Καρκίνος Τυφλού μετά ΑΜΜΟ για Πολλαπλούν Μυέλωμα.
Cecal Carcinoma following autologous transplantation for Multiple Myeloma.

Εισαγωγή
ΑΝΑΠΤΥΞΗ ΔΙΗΘΗΤΙΚΟΥ ΚΑΡΚΙΝΟΥ ΤΥΦΛΟΥ ΜΕΤΑ ΑΠΟ ΑΥΤΟΜΕΤΑΜΟΣΧΕΥΣΗ ΓΙΑ ΠΟΛΛΑΠΛΟΥΝ ΜΥΕΛΩΜΑ . ΑΝΑΚΟΙΝΩΣΗ ΜΟΝΑΔΙΚΗΣ ΠΕΡΙΠΤΩΣΗΣ ΚΑΙ ΑΝΑΣΚΟΠΗΣΗ ΤΗΣ ΒΙΒΛΙΟΓΡΑΦΙΑΣ . ΒΑΣΙΛΕΙΟΣ ΠΕΝΟΠΟΥΛΟΣ – ΓΕΝΙΚΟΣ ΧΕΙΡΟΥΡΓΟΣ . ΔΕΣΠΟΙΝΑ ΣΓΟΥΡΙΔΗ – ΓΕΝΙΚΟΣ ΧΕΙΡΟΥΡΓΟΣ . Β’ ΧΕΙΡΟΥΡΓΙΚΗ ΚΛΙΝΙΚΗ – Γ . Ν . Θ . «Γ . ΠΑΠΑΝΙΚΟΛΑΟΥ» .
Το πολλαπλούν μυέλωμα ( ΠΜ ) , αποτελεί μία κακοήθεια των πλασματοκυττάρων , η οποία χαρακτηρίζεται από την ταχεία αναπαραγωγή των κλώνων των πλασματοκυττάρων , με αποτέλεσμα των παραγωγή μονοκλωνικών ανοσοσφαιρινών . Αν και τυπικά θεωρείται ανίατη ασθένεια εν τούτοις πρόοδοι στην θεραπευτικές επιλογές , έχουν επιφέρει σημαντικές βελτιώσεις στην επιβίωση των ασθενών αυτών . Ως νέες θεραπείες , θεωρούμε την αυτό-μεταμόσχευση και νεωτεριστικά φάρμακα , όπως τα ανοσο-τροποποιητικά φάρμακα και οι αναστολείς των πρωτεασωμάτων ( κυτταρικές κατασκευές που διασπούν πρωτείνες ) . Η χορήγηση melphalan , σε υψηλές δόσεις , σαν μονοθεραπεία , ήταν το συχνότερο ( 81% ) θεραπευτικό σχήμα . Από το 1990 μέχρι