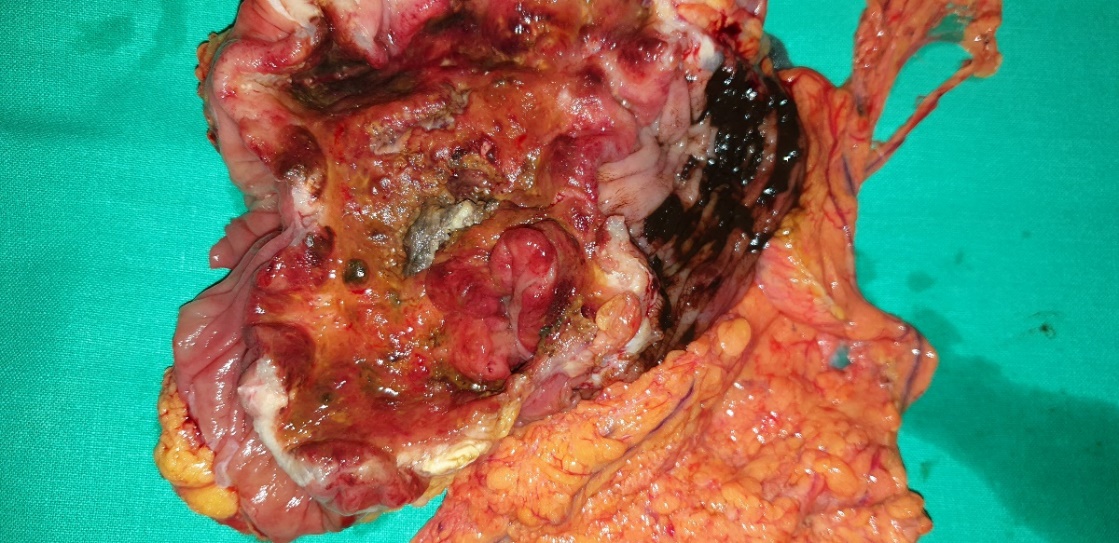
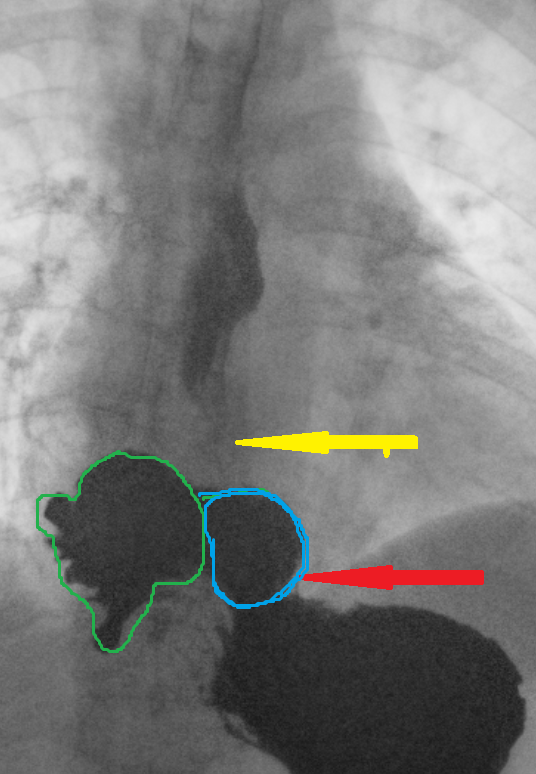
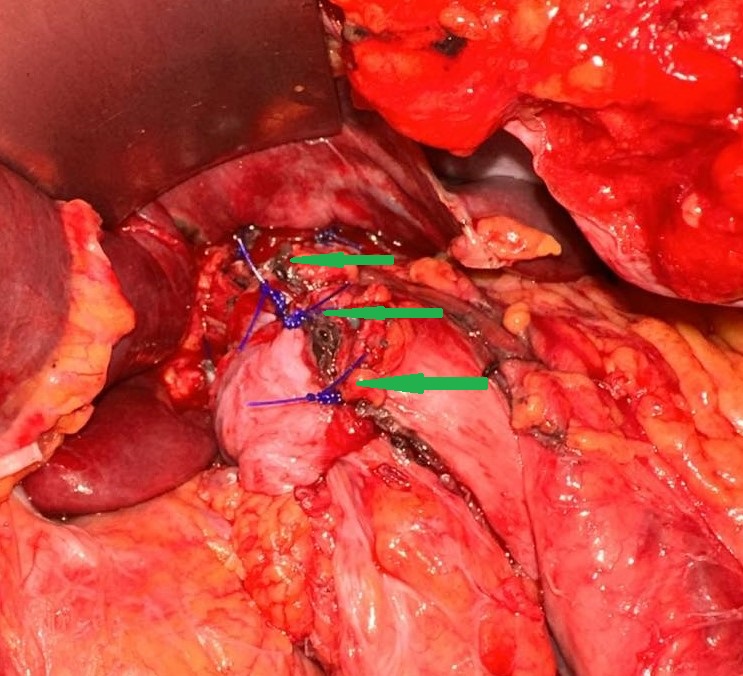
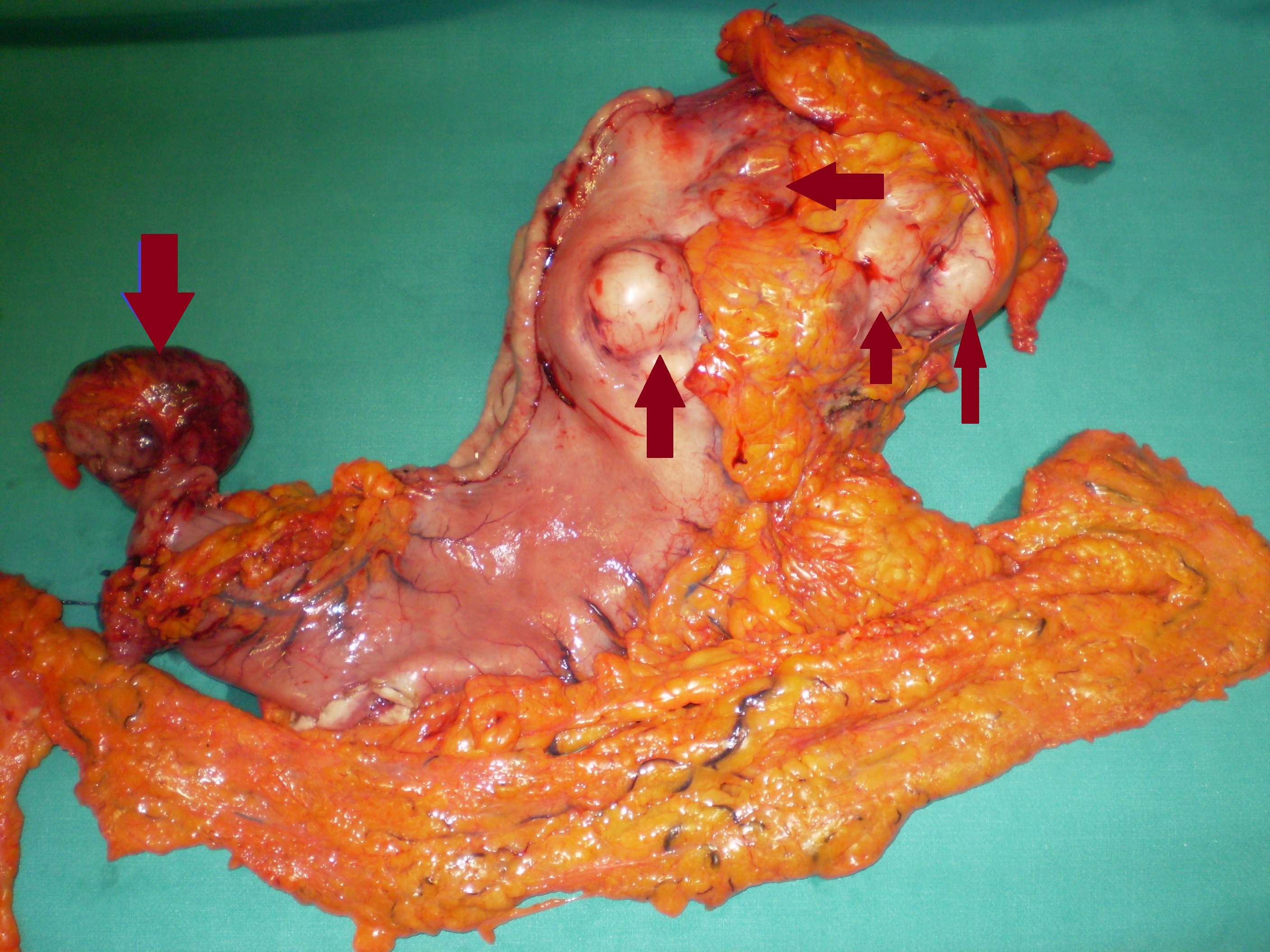
Yellow arrow — Thick-walled gallbladder with gallstones. Blue arrow — Stomach segment. Light blue arrows — Cholecystogastric fistula (Courtesy Dr. V. Penopoulos)
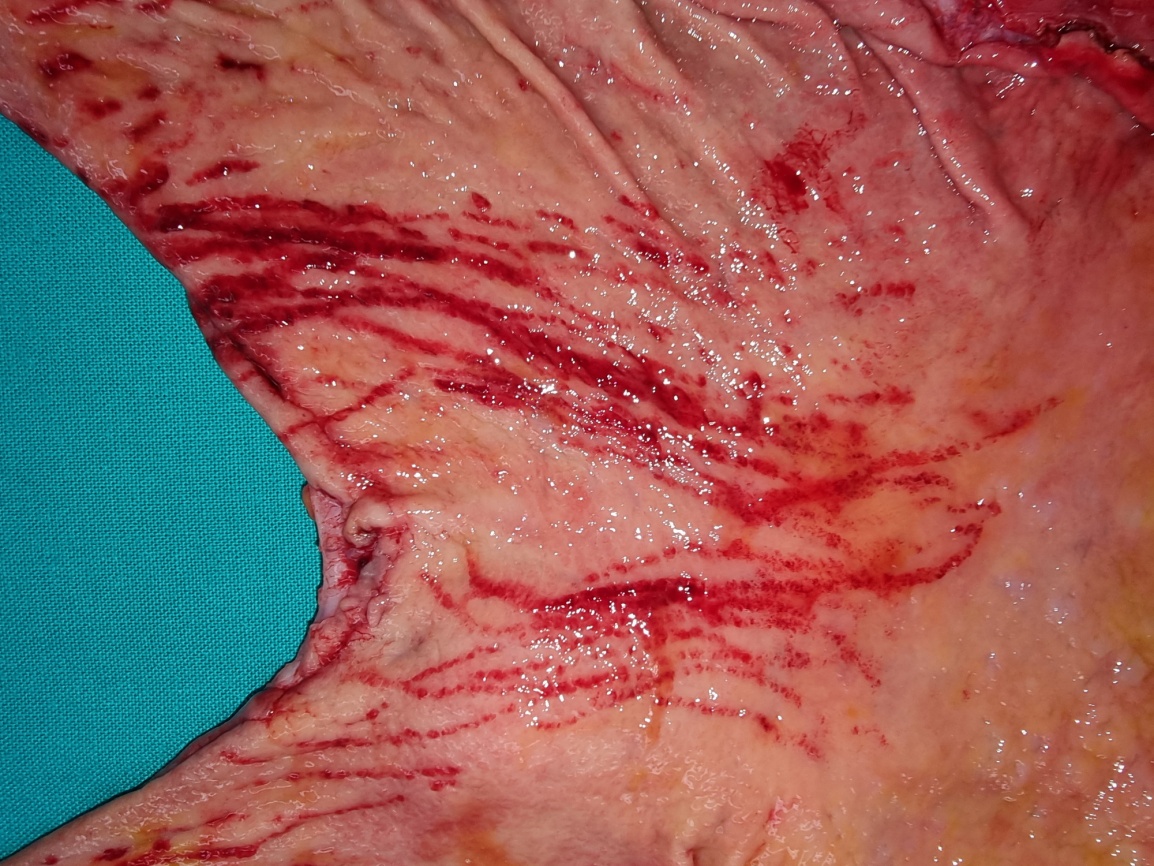
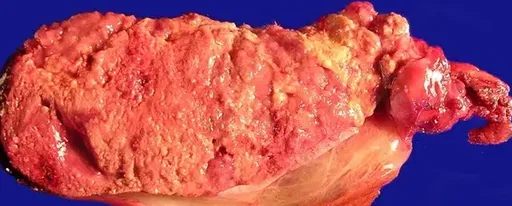
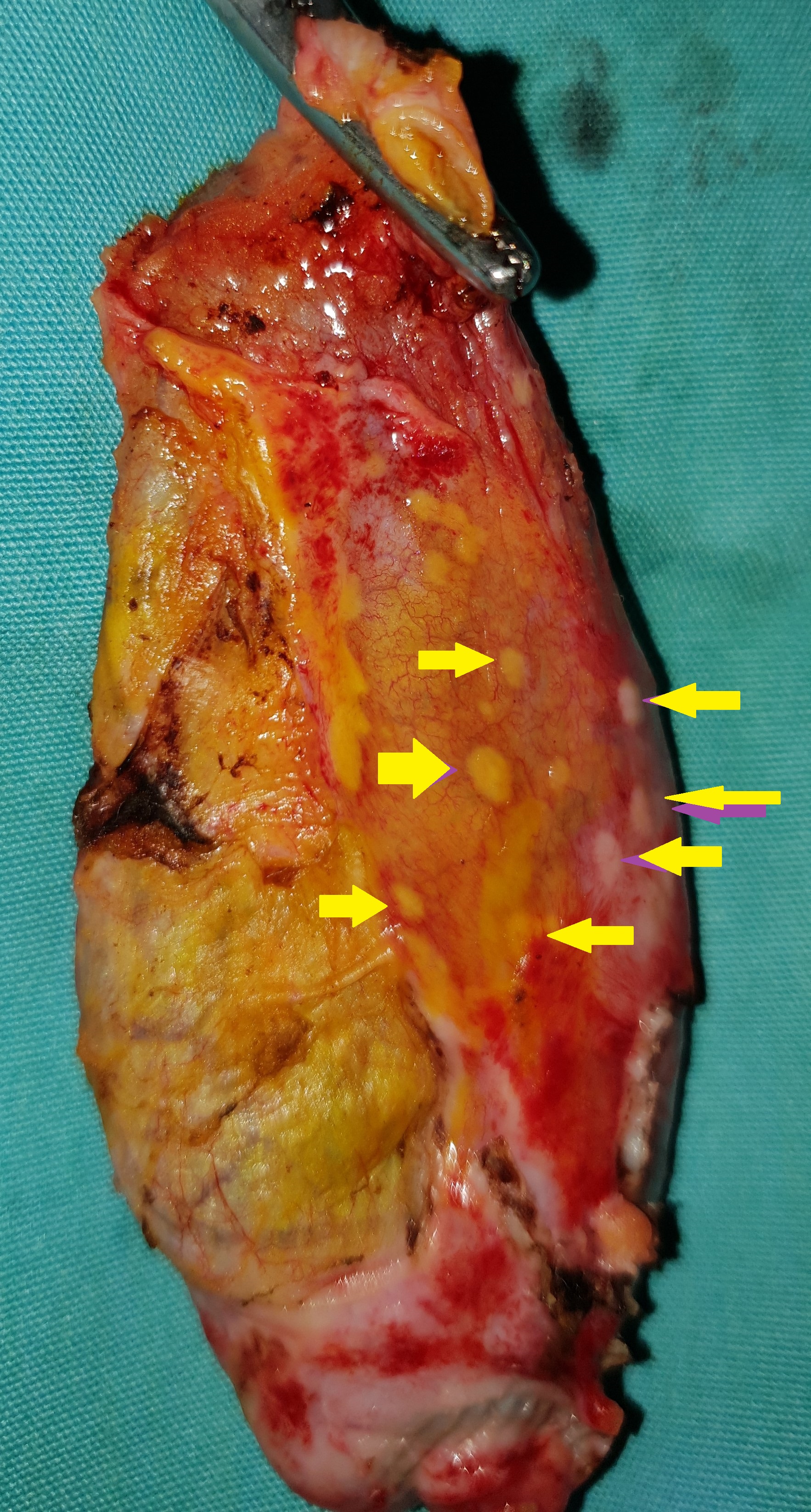
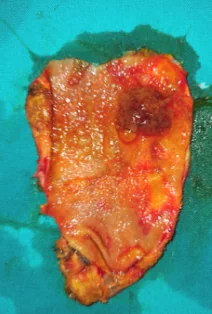
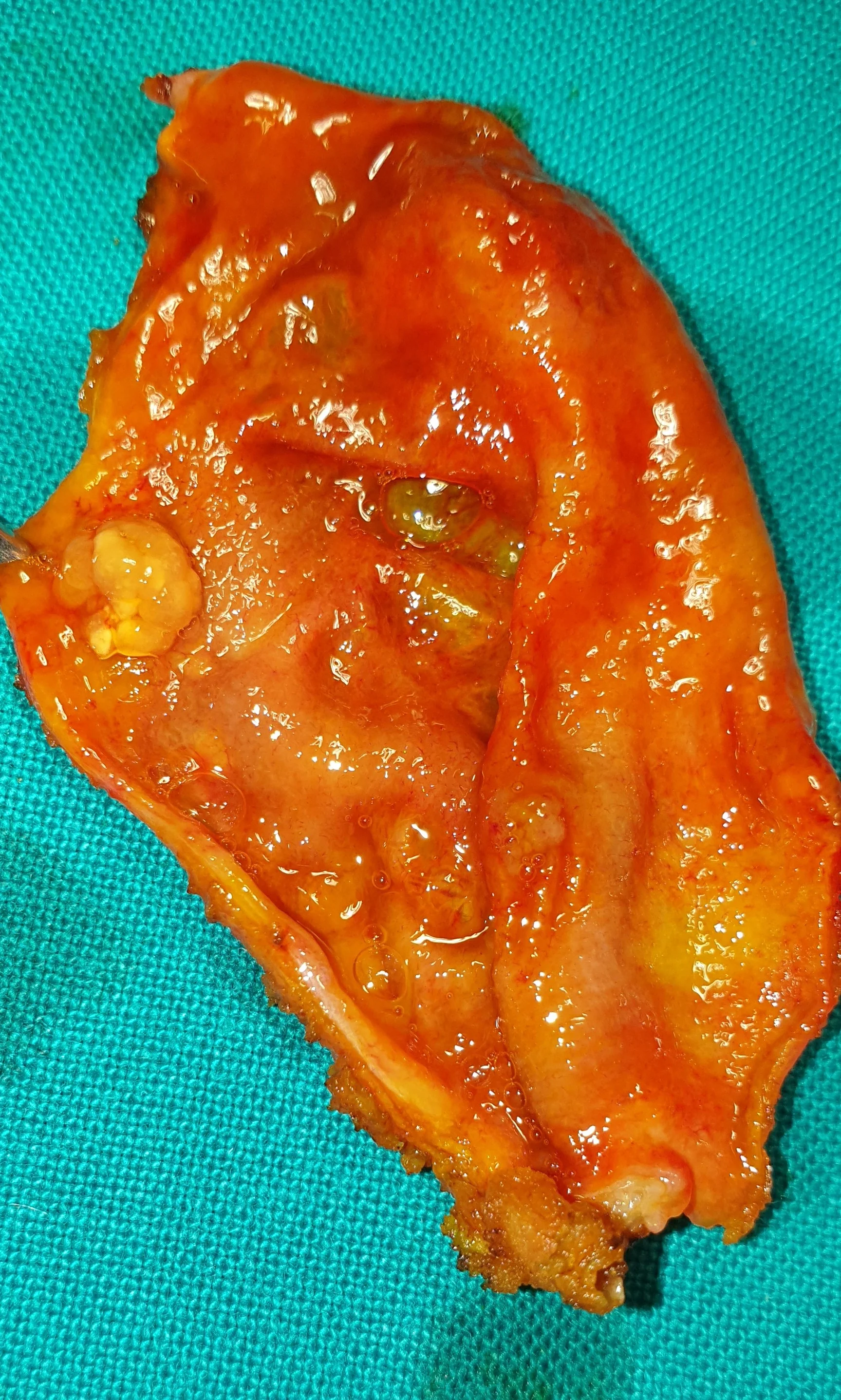
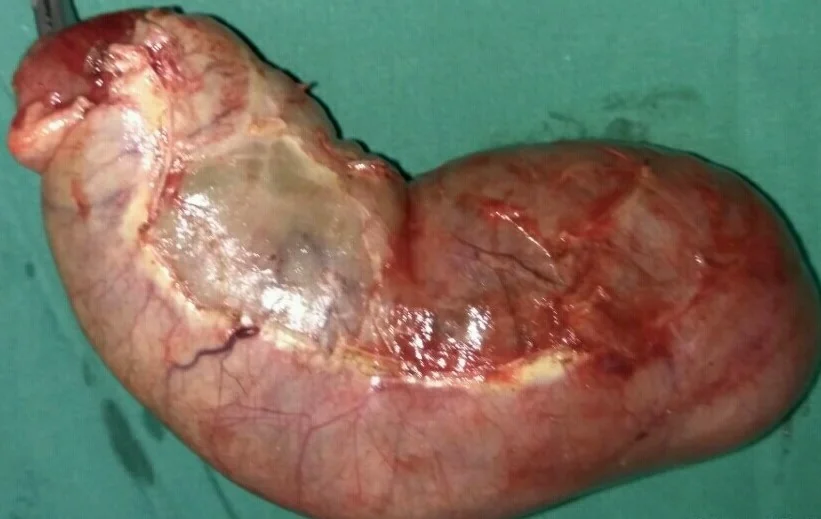
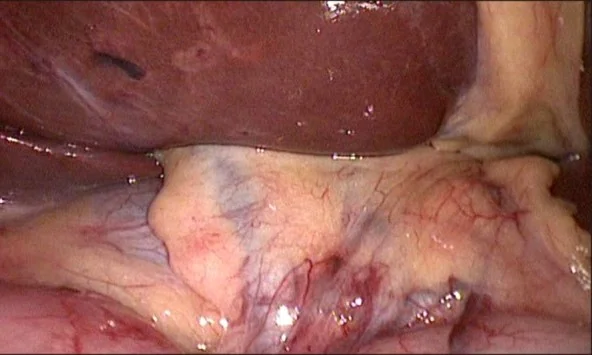
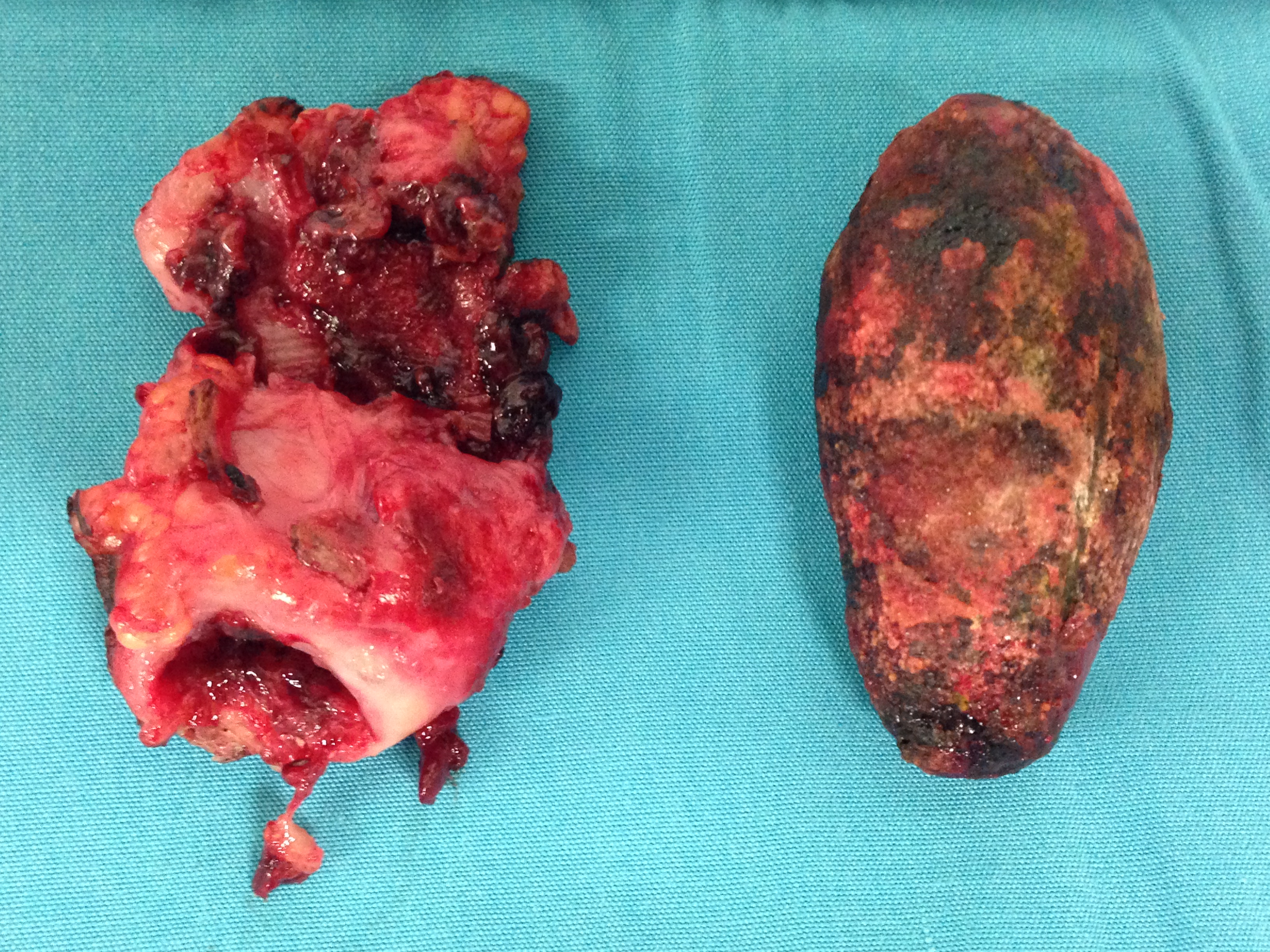
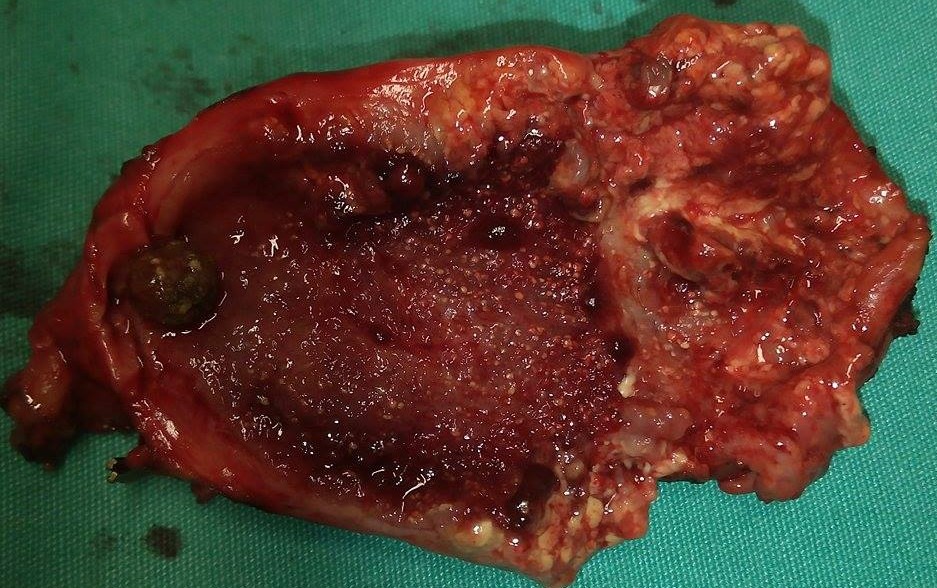
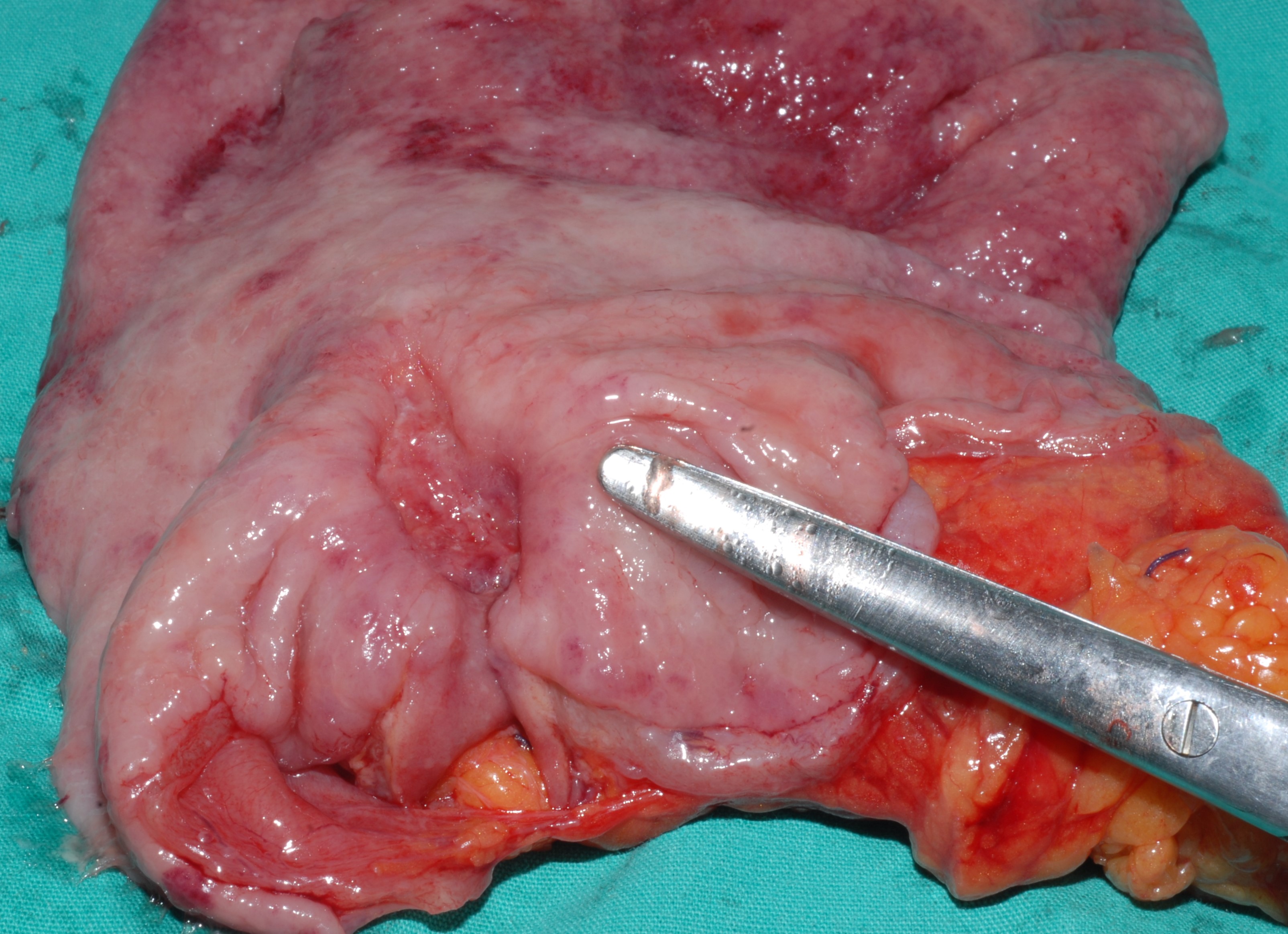