και το 2010 , νεότερα φάρμακα , χρησιμοποιήθηκαν πριν από την μεταμόσχευση στο 69% των ασθενών , συμπεριλαμβανομένων της thalidomide στο 34%, lenalidomide στο 14%, και του bortezomib στο 21% . Μετά την μεταμόσχευση , η θεραπεία συντήρησης περιελάμβανε , την thalidomide (15%) , lenalidomide (11%) , bortezomib (9%) , και την interferon (6%). Οι περισσότεροι ασθενείς ( 59% ) υποβάλλονται σε μεταμόσχευση μετά παρέλευση 6 έως 12 μηνών από την διάγνωση της νόσου , 27% μετά παρέλευση 6μήνου και τέλος 14% μεταξύ 12 και 18 μήνες μετά την διάγνωση . Οι ανοσοτροποποιητικοί παράγοντες , αποτελούν πλέον μέρος της ολοκληρωμένης θεραπείας του πολλαπλού μυελώματος . Καθώς όλο και περισσότερα στοιχεία , συγκεντρώνονται αναφορικά με την αποτελεσματικότητα τους , συνεχίζουμε να μαθαίνουμε περισσότερα για τους κινδύνους που σχετίζονται με αυτά . Ειδικότερα , υπάρχουν πολλές αναφορές που υποστηρίζουν , τους αυξημένους κινδύνους ανάπτυξης μιας δευτερογενούς πρωτοπαθούς κακοήθειας (ΔΠΚ) , μεταξύ των ασθενών που αντιμετωπίστηκαν μ’ αυτούς τους παράγοντες . Εάν λάβουμε υπ’ όψιν μας , τις επανειλημμένες βελτιώσεις στην επιβίωση , ως αποτέλεσμα της χρήσης αυτών των θεραπευτικών αγωγών , οι ασθενείς με πολλαπλούν μυέλωμα , θα συνεχίσουν να επιβιώνουν περισσότερο , «προσφέροντας» περισσότερο χρόνο για την ανάπτυξη αυτών των κακοηθειών . Καθώς λοιπόν , το πολλαπλούν μυέλωμα , δεν θεωρείται μία ιάσιμη νόσος – με την σπάνια εξαίρεση της αλλογενούς μεταμόσχευσης βλαστοκυττάρων – οι πάροχοι θεραπειών , θα έρχονται ολοένα και συχνότερα με το δίλημμα , της επιλογής της κατάλληλης θεραπείας , για τους ασθενείς με πολλαπλούν μυέλωμα και δευτερογενείς πρωτοπαθείς κακοήθειες , καθώς οι θεραπευτικές επιλογές έχουν πολύ μικρή επικαλυπτόμενη αποτελεσματικότητα . Επομένως είναι σημαντικό , να καθορίσουμε , εάν ο αυξημένος κίνδυνος ανάπτυξης νέων καρκίνων , οφείλεται στην νόσο αυτή καθ’ εαυτή ή στην θεραπεία της. Αρκετές , αλλά όχι όλες , οι μελέτες υποστηρίζουν την ύπαρξη αυξημένου κινδύνου ανάπτυξης νέων καρκίνων , συμπεριλαμβανομένης της οξείας μυελογενούς λευχαιμίας ( ΟΜΛ ) του μυελοδυσπλαστικού συνδρόμου (ΜΔΣ ) και των δευτερογενών πρωτοπαθών κακοηθειών (ΔΠΚ) , σε ασθενείς με πολλαπλούν μυέλωμα , ανεξαρτήτως αν έτυχαν ή όχι αυτόλογης μεταμόσχευσης . Ως νέος καρκίνος , ορίζεται , ένας προηγούμενα μη ανιχνεύσιμος διηθητικός καρκίνος , ο οποίος εμφανίζεται μετά την μεταμόσχευση για τη αντιμετώπιση του πολλαπλού μυελώματος . Καρκίνοι in situ και άλλες προ-καρκινικές ανωμαλίες ( π.χ. ενδοεπιθηλιακή νεοπλασία από πλακώδες επιθήλιο ) εξαιρούνται / αποκλείονται . Παρουσιάζουμε την περίπτωση ενός ασθενούς , ο οποίος ανέπτυξε ένα διηθητικό αδενοκαρκίνωμα του τυφλού , ενώ ειχε προηγηθεί αυτομεταμόσχευση και ελάμβανε επαγωγική θεραπεία .
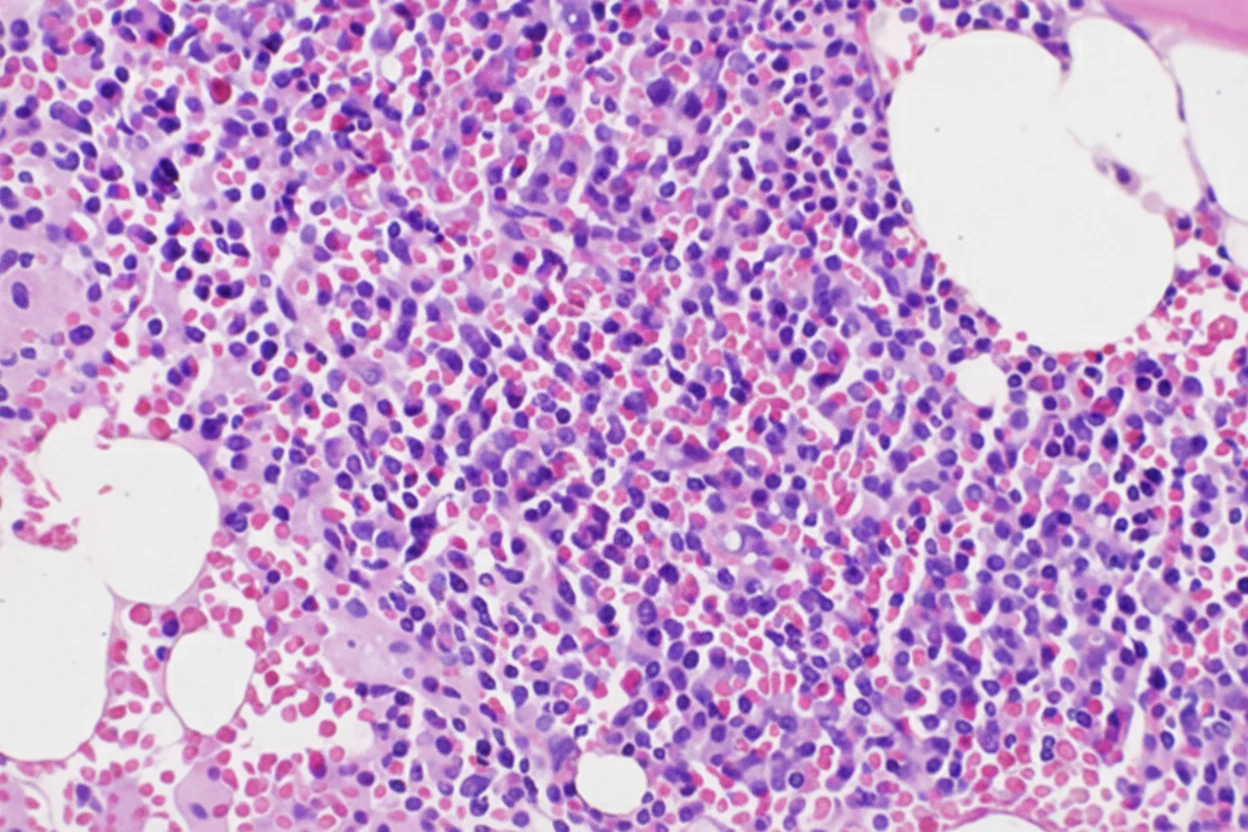
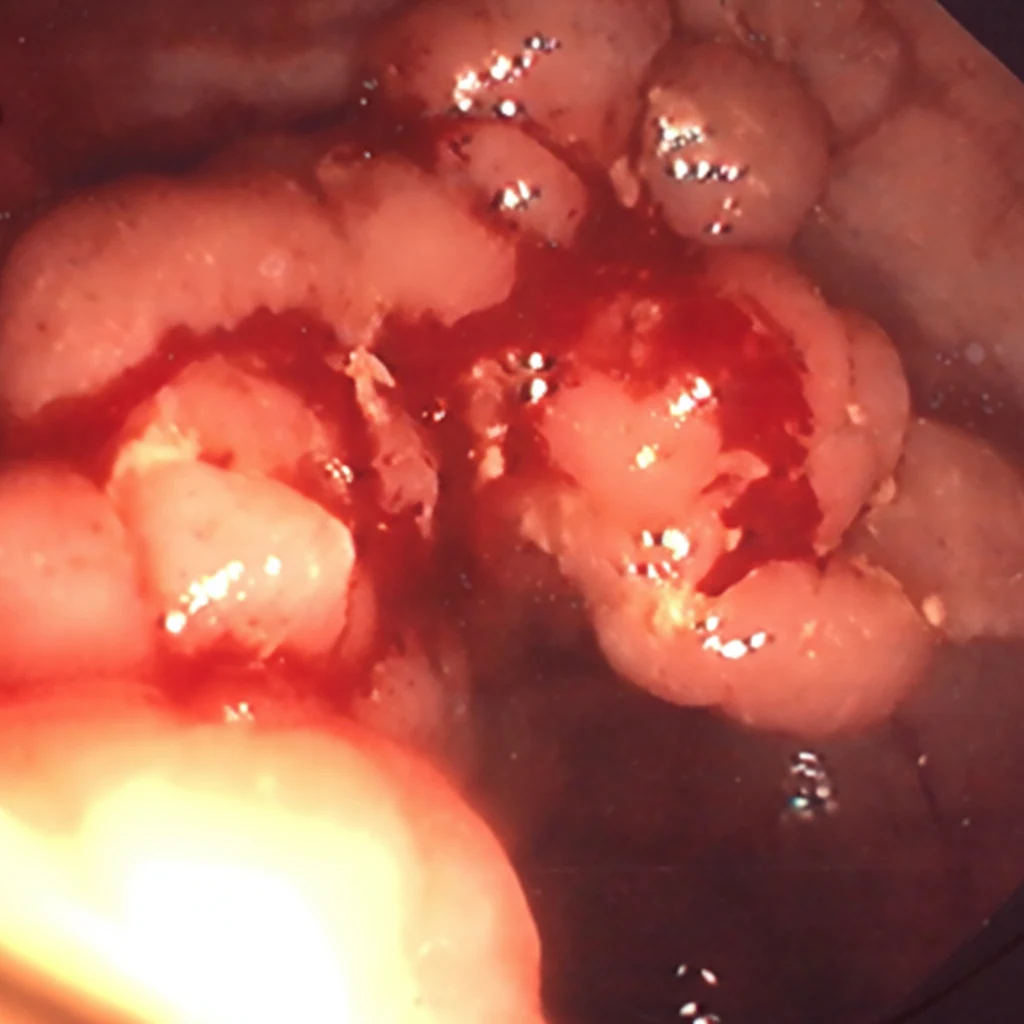
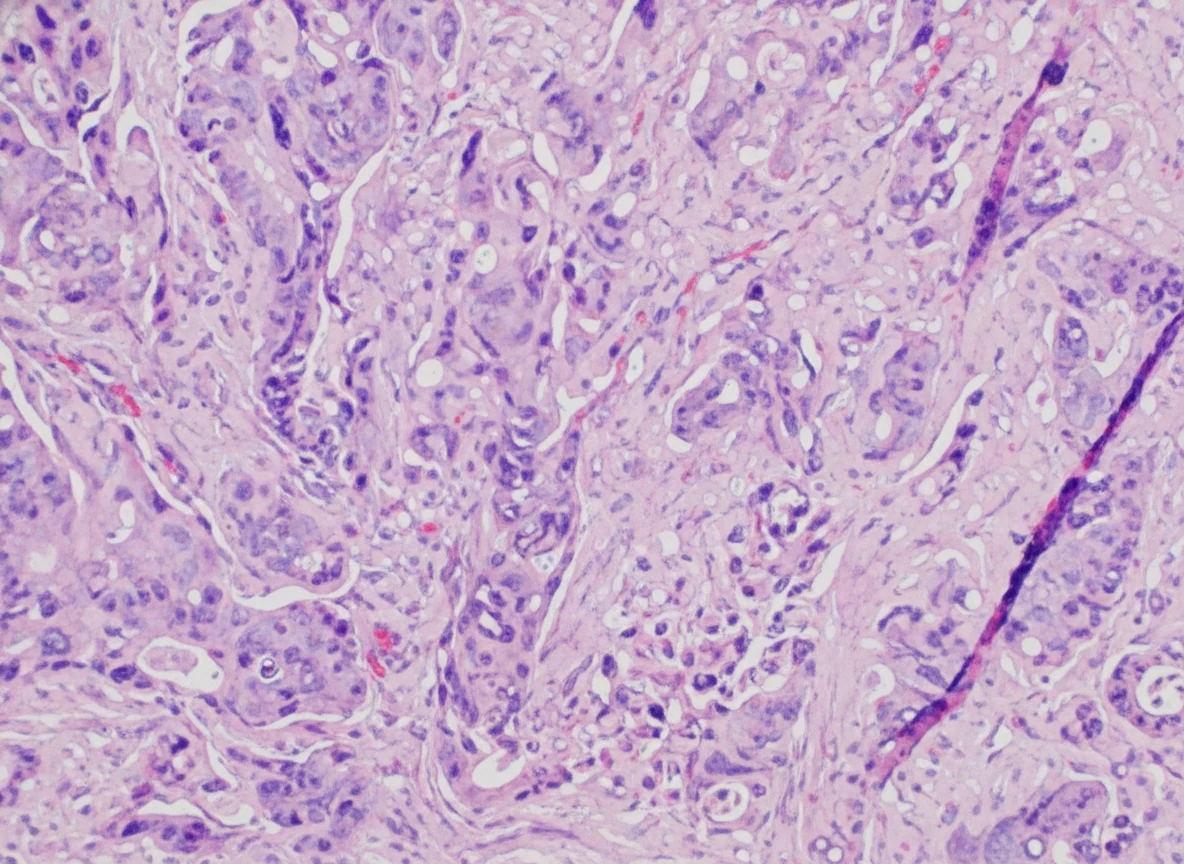
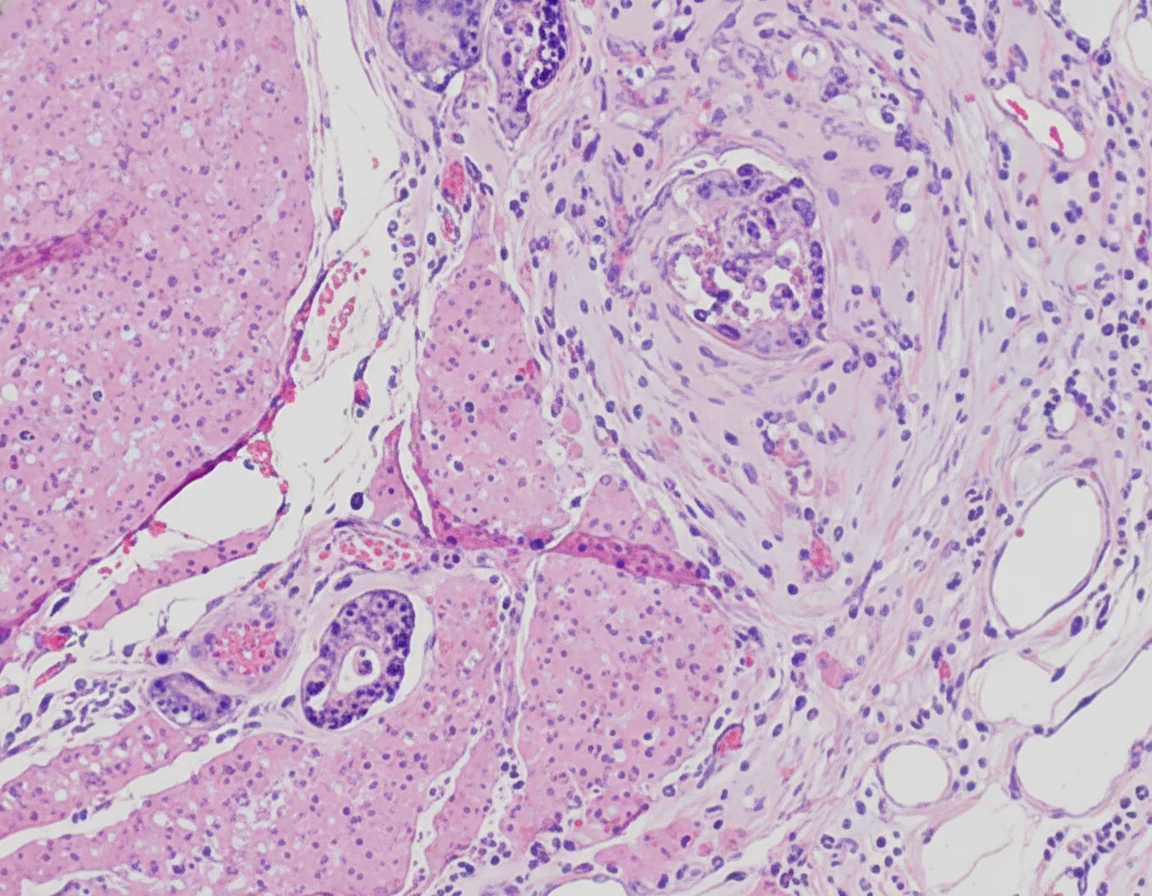
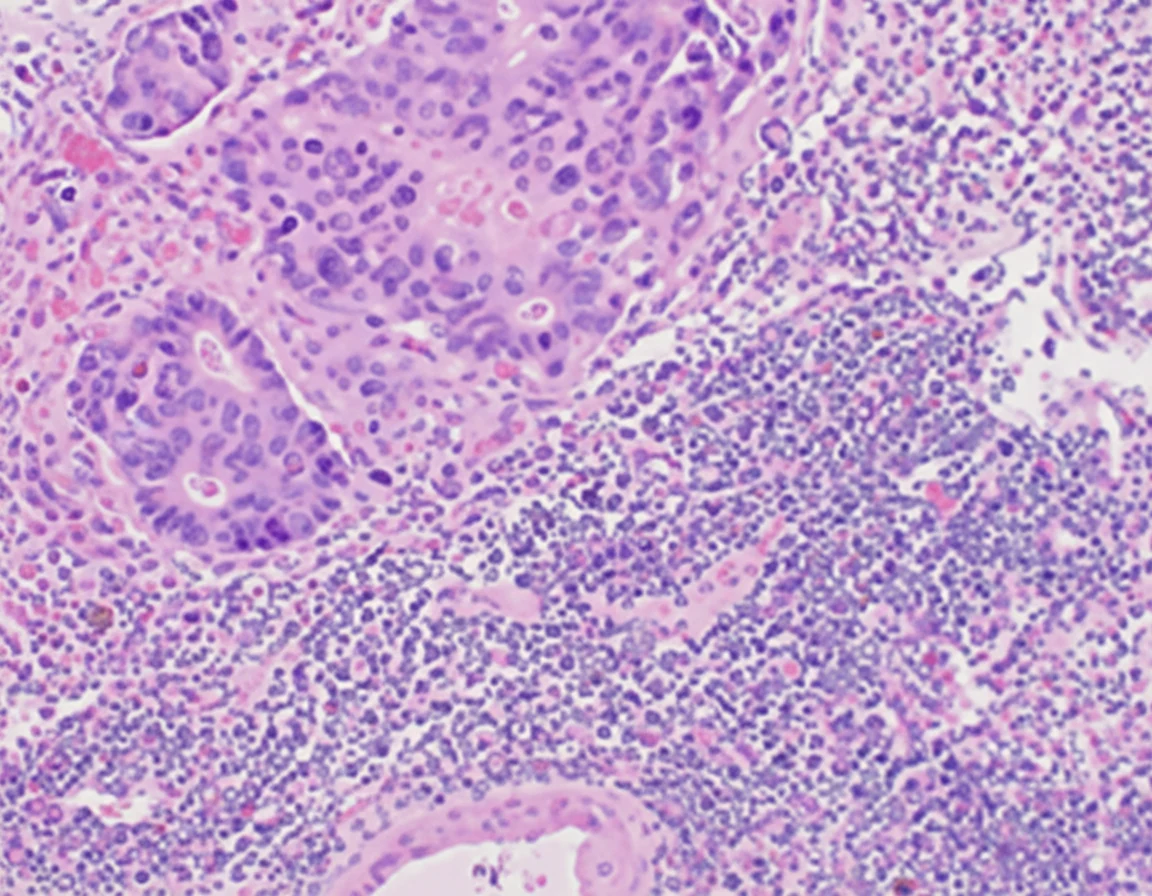
Ένας 67χρονος ασθενής , ο οποίος διαγνώστηκε με πολλαπλούν μυέλωμα , το 2017 , αντιμετωπίστηκε αρχικά με την χορήγηση lenalidomide, bortezomib, dexamethasone και zoledronic acid . Επετεύχθη τότε μερική ανταπόκριση , σύμφωνα με τα κριτήρια του International Myeloma Working Group (IMWG) . Εικόνα 1 . Χρώση με αιματοξυλίνη και εωσίνη , αναδεικνύουσα κυτταροβριθή μυελό με τριπλή αιμοποίηση – όλων των σειρών – και άφθονα ώριμα μικρά πλασματοκύτταρα . Ο ασθενής , θεωρήθηκε καλός υποψήφιος για αυτόλογη μεταμόσχευση , καθώς ήταν σε άριστη γενική κατάσταση , δεν εμφάνιζε καμία οργανική δυσλειτουργία και τέλος επετεύχθη επιτυχής συλλογή βλαστοκυττάρων . Μετά από 6 κύκλους της αρχικής θεραπείας , μεταπήδησε στο σχήμα daratumumab , pomalidomide , και dexamethasone , με την ελπίδα να επιτευχθεί η δυνατόν καλύτερη ανταπόκριση πριν από την αυτόλογη μεταμόσχευση βλαστοκυττάρων . Η μεταμόσχευση εκτελέστηκε με επιτυχία και ο ασθενής βρισκόταν κάτω από την στενή παρακολούθηση των αιματολόγων . Το 2019 και ενώ η αρχική νόσος ήταν σε ύφεση , παραπονέθηκε για κοιλιακό άλγος και παραγωγή/έξοδο σκουρόχρωμων κοπράνων . Η αξονική τομογραφία κοιλίας , ανέδειξε την παρουσία πιθανότατα νεοπλασματικής βλάβης στο τυφλό . Ακολούθως , εκτελέσαμε κολοσκόπηση , η οποία ανέδειξε την παρουσία μάζας , περίπου 6 εκ . από την οποία και ελήφθησαν πολλαπλές βιοψίες , οι οποίες έθεσαν την διάγνωση ενός μετρίως διαφοροποιημένου αδενοκαρκινώματος . Εικόνα 2 . Κολοσκόπηση . Ανθοκραμβοειδής μάζα τυφλού . ( Αρχείο κος Β . Πενόπουλος ) . Εικόνα 3 . Αξονική Τομογραφία κοιλίας . Κόκκινο βέλος . Καρκίνος τυφλού . (Αρχείο κος Β . Πενόπουλος ) . Σημειωτέον , ο ασθενής είχε ελεγχθεί το 2016 κολοσκοπικά και είχαν αφαιρεθεί δύο καλοήθεις υπερπλαστικοί πολύποδες από το κατιόν κόλον . Με την σύμφωνη γνώμη των αιματολόγων , εκτελέσαμε δεξιά ημικολεκτομή. Η σταδιοποίηση της νόσου , ήταν IIIB (pT3N2aM0) . Εικόνα 4 . Παρασκεύασμα δεξιάς ημικολεκτομής .(Αρχείο κος Β . Πενόπουλος). Εικόνα 4 . Μετρίως διαφοροποιημένο καρκίνωμα τυφλού . (Αρχείο κος Β . Πενόπουλος ) . Εικόνα 5 . Διήθηση περικολικού λίπους . (Αρχείο κος Β . Πενόπουλος ) . Εικόνα 6 . Διήθηση περιοχικών λεμφαδένων . (Αρχείο κος Β . Πενόπουλος ) . Ο ασθενής είχε ομαλή μετεγχειρητική πορεία και εξήλθε του Νοσοκομείου 8 ημέρες αργότερα . Με την σύμφωνη γνώμη ογκολόγων και αιματολόγων , ξεκίνησε την λήψη συμπληρωματικής αγωγής που περιελάμβανε την λήψη capecitabine και την συνέχιση της διφωσφονικής θεραπείας για 6 μήνες . Κατά την διάρκεια αυτής της περιόδου , η κατάσταση του μυελώματος παρέμεινε σταθερή , με την μονοκλωνική πρωτείνη – Μ – spike επίπεδα 0.26 g/dL. Κατόπιν τούτου , ανέλαβε εκ νέου την κατευθυνόμενη προς το μυέλωμα θεραπέια , με daratumumab , pomalidomide , και dexamethasone .
Παρουσίαση Περιστατικού
Οι εξελίξεις στην θεραπευτική αντιμετώπιση του πολλαπλού μυελώματος , συμπεριλαμβανομένου του συνδυασμού υψηλών δόσεων melphalan και αυτόλογης μεταμόσχευσης βλαστοκυττάρων , καθώς και η εισαγωγή νέων ανοσο-τροποποιητικών κατά του μυελώματος παραγόντων και αναστολέων των πρωτεασωμάτων , έχουν αυξήσει το προσδόκιμο επιβίωσης των ασθενών με πολλαπλούν μυέλωμα . Όμως , με την επιμήκυνση της επιβίωσης , η αντιμετώπιση κλινικών καταστάσεων , οι οποίες σχετίζονται με την παράταση του χρόνου ζωής , όπως οι δευτερογενείς πρωτοπαθείς κακοήθειες , καθίσταται πλέον σχετικό κλινικά . Οι δευτερογενείς πρωτοπαθείς κακοήθειες , πρωτίστως εκδηλώνονται σαν αιματολογικές κακοήθειες , με 7πλάσια αύξηση της εμφάνισης οξείας μυελογενούς λευχαιμίας , μετά την διάγνωση του πολλαπλού μυελώματος . Πάντως οι συμπαγείς δευτερογενείς πρωτοπαθείς κακοήθειες , έχουν μελετηθεί / ανακοινωθεί , σε μία μελέτη 36.491 περιπτώσεων πολλαπλού μυελώματος , στο Surveillance Epidemiology and End Result (SEER) Program , μεταξύ 1973 και 2008 , με την ετερογενή κατανομή του κινδύνου βασιζόμενη στο ειδικό συμπαγή υπο-τύπο . Η σχέση , ανάμεσα στην θεραπεία του πολλαπλού μυελώματος και των δευτερογενών πρωτοπαθών κακοηθειών , πρωτοεντοπίστηκε το 1996 , από τον Govindarajan et al. , μετά την χορήγηση υψηλών δόσεων χημειοθεραπέιας , ιδιαίτερα melphalan . Επιπρόσθετα , ο Krishnan et al. , διαπίστωσε την παρουσία αυξημένου κινδύνου κατά 11.2% ανάπτυξης δευτερογενών πρωτοπαθών κακοηθειών , 10 χρόνια μετά την αυτόλογη μεταμόσχευση βλαστοκυττάρων . Με την εξέλιξη των ανοσο-τροποποιητικών φαρμάκων , βρέθηκε μία συσχέτιση μεταξύ της lenalidomide και των δευτερογενών πρωτοπαθών όγκων , ιδιαίτερα σε ασθενείς που έλαβαν από του στόματος melphalan . Η ανάπτυξη των δευτερογενών πρωτοπαθών κακοηθειών , είναι πιθανότατα πολυπαραγοντική , συμπεριλαμβάνοντας , την θεραπεία του πολλαπλού μυελώματος , το μικροπεριβάλλον του όγκου , γενετικούς και περιβαλλοντικούς παράγοντες . Ο μηχανισμός δράσης της lenalidomide , είναι σύνθετος και η ικανότητα της να προωθεί την ανάπτυξη ΔΠΚ , παραμένει ασαφής . Τα ανοσοκατασταλτικά αποτελέσματα του φαρμάκου , στο μικροπεριβάλλον του όγκου , μπορεί να οδηγήσουν στην διαφυγή και / ή την ανάπτυξη ανώμαλων ογκογόνων κλώνων , με αποτέλεσμα την ανάπτυξη ενός ΔΠΚ . Διευκόλυνση στην ανάπτυξη ενός ΔΠΚ , μπορεί να προκύψει , καθώς η lenalidomide , εμποδίζει τους μηχανισμούς αποκατάστασης αφαιρεθέντων νουκλεοτιδίων , μετά από βλάβη στο DNA που προκλήθηκε από την χορήγηση melphalan . Ο κίνδυνος ανάπτυξης ορθο-κολικού καρκίνου , αυξάνεται κατά 50 % , 5 χρόνια μετά την διάγνωση πολλαπλού μυελώματος και μπορεί να οφείλεται σε συσχετιζόμενες ανοσολογικές ανωμαλίες των δύο ασθενειών . Είναι δύσκολο να διαπιστωθεί , αν κάποιος ειδικός παράγοντας , συνετέλεσε στην ανάπτυξη του καρκίνου του τυφλού στον ασθενή μας , μετά την λήψη θεραπευτικής αγωγής και μεταμόσχευσης για την αντιμετώπιση του πολλαπλού μυελώματος ή απλά η εμφάνιση του καρκίνου θα μπορούσε να αποδοθεί στην ηλικία του . Στο σημείο αυτό , θα θέλαμε να υπενθυμίσουμε , ότι το 2016 , είχαν αφαιρεθεί κολοσκοπικά από τον ασθενή 2 υπερπλαστικοί πολύποδες , ενώ το 2014 η εκτελεσθείσα προληπτική κολοσκόπηση , ήταν απολύτως φυσιολογική . Επιπρόσθετα , πρέπει να τονιστεί , πως κατά την διάρκεια της συμπληρωματικής θεραπείας με capecitabine , για τον καρκίνο του τυφλού , η θεραπέια για την αντιμετώπιση του ΠΜ ανεστάλη , εκτός από το zoledronic acid και πσρ’ όλα αυτά , οι δείκτες δραστηριότητας του μυελώματος , παρέμειναν σταθεροί . Επομένως , παραμένει άγνωστος σε εμάς , ο λόγος για τον οποίο η νόσος του ασθενή παρέμεινε σταθερή για περίοδο 6 μηνών χωρίς την λήψη θεραπείας για το μυέλωμα , εκτός από το zoledronic acid . Το πολλαπλούν μυέλωμα , χαρακτηρίζεται , από οστεολυτική νόσο των οστών εξ’ αιτίας της αυξημένης οστεοκλαστικής δραστηριότητας και της μειωμένης οστεοβλαστικής λειτουργίας , στοιχεία που αποτελούν την κυρίαρχη παθολογοφυσιολογική βάση για την χρήση διφωσφονικών στην διαδικασία της νόσου . . Ο ρόλος των διφωσφονικών στην αντιμετώπιση του πολλαπλού μυελώματος , είναι να μειώσει τον αριθμό των σπονδυλικών και μη σπονδυλικών καταγμάτων και των οστεολυτικών βλαβών . Εικοτολογούμε , πως η σταθεροποίηση της νόσου του ασθενή μας , για την 6μηνη περίοδο θεραπέιας του καρκίνου του τυφλού , ενδεχόμενα να οφείλεται στην συνέχιση της χορήγησης του zoledronic acid . Από τα παραπάνω συνάγεται , πως οι ασθενείς θα πρέπει να ενημερώνονται σχετικά με τους κινδύνους ανάπτυξης ΔΠΚ , σαν αποτέλεσμα της χορηγούμενης θεραπείας για την αντιμετώπιση του πολλαπλού μυελώματος .


Συζήτηση
Συσσωρευμένα αποδεικτικά στοιχεία , υποστηρίζουν την συσχέτιση μεταξύ πολλαπλού μυελώματος και της ανάπτυξης ΔΠΚ , είτε οφειλόμενης στην θεραπεία είτε σαν αποτέλεσμα της υποκείμενης διαδικασίας της νόσου . Ο ασθενής μας , αντιμετωπίστηκε επιτυχώς χειρουργικά , έλαβε συμπληρωματική θεραπεία για τον καρκίνο του τυφλού , ενώ διέκοψε την θεραπευτική αγωγή κατά του μυελώματος , χωρίς να εντοπιστούν επιπλοκές.Η δε συνέχιση λήψης των διφωσφονικών , ενδεχόμενα παρείχε κάποιο προφυλακτικό αποτέλεσμα έναντι του μυελώματος . Οι κλινικοί ιατροί , οφείλουν να είναι προσεκτικοί , σχετικά με την πιθανότητα ανάπτυξης ΔΠΚ , κατά την διάρκεια χορήγησης ανοσο-τροποποιητικών θεραπειών ή κυτταροτοξικών χημειοθεραπειών πριν από την αυτόλογη μεταμόσχευση για την αντιμετώπιση του πολλαπλού μυελώματος .
Συμπεράσματα
<p><strong><u>Συγκεντρωτικά στοιχεία υποστηρίζουν μια συσχέτιση μεταξύ του πολλαπλού μυελώματος και της ανάπτυξης μιας δευτερογενούς πρωτοπαθούς κακοήθειας (SPM), είτε αποδιδόμενης στη θεραπεία είτε ως αποτέλεσμα της υποκείμενης διαδικασίας της νόσου.</u></strong> Ο ασθενής μας αντιμετωπίστηκε επιτυχώς χειρουργικά, έλαβε επικουρική θεραπεία για καρκίνωμα του τυφλού και διέκοψε την αντιμυελωματική θεραπεία χωρίς να εντοπιστούν επιπλοκές. Η συνεχής χορήγηση διφωσφονικών μπορεί να παρείχε κάποια προστατευτική δράση έναντι του μυελώματος.</p><p>Οι κλινικοί ιατροί θα πρέπει να είναι σε επαγρύπνηση σχετικά με την πιθανότητα ανάπτυξης SPM κατά τη χορήγηση ανοσοτροποποιητικών θεραπειών ή κυτταροτοξικών χημειοθεραπειών πριν από την αυτόλογη μεταμόσχευση για τη διαχείριση του πολλαπλού μυελώματος.</p>
Βασικά Σημεία Μάθησης
- Οι δευτερογενείς συμπαγείς κακοήθειες αποτελούν αναγνωρισμένη όψιμη επιπλοκή της θεραπείας του μυελώματος
- Η παρατεταμένη ανοσοτροποποιητική θεραπεία αυξάνει τον κίνδυνο καρκίνου του παχέος εντέρου
- Η σιδηροπενική αναιμία σε ασθενείς με μυέλωμα θα πρέπει να οδηγήσει σε κολονοσκοπική αξιολόγηση
- Η διεπιστημονική συνεργασία μεταξύ χειρουργικής ογκολογίας και αιματολογίας είναι απαραίτητη
- Η επιτήρηση για καρκίνο του παχέος εντέρου θα πρέπει να λαμβάνεται υπόψη σε μακροχρόνιους επιζώντες μυελώματος
This is a unique reported case of invasive cecal adenocarcinoma developing after autologous stem cell transplantation for multiple myeloma.
Συνδεθείτε για να σχολιάσετε
Φόρτωση...