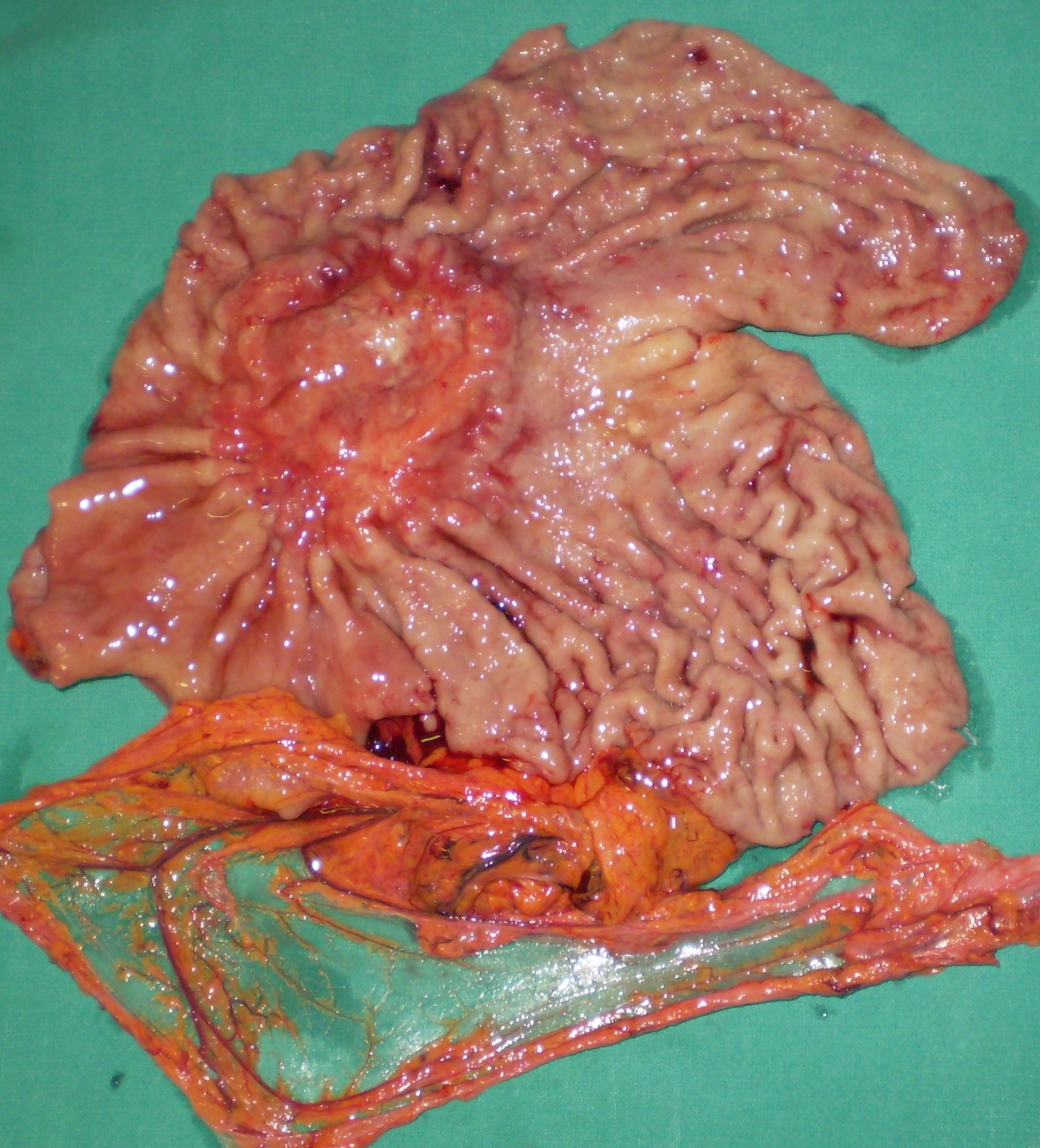
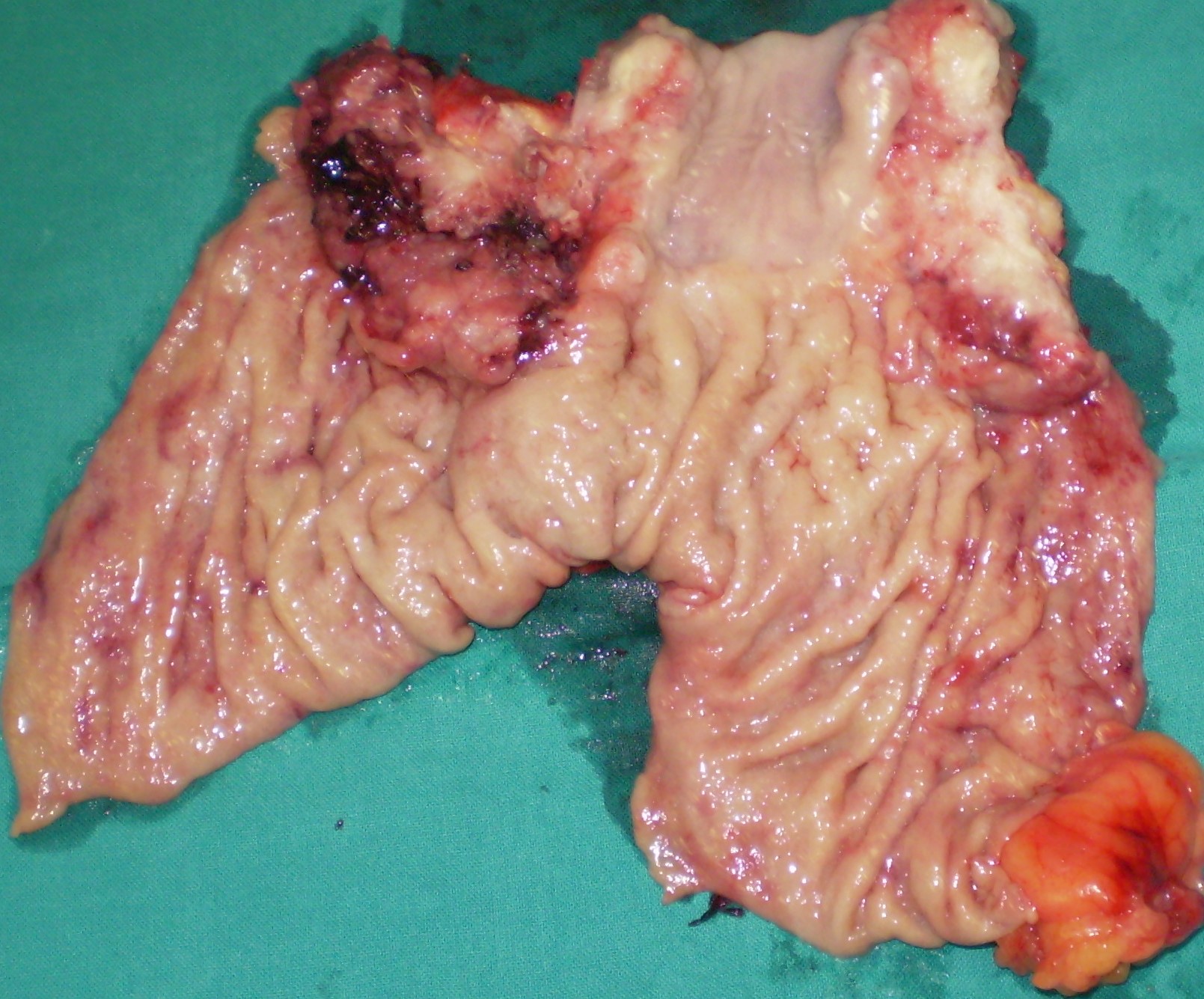
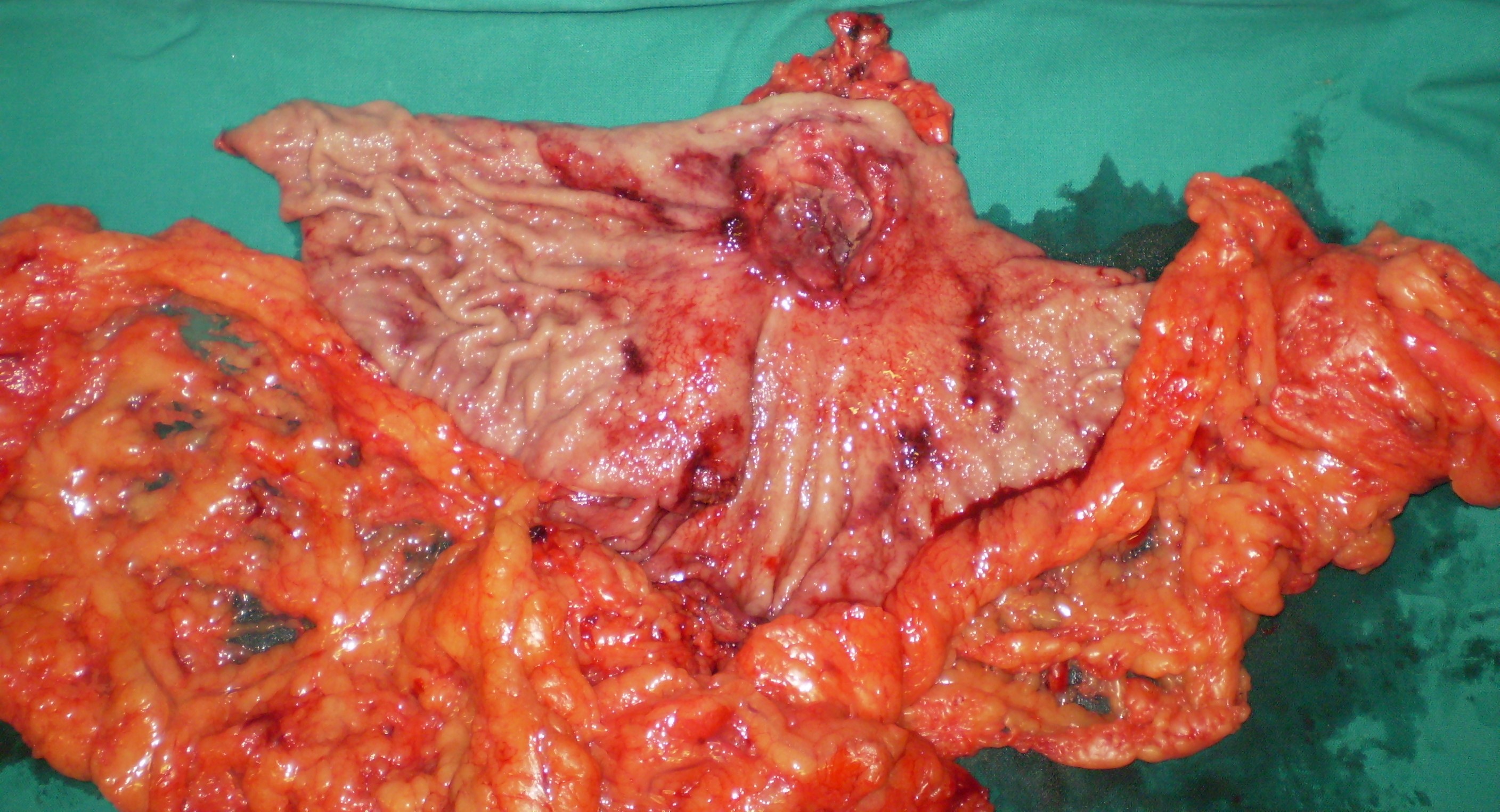
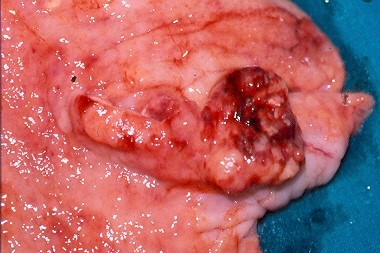
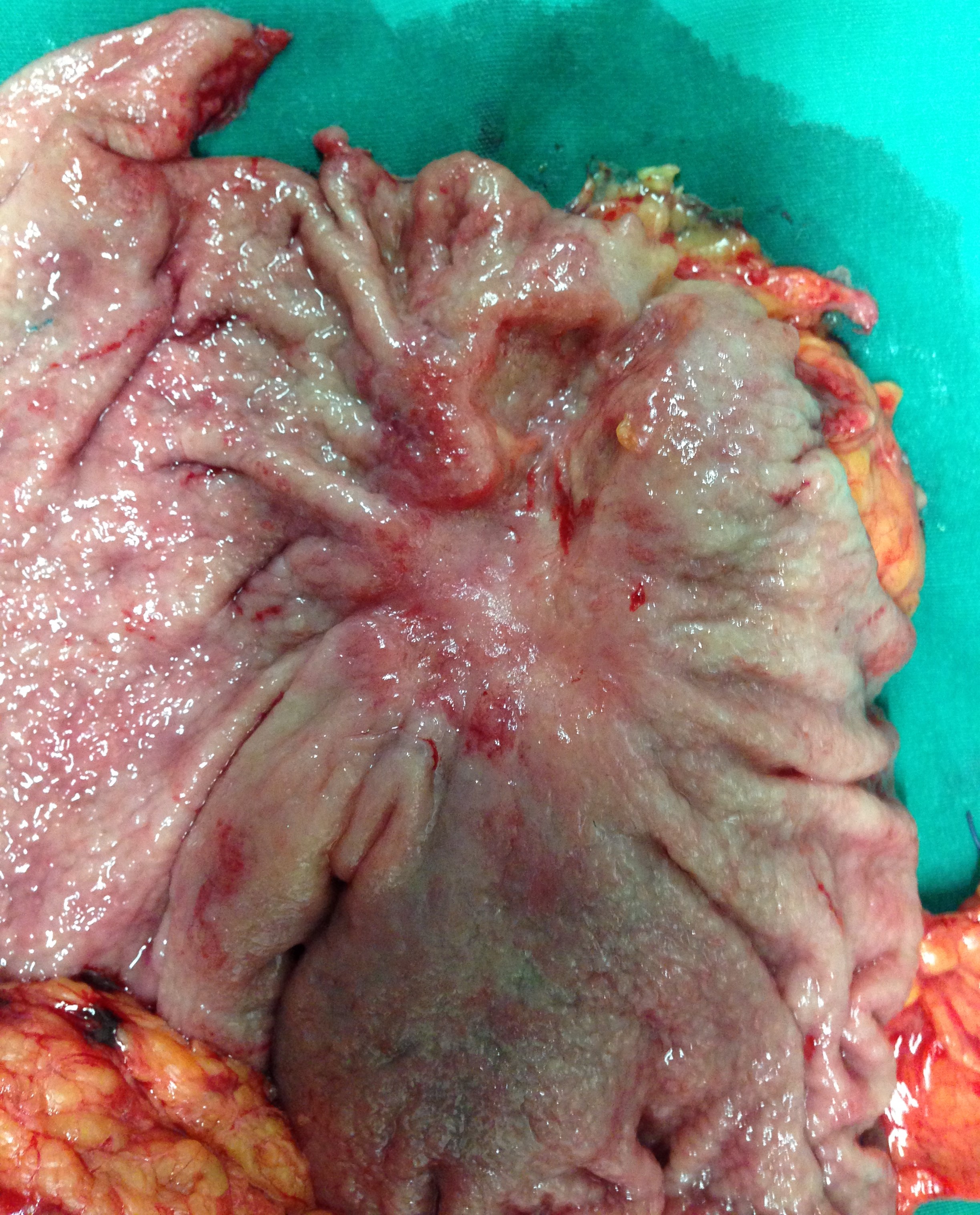
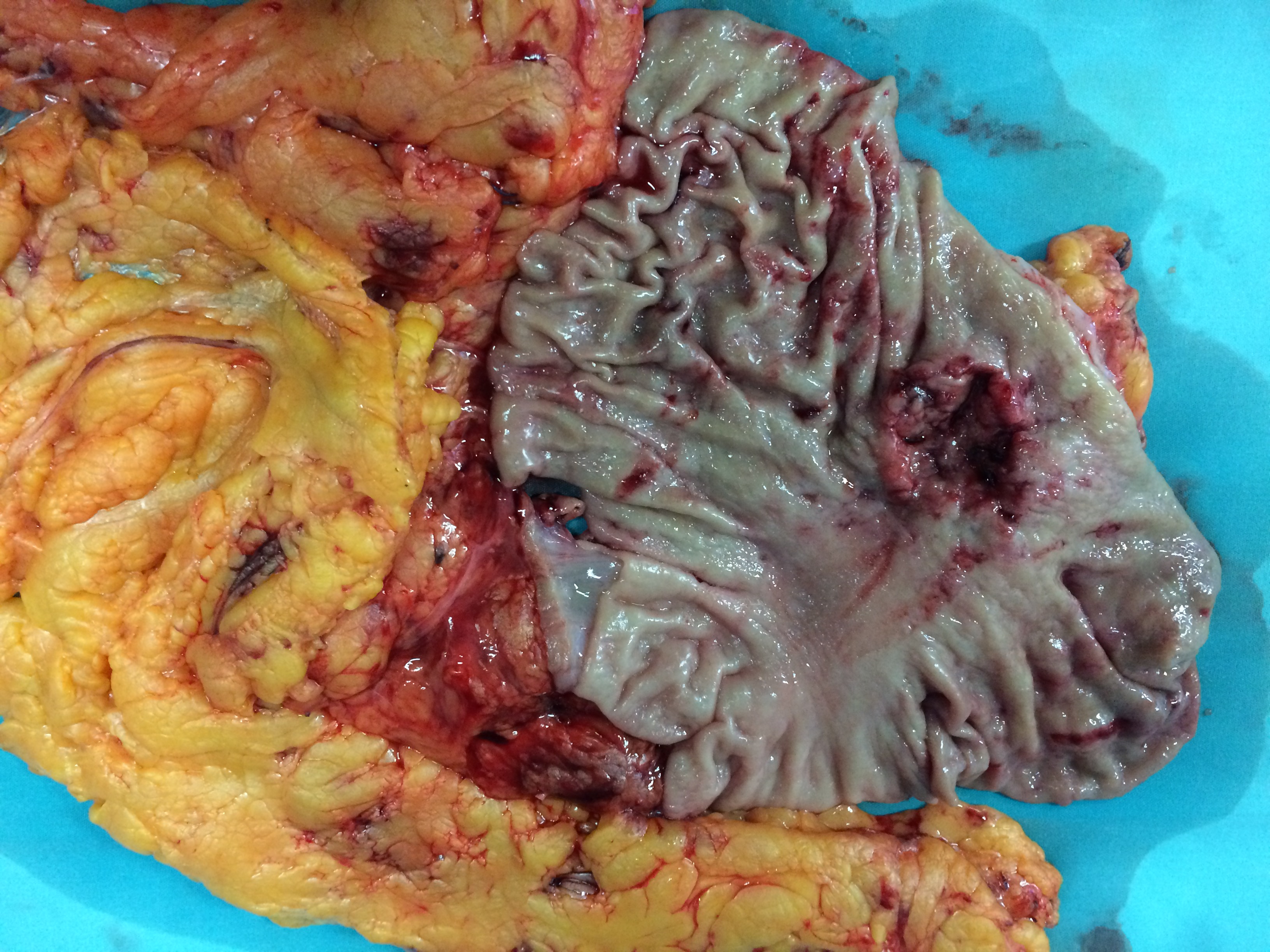
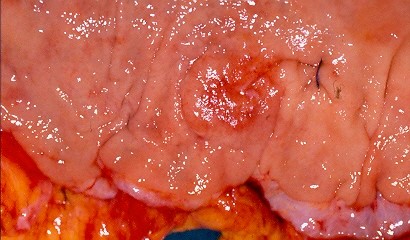
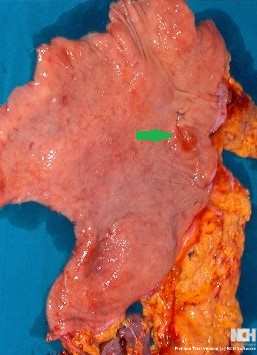
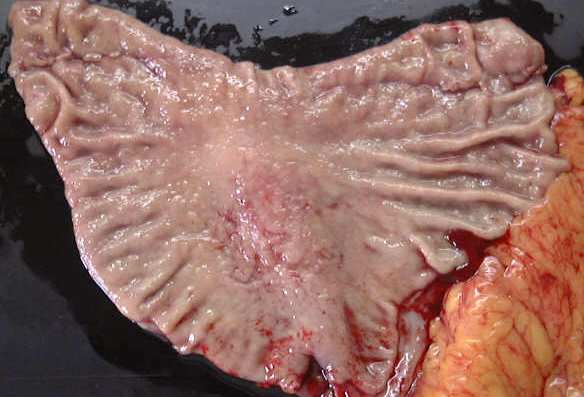
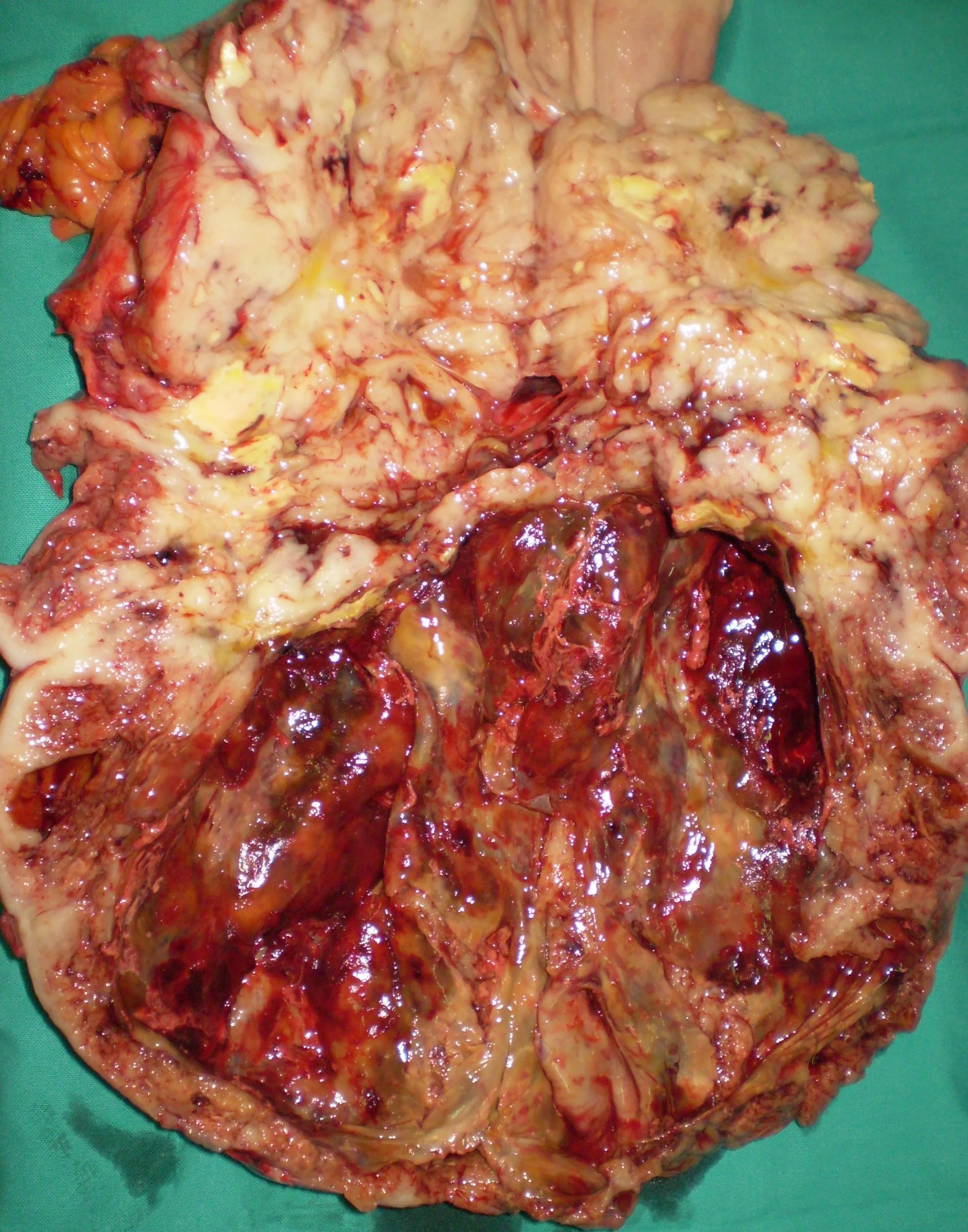
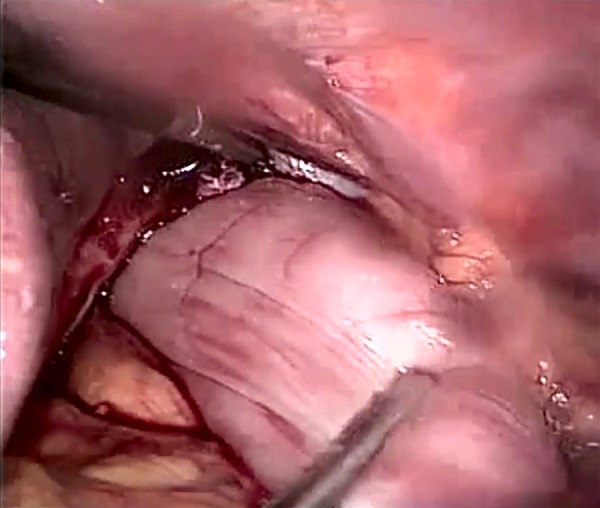
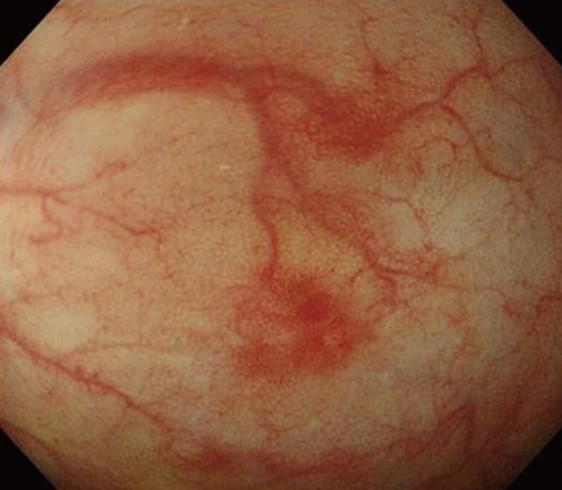
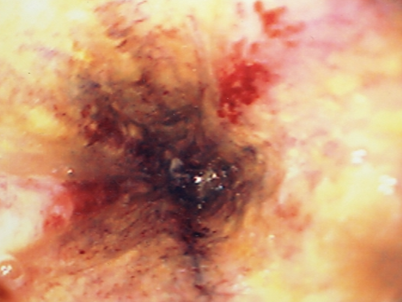
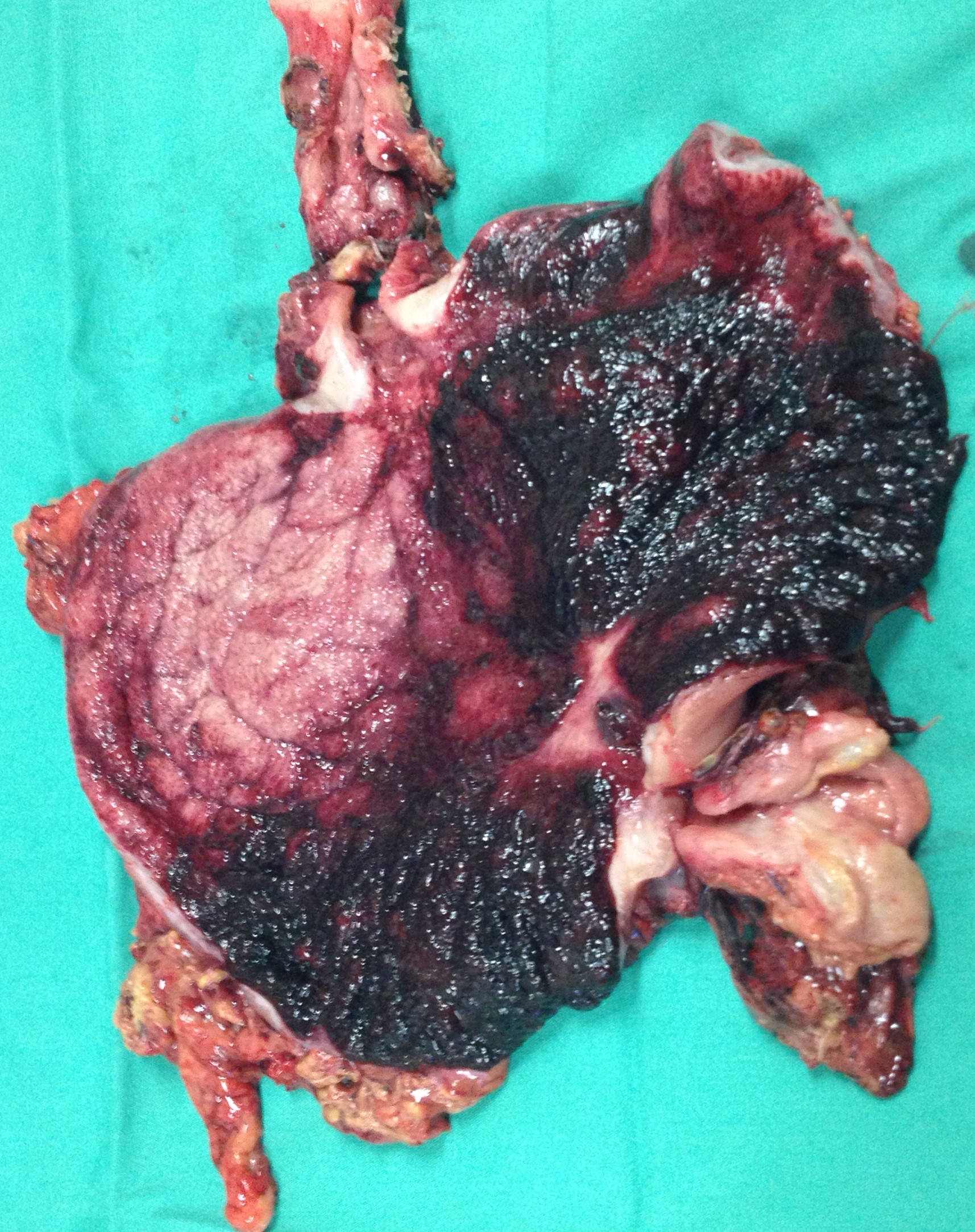
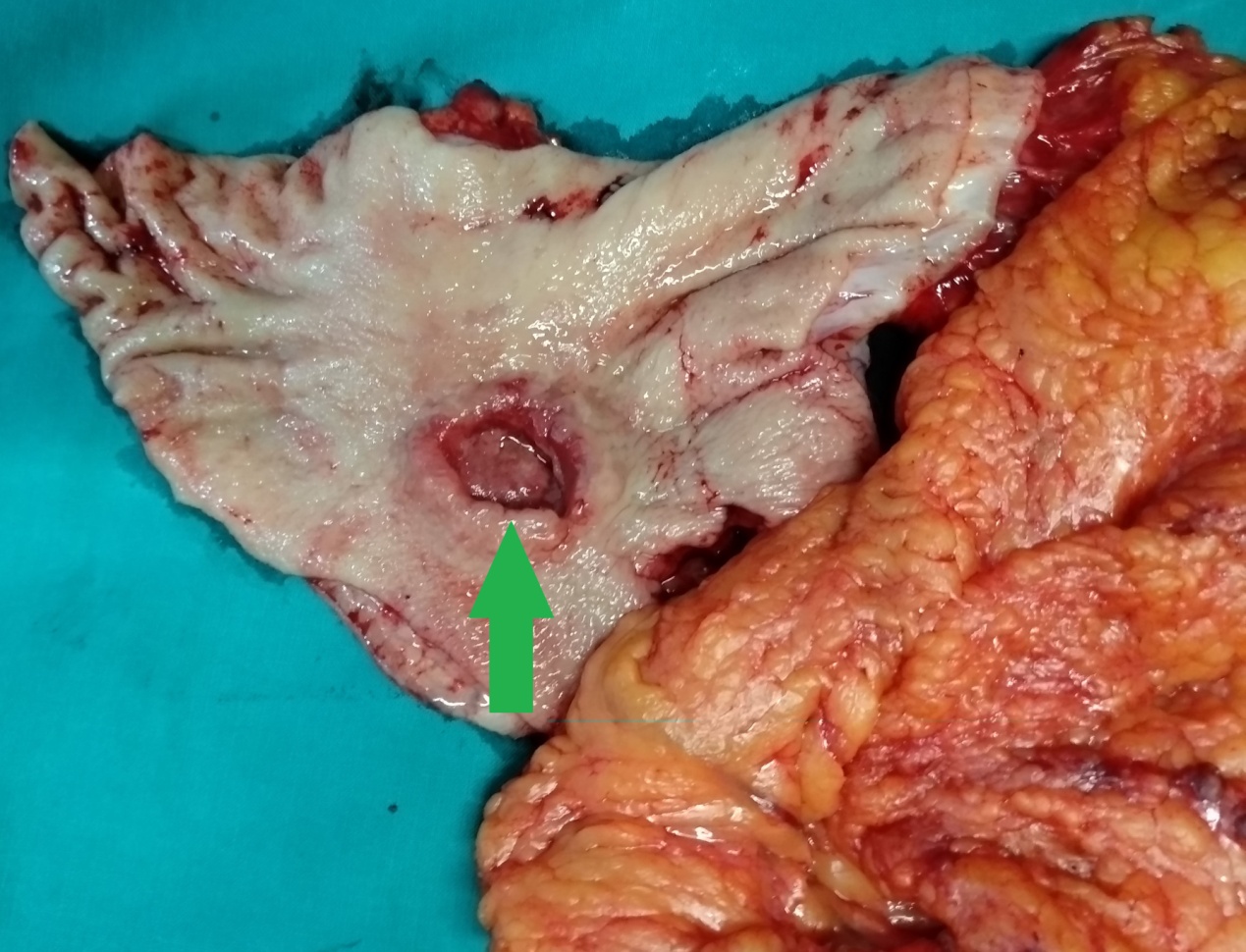
Detail of the lesser curvature of the stomach. Early ischemic changes (Courtesy Dr. V. Penopoulos)

Plain Abdominal X-Rays.Retrocardiac air-filled mass and soft-tissue density mass in the upper abdomen. (Courtesy Dr.V.Penopoulos).


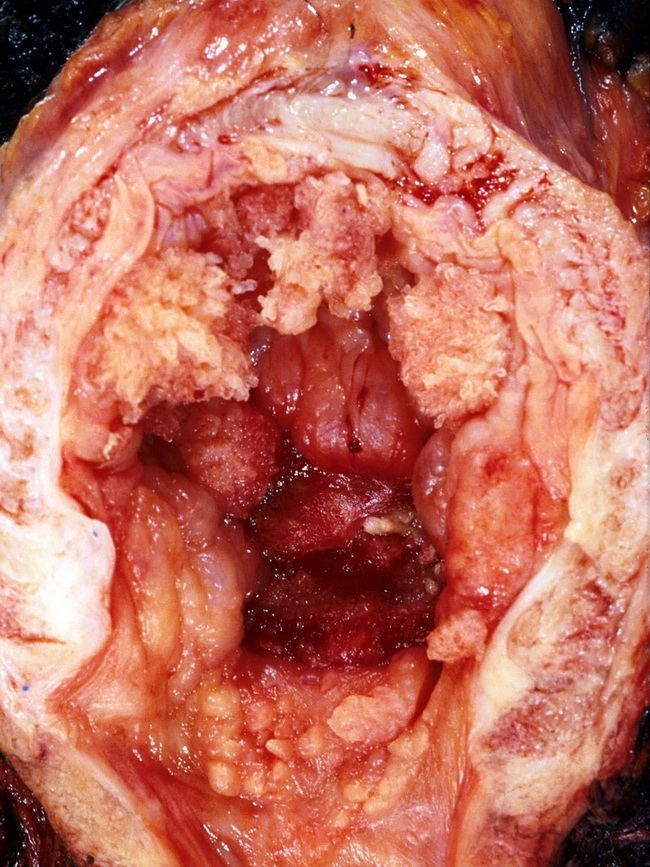
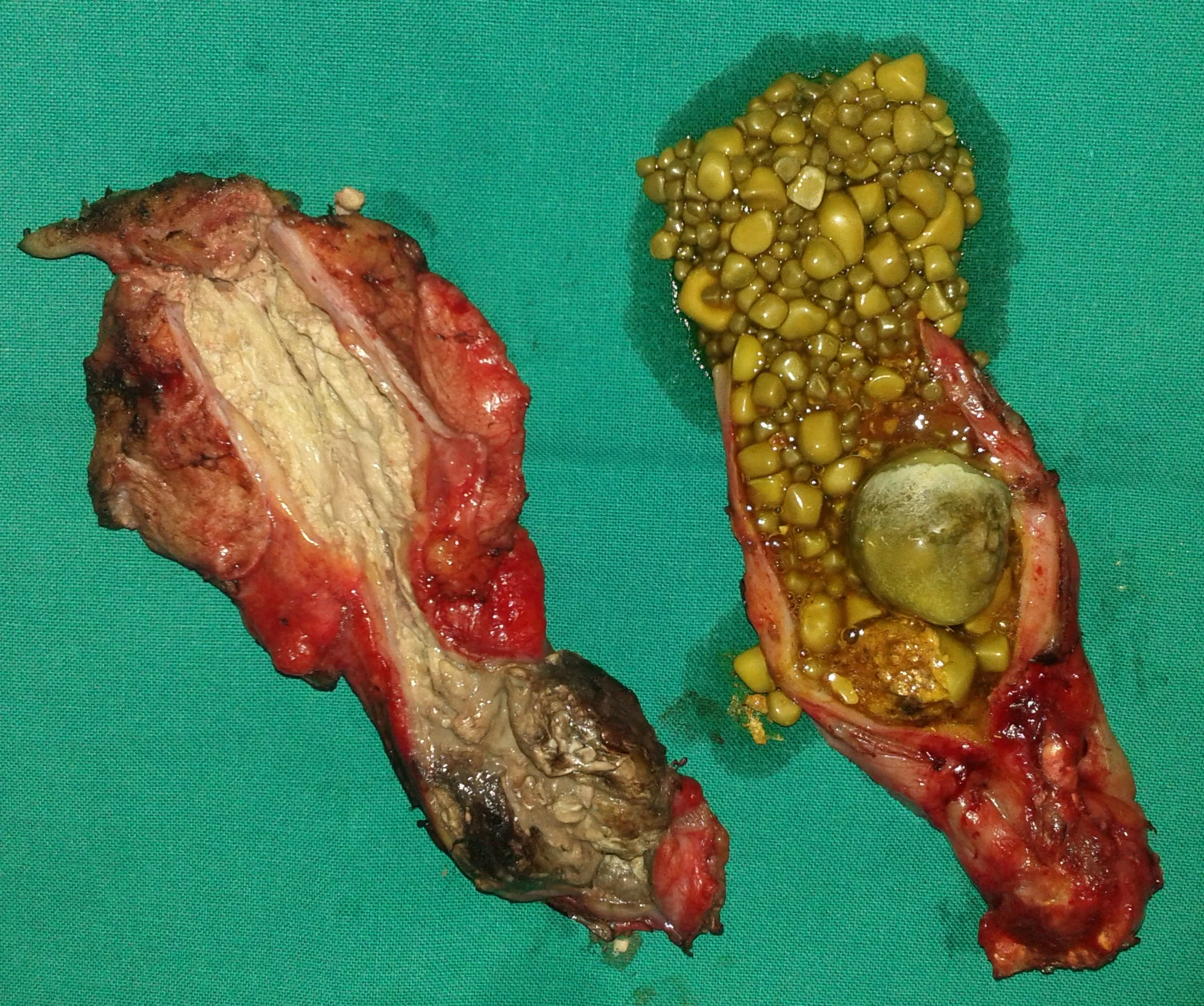
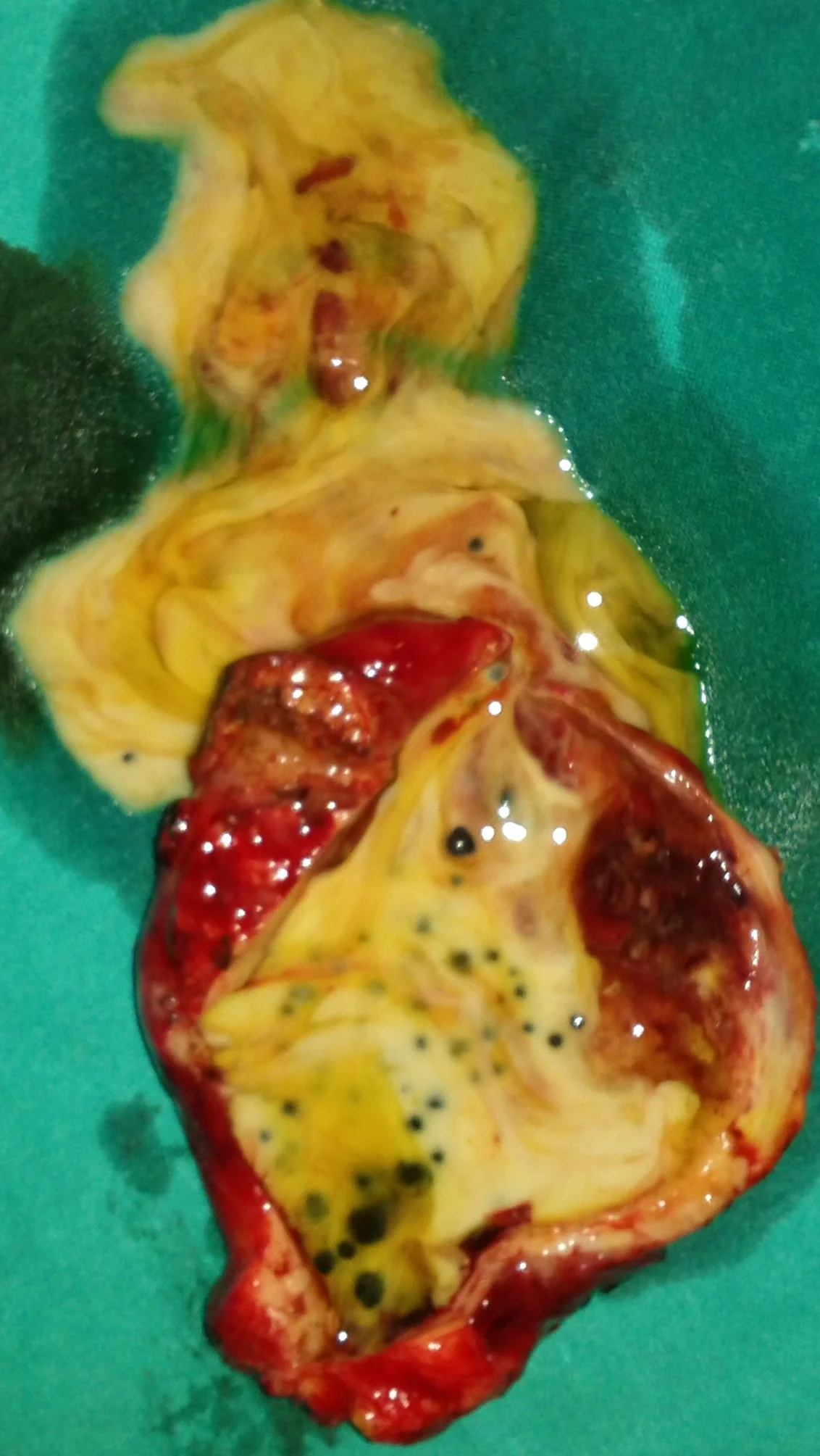
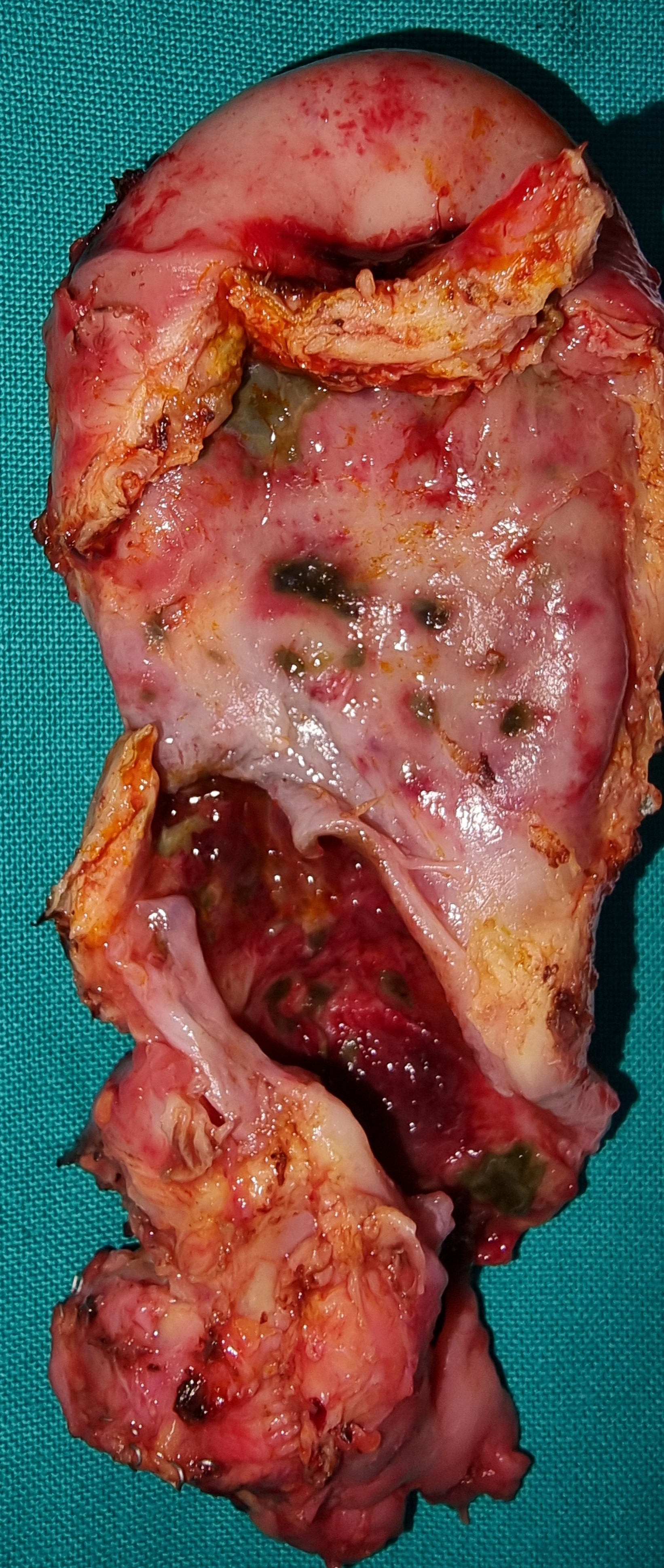
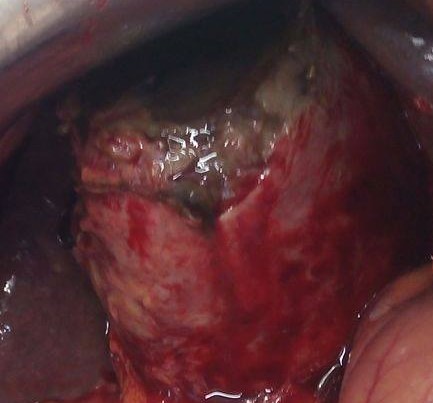
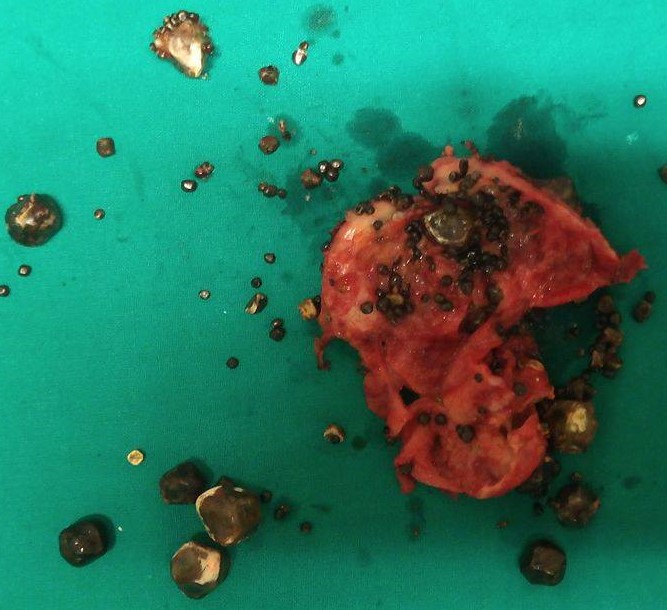
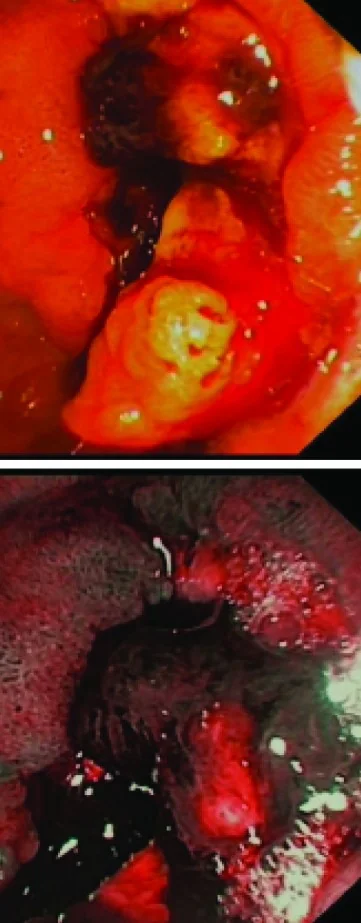
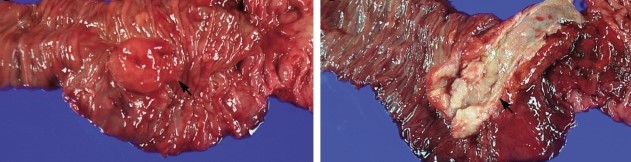
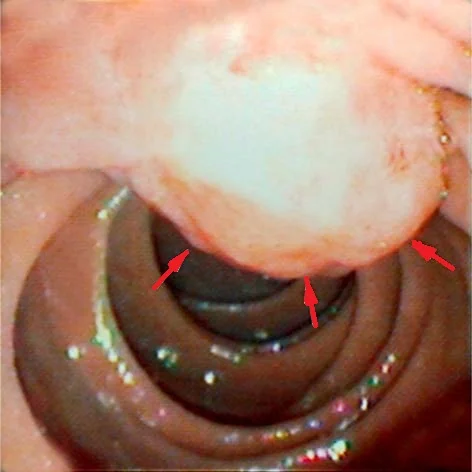
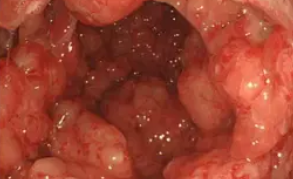
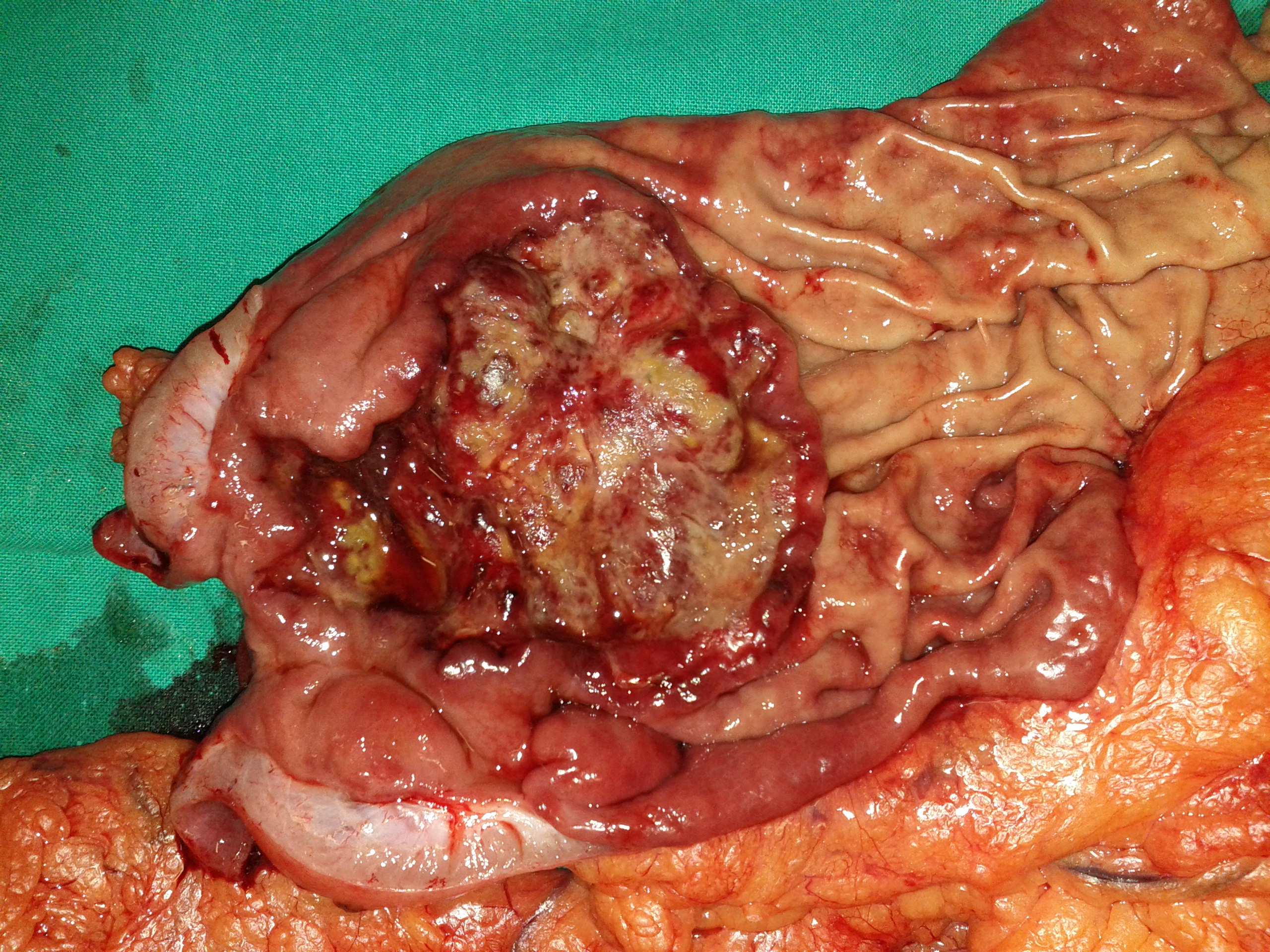
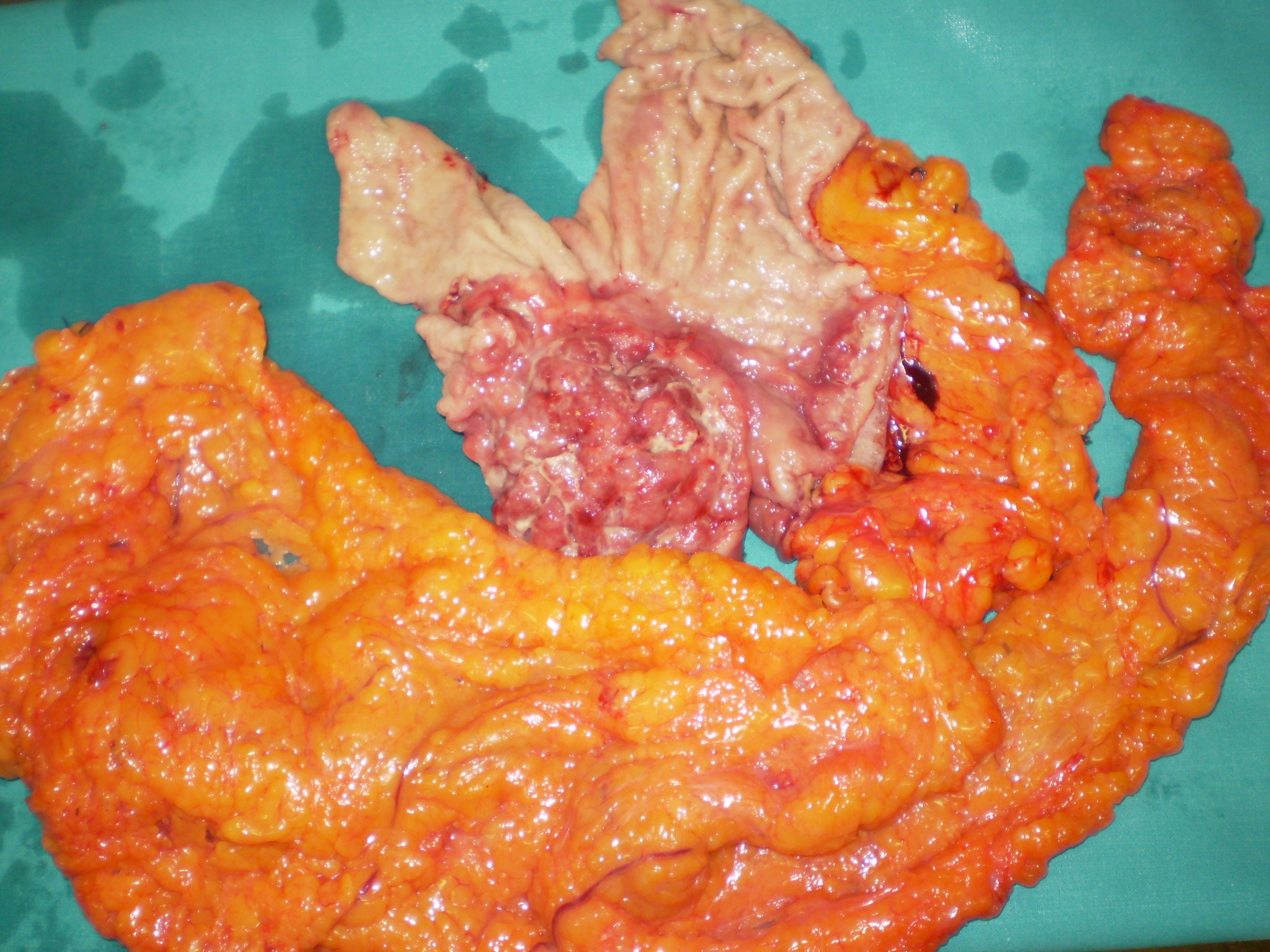
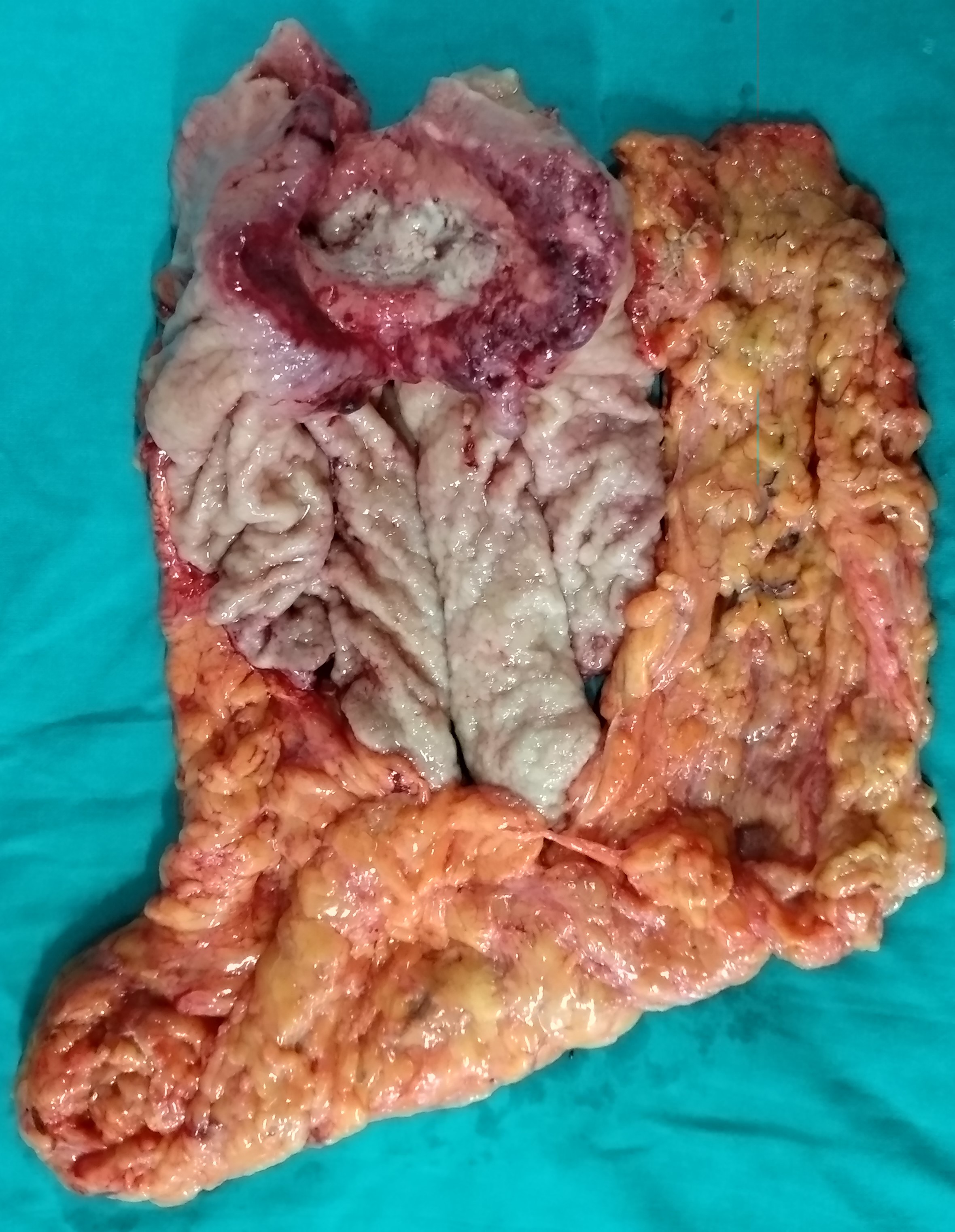
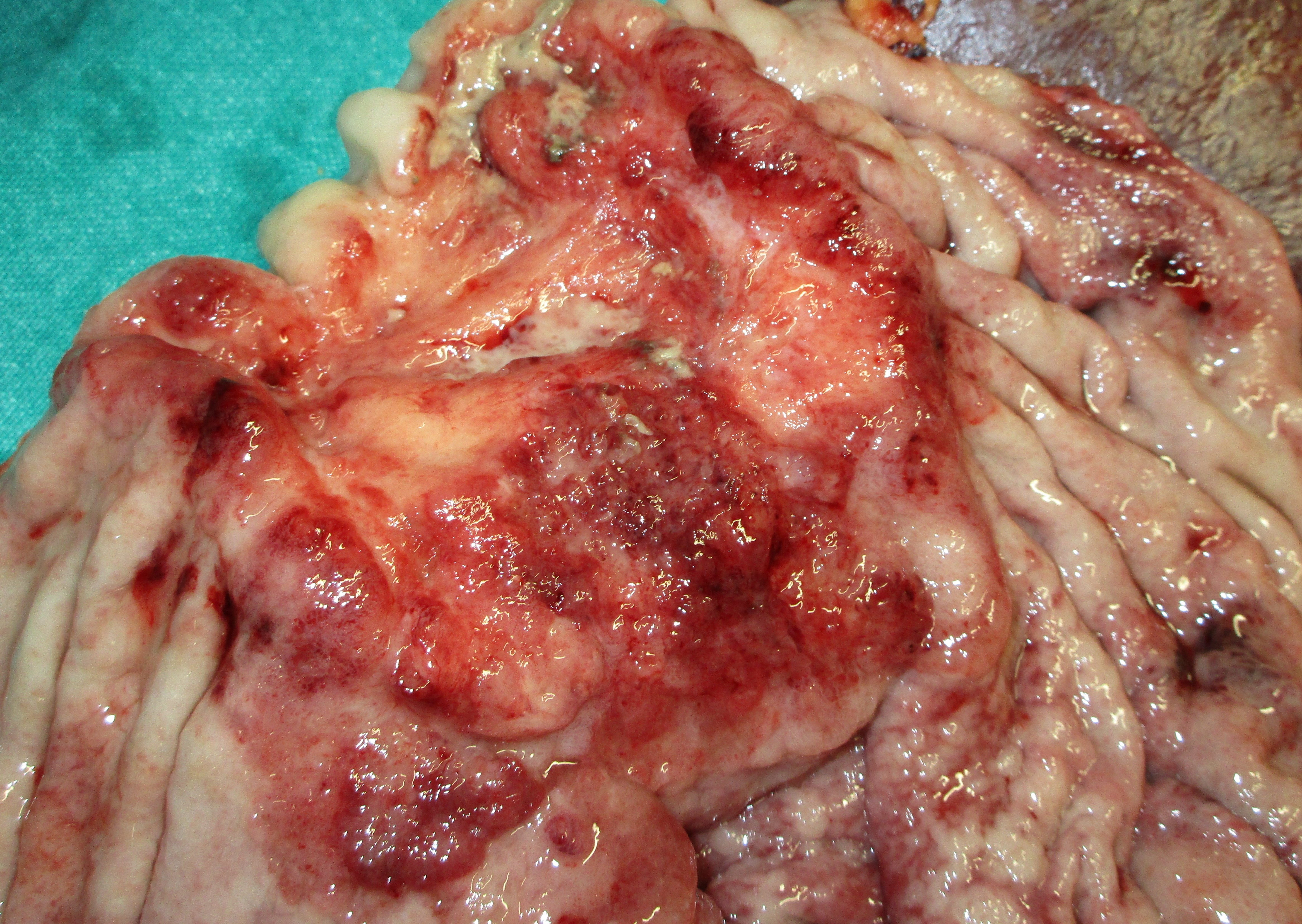
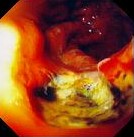
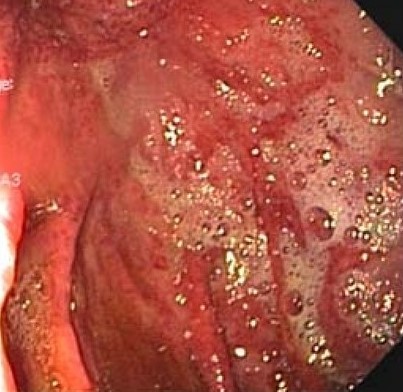
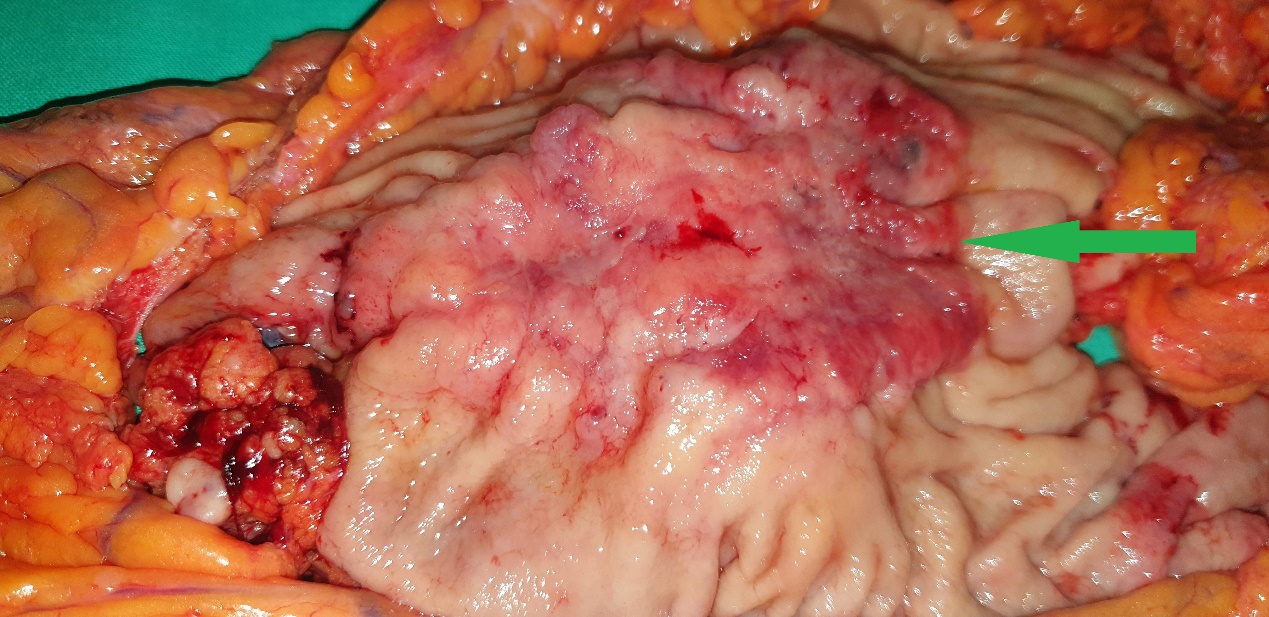
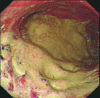
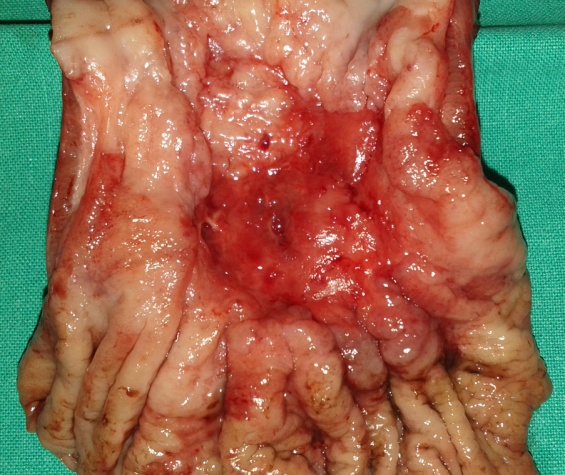
Extreme stenosis of the involved transverse colon . Residual seeds were unable to overcome the stenotic segment (Courtesy Dr. V. Penopoulos)

Bluish discoloration of toes suggestive of microangiopathic hemolytic anemia.(Courtesy Dr.V.Penopoulos).

Skin changes right foot suggestive of microangiopathic hemolytic anemia.(Courtesy Dr.V.Penopoulos).

Retrocardiac air-filled mass and soft-tissue density mass in the upper abdomen. (Courtesy Dr.V.Penopoulos).
Gastrografin swallow. Esophago-gastric anastomosis in right hemithorax. (Courtesy Dr.V.Penopoulos).
Postoperative stricture development at the esophagogastric anastomosis (Courtesy Dr. V. Penopoulos)
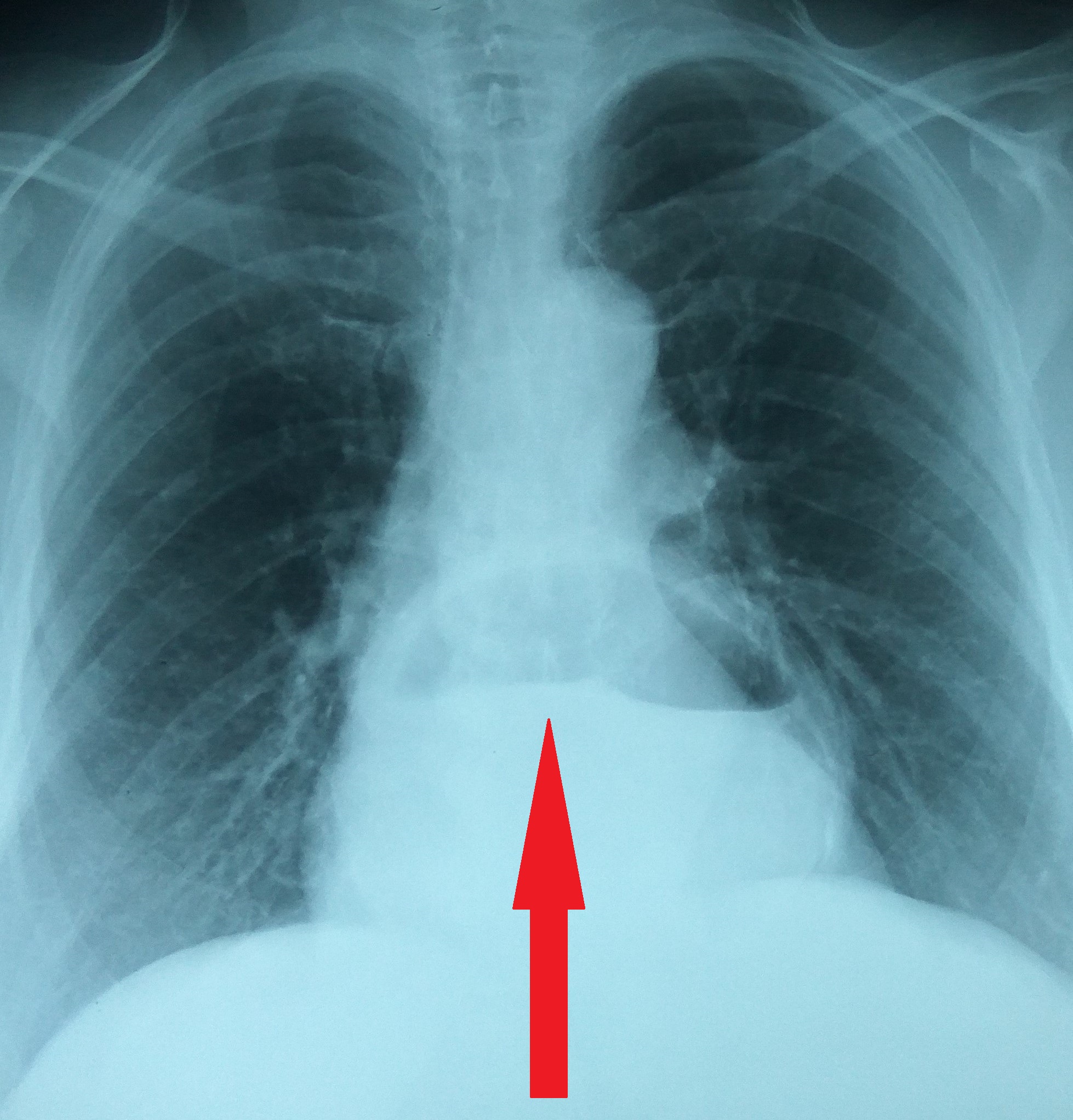
Chest x-ray showing an elevated air-fluid level - ( red arrow ).(Courtesy Dr. V . Penopoulos).

Diaphragmatic hernia after reduction of the stomach.(Courtesy Dr. V . Penopoulos).
Water-soluble gastrografin meal showing postoperative normal positioning of stomach (Courtesy Dr. V. Penopoulos)

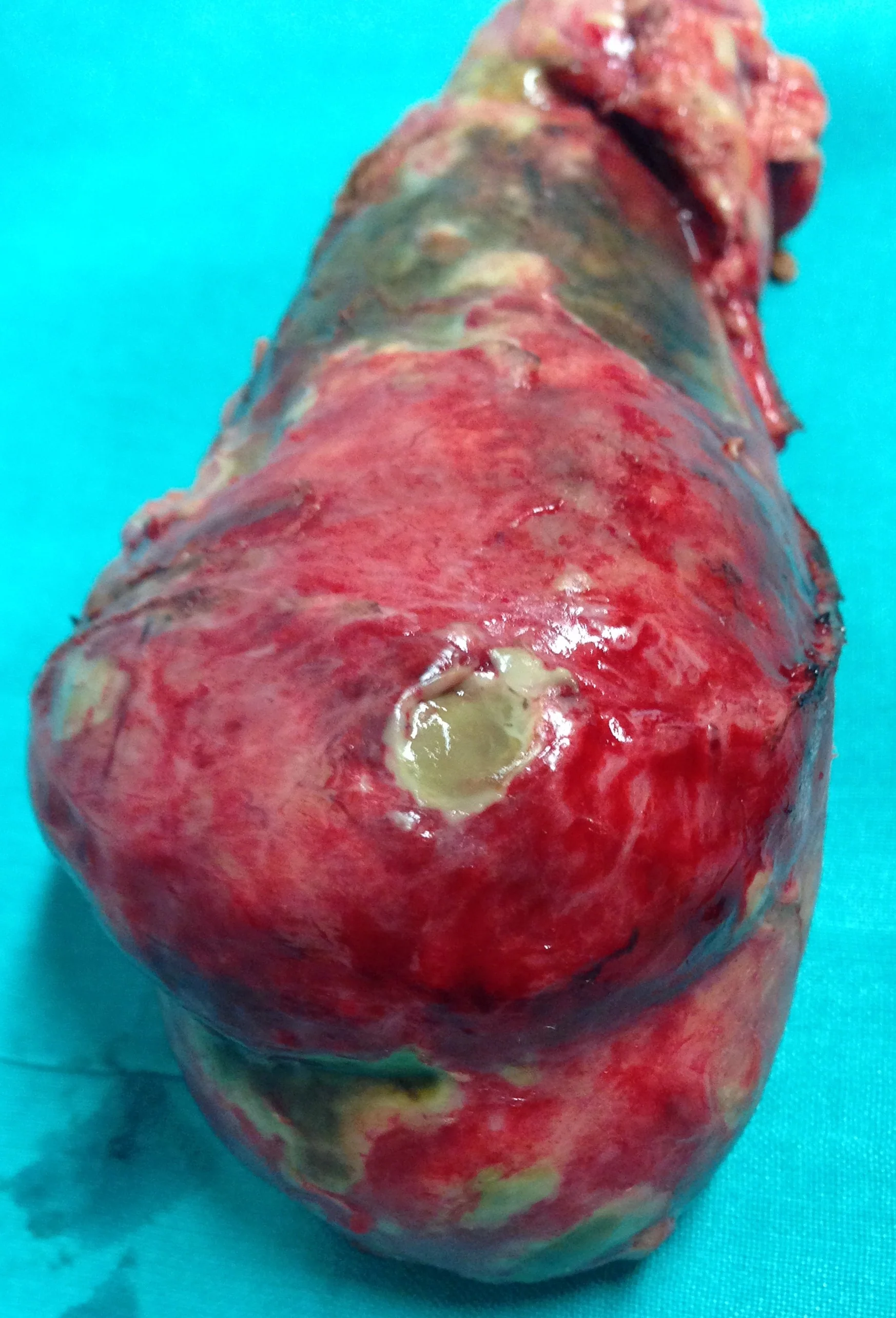
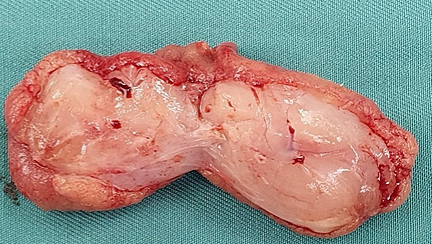
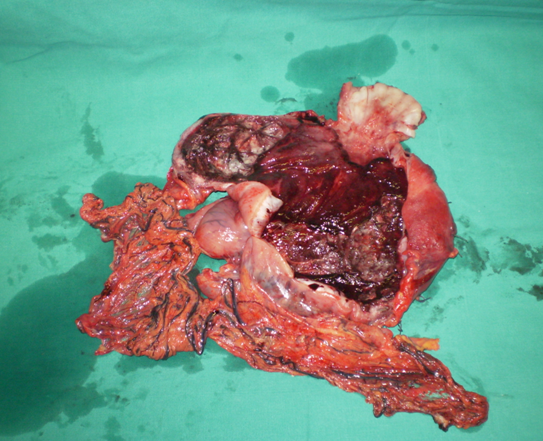
Esophagectomy. Esophageal burns following ingestion of acid . (Courtesy Dr.V.Penopoulos).

Diaphragmatic hernia before reduction of the stomach.(Courtesy Dr. V . Penopoulos).

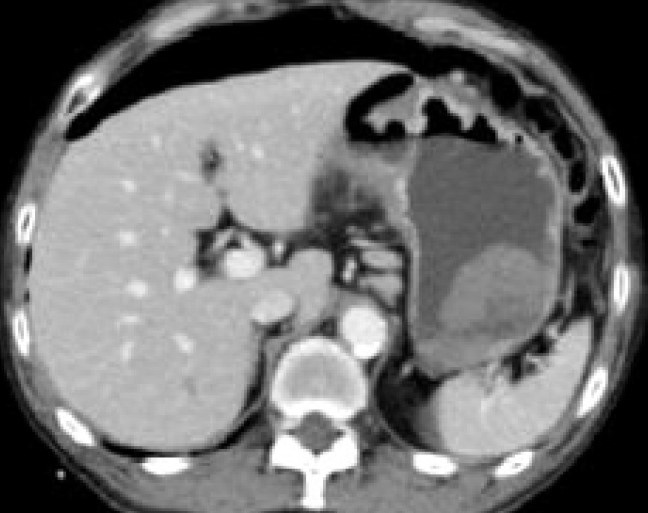
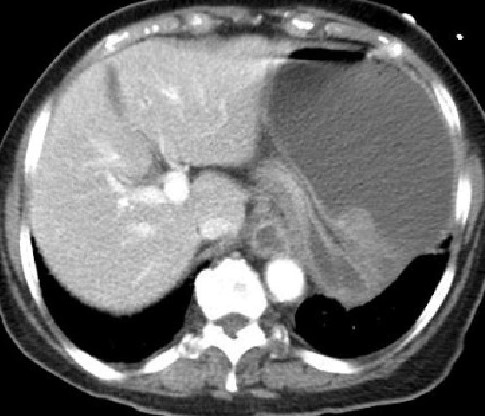
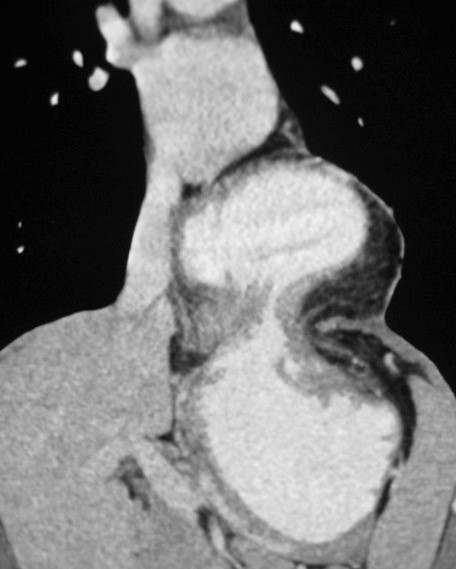
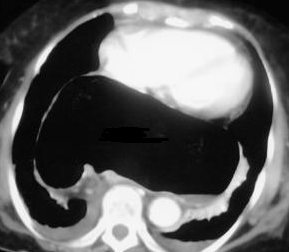
Abdominal CT Scan.Left diaphragmatic hernia with a dilated stomach.(Courtesy Dr. V . Penopoulos).

Burns following ingestion of acids ( HCl ).Diffuse burns and shrinkage of esophagus .(Courtesy Dr.V.Penopoulos).
Endoscopic view of esophago-jejunal anastomosis. (Courtesy Dr.V.Penopoulos).


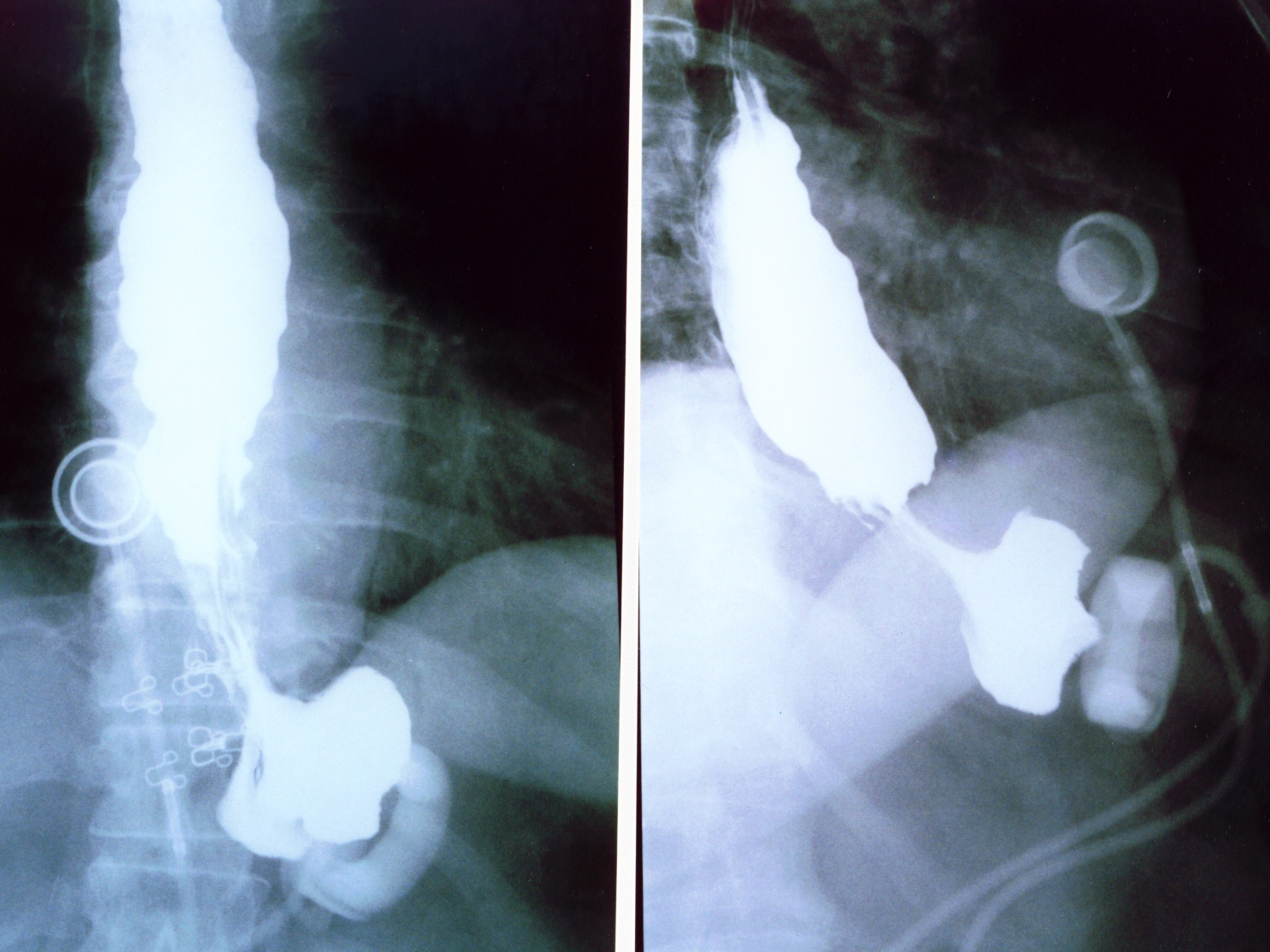
Esophagographies.Various types of esophageal strictures.(Courtesy Dr.V.Penopoulos).

Esophagographies.Various types of esophageal strictures.(Courtesy Dr.V.Penopoulos).
Esophagographies.Various types of esophageal strictures.(Courtesy Dr.V.Penopoulos).

Endoscopic view of esophago-gastric anastomosis. (Courtesy Dr.V.Penopoulos).
Performing a transthoracic esophago-jejunal anastomosis. (Courtesy Dr.V.Penopoulos).
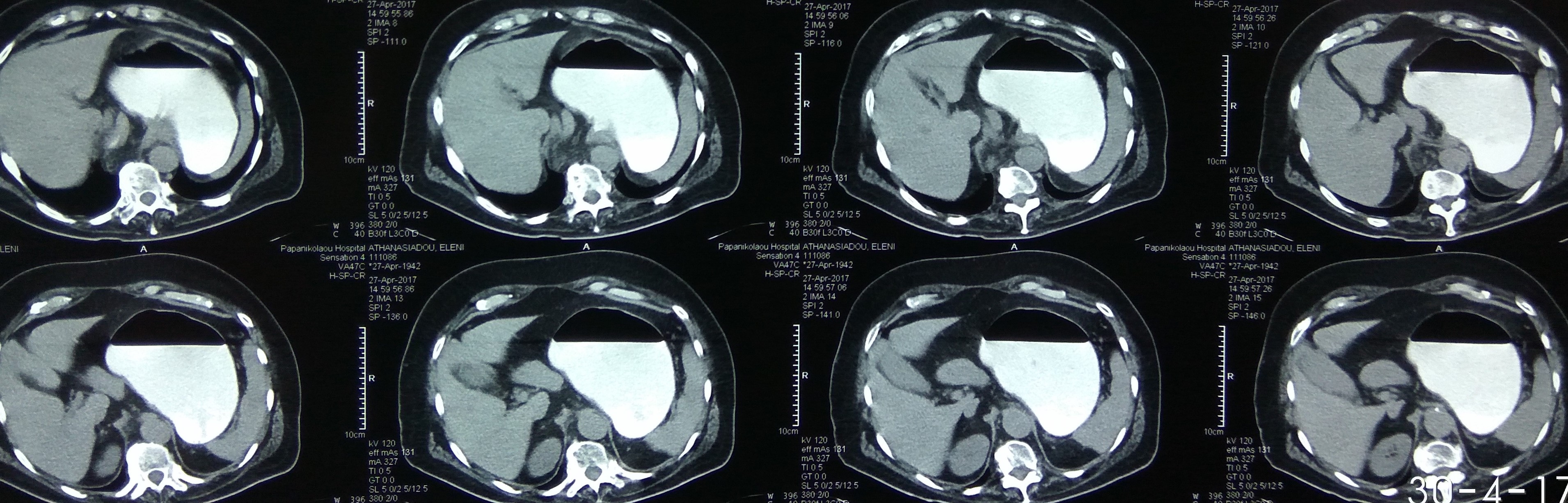
Abdominal CT Scan.Left diaphragmatic hernia with a dilated stomach.(Courtesy Dr. V . Penopoulos).

Esophagographies.Various types of esophageal strictures.(Courtesy Dr.V.Penopoulos).

Esophagographies.Various types of esophageal strictures.(Courtesy Dr.V.Penopoulos).


Burns following ingestion of acids ( HCl ).Diffuse burns and shrinkage of esophagus .(Courtesy Dr.V.Penopoulos).

Esophagography .Various types of esophageal strictures.(Courtesy Dr.V.Penopoulos).

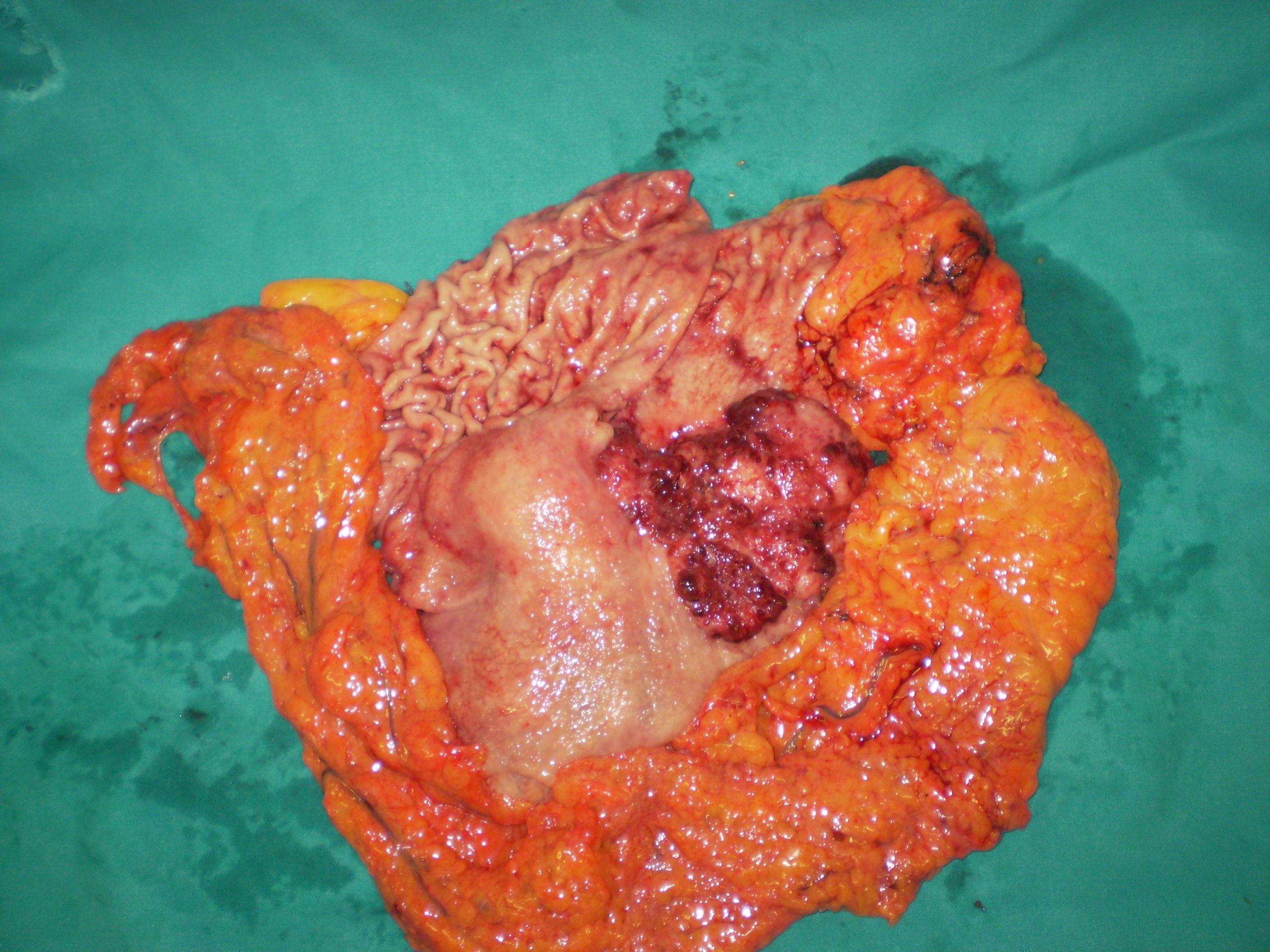
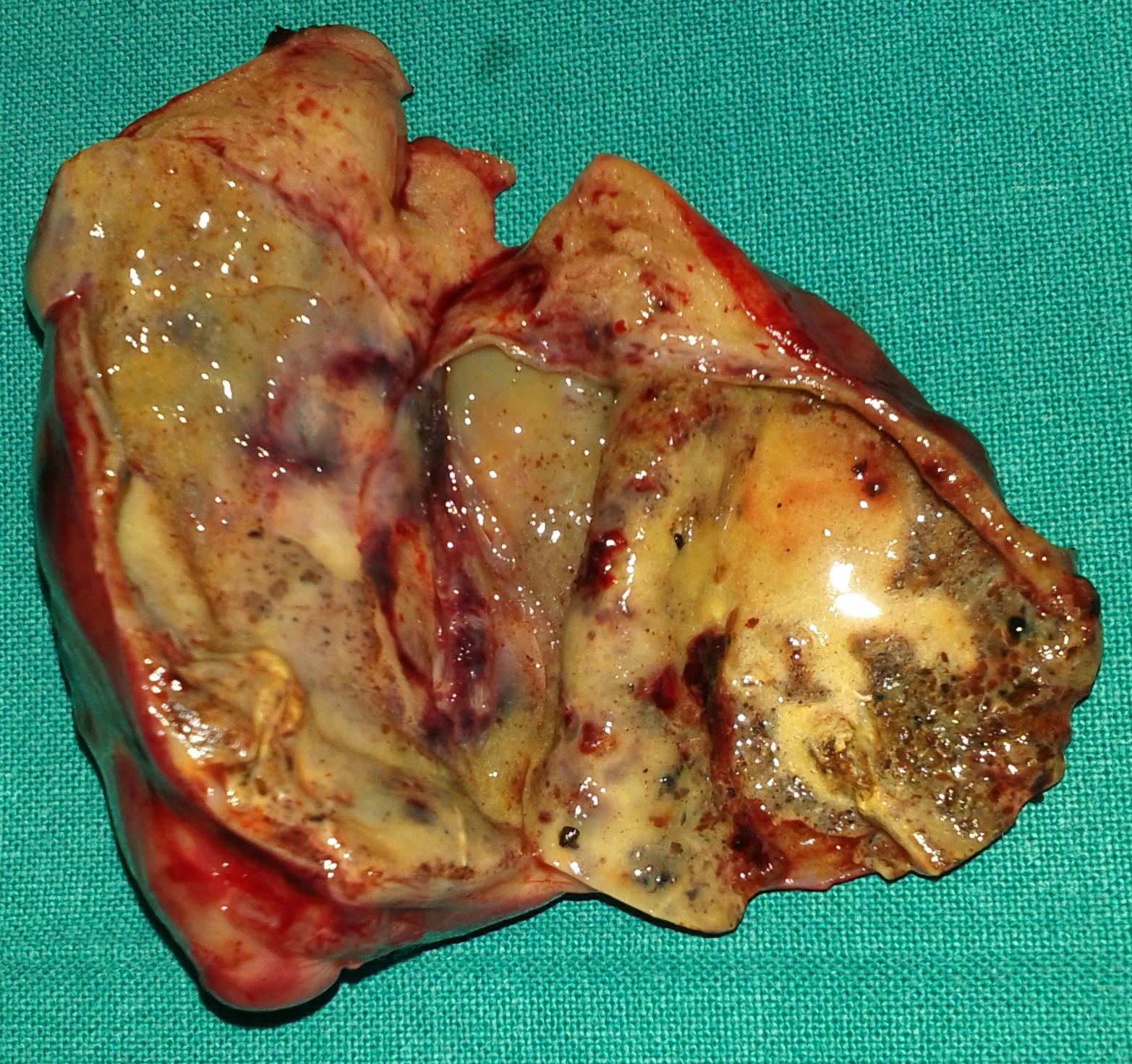
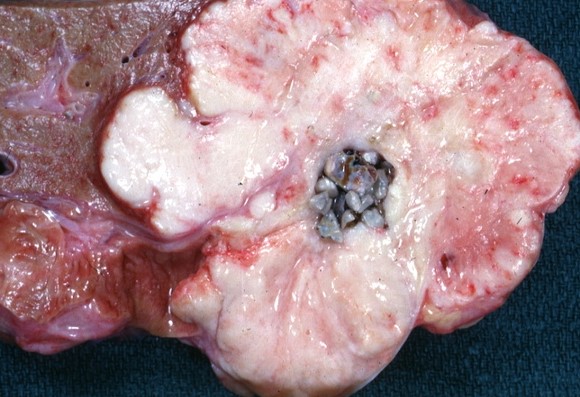
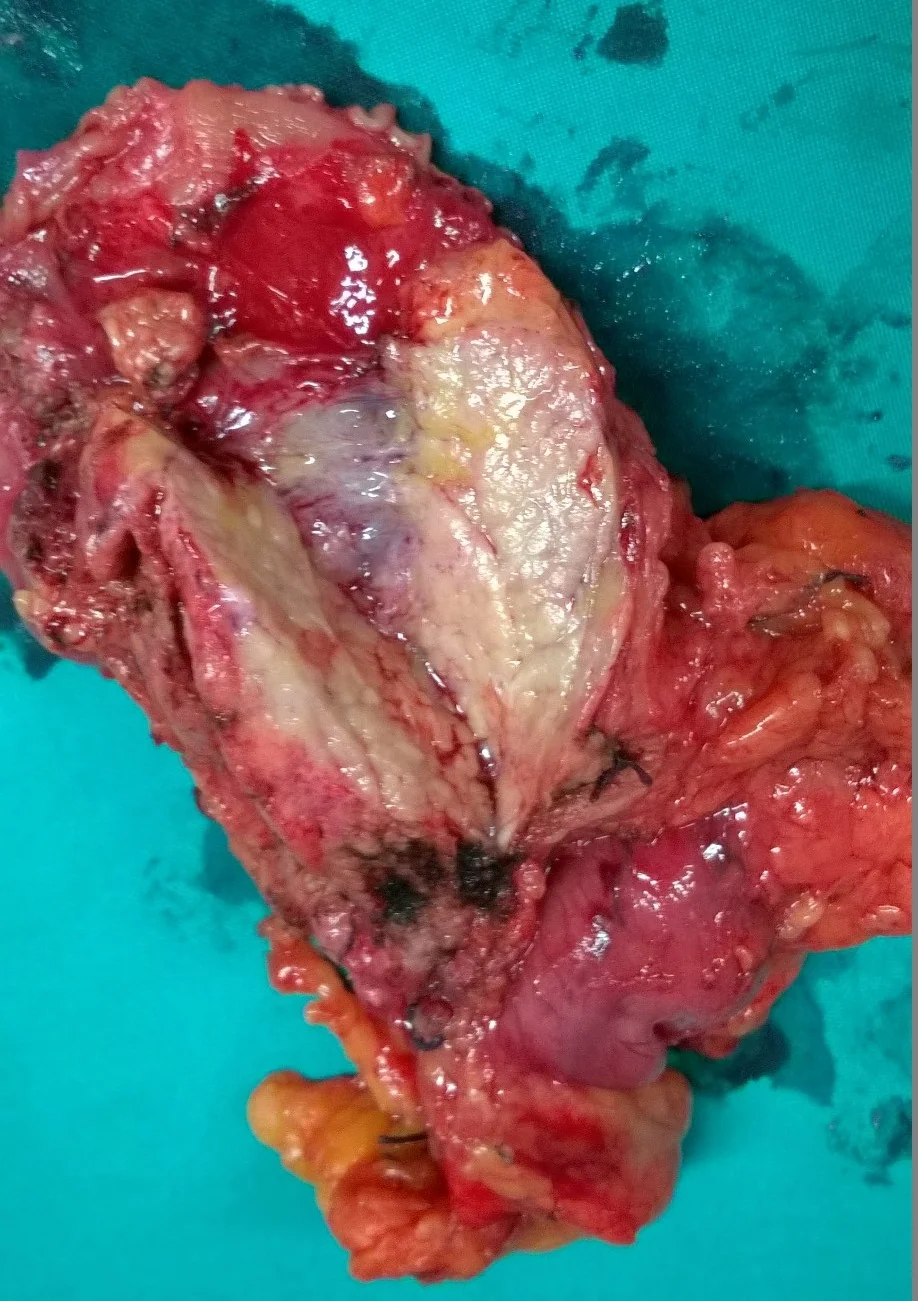
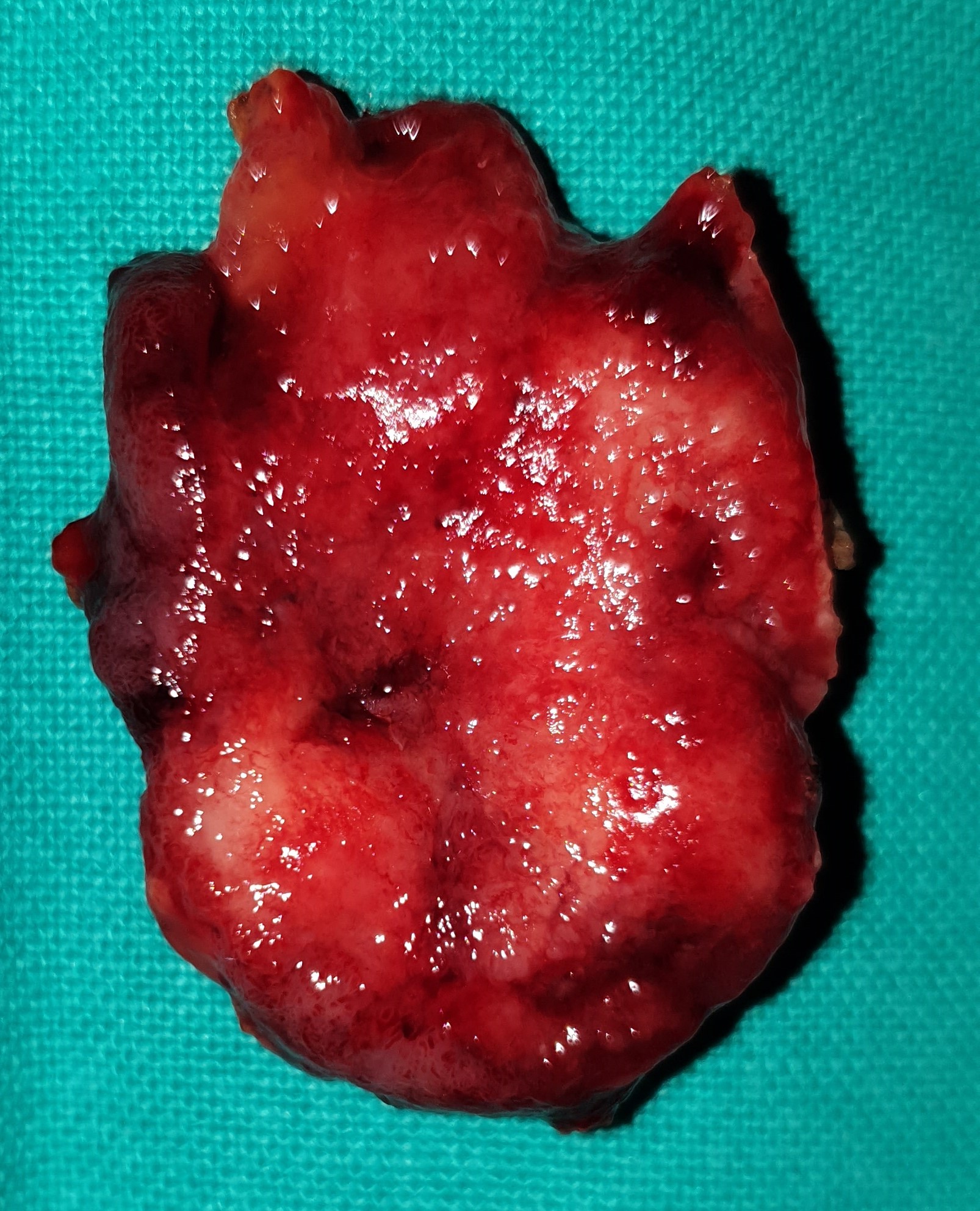
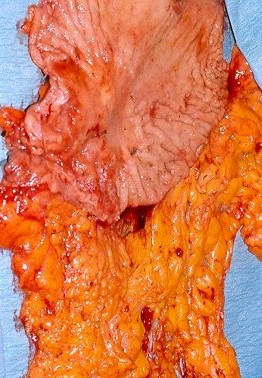
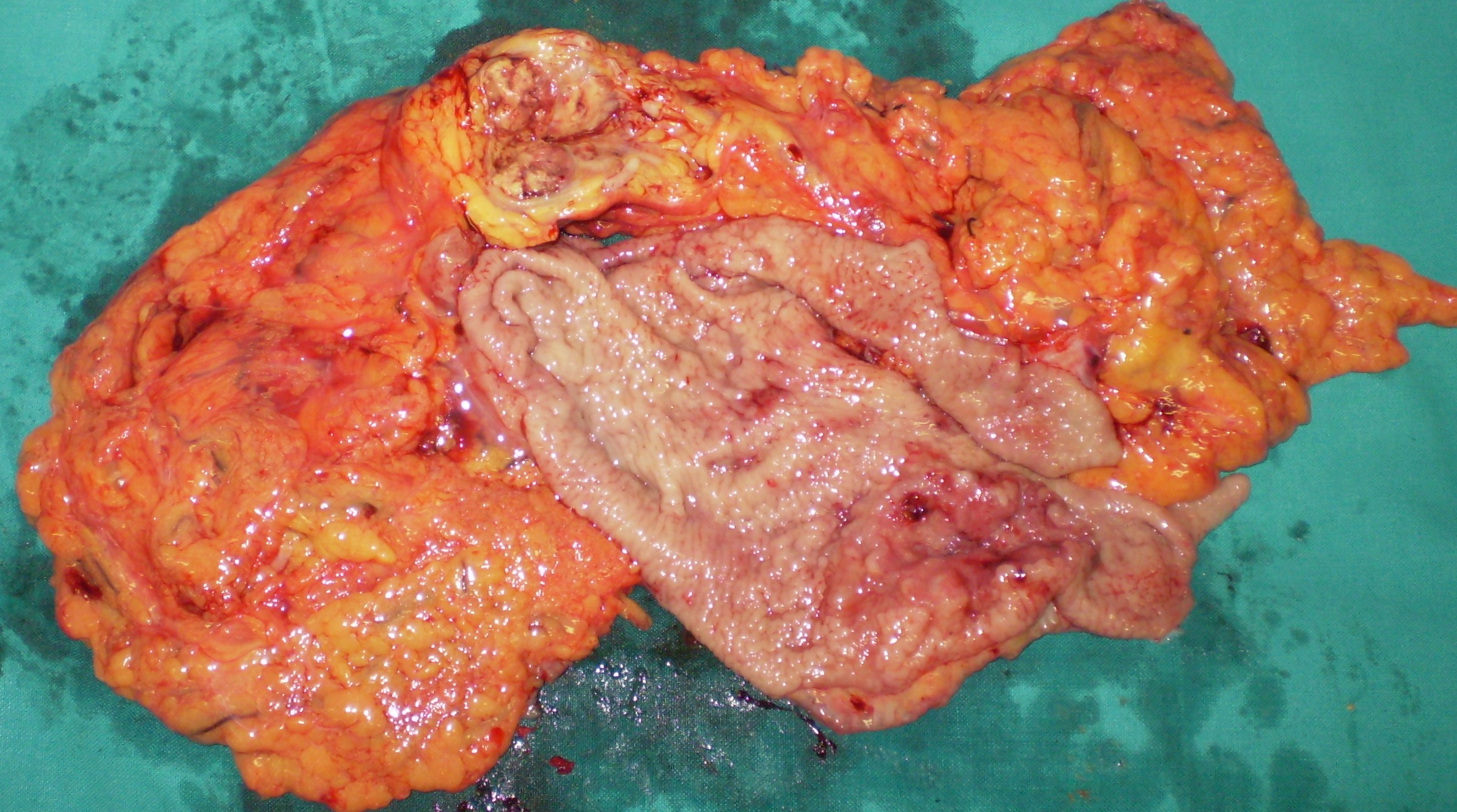
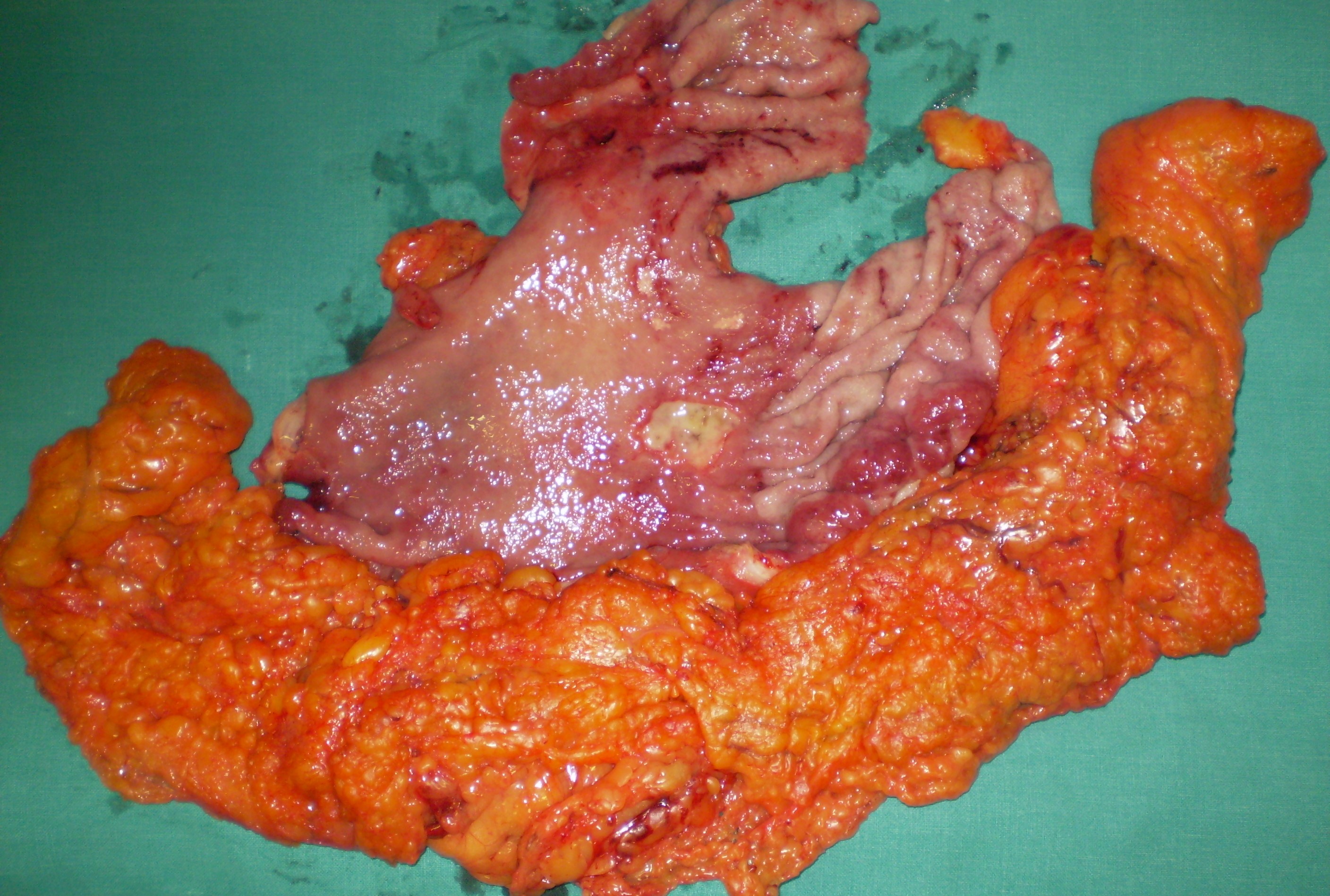
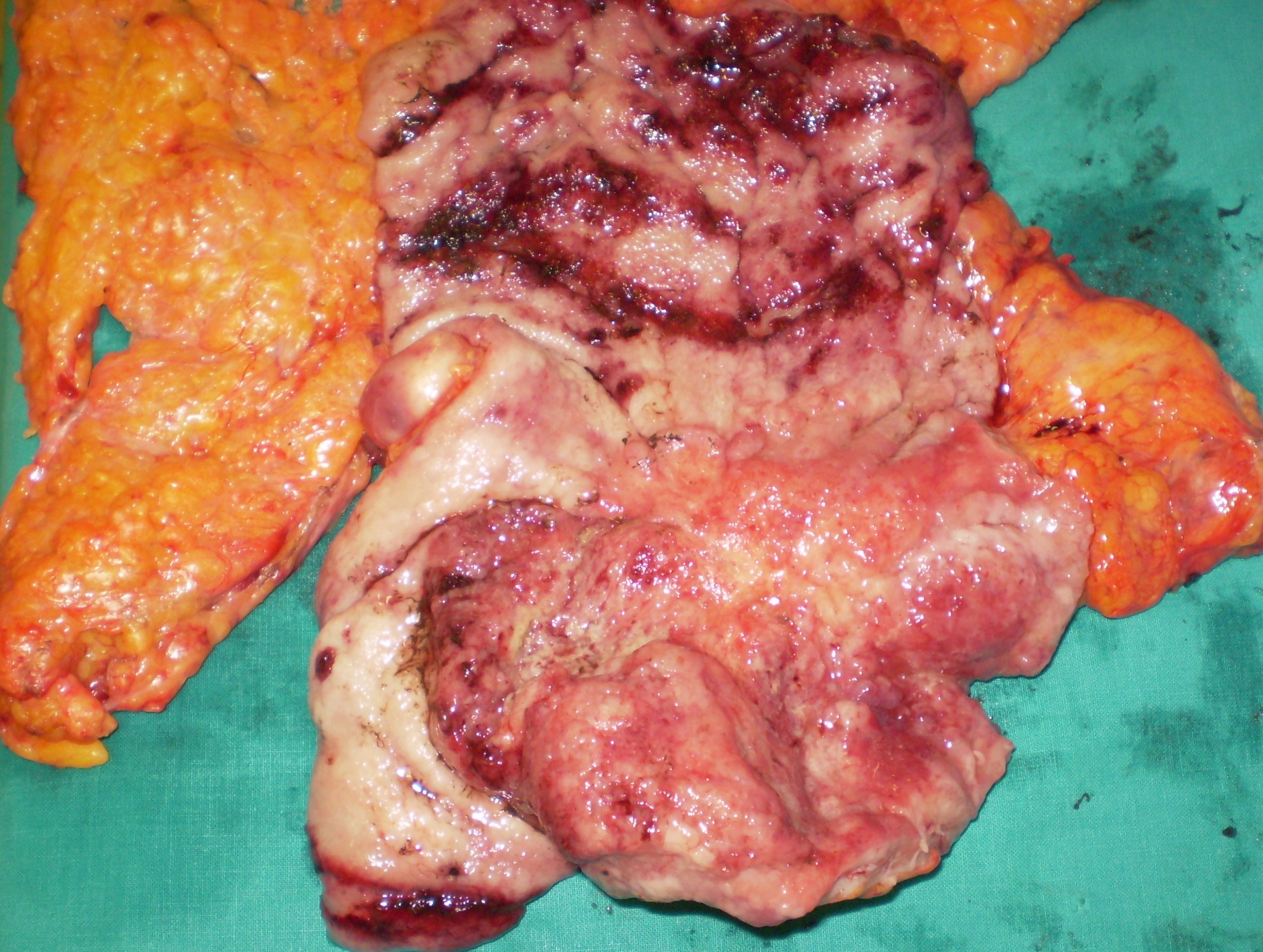
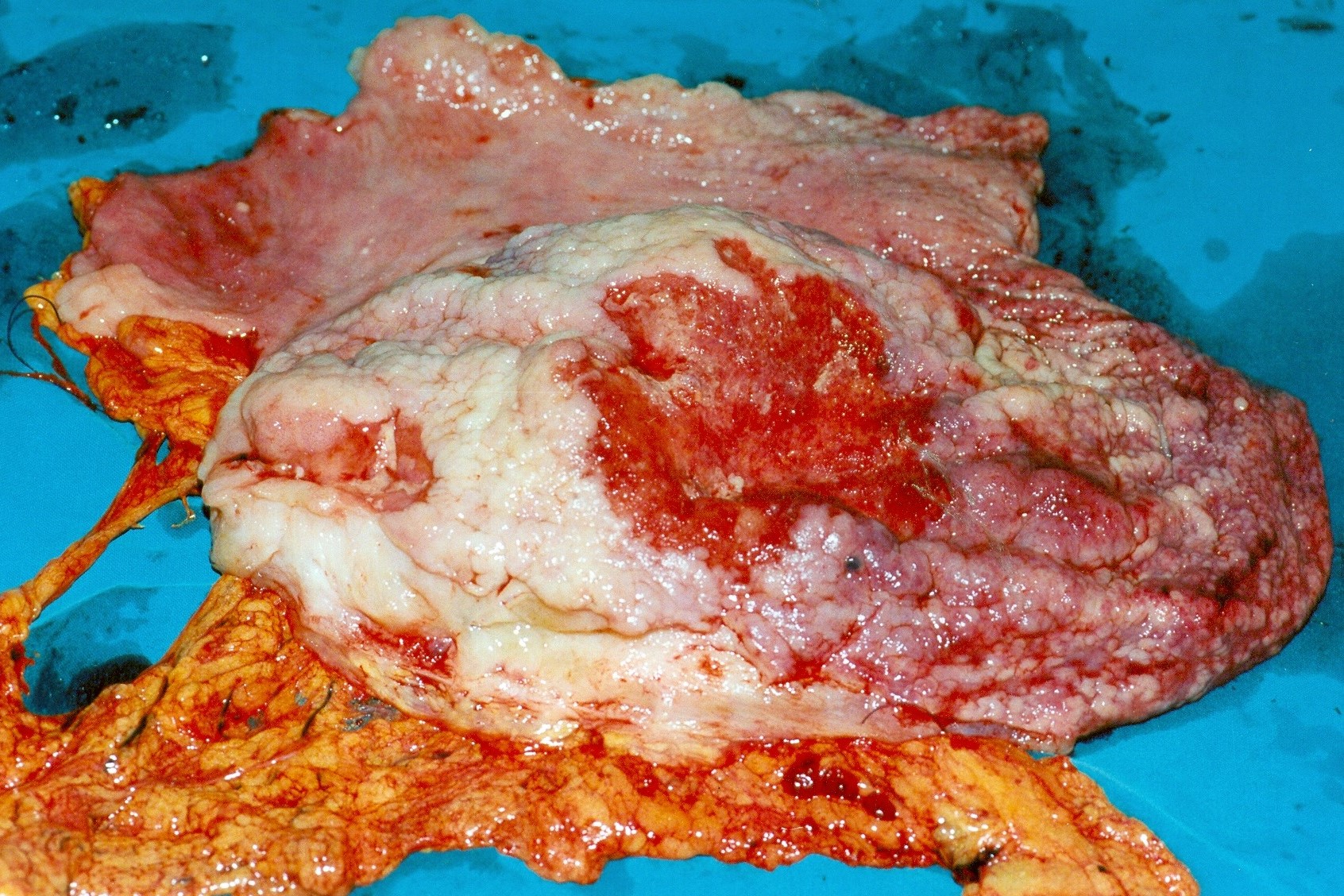
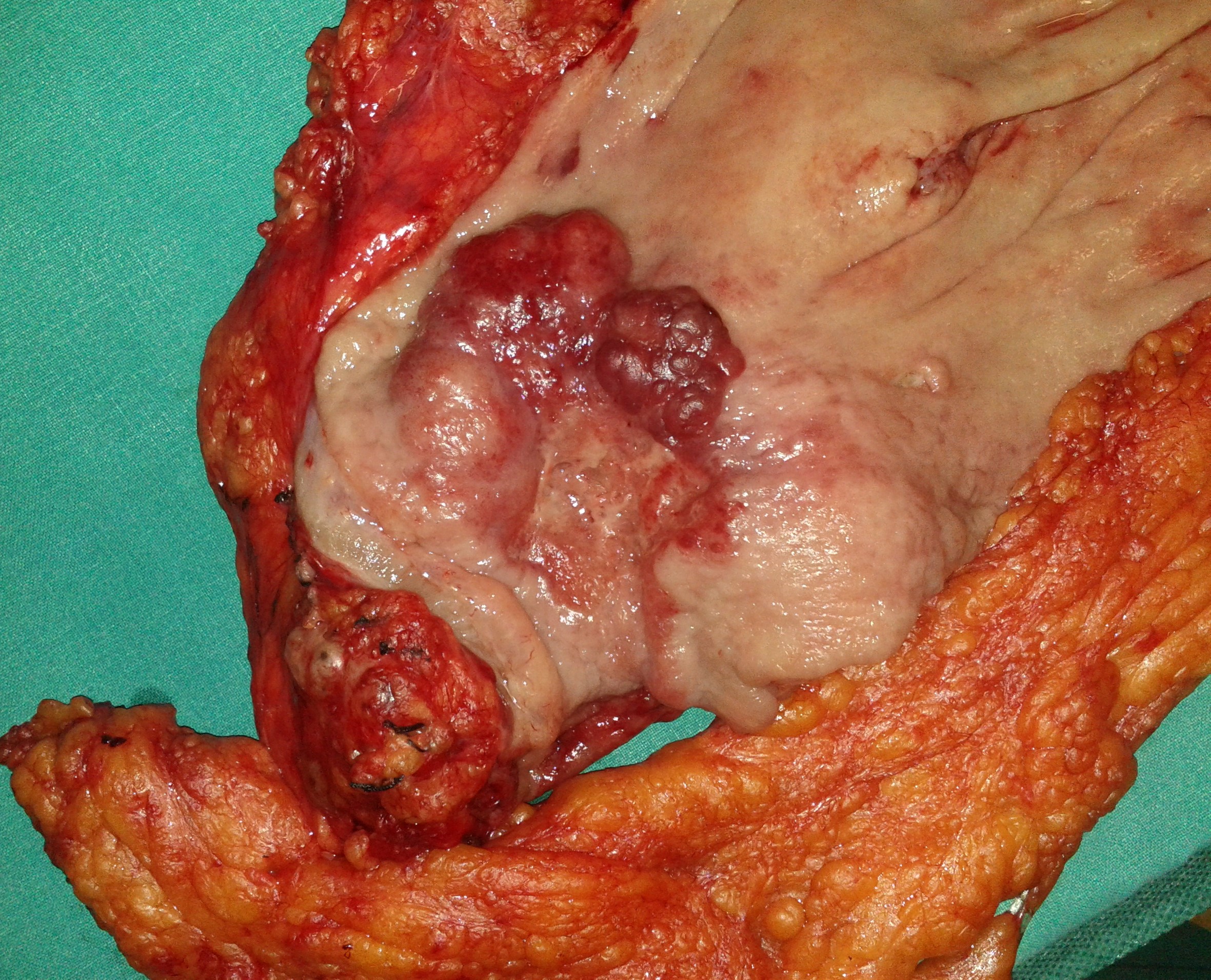
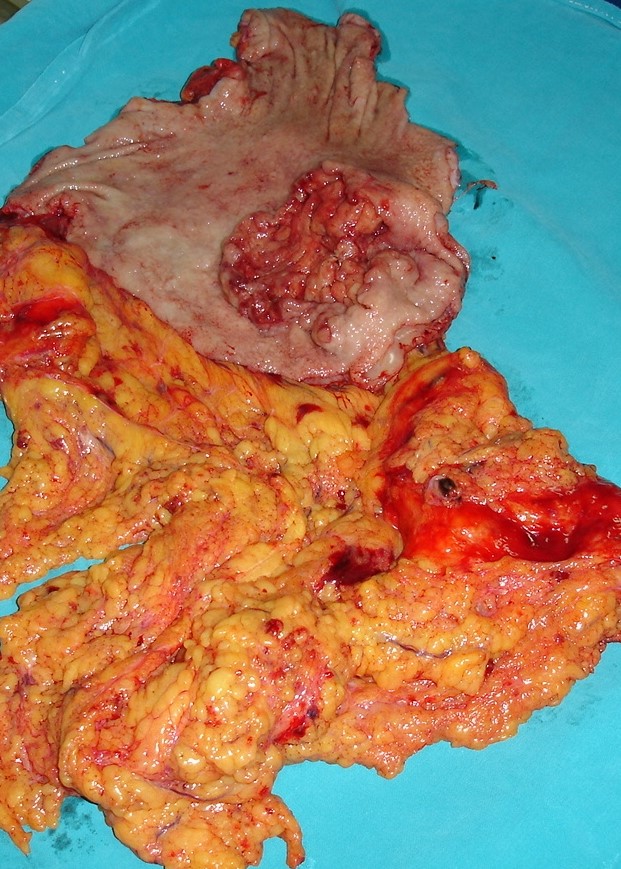
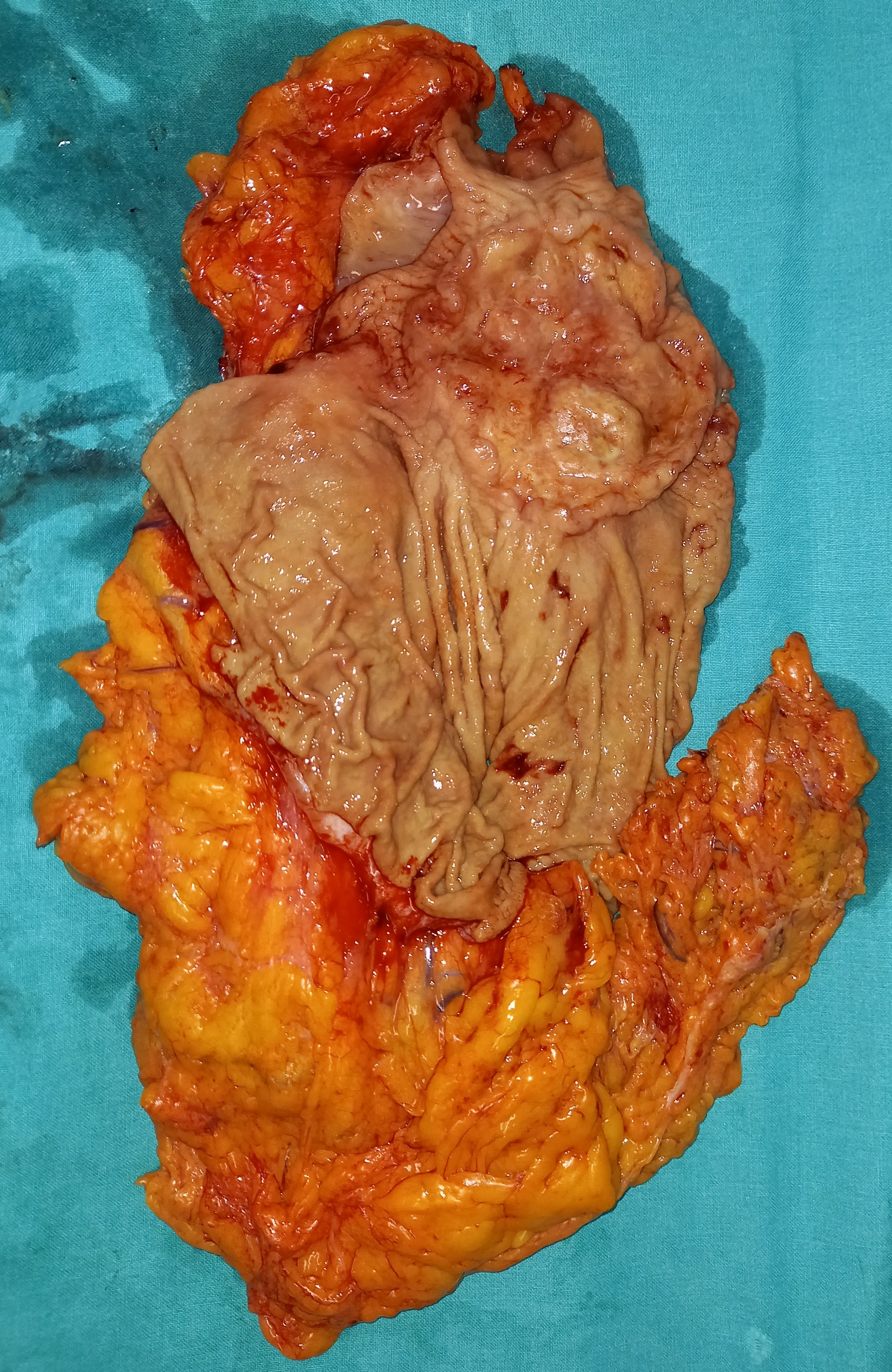
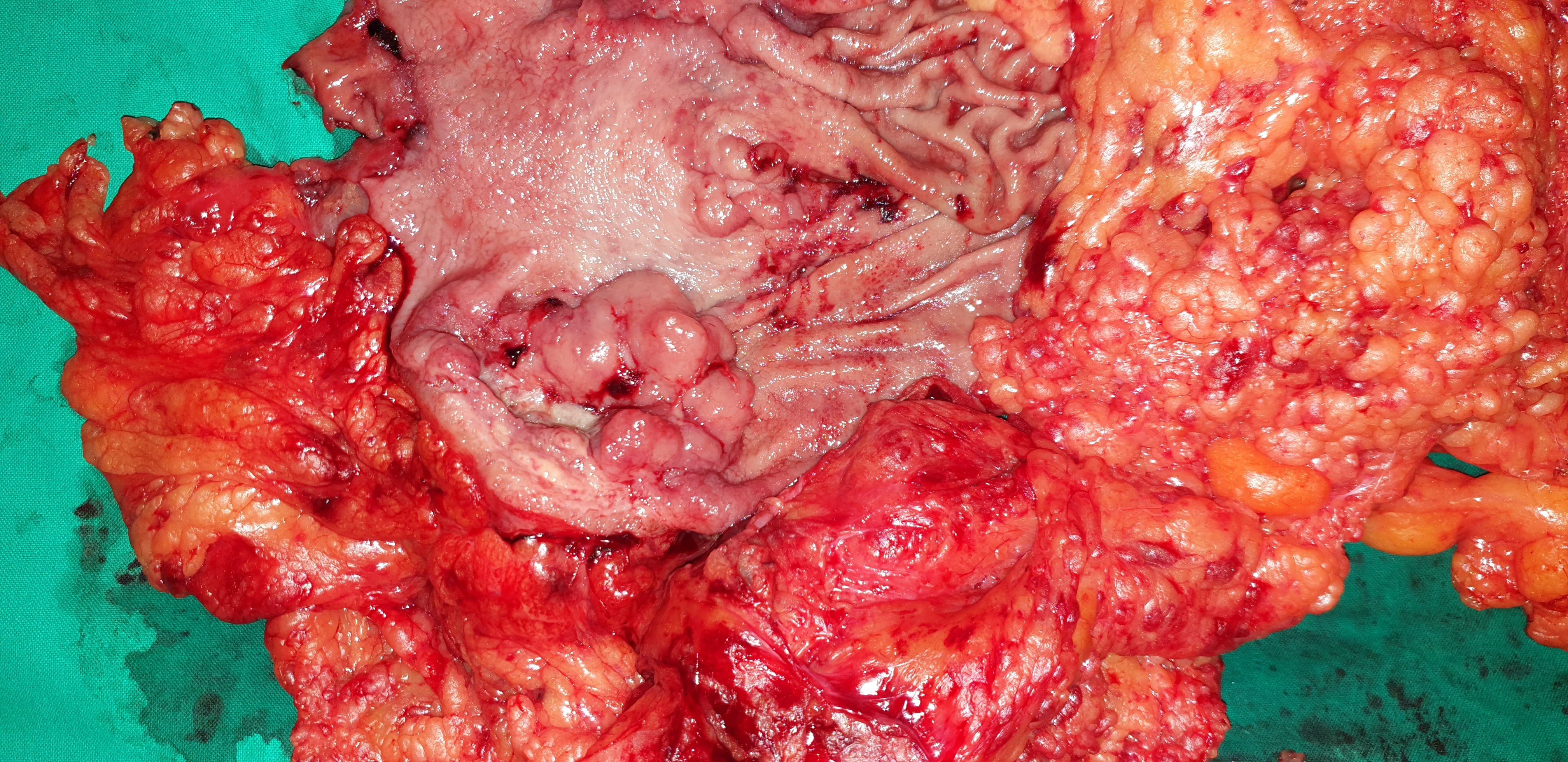
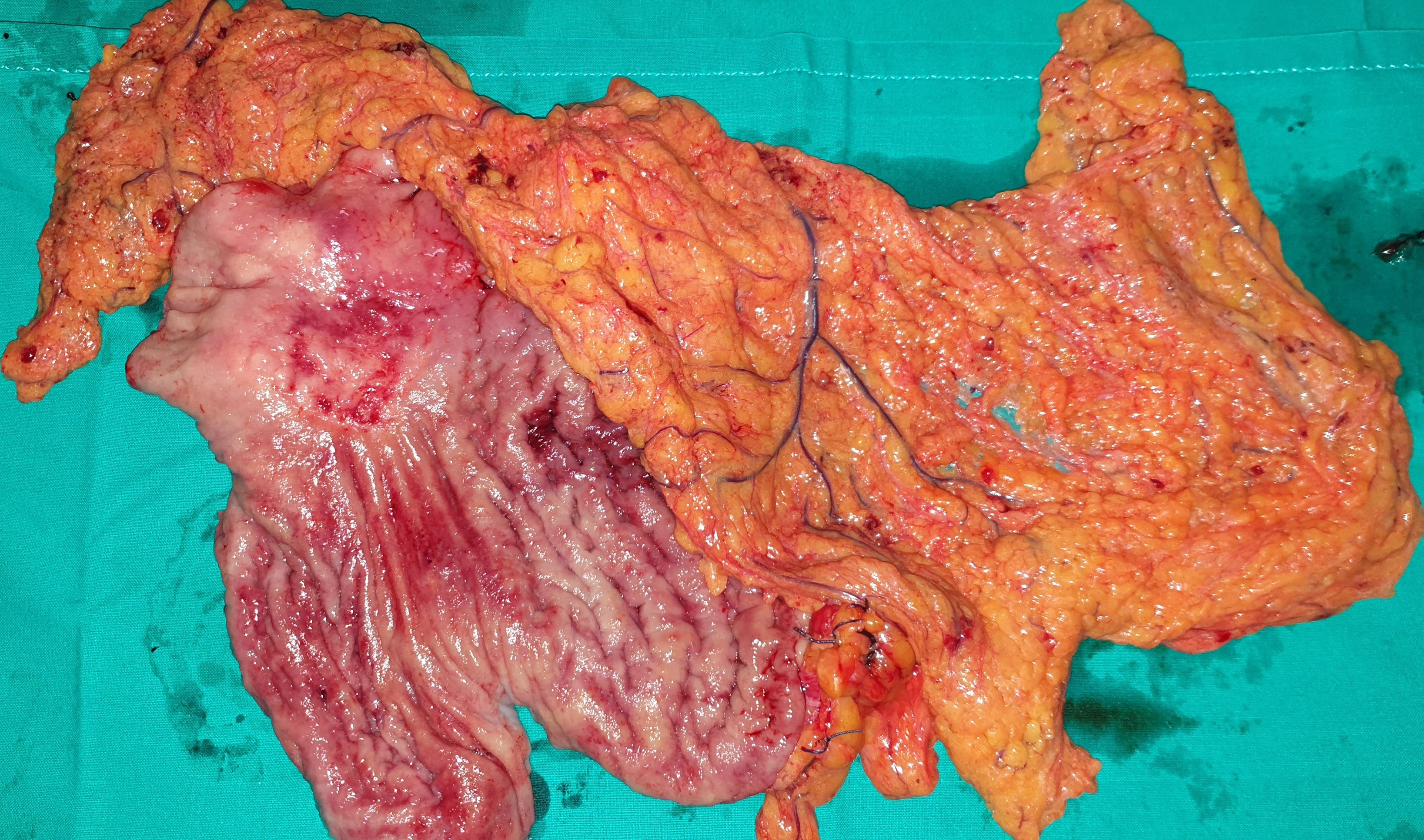
Poorly differentiated adenocarcinoma invading full thickness the gastric wall and surrounding fatty tissue with clear cut margins .( Courtesy Dr . V . Penopoulos ) .
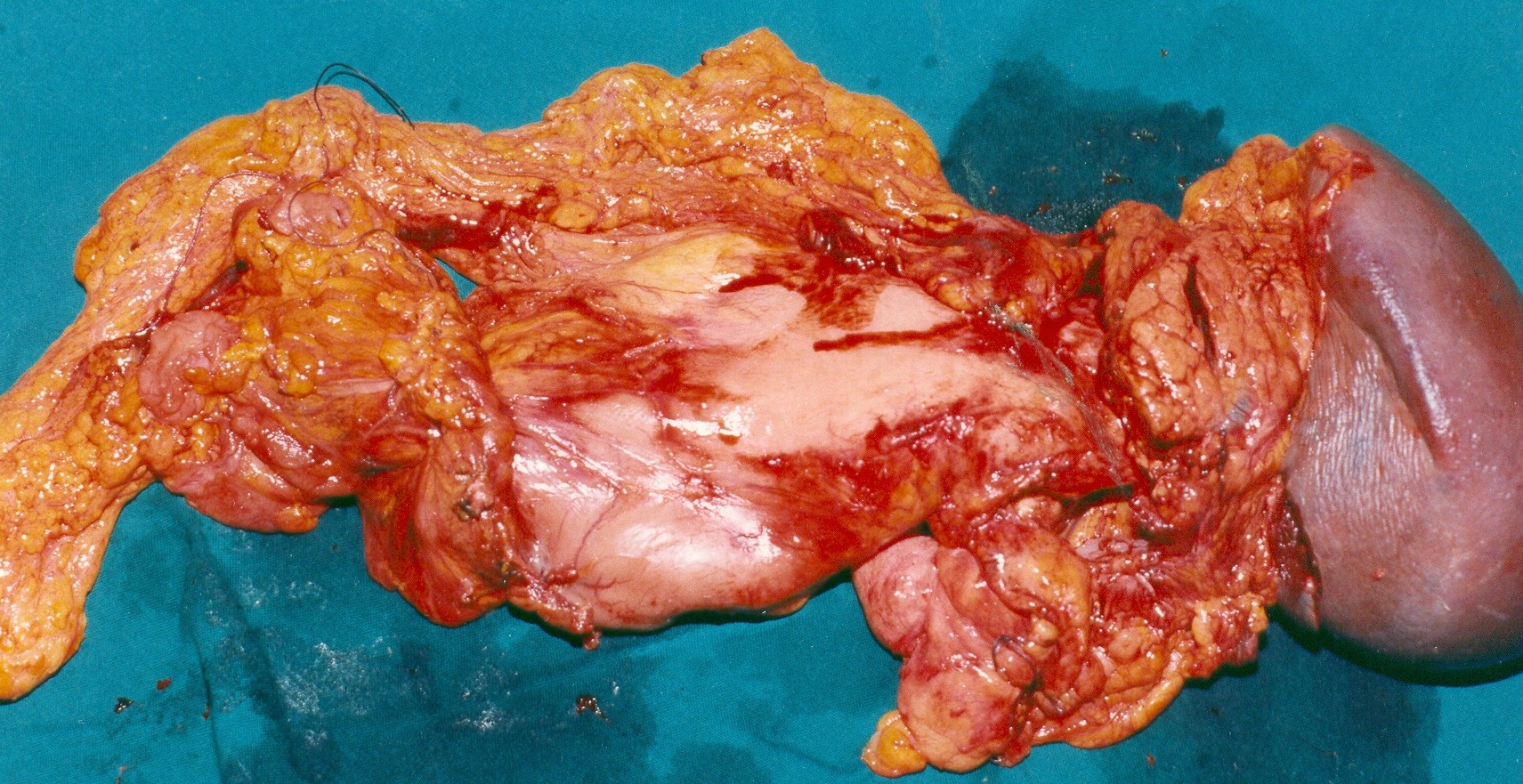
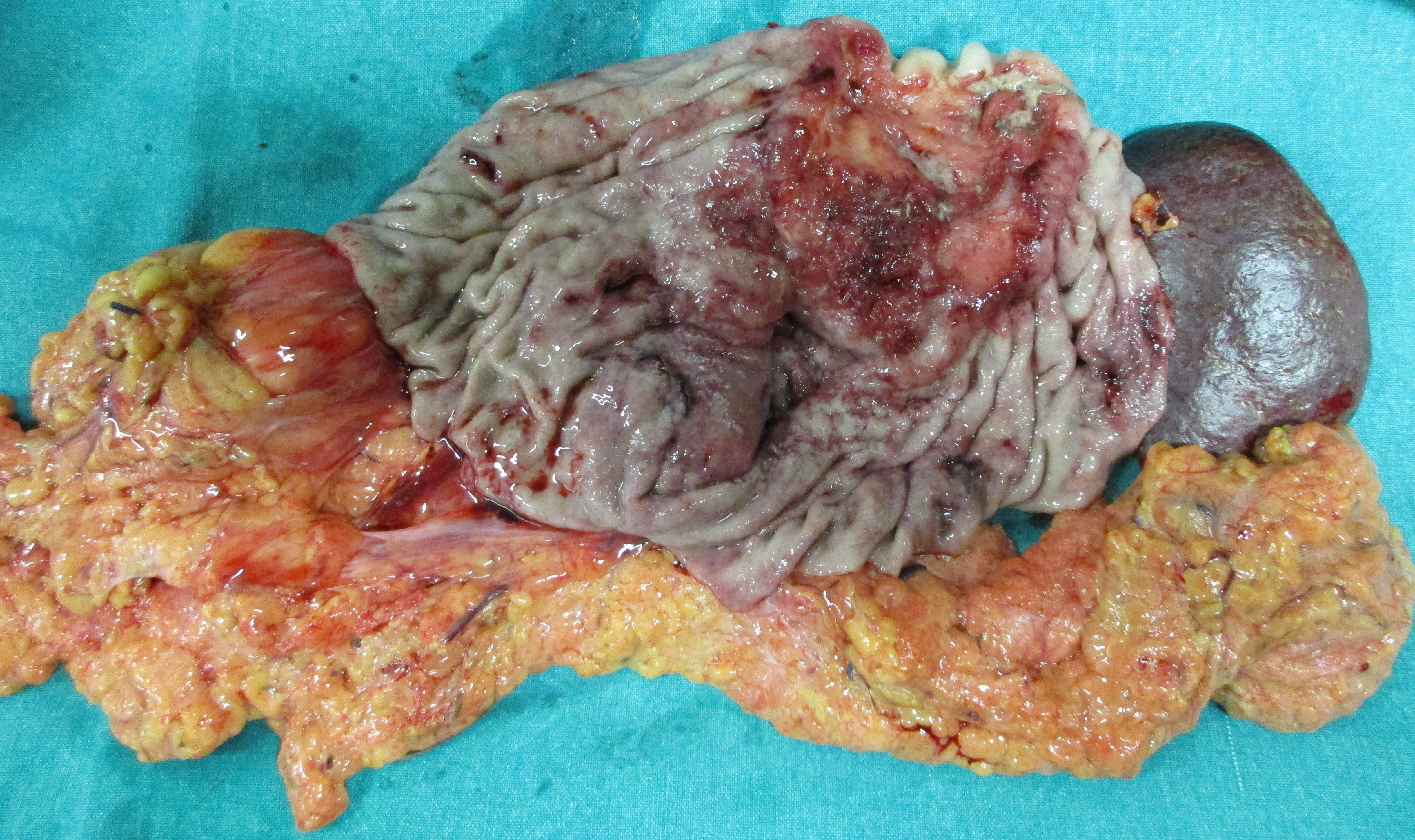
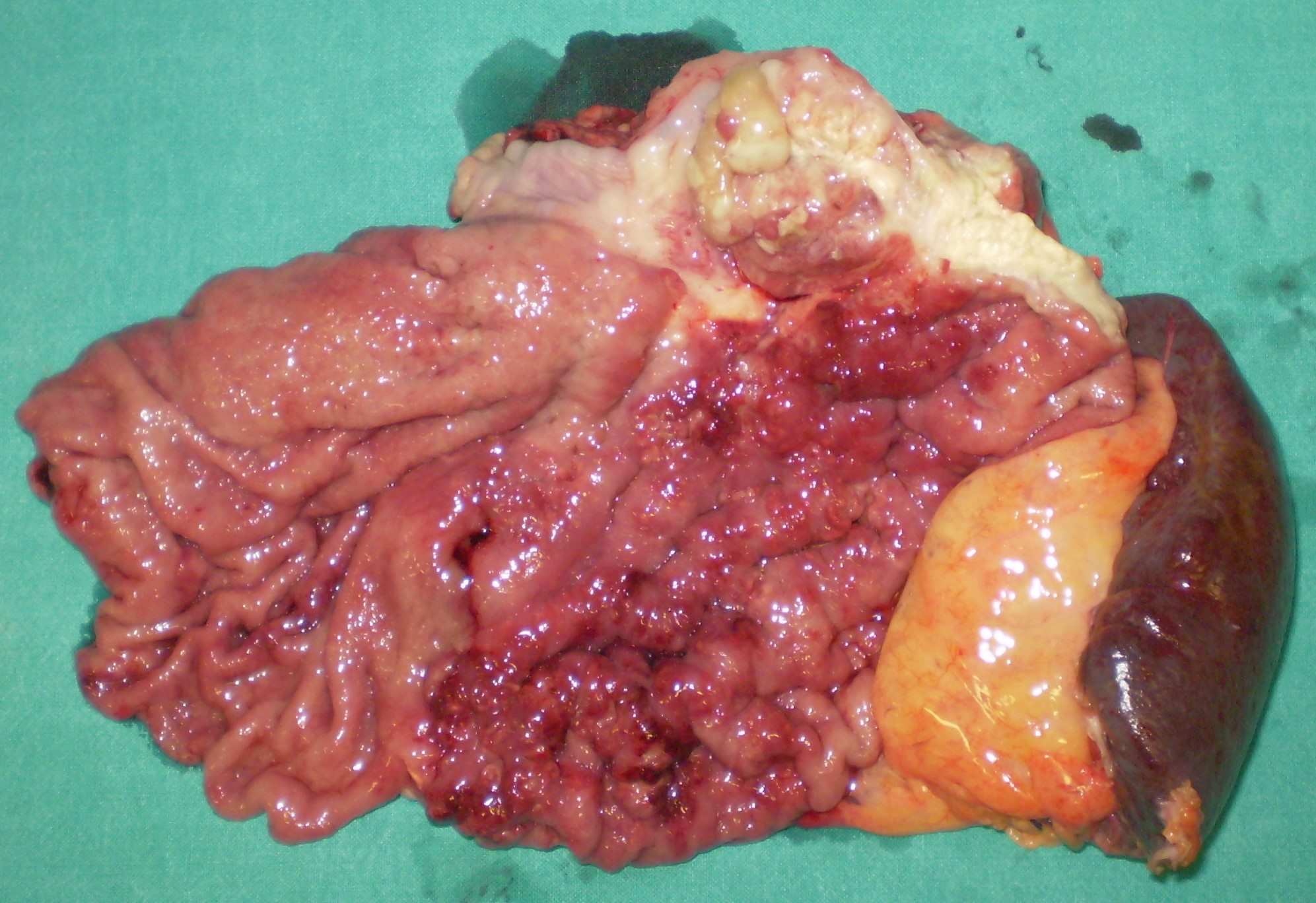
Colonic carcinoma in contact with the splenic abscess cavity. (Courtesy Dr . V . Penopoulos).

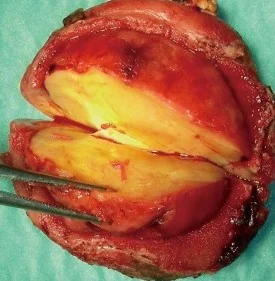
Duodenectomy sparing Vater s papilla .Poorly differentiated adenocarcinoma invading full thickness the duodenal wall and surrounding fatty tissue with clear cut margins (Courtesy Dr. V. Penopoulos)


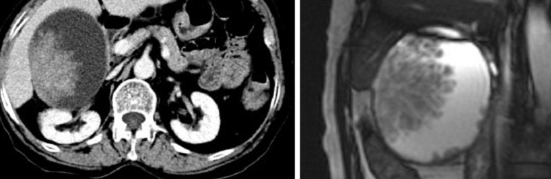
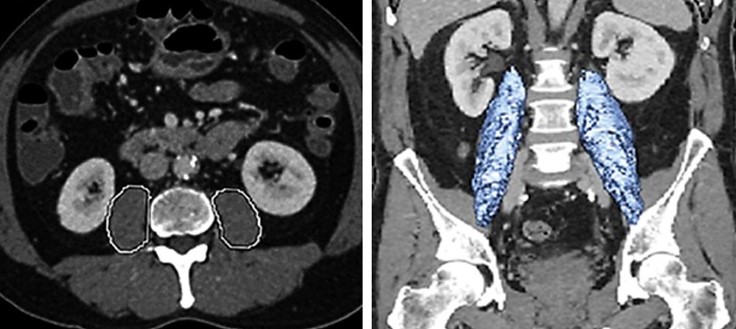
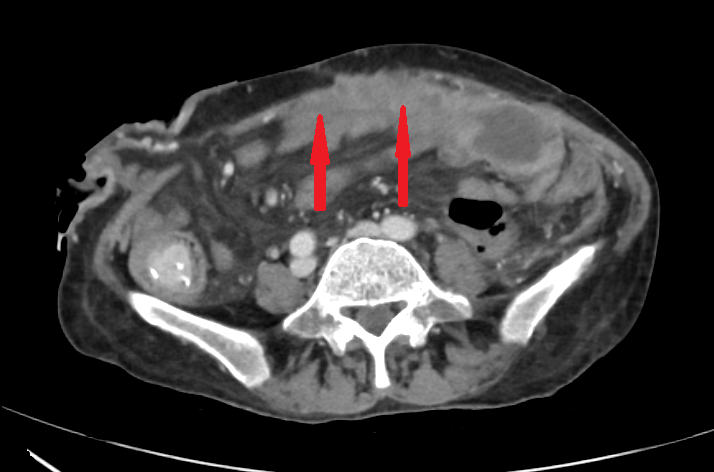
CT Scan. The gastric tumors are obvious (red arrow). Incidental finding right sided sizable renal cysts (blue arrow)


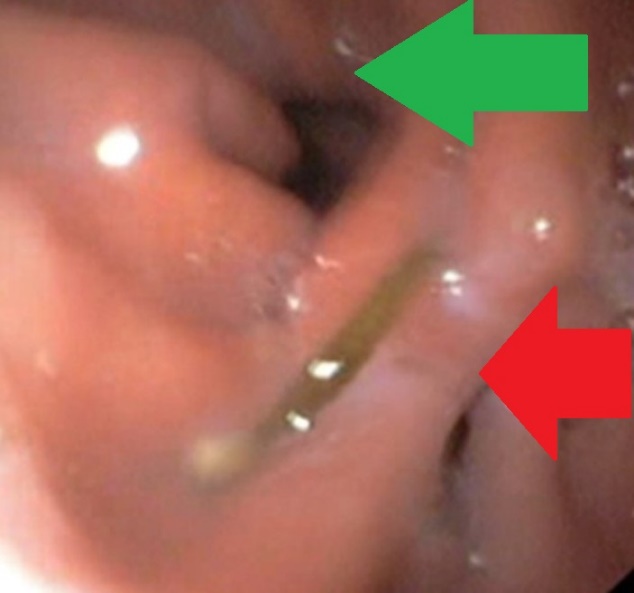
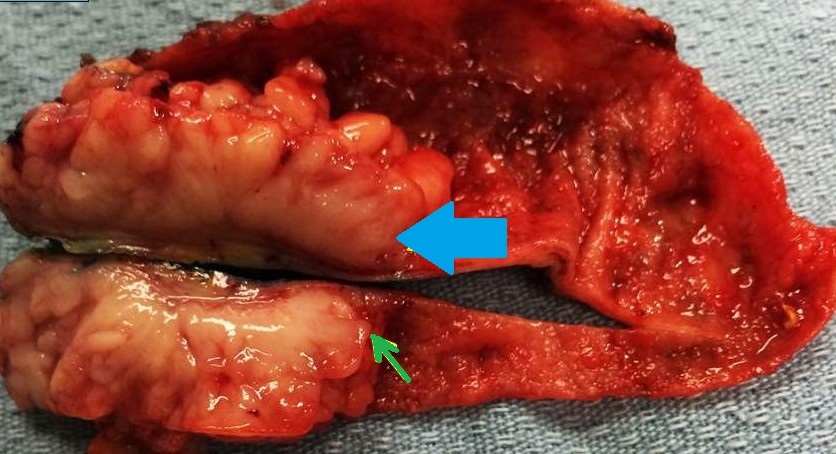
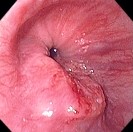
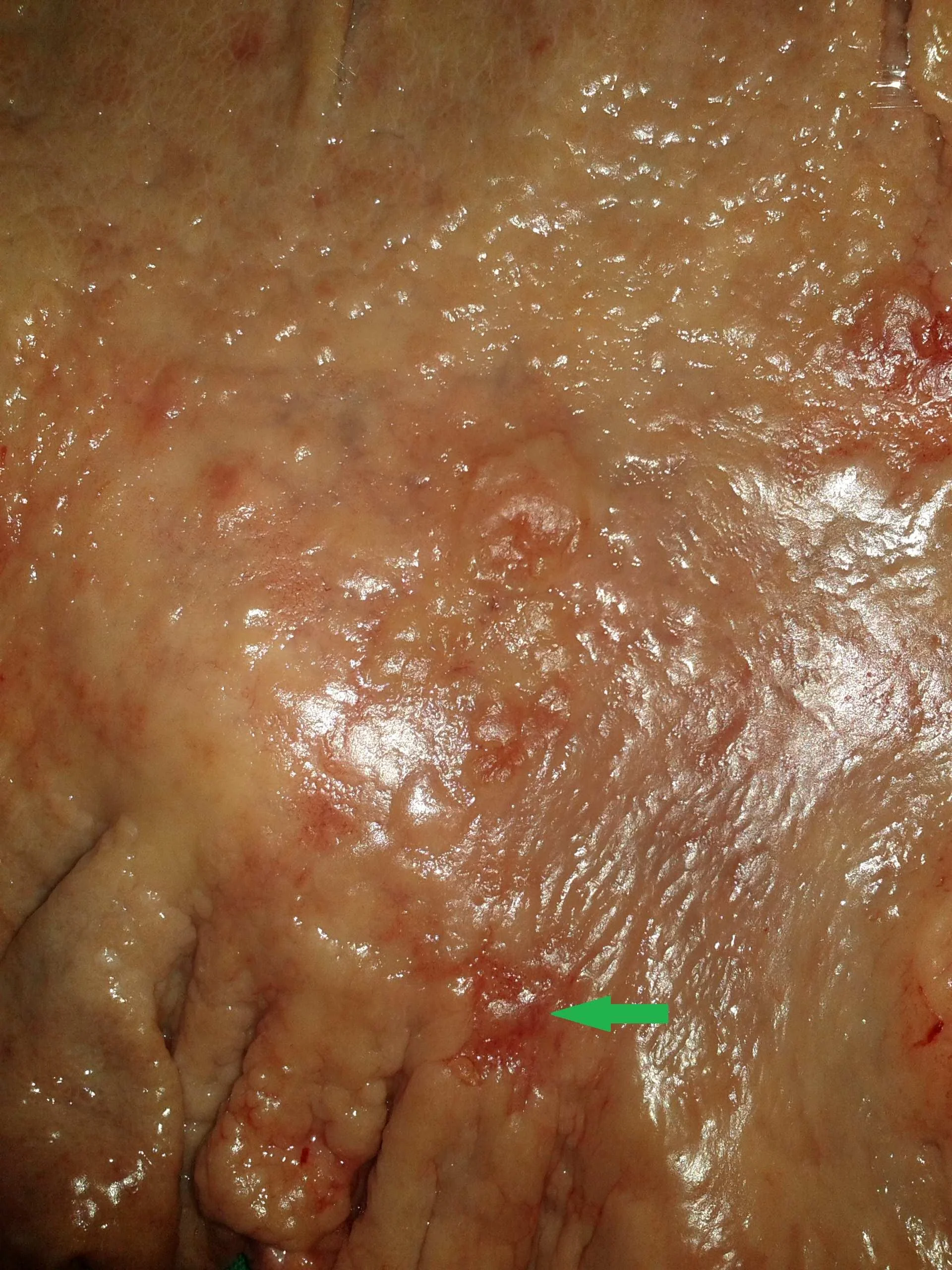
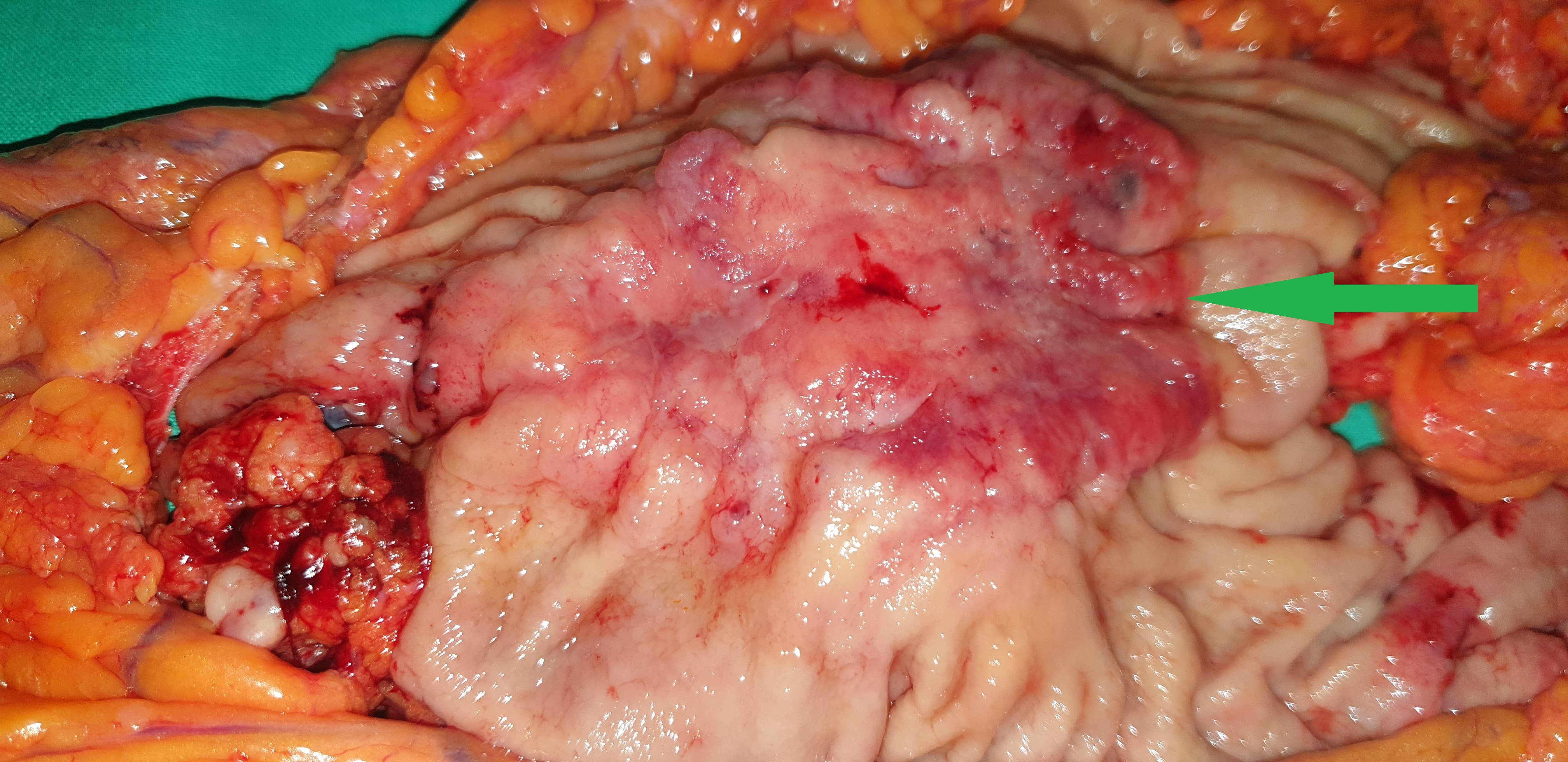
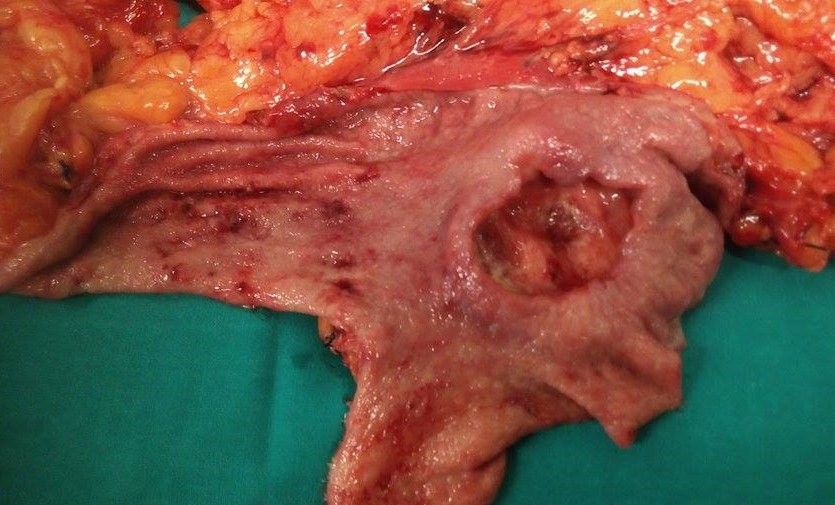
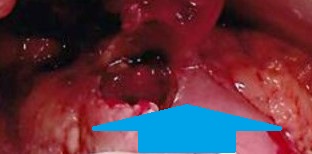
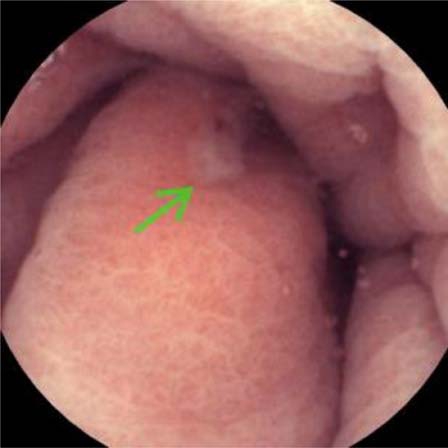
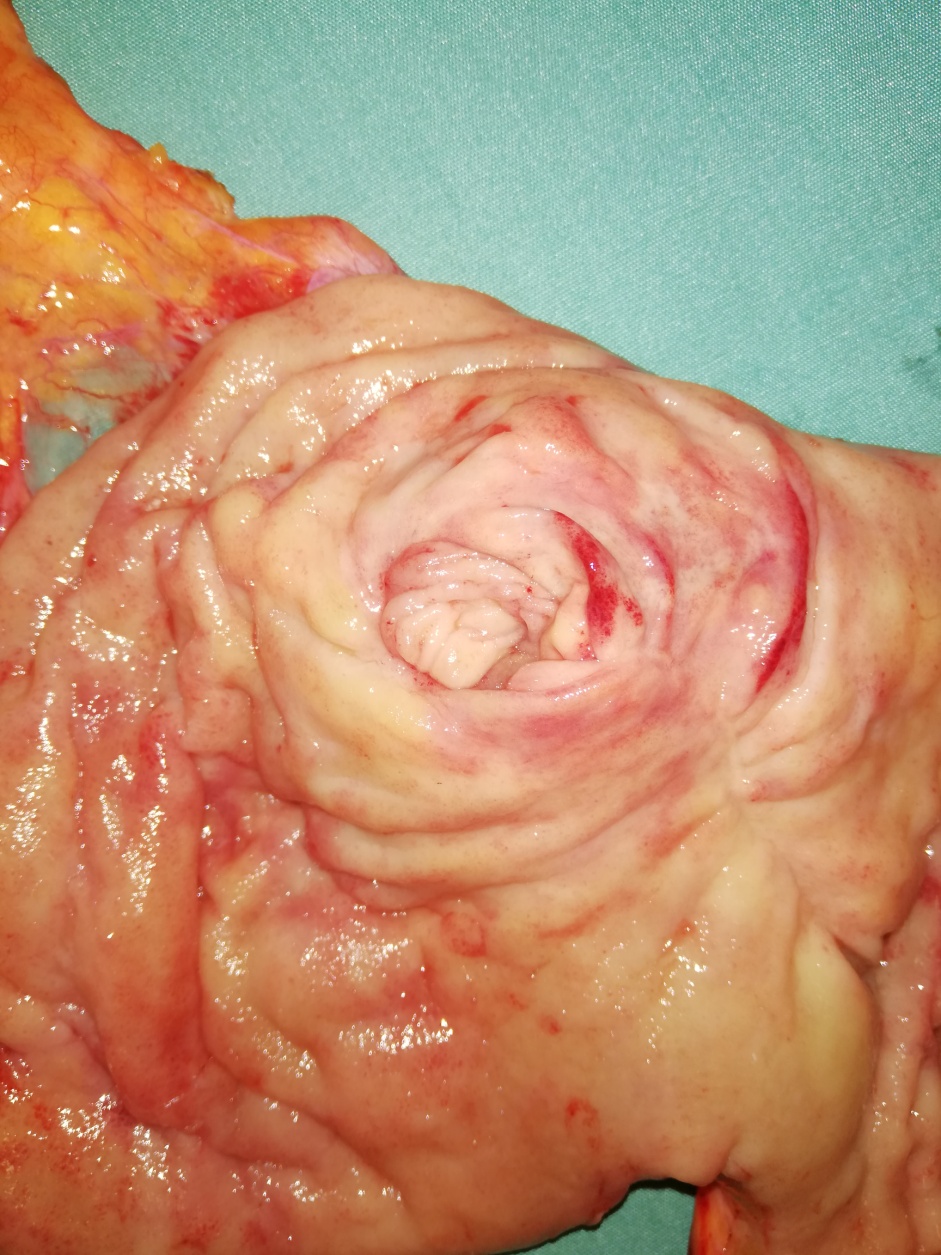
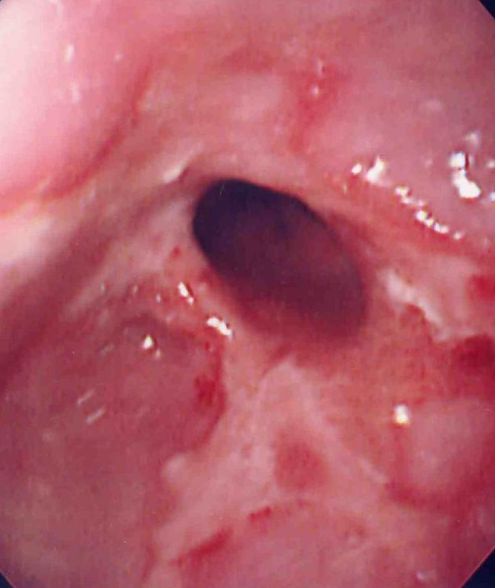
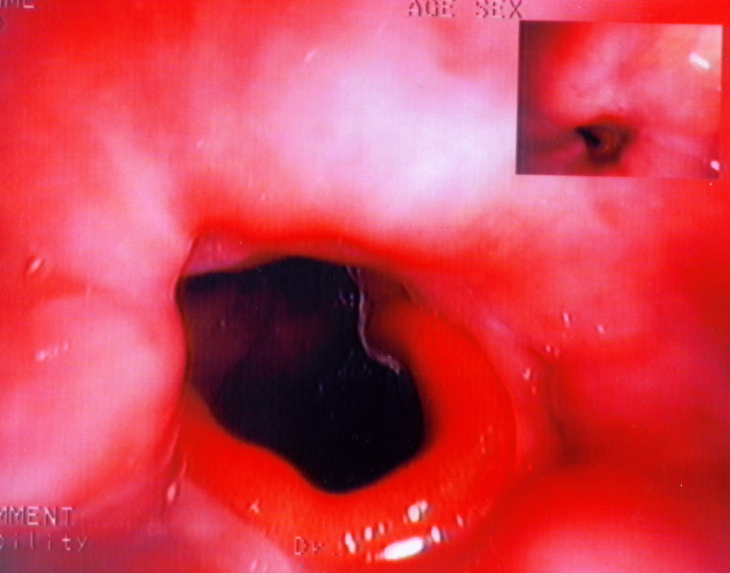
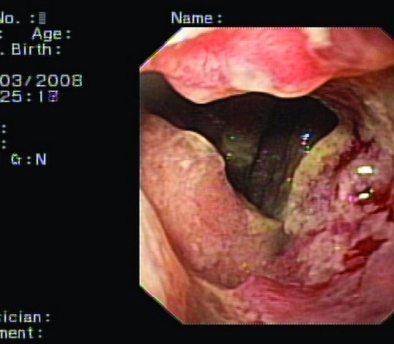
Gastroscopy image showing the normal gastric lumen (green arrow) and the fistula orifice (red arrow). ( Courtesy Dr . V . Penopoulos ) .
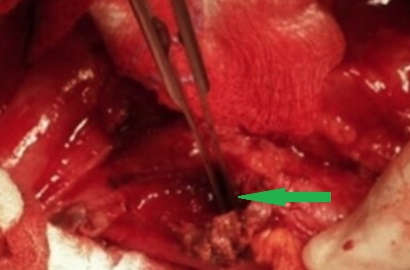
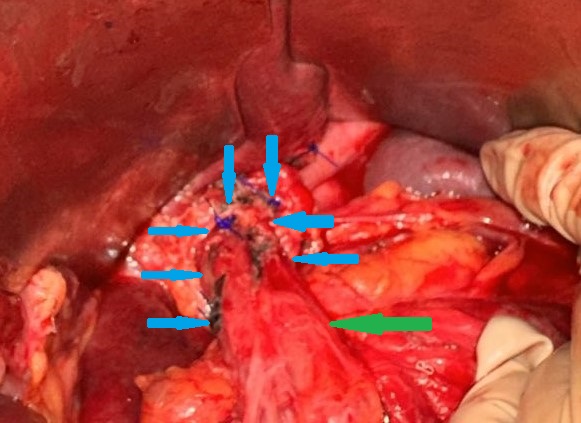
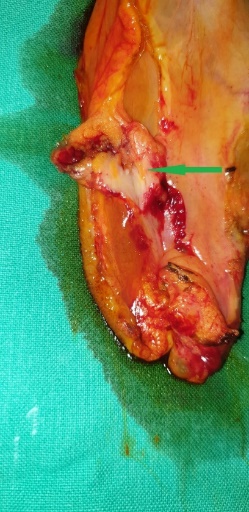
The fistulous opening in the diaphragm is shown by the green arrow.( Courtesy Dr . V . Penopoulos ) .

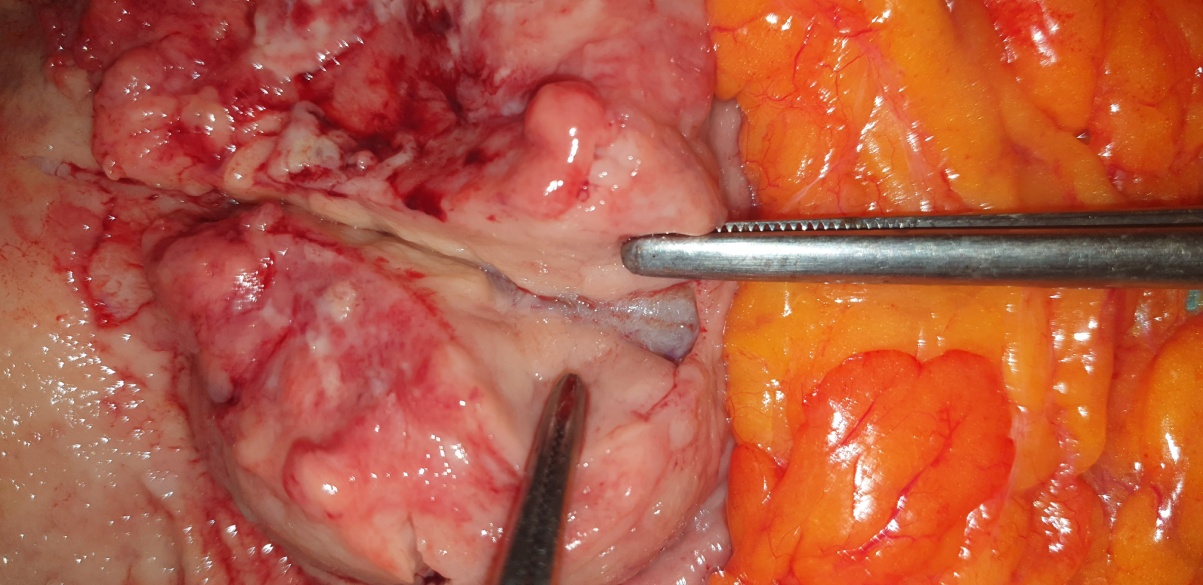
The fistula shown by green arrow ,following separation of the proximal stomach from the diaphragm.( Courtesy Dr . V . Penopoulos ) .
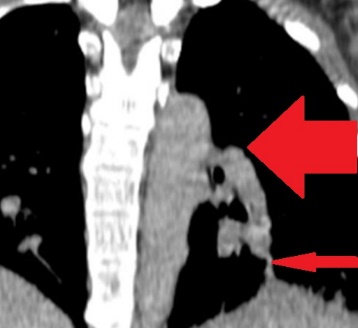
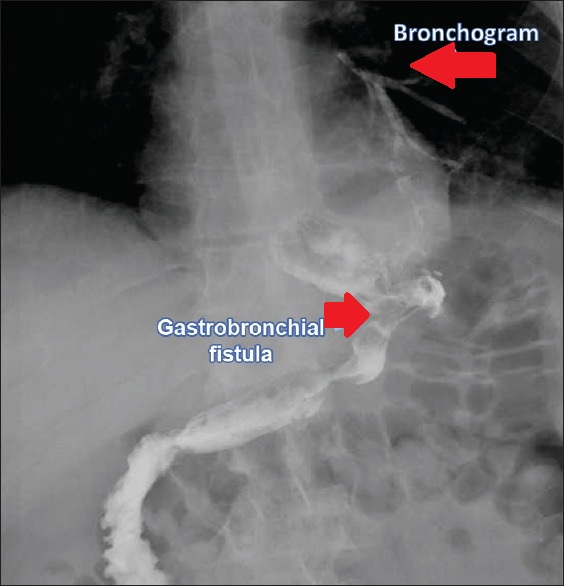
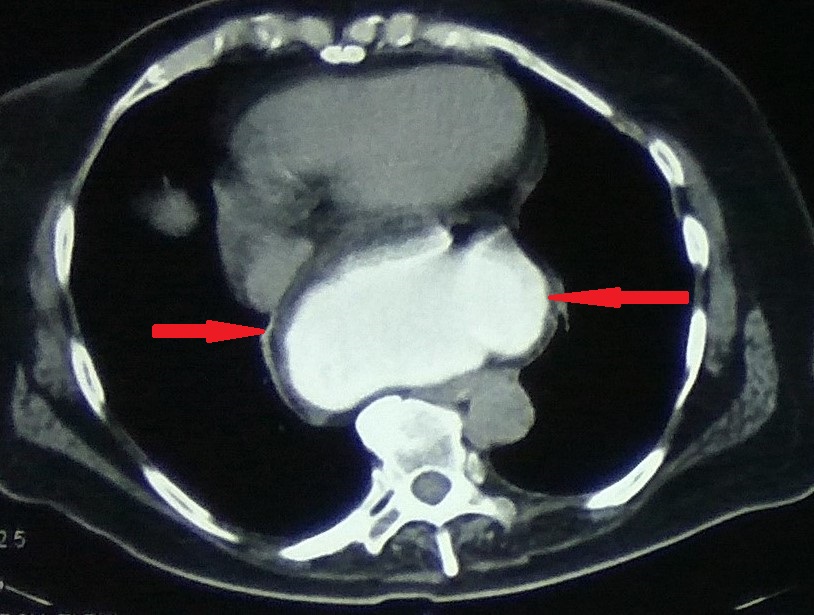
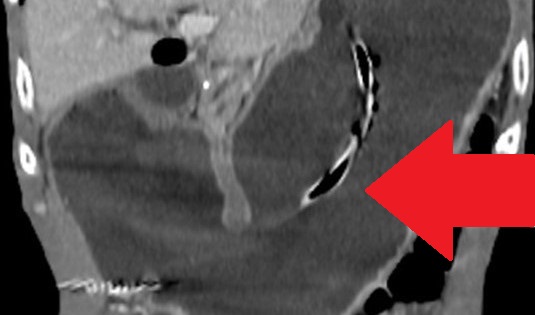
Coronal view of a chest computed tomography scan with gastrografin swallow showing back flow of contrast from the digestive tract to the left bronchus (red arrows) with left lung lower lobe phlegmon. ( Courtesy Dr . V . Penopoulos ) .
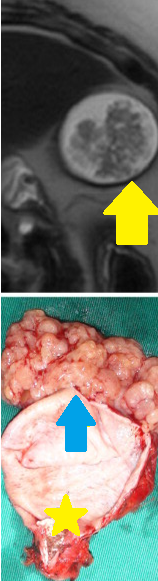
Gastrectomy specimen. Green arrow - Mucus Adenocarcinoma. Blue arrow - Neuroendocrine Carcinoma

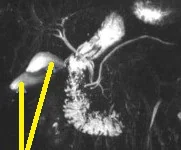
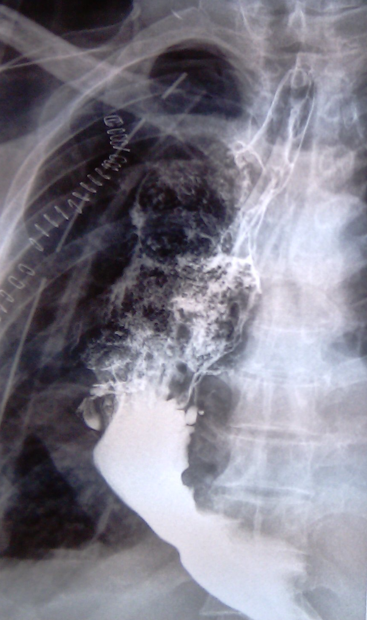
Gastrografin swallow showing an opacification of fistula between fundus of stomach and left lower bronchus.( Courtesy Dr . V . Penopoulos ) .
The jejunal interposition loop is clearly seen ( Merendino’s technique ) (Courtesy Dr. V. Penopoulos)
White arrows indicate the leak from the posterior esophageal wall (Courtesy Dr. V. Penopoulos)
Esophagography. Arrows demonstrate a small posterior pseudodiverticulum of the esophagus adjacent to the metallic plate and screws (Courtesy Dr. V. Penopoulos)
Esophagography. Arrows demonstrate a small posterior pseudodiverticulum of the esophagus adjacent to the metallic plate and screws (Courtesy Dr. V. Penopoulos)
Endoscopic image of esophagocolonic anastomosis.(Courtesy Dr. V. Penopoulos).
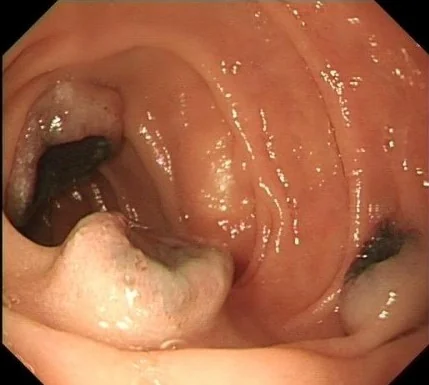
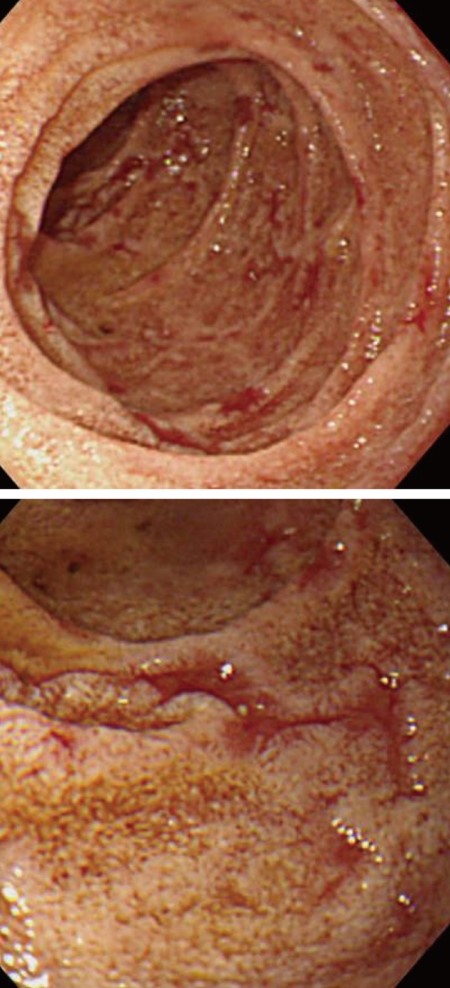
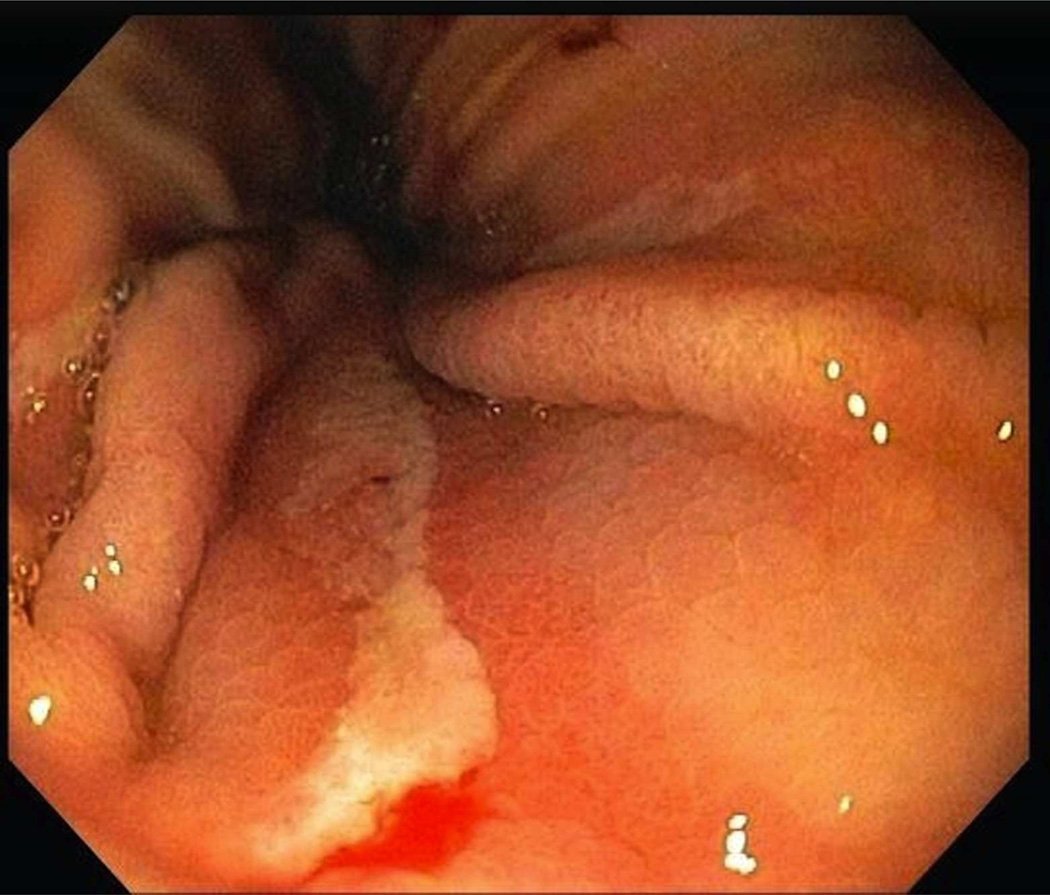
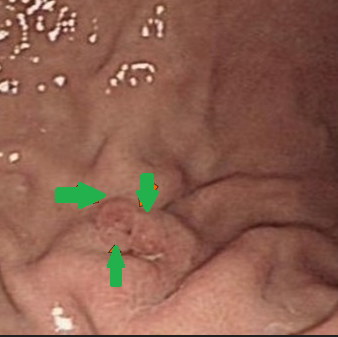
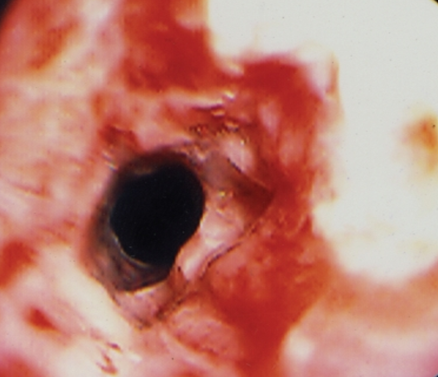
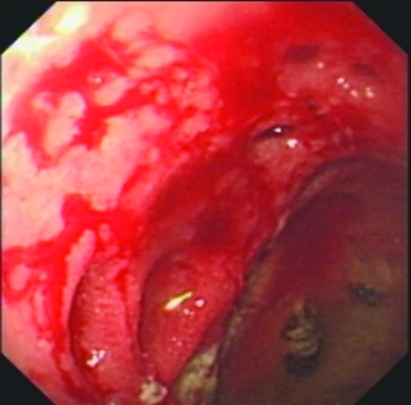
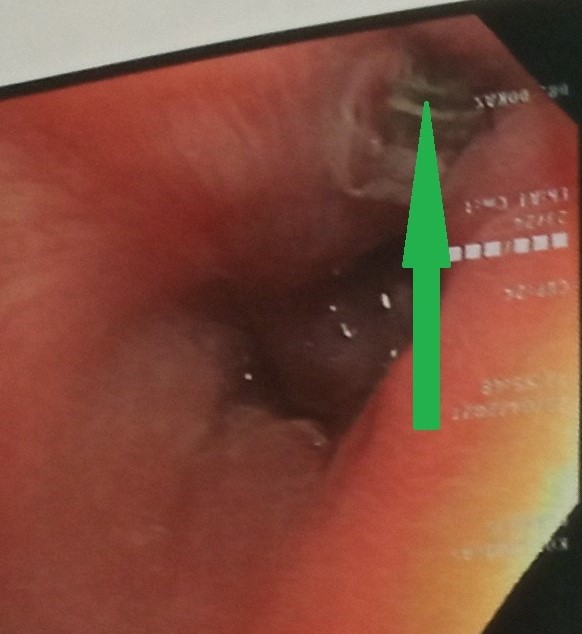
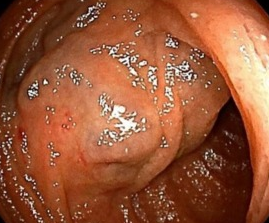
Upper gastrointestinal endoscopy showing a grossly deformed duodenal bulb. A steady trickle of bile was also seen to come from a slit-like orifice on the anterior duodenal wall suggestive of biliary duodenal fistula (green arrow)
Complete mobilization of the upper esophagus and encirclement with Penrose drains (Courtesy Dr. V. Penopoulos)
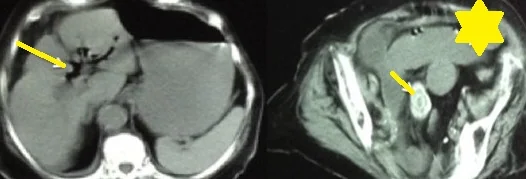
Contrast-enhanced CT of the abdomen, revealing air in intrahepatic biliary tree (pneumobilia) (red arrow)
Esophagoscopy. Green arrow: Esophageal pseudodiverticulum (Courtesy Dr. V. Penopoulos)

Adenosquamous carcinoma of the upper third of esophagus.(Courtesy Dr. V. Penopoulos).
Adenosquamous carcinoma of the gastroesophageal junction.(Courtesy Dr. V. Penopoulos).
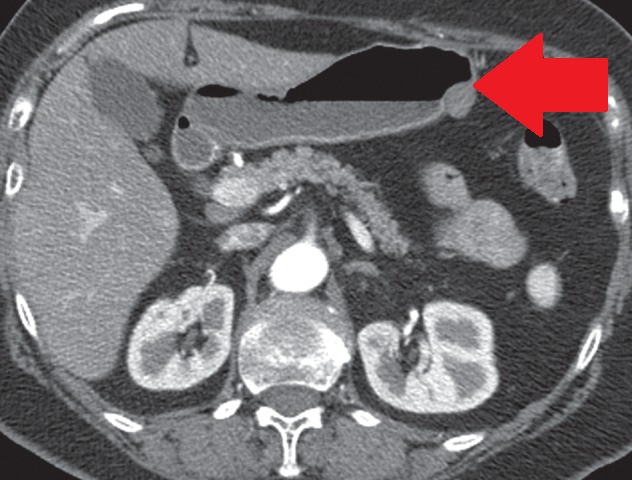
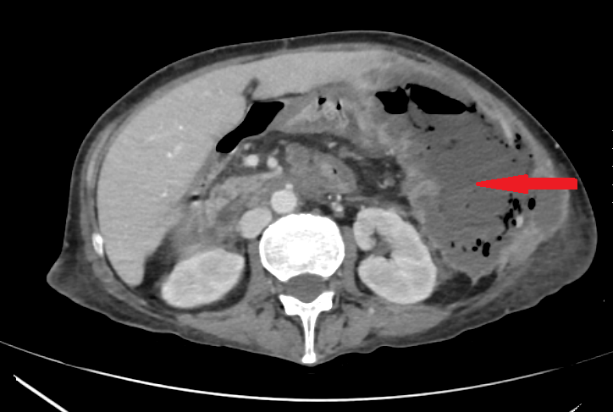
Contrast-enhanced CT of the abdomen, revealed a grossly distended stomach with mild diffuse thickening of its wall (red arrow)
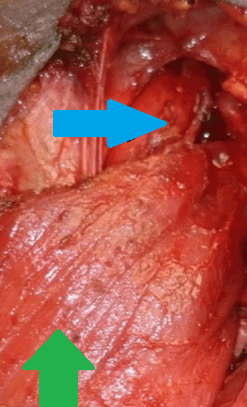
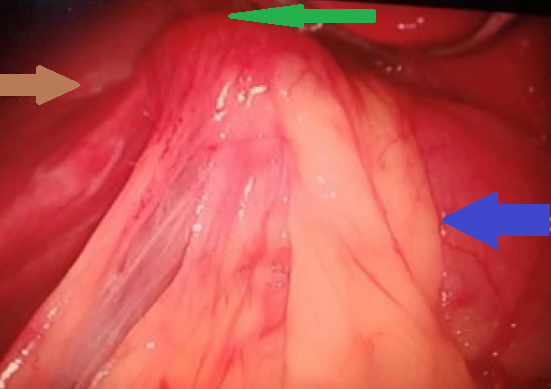
Green arrow - Sternocleidomastoid muscle prior to wrapping.Blue arrow - Esophagus. (Courtesy Dr.V.Penopoulos).


Adenosquamous carcinoma of the middle third of the esophagus (Courtesy Dr. V. Penopoulos)

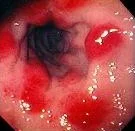
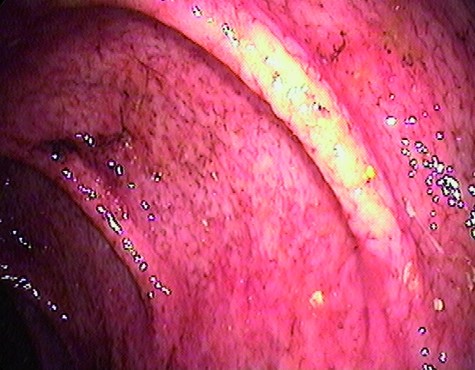
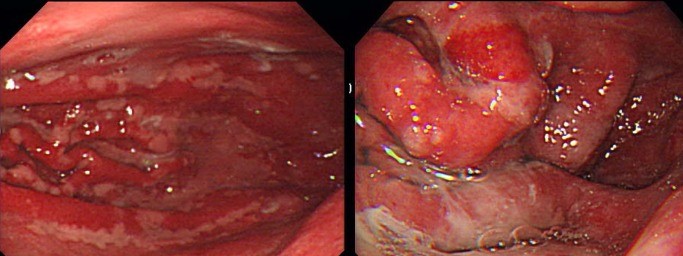
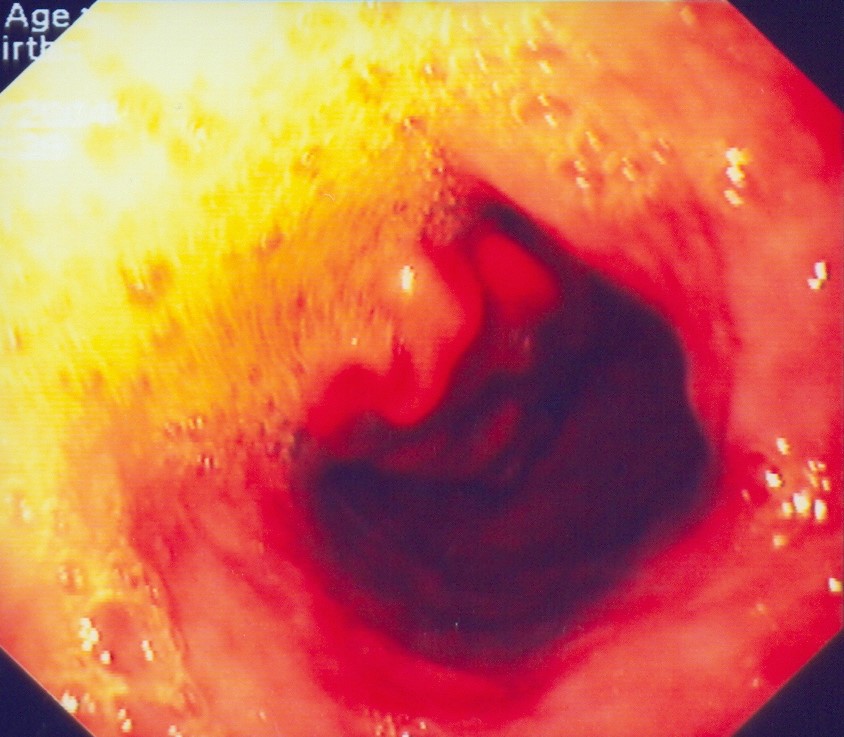
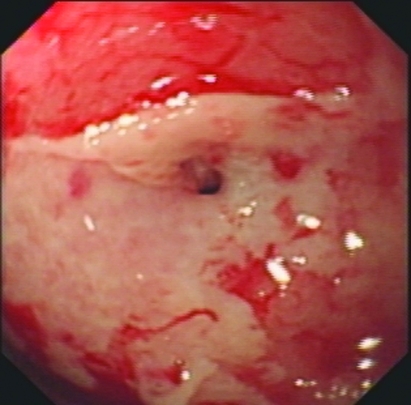
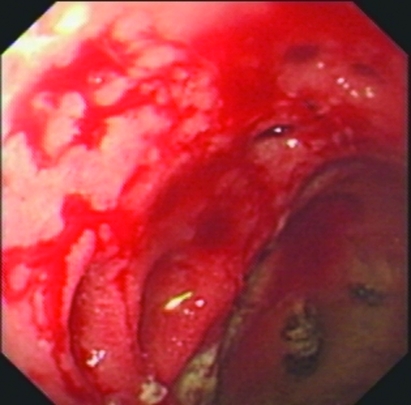
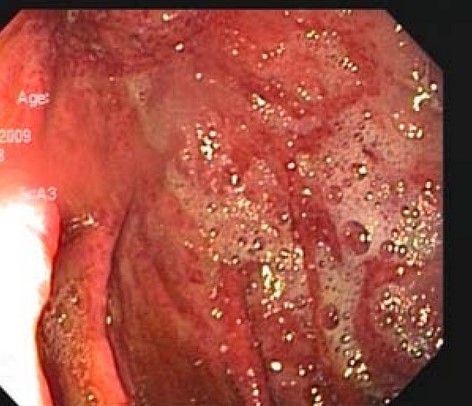
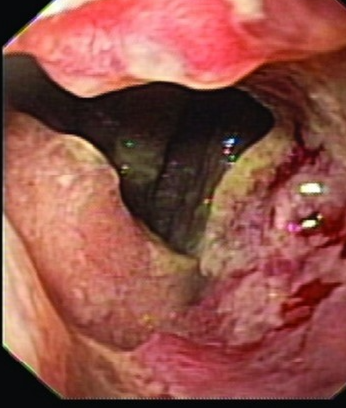
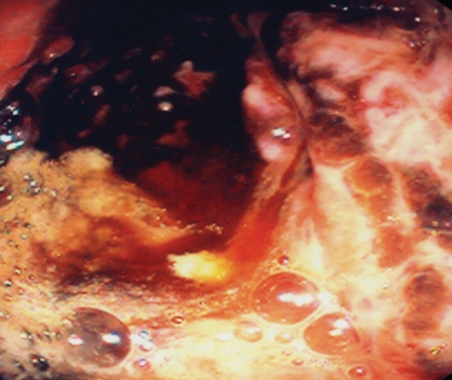
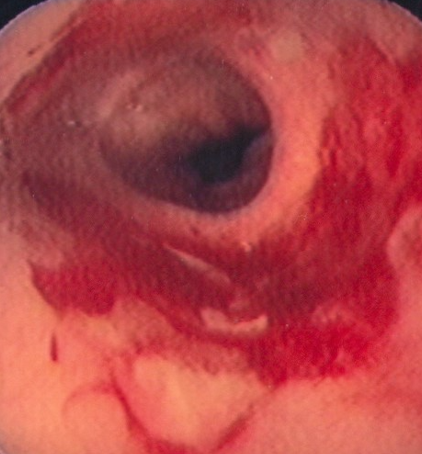
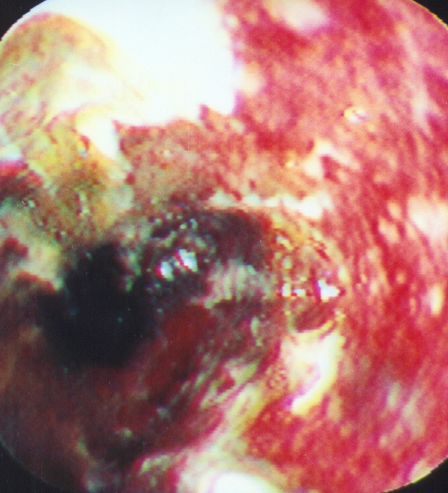
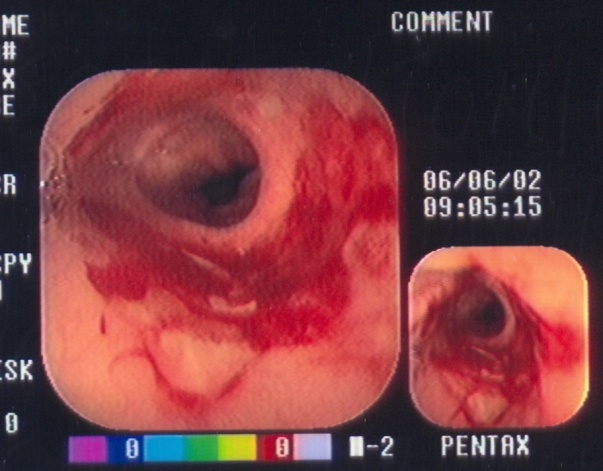
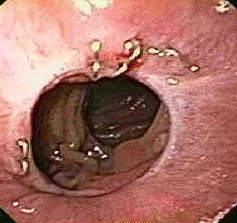
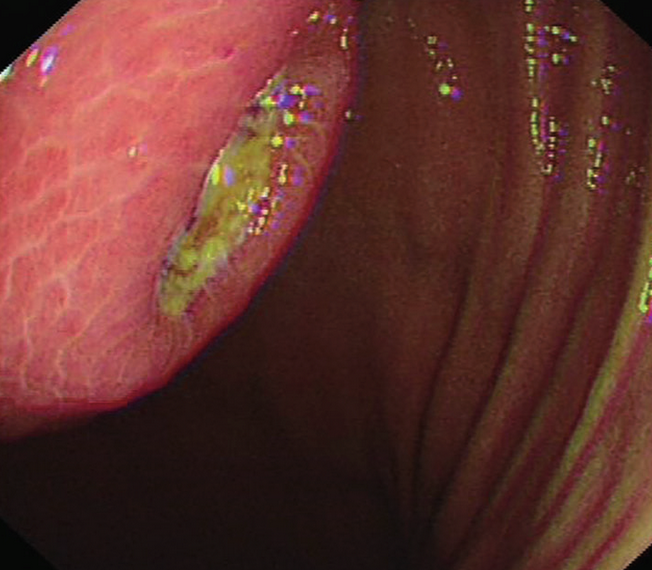
Endoscopy.Diffuse erosion and erythema in the lower esophagus.(Courtesy Dr.T.Maris).

Esophagojejunal anastomosis - endoscopic image on the 30th postoperative day (Courtesy Dr. V. Penopoulos).


Normal jejunojejunal anastomosis (lower Roux anastomosis) (Courtesy Dr. V. Penopoulos).

Green arrow-Large bowel.Purple arrows-Proximal jejunal loops invaded by the colonic carcinoma.(Courtesy Dr.V.Penopoulos).



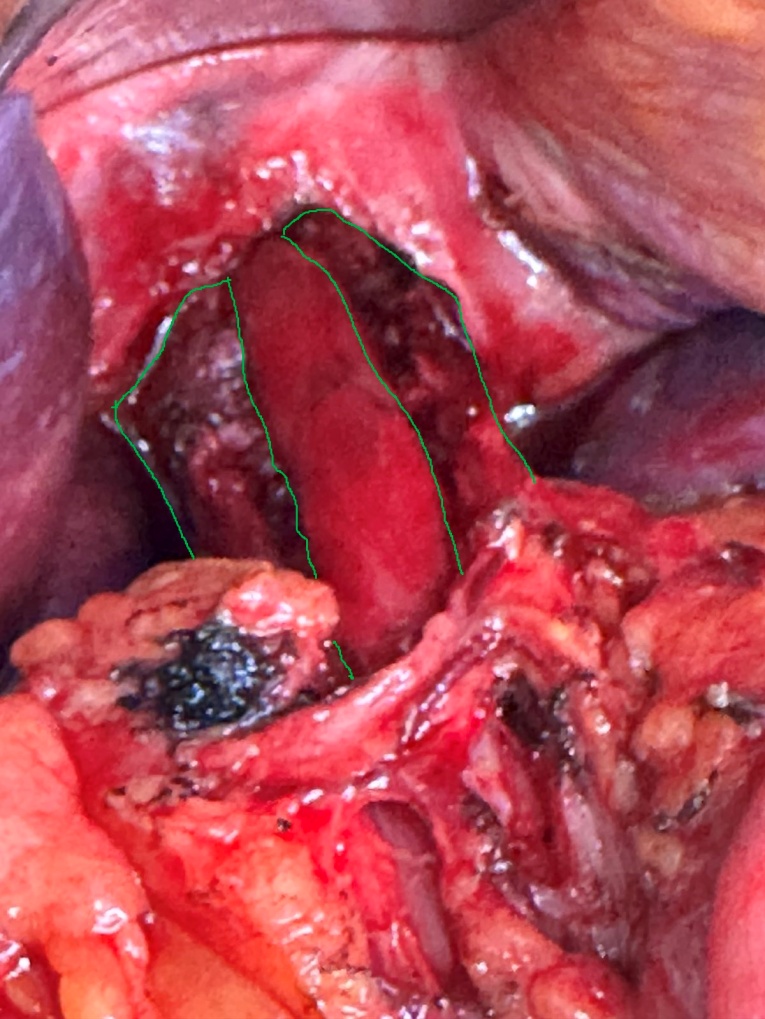
Postoperative image of long myotomy. Green outline — the divided muscular layers of the esophagus. The esophageal mucosa is exposed at the center. The myotomy extends onto the stomach (Courtesy Dr. V. Penopoulos)
Barium swallow. Red arrow — previous Nissen fundoplication. Yellow arrow — narrowed distal esophagus with tapering of its terminal segment. Green outline — right paraesophageal hiatal hernia (Courtesy Dr. V. Penopoulos)

Green arrows — reconstruction of the Nissen fundoplication (Courtesy Dr. V. Penopoulos)



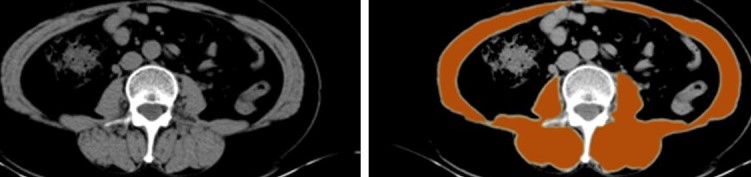
Abdominal CT scan. Distended small bowel loops with fluid content (Courtesy Dr. V. Penopoulos)
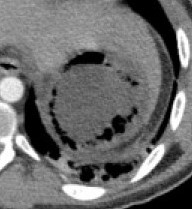
Abdominal CT scan. Ruptured abdominal aortic aneurysm. (Courtesy Dr. V. Penopoulos).

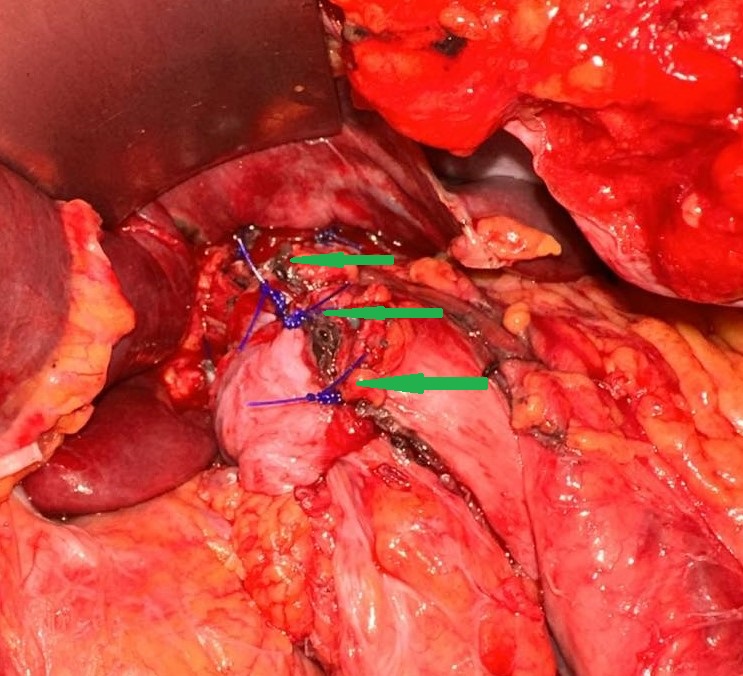
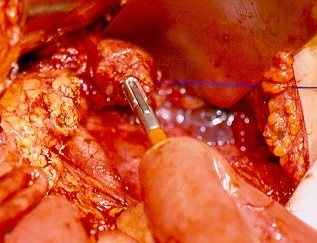
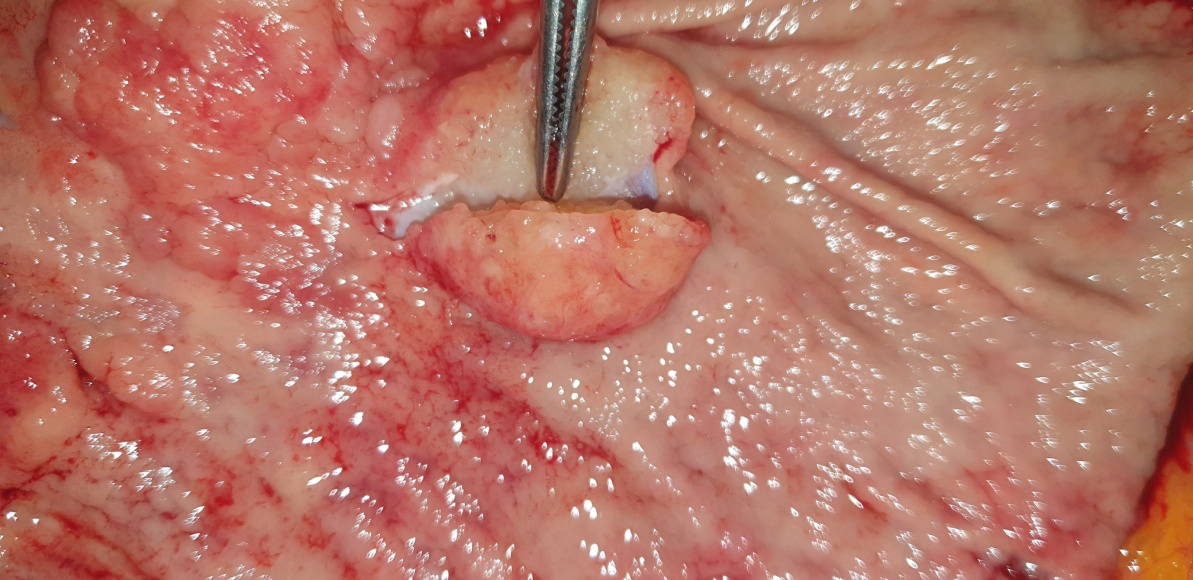
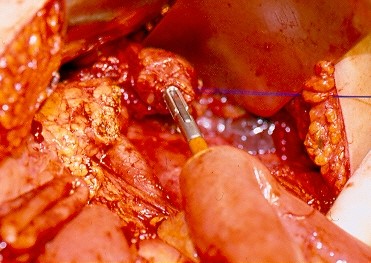
Anatomical forceps within the fistula orifice in the duodenum (Courtesy Dr. V. Penopoulos)
Green arrow - Fistula.Yellow arrow - The interior of the opened aneurysmal sac. (Courtesy Dr. V. Penopoulos).
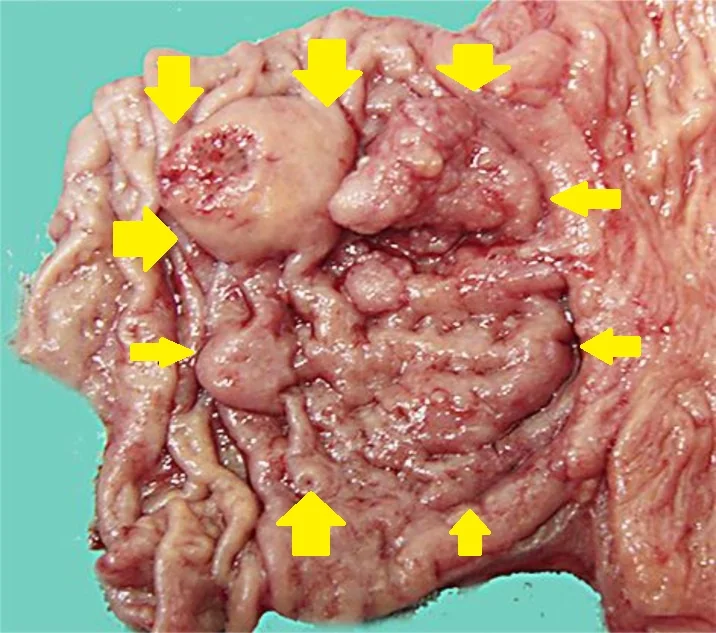
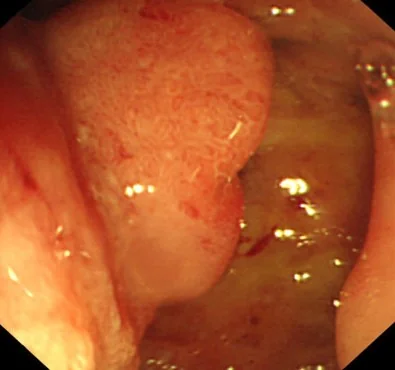
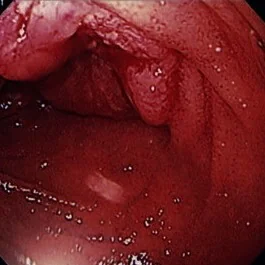
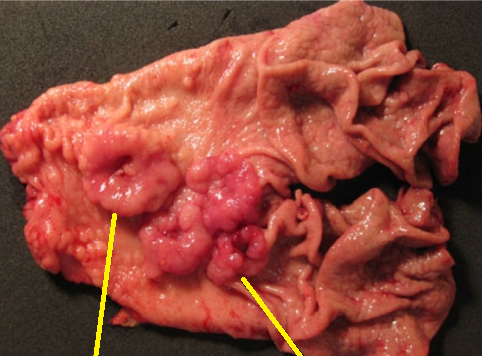
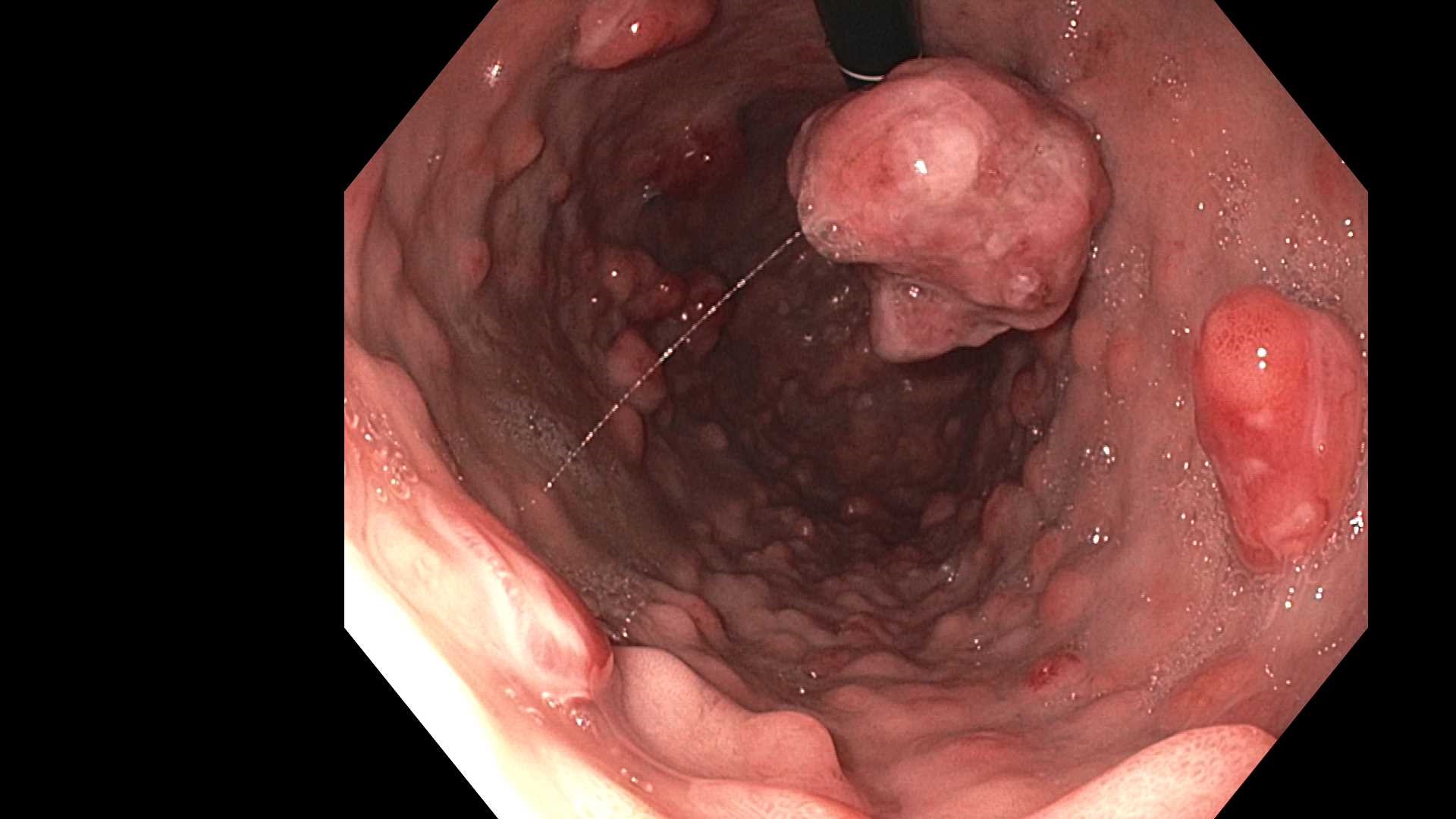
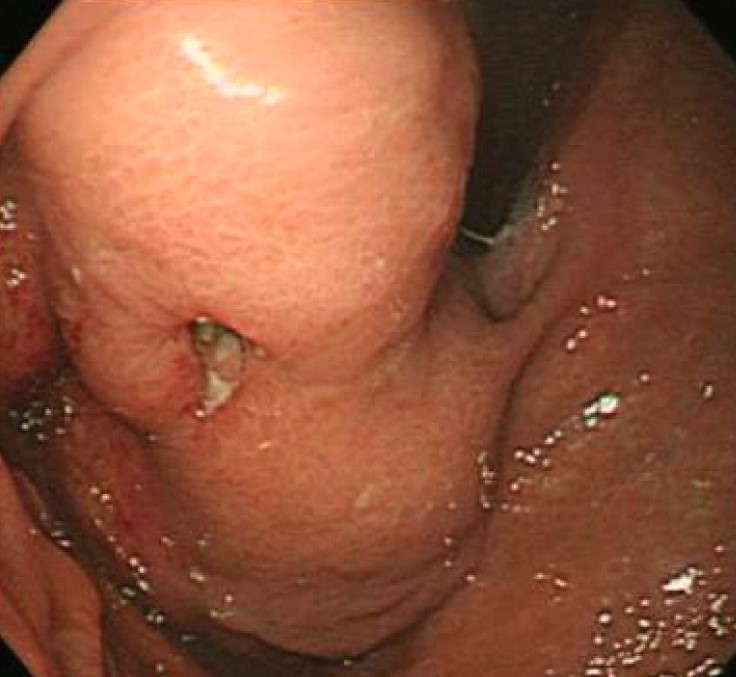
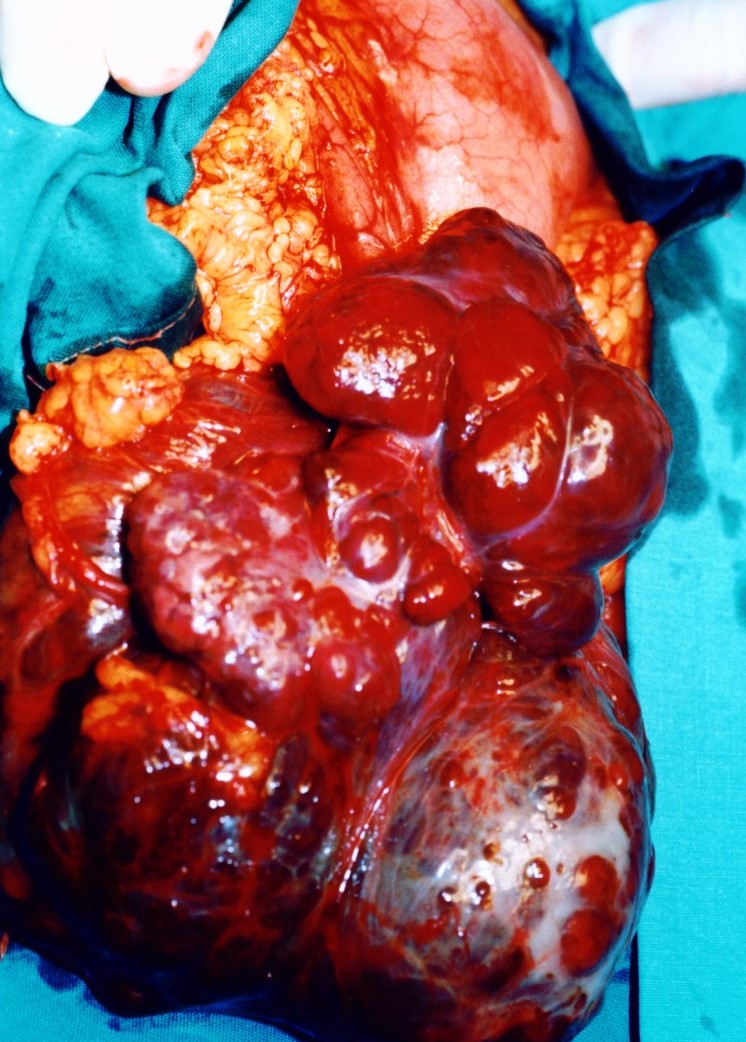
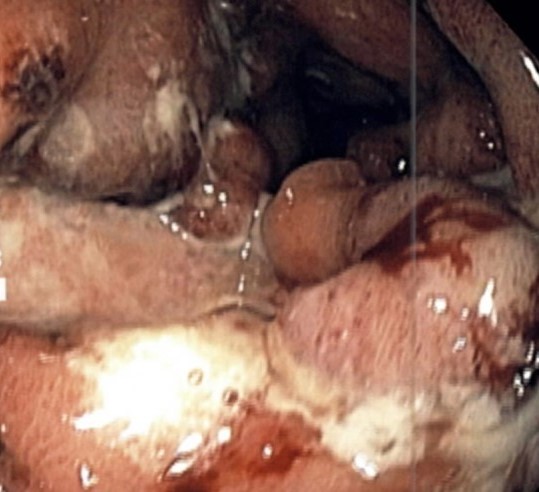
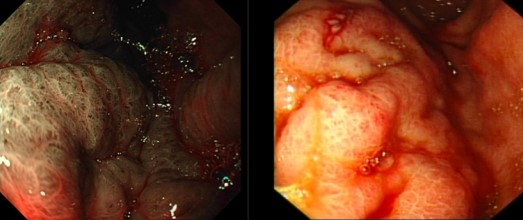
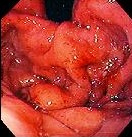
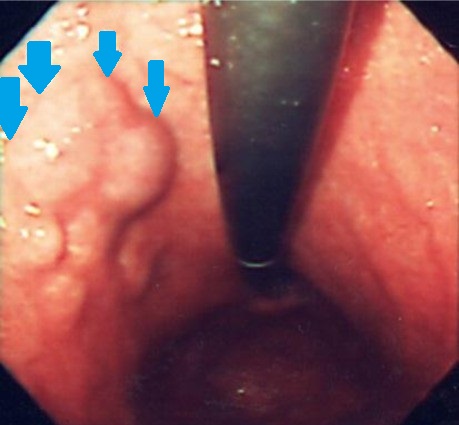
Endoscopic image - Multiple gastric stromal tumors.(Courtesy Dr. V. Penopoulos).




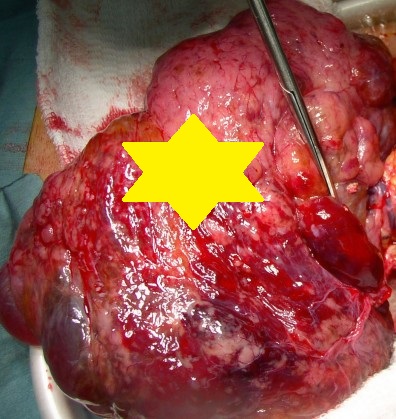
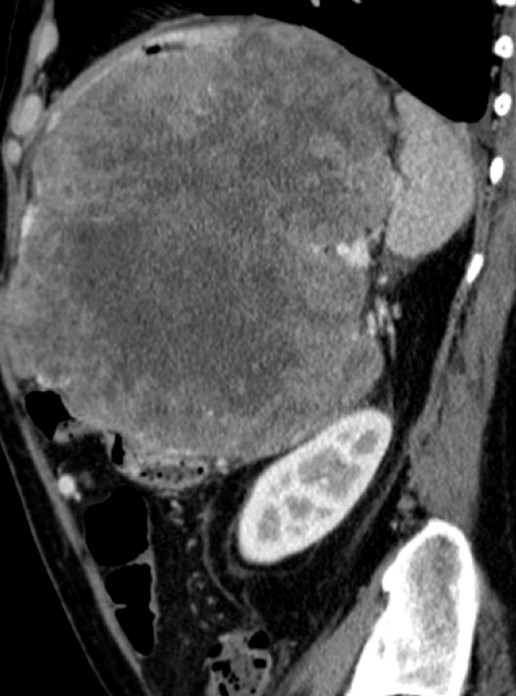
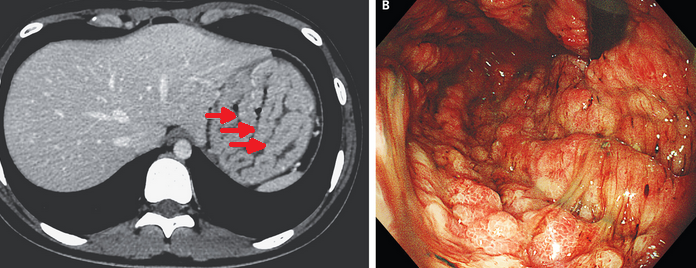
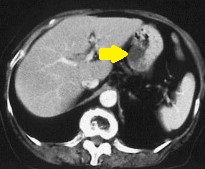
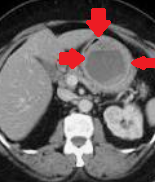
Abdominal CT Scan . Red arrow - Gastric stromal tumor. (Courtesy Dr.V.Penopoulos).
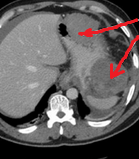
Abdominal CT Scans . Red arrows - Gastric stromal tumors. (Courtesy Dr.V.Penopoulos).

Endoscopic images of multiple gastric stromal tumors.(Courtesy Dr.V.Penopoulos).

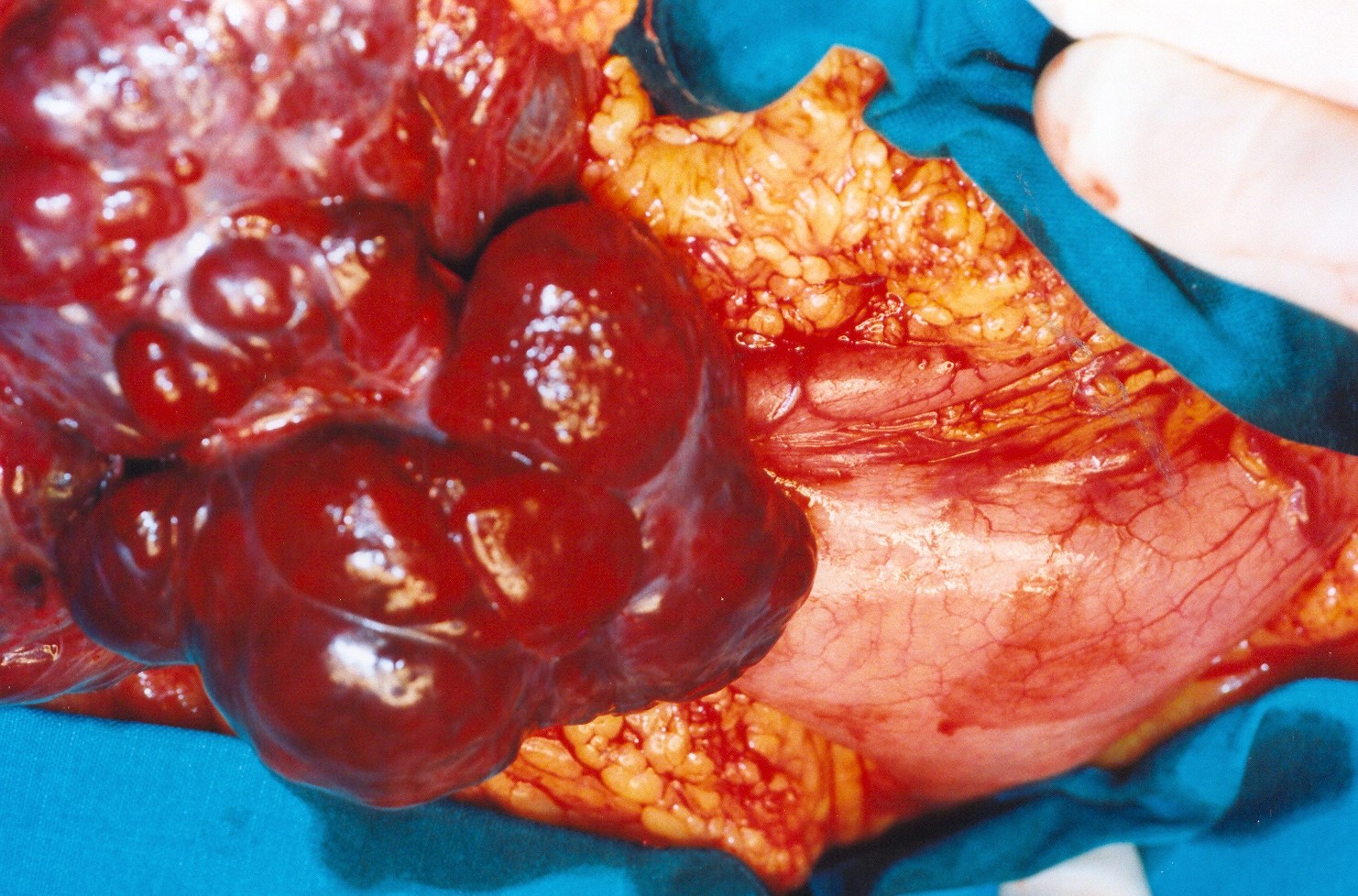
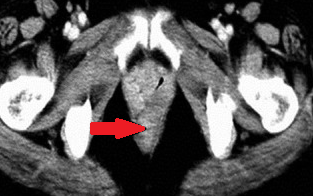
Rectal stromal tumor.Red arrows-Multiple liver secondary deposits.(Courtesy Dr.V.Penopoulos).
Abdominal CT Scans . Red arrows - Gastric stromal tumors. (Courtesy Dr.V.Penopoulos).

Endoscopic images of multiple gastric stromal tumors.(Courtesy Dr.V.Penopoulos).
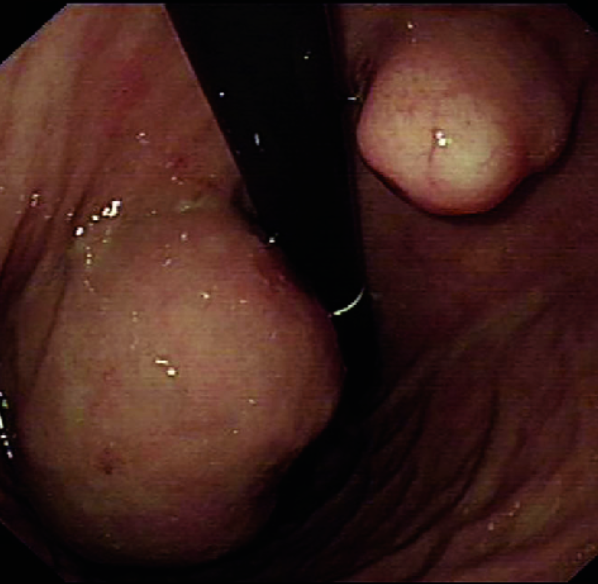
Endoscopic images of multiple gastric stromal tumors.(Courtesy Dr.V.Penopoulos).
Endoscopic images of multiple gastric stromal tumors.(Courtesy Dr.V.Penopoulos).

Endoscopic images of multiple gastric stromal tumors.(Courtesy Dr.V.Penopoulos).
Abdominal CT Scan . Red arrow - Gastric stromal tumor. (Courtesy Dr.V.Penopoulos).
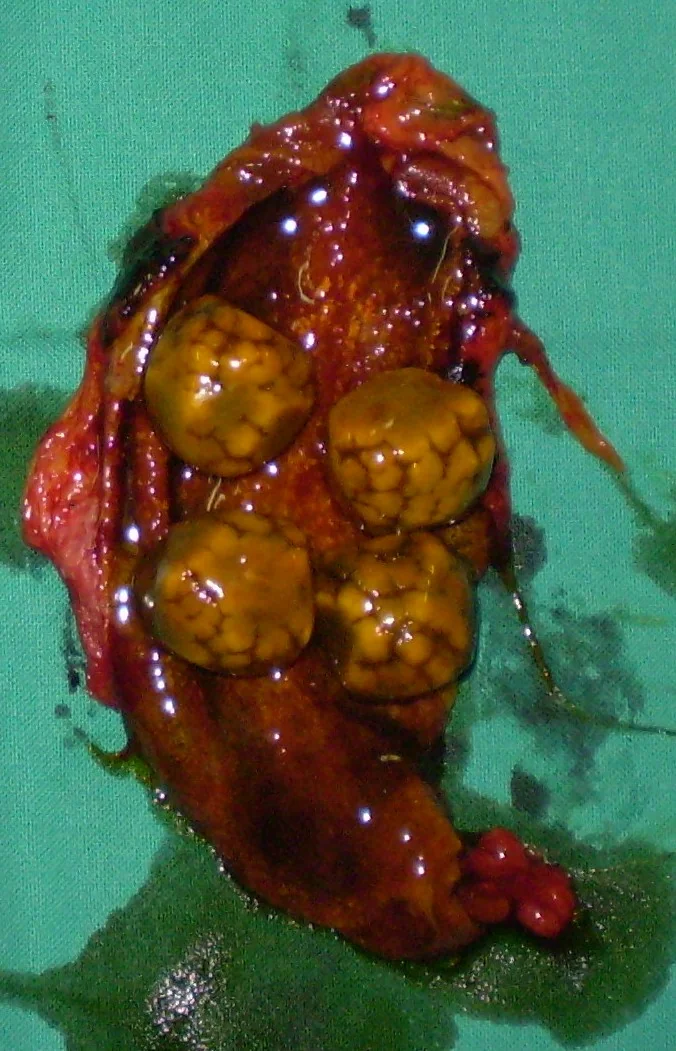
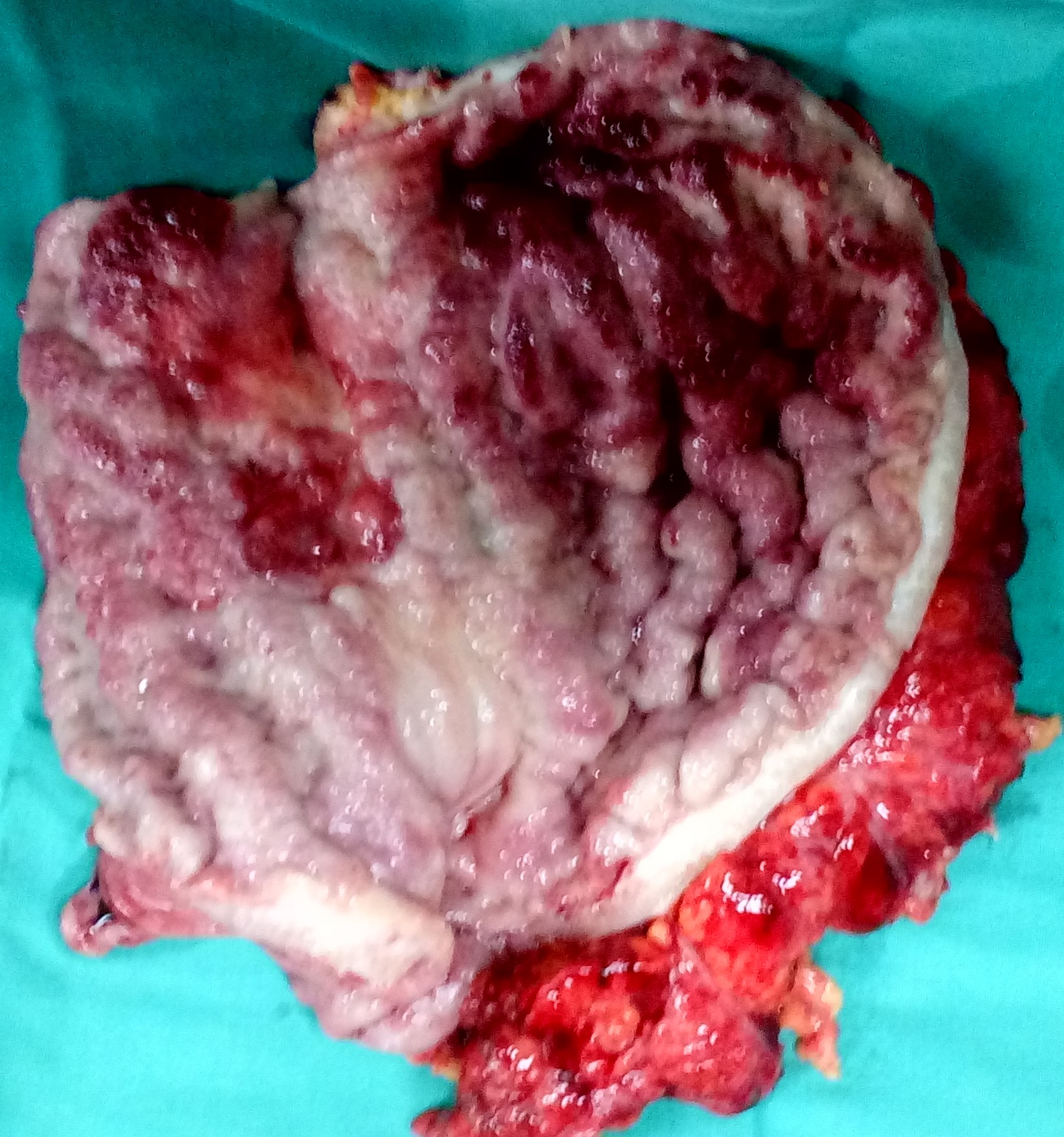
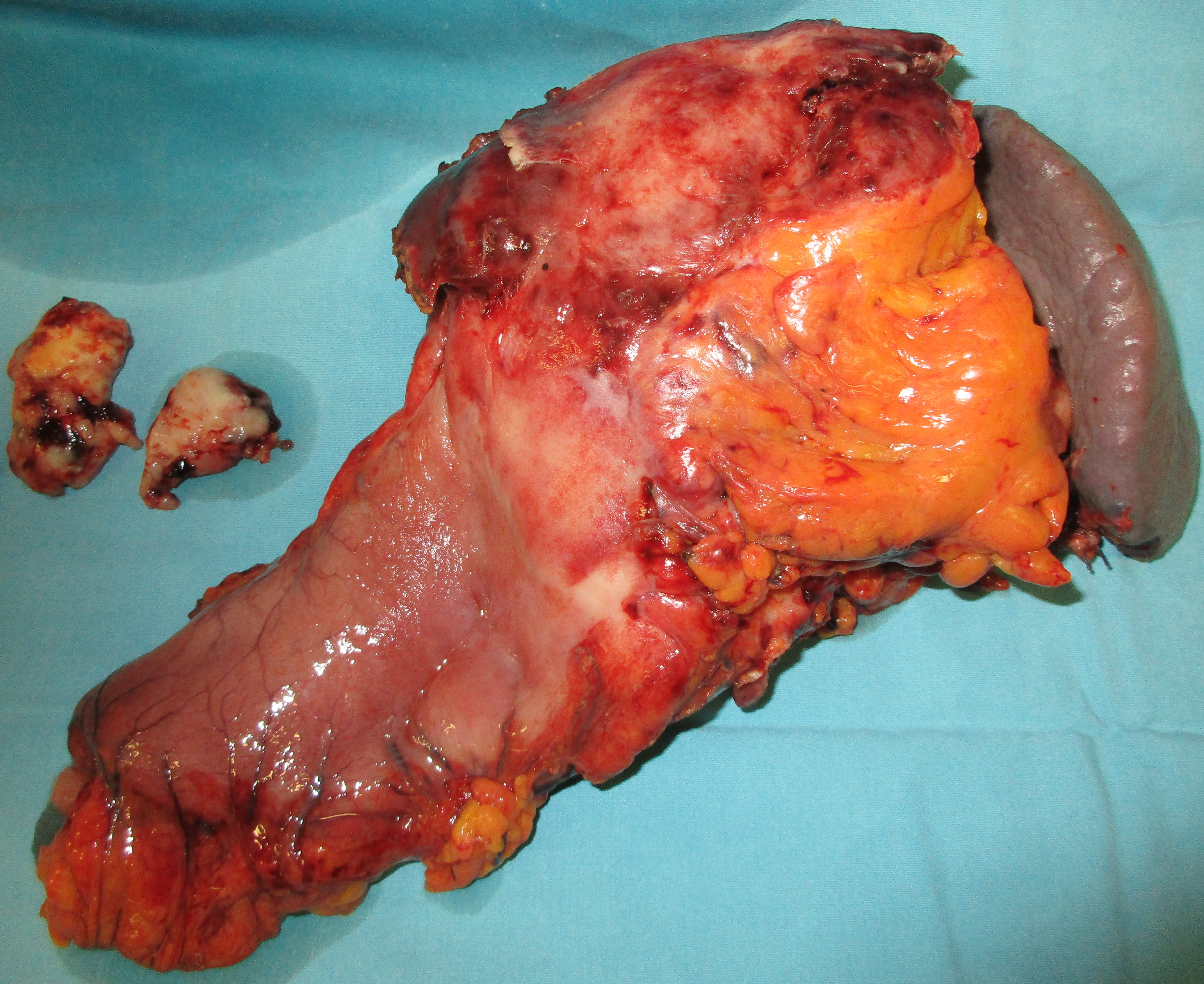
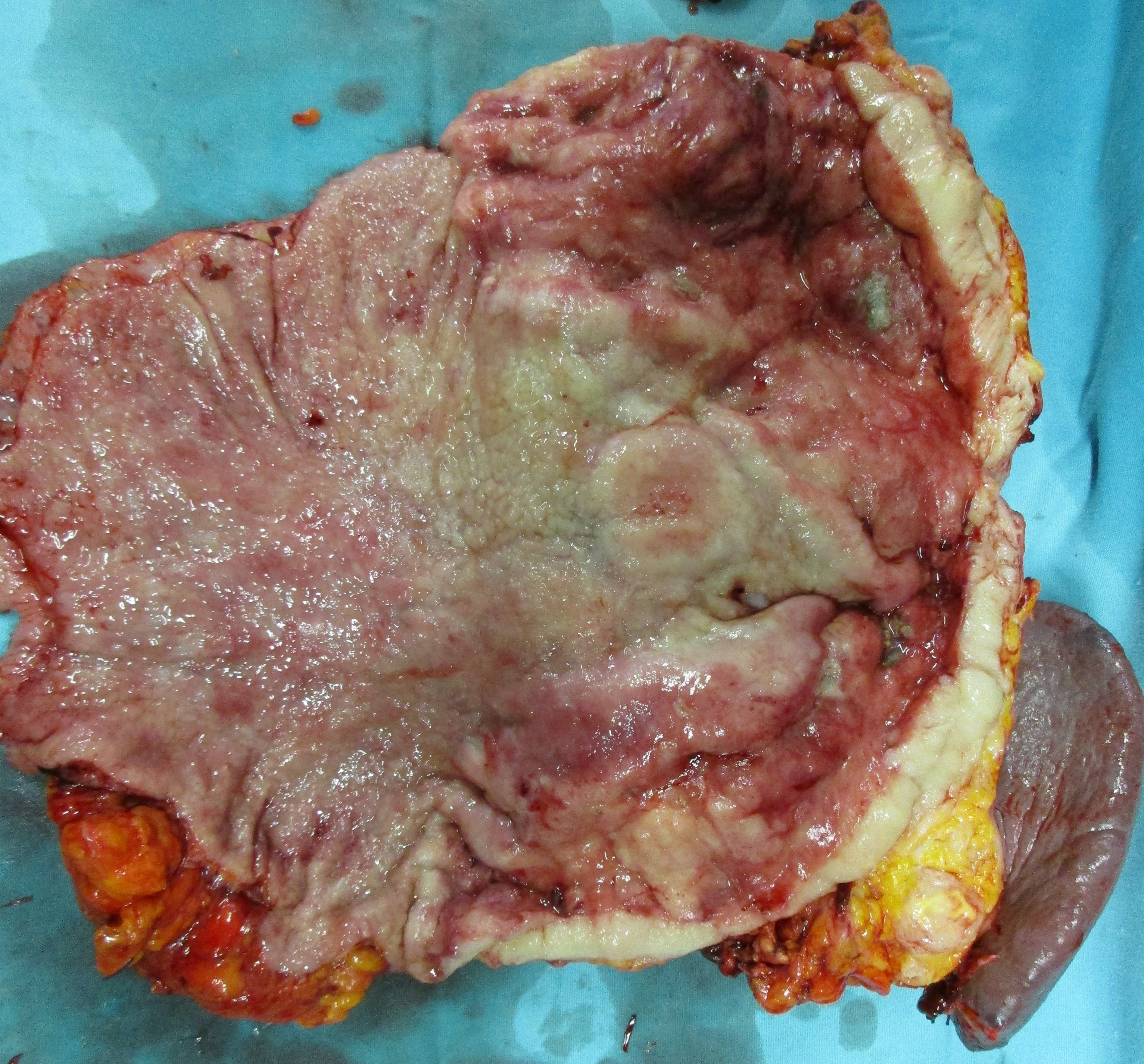
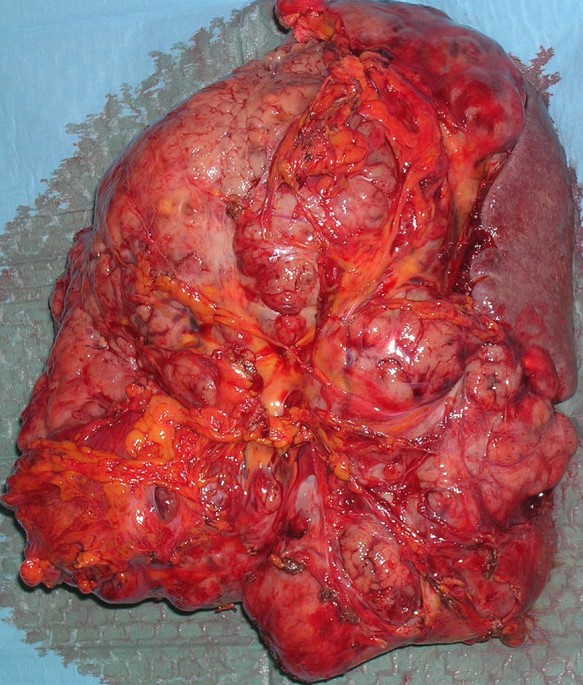
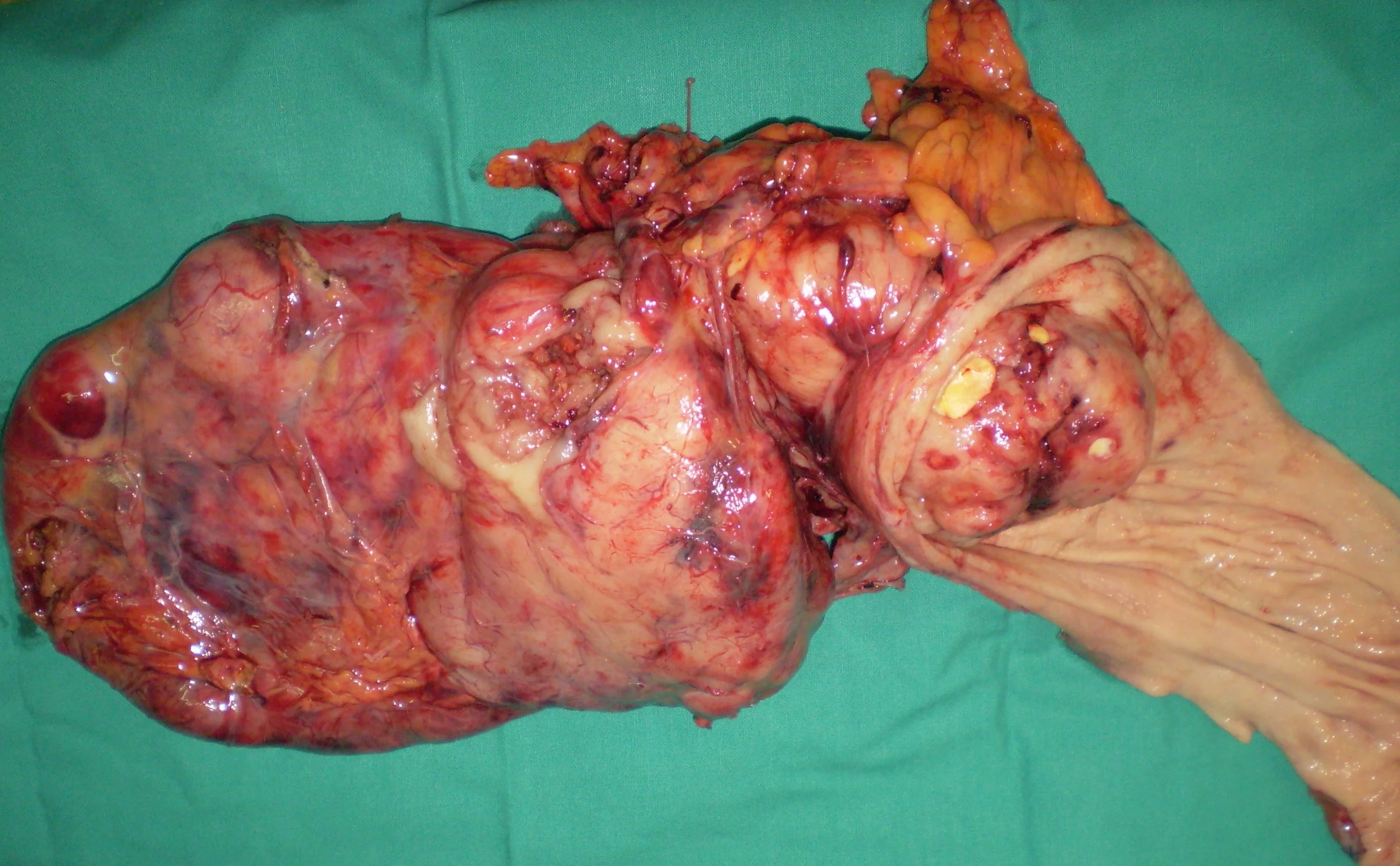
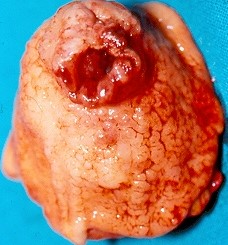
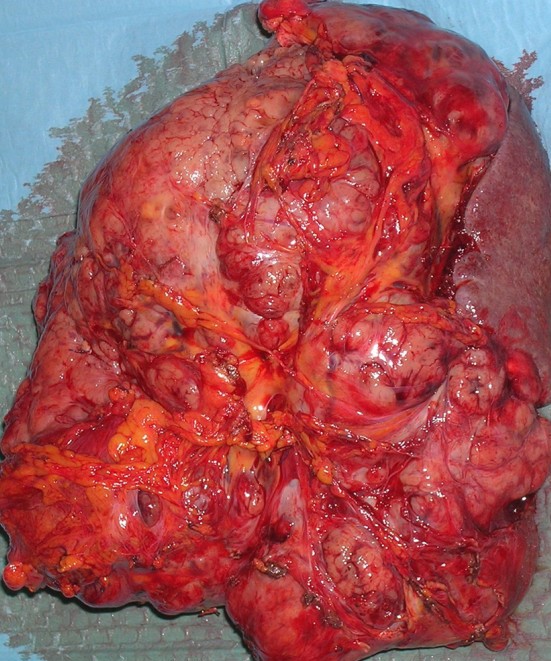
Total gastrectomy specimen. Brown arrows – Multiple gastric stromal tumors (Courtesy Dr. V. Penopoulos